细胞分布宽度与冠状动脉粥样硬化性心脏病及其病变程度的相关研究
2013-03-04 00:38:58董梦舒吴清华
重庆医学 2013年8期
董梦舒,吴清华
(南昌大学第二附属医院心血管内科 330006)
冠状动脉粥样硬化性心脏病(coronary heart disease,CHD)已成为危害人类健康和生命的重要疾病,寻求简便易行的检测指标对CHD患者行早期危险分层,区分高危人群,是临床急需解决的问题。近年发现红细胞分布宽度(red cell distribution width,RDW)与急性心肌梗死[1-3]、心力衰竭[4-5]和稳定型心绞痛[6-8]的不良预后密切相关。本研究以2007年1月至2011年6月在本院行冠状动脉造影的患者为研究对象,回顾分析RDW水平与冠状动脉病变程度的关系,以及RDW是否是CHD的独立危险因素,为CHD的早期防治提供科学依据。
1 资料与方法
1.1 一般资料 收集2007年1月至2011年6月在本院行冠状动脉造影检查确诊为CHD的患者424例,其中男性319例(75%),女性105例(25%),年龄(66.58±11.46)岁。CHD诊断标准为冠状动脉及其主要分支内径狭窄大于或等于50%。排除心肌病、血液系统疾病、肝肾功能不全、冠状动脉旁路移植或冠状动脉内支架术病史者。
1.2 方法及评估 采用Gensini评分[9]方法对冠状动脉病变程度作定量分析。每处病变的积分为狭窄程度评分(狭窄程度1%~25%为1分,26%~50%计2分,51%~75%计4分,76%~90%计8分,91%~99%计16分,100%计32分)乘以病变部位评分(左主干病变计5分,左前降支或回旋支近段计2.5分,左前降支中段计1.5分,左前降支远段、左回旋支中、远段计1分,右冠状动脉计1分),每例患者的积分为所有病变积分的总和。
1.3 统计学处理 应用SPSS17.0统计软件进行数据分析,计量资料以±s表示,组间比较采用t检验和χ2检验,计量资料间相关性采用直线相关分析,以P<0.05为差异有统计学意义。
2 结 果
4组Gensini评分、CHD病变程度相关危险因素及RDW与其他指标的相关性分析见表1~3。直线相关分析显示RDW 与Gensini评分正相关(r=0.207,P<0.05),见图1。

表1 各组基本临床资料Gensini评分比较

续表1 各组基本临床资料Gensini评分比较
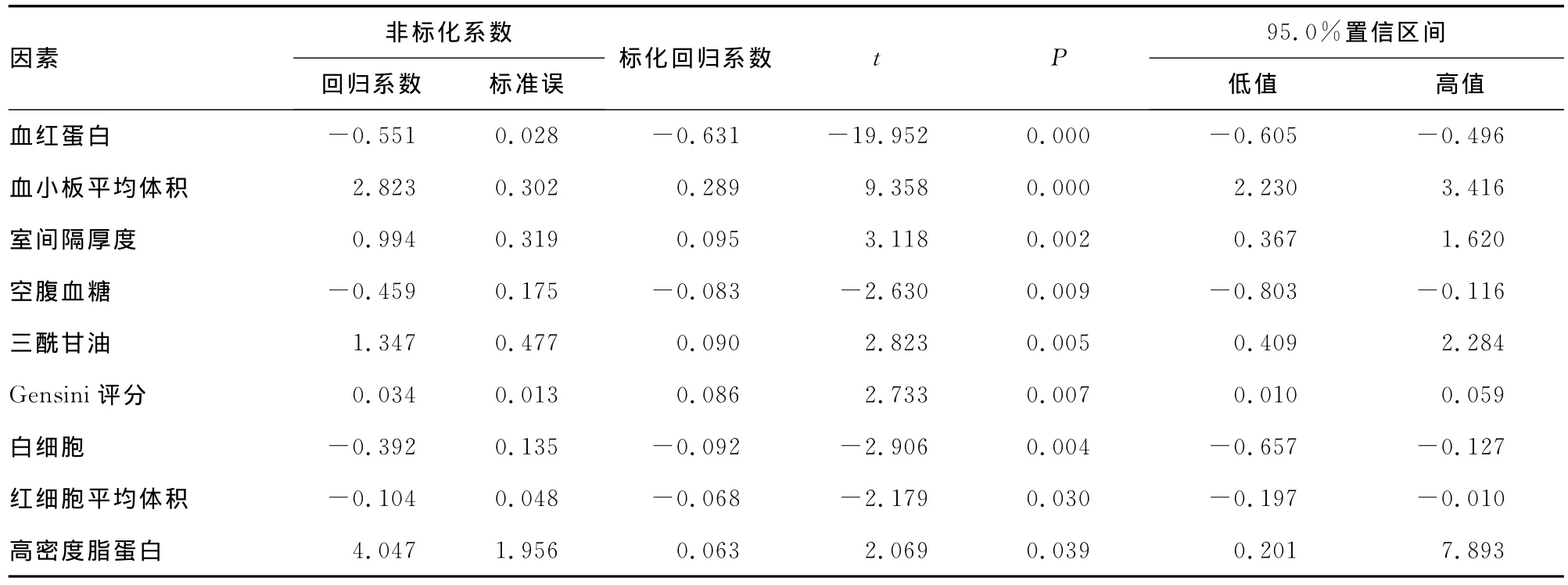
表2 RDW与其他指标的相关性分析
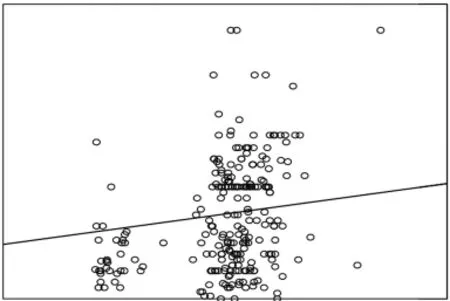
