
Management of Pregnancy with Ankylosing Spondylitis
2012-11-22 02:36:40QianZhouXumingBianandJuntaoLiu
Chinese Medical Sciences Journal 2012年1期
Qian Zhou,Xu-ming Bian*,and Jun-tao Liu
Department of Obestetric and Gynecology,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences &Peking Union Medical College,Beijing 100730,China
ANKYLOSING spondylitis (AS) is a chronic,progressive autoimmune disease,mainly involving sacroiliac joint,vertebral column,paravertebral soft tissue,and joints of four limbs.It is also accompanied with some other manifestations except joint,in which the most common is heart aortic valve lesions.Clinical manifestation is characterized by lumbago,even spinal deformity and arthrocleisis in patients with sever state of illness.A few cases have been reported about the effect of pregnancy on AS.1In order to investigate the treatment for AS during pregnancy and pregnancy outcome,we performed a retrospective analysis of the clinical data of 12 pregnant women with AS.
PATIENTS AND METHODS
Twelve pregnant women with AS were treated in Peking Union Medical College Hospital from September 2004 to July 2011.The average age was 32.7±2.4 years (range,29-38 years).Both 11 cases of primipara and 1 case of pluripara were diagnosed as AS before pregnancy.At the time of AS diagnosis,the patients’ average age was 25.1±4.7 years (range,15-31 years).Drug was administered for case 5 considering patient's condition during pregnancy.General state of the patients’ health as well as diagnosis of and treatment for AS before pregnancy are shown in Table 1.
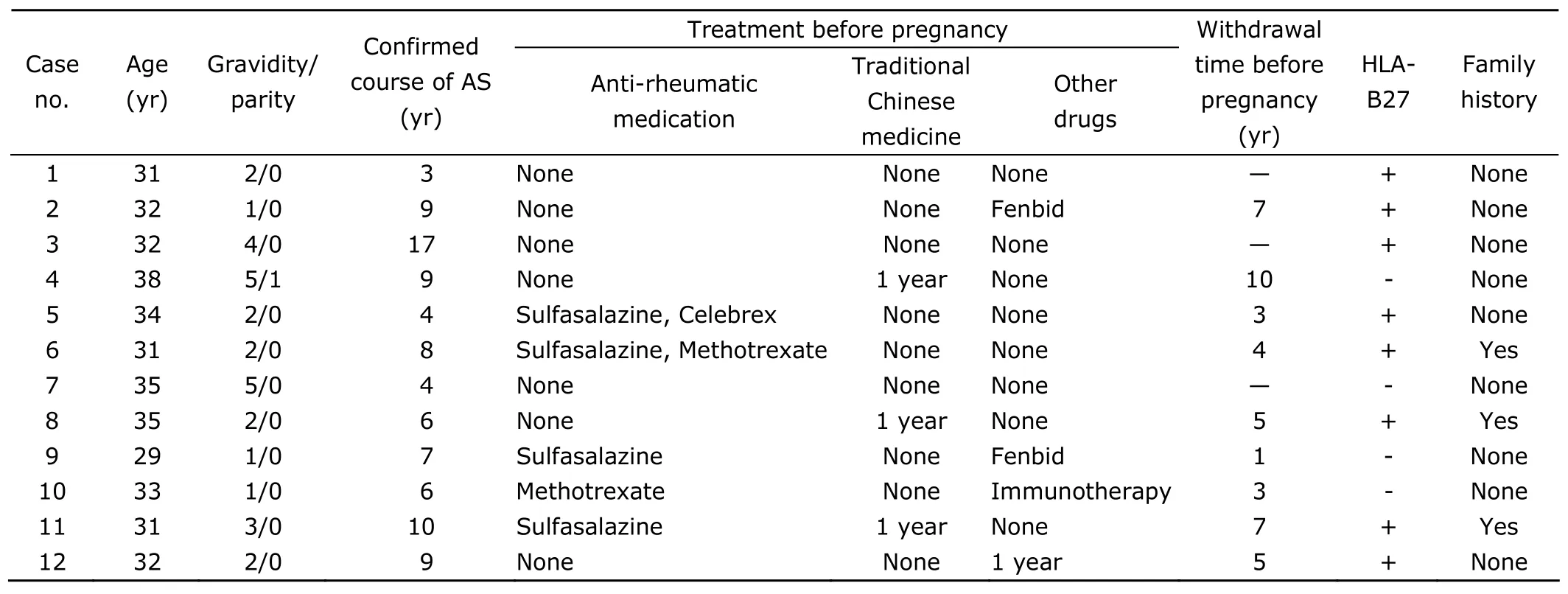
Table 1.General information of 12 pregnant AS patients
RESULTS
Waist pain appeared in cases 1,8,and 9 during the second trimester,which gradually improved with no medication administered.Hip pain became more serious in case 5 during late pregnancy,and laboratory examination showed an increase of erythrocyte sedimentation rate.She was considered suffering from AS in active stage after evaluated by the doctor of rheumatology department.After administration of hexadecadrol,she was kept in a stable condition to full-term pregnancy.In the other 11 cases,the condition of AS was stable during pregnancy.The patients were regularly followed up in the hospital,special attention being paid to pain symptom,fetal growth and development.