图1 CHD患者RDW水平与Gensini评分散点图

表3 Gensini评分与相关危险因素的相关分析
3 讨 论
本研究发现,随着冠状动脉病变加重,RDW逐渐增高,差异有统计学意义,可能是CHD病变程度的早期预测因子。同时,在以RDW为因变量的回归分析中显示RDW的升高与多种因素相关,其中与血红蛋白(Hb)呈负相关,在控制了Hb后,RDW依然与Gensini评分独立相关,可能是病变早期伴有红细胞破坏或无效造血时,RDW已经发生变化,但Hb可能仍正常[10],因而RDW较Hb更敏感。
RDW影响冠状动脉病变程度的生理机制尚不明确,一些研究认为RDW增高是机体潜在炎症状态的标志物[7],炎症能影响红细胞生成、红细胞半衰期、红细胞细胞膜可变形性等一些增加红细胞异质性的因素[11],同时大量炎症因子抑制骨髓造血功能和促红细胞生成素的生成、影响铁代谢[12],抑制红细胞成熟,幼稚红细胞释放入血循环导致RDW增高[13]。已发现C-反应蛋白[14]、白介素-6[15]等炎性标记因子与冠状动脉病变程度相关。在本研究中发现,非特异性炎症指标白细胞可能是RDW的独立影响因子,随着冠状动脉病变的加重及心功能的恶化,白细胞逐渐升高,具有明显统计学意义。
此外,病程中神经内分泌系统激活,缩血管物质水平增高,使肾血管收缩,造成肾缺血性损伤,促红细胞生成素合成下降,骨髓内红细胞生成减少引起贫血[16]。肾功能减退亦被认为是心血管事件的独立预测因子[17]。肾小球滤过率随RDW增加而逐级递减[18],低滤过率可强烈预测高RDW,提示RDW与肾功能之间呈负性相关性。最后,临床上血管紧张素转换酶抑制剂在CHD患者中的大量应用,干扰了促红细胞生成素的生成和骨髓红细胞生成素的活性致贫血发生[19]。上述任何一种或多种作用机制最终都可影响红细胞生成,进而导致RDW增高。
本研究以Gensini评分来量化冠状动脉病变程度,应用多元回归模型分析研究RDW与冠状动脉病变程度的关系,较好地控制了混杂偏倚,但CHD影响因素较多,无法将其他因素一一进行匹配对比分析。未来研究方向应致力于进一步了解RDW与CHD相关的病理生理机制,以对CHD的早期防治有更深入的认识。
[1]Uyarel H,Ergelen M,Cicek G,et al.Red cell distribution width as a novel prognostic marker in patients undergoing primary angioplasty for acute myocardial infarction[J].Coron Artery Dis,2011,22(3):138-144.