All of the 12 pregnant AS patients maintained gestation till term delivery,including 5 cases of spontaneous vaginal delivery (SVD) and 7 cases of cesarean section delivery(CSD) due to obstetric factor.No adverse pregnancy outcome occurred.For the 2 cases with waist pain,case 1 had SVD,and cases 8 and 9 had CSD successfully.Pregnancy complications and pregnancy outcomes of the 12 patients were shown in Table 2.
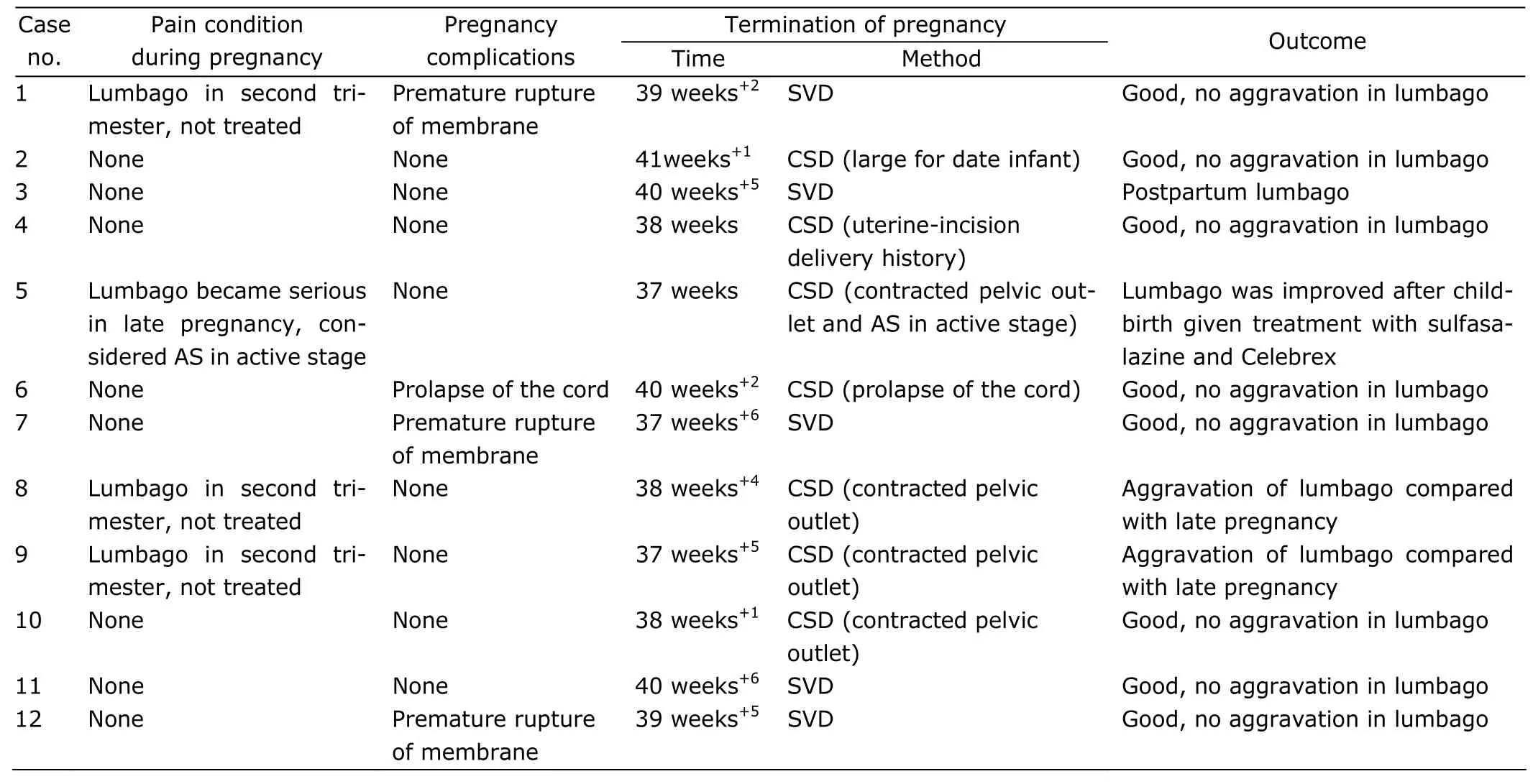
Table 2.Pregnancy complications and outcomes of 12 pregnant AS patients
DISCUSSION
The morbidity of AS varies with country in different reports,and it is 0.26% in China.2It was believed that this disease occurred mostly in male,with the ratio of male to female being 10.6∶1.The ratio acknowledged at present is 5 ∶1.However,female have slower onset and lighter pathogenetic condition.2,3The peak age of AS onset is commonly from 18 to 22 years old,and the onset over 30 years or less than 8 years old is rare.The onset appears insidiously,developing from lumbar to thoracic vertebra and cervical vertebra,accompanied by pain in the corresponding position,limitation of motion,and spinal deformity.4Now,AS is still diagnosed based on New York standard revised in 1984:4(1) pain in inferior part of waist and back lasting for at least 3 months,improved following activity,but not relieved after resting;(2) limitation of forward,backward,and lateral activity for lumbar;(3)compromised chest expansion compared with the same age and same sex;(4) bilateral sacroiliitis at degree II-IV,or unilateral sacroiliitis at degree III-IV.AS can be diagnosed if the patient has (4) combined with any one of(1)-(3).The etiology of this disease is not clear,and epidemic investigation has found that gene and environmental agent play a certain role in the onset.It has been proved that AS onset has a close relationship with HLA-B27 (+),5and is significantly predisposed to family clan.Although the positive rate of HLA-B27 in AS patients reaches about 90%,it is not a specific diagnosis,because there is also HLA-B27(+) person in healthy population.As for HLA-B27 (-) patients,as long as clinical and imaging test accord with AS diagnostic criteria,AS can not be ruled out.
It is difficult to evaluate whether AS is in active stage in pregnant patients.During pregnancy,erythrocyte sedimentation rate,C-reactive protein,and other indexes as well as pain and other clinical symptoms are not obvious,thus the patients should be dynamically and closely observed.