[2]Dabbah S,Hammerman H,Markiewicz W,et al.Relation between red cell distribution width and clinical outcomes after acute myocardial infarction[J].Am J Cardiol,2010,105(3):312-317.
[3]Poludasu S,Marmur JD,Weedon J,et al.Red cell distribution width(RDW)as a predictor of long-term mortality in patients undergoing percutaneous coronary intervention[J].Thromb Haemost,2009,102(3):581-587.
[4]Felke GM,Allen LA,Poeoek SJ,et al.Red cell distribut ion width as a Hovel prognost ic marker in heart failure:data from CHARM program and the duke databank[J].J Am Coil Cardinl,2007,50(1):40-47.
[5]Al-Najjar Y,Goode KM,Zhang J,et al.Red cell distribution width:an inexpensive and powerful prognostic marker in heart failure[J].Eur J Heart Fail,2009,11(12):1155-1162.
[6]Fukuta H,Ohte N,Mukai S,et al.Elevated plasma levels of B-type natriuretic peptide but not C-reactive protein are associated with higher red cell distribution width in patients with coronary artery disease[J].Int Heart J,2009,50(3):301-312.
[7]Tonelli M,Sacks F,Arnold M,et al.Relation between red blood cell distribution width and cardiovascular event rat e in people with coronary disease[J].Circulation,2008,117(2):163-168.
[8]Isik T,Uyarel H,Tanboga IH,et al.Relation of red cell distribution width with the presence,severity,and complexity of coronary artery disease[J].Coron Artery Dis,2012,23(1):51-56.
[9]Gensini GG.A more meaningful scoring system for determining the severity of coronary heart disease[J].Am J Cardiol,1983,51(3):606.
[10]McLaughlin VV,Presberg KW,Doyle RL,et al.Prognosis of pulmonary arterial hypertension:ACCP evidence based clinical practice guidelines[J].Chest,2004,126(1):S78-92.
[11]Weiss G,Goodnough LT.Anemia of chronic disease[J].N Engl J Med,2005,352(10):1011-1023.
[12]Deswal A,Peterson MJ,Feldman AM,et al.Cytokines and cytokine receptors in advanced heart failure:an analysis of the cytokine database from the Vesnarinone Trial(VEST)[J].Circulation,2001,103(16):2055-2059.
[13]Caramelo C,Justo S.Anemia in heart failure[J].Rev Esp Carliol,2007,60(8):848-60.
[14]Drakopoulou M,Toutouzas K,Stefanadi E,et al.Association of inflammatory markers with angiographic severity and extent of coronary artery disease[J].Atherosclerosis,2009,206(2):335-339.
[15]Tanindi A,Sahinarslan A,Elbeg S,et al.Relationship between MMP-1,MMP-9,TIMP-1,IL-6and risk factors,clinical presentation,extent and severity of atherosclerotic coronary artery disease[J].Open Cardiovasc Med J,2011,5:110-116.
[16]Spinarova L,Toman J,Pospisilova J,et al.Humoral response in patients with chronic heart failure[J].Int J Cardiol,1998,65(3):227-232.
[17]Dries DL,Exner DV,Domanski MJ,et al.The prognostic implications of renal insufficiency in a symptomatic and symptomatic patients with left ventricular systolic dysfunction[J].J Am Coll Cardiol,2000,35(3):681-689.
[18]Lippi G,Targher G,Montaqnana M,et al.Relationship between red blood cell distribution width and kidney function tests in a large cohort of unselected outpatients[J].Scand J Chin Lab Invest,2008,68(8):745-748.
[19]Chatterjec B,Nydegger UE,Mohacsi P.Serum erythropoietin in heart failure patients treated with ACE-inhibitors or ATI antagonists[J].Eur J Heart Fail,2000,2(4):393-398.
猜你喜欢
家教世界(2022年34期)2023-01-08 13:52:50
意林(2021年2期)2021-02-08 08:32:47
考试与评价·八年级版(2020年4期)2020-10-26 02:25:23
考试与评价·八年级版(2020年1期)2020-10-26 02:24:50
考试与评价·八年级版(2020年1期)2020-10-26 02:24:50
兽医导刊(2016年6期)2016-05-17 03:50:31
断块油气田(2014年6期)2014-03-11 15:33:53
当代畜禽养殖业(2014年12期)2014-02-27 08:00:10
当代畜禽养殖业(2014年11期)2014-02-27 08:00:01
环球时报(2012-03-21)2012-03-21 14:05:51