Previous reports expressed controversial views on the effect of pregnancy on AS.Some believe that the condition of 80% of AS patients may change during pregnancy.5Lumbago becomes more serious in second trimester,is relieved in late pregnancy,and may be aggravated 6-12 weeks after childbirth.6,7It is relatively difficult to evaluate whether AS is in active stage based on the degree of lumbar pain in pregnancy,because the reason of lumbago can not be distinguished clearly.Østensen et al7reported that in 9 pregnant women suffering from AS,the pain symptom increased in 7 during second trimester,but was relieved in late pregnancy;the symptom aggravated again in 8 cases 12 weeks after childbirth,7 of which were those showing increased pain in second trimester.In this study,lumbago was exacerbated in 3 of the 12 pregnant AS patients.Based on immunology evaluation,the disease activity was not considered,therefore,the 3 cases did not receive drug treatment,and the patients’ condition was improved in late pregnancy.Drug was administered in case 5 considering the patient's condition,and she continued to take anti-rheumatic medication after childbirth.Three cases showed aggravated pain after childbirth.AS condition kept stable for 8 cases in pregnancy and after childbirth in the present study.It may suggest that patients developing lumbago in the second trimester are apt to experience postpartum condition change.
Reports have showed that AS has no significant effect on pregnancy outcome,8,9but anti-rheumatic medication used in AS treatment may produce adverse effect on fetus.10For example,sulfasalazine affects qualities of spermatozoa and ovum;methylaminopterin and non-steroidal anti-inflammatory drugs (NSAID) have teratogenic effect on fetus.Therefore,it is suggested the abovementioned drugs should be stopped more than 3 months before conception.Prednisone can be applied for patients with active condition,because this drug has no harmful effects on fetus.It is also suggested that breast-feed be stopped for the medication-taking patients who have active AS after childbirth.In the present study,the period of drug withdrawal was more than 1 year in all the cases taking medication.Neither obvious complications nor harmful pregnancy outcome occurred.
For AS patients planning to have children,consultation should be conducted,and the doctor of rheumatology should evaluate the patients’ common condition,the stage of AS,and drug safety.The patients who have suffered from severe joint or spinal deformity and no ability of self-care are difficult to bear pregnancy and delivery,so the risk of pregnancy should be fully explained to the patients for careful consideration.11During pregnancy,regular monitoring and condition evaluation should be preformed for AS patients.If the AS symptom in early pregnancy is not alleviated by medication,termination of pregnancy is suggested.For AS activity in second trimester,prednisone can be used,and minimum effective dosage is better.Drugs affecting pregnancy outcome (e.g.sulfasalazine,NSAID) should be used with extreme caution.In choosing delivery mode,combination of AS is not the indication for CSD,and delivery mode choice is mainly dependent on obstetric indication.It has also been reported that choice of delivery mode does not affect AS condition and pregnancy outcome.12The pregnant AS patients’condition may be aggravated 6-12 weeks after childbirth.13Therefore,close monitoring is required after delivery.Drug treatment (sulfasalazine,methylaminopterin,etc.) should be performed if the patients’ condition deteriorates,and breast-feeding should be stopped during medication.
In conclusion,AS is a disease related to hereditary factor.AS patients should be fully evaluated both before and during pregnancy.The patients are suggested not consider pregnancy until the condition becomes stable.Close monitoring and regular follow-up during pregnancy and after childbirth are necessary to ensure good pregnancy outcome and prognosis.
1.Anderson JJ,Baron G,van der Heijde D,et al.Ankylosing spondylitis assessment group preliminary definition of short-term improvement in ankylosing spondylitis.Arthritis Rheum 2001;44:1876-86.
2.Ostensen M,Ostensen H.Ankylosing spondylitis-the female aspect.J Rheumatol 1998;25:120-4.
3.Adams DD,Knight JG,Ebringer A.Autoimmune diseases:solution of the environmental,immunological and genetic components with principles for immunotherapy and transplantation.Autoimmun Rev 2010;9:525-30.
4.Braun J,Sieper J.Ankylosing spondylitis.target treatment criteria.Z Rheumatol 2009;68:30-6.
5.Märker-Hermann E,Fischer-Betz R.Rheumatic diseases and pregnancy.Curr Opin Obstet Gynecol 2010;22:458-65.
6.Østensen M,Husby G.Ankylosing spondylitis and pregnancy.Rheum Dis Clin North Am 1989;15:241-54.
7.Østensen M,Fuhrer L,Mathieu R,et al.A prospective study of pregnant patients with rheumatoid arthritis and ankylosing spondylitis using validated clinical instruments.Ann Rheum Dis 2004;63:1212-7.
8.Munoz-Suano A,Hamilton AB,Betz AG.Gimme shelter:the immune system during pregnancy.Immunol Rev 2011;241:20-38.
9.Marker-Hermann E,Bauer H,Gromnica-Ihle E.Rheumatic diseases in pregnancy.Dtsch Med Wochenschr 2008;133:2410-4.
10.Østensen M,Lockshin M,Doria A,et al.Update on safety during pregnancy of biological agents and some immunosuppressive antirheumatic drugs.Rheumatology (Oxford) 2008;47 Suppl 3:iii28-31.
11.Clowse ME.Managing contraception and pregnancy in the rheumatologic diseases.Best Pract Res Clin Rheumatol 2010;24:373-85.
12.Incel NA,Erdem HR,Ozgocmen S,et al.Pain pressure threshold values in ankylosing spondylitis.Rheumatol Int 2002;22:148-50.
13.Gromnica-Ihle E,Østensen M.Pregnancy in patients with rheumatoid arthritis and inflammatory rheumatic diseases.Z Rheumatol 2006;65:209-12,214-6.
 Chinese Medical Sciences Journal2012年1期
Chinese Medical Sciences Journal2012年1期
- Chinese Medical Sciences Journal的其它文章
- Applicability of Community Periodontal Index Teeth and Random Half-mouth Examination to Gingival Bleeding Assessment in Untreated Adult Population in Beijing
- Personalized Management of Anastomotic Leak after Surgery for Esophageal Carcinoma
- Spectral Domain Optical Coherence Tomography of Vogt-Koyanagi-Harada Disease:Novel Findings and New Insights into the Pathogenesis
- Radiofrequency Ablation of Hepatic Paragonimiasis:a Case Report
- Electrocorticography with Direct Cortical Stimulation for a Left Temporal Glioma with Intractable Epilepsy
- Primary Sjögren's Syndrome Accompanied by Intestinal Obstruction:a Case Report and Literature Review