
Prognostic value of clonal evolution identified by sequential FISH in untreated chronic lymphocytic leukaemia
2024-05-17 07:04RiccardoDondolinMatteoBelliaSilviaRasiClaraDeambrogiDonatellaTalottaSamirMouhssineWaelAlEssaAbdurraoufMokhtarMahmoudDaniloFaraciGianlucaGaidanoRiccardoMoia
Riccardo Dondolin, Matteo Bellia, Silvia Rasi, Clara Deambrogi, Donatella Talotta, Samir Mouhssine,Wael Al Essa, Abdurraouf Mokhtar Mahmoud, Danilo Faraci, Gianluca Gaidano, Riccardo Moia
Division of Hematology, Department of Translational Medicine, Università del Piemonte Orientale and Azienda Ospedaliero-Universitaria Maggiore Della Carità, Novara 28100, Italy.
Abstract Aim: The aim of the current study was to evaluate the potential clinical impact of clonal evolution detected by fluorescence in situ hybridization (FISH) in untreated chronic lymphocytic leukaemia (CLL) patients managed with a watch-and-wait strategy.Methods: We performed both overall survival (OS) and time to first treatment (TTFT) analysis.For the first one,we exploited a real-life cohort of 123 consecutive CLL patients followed at our institution, for which at least a second FISH evaluation during watch and wait was available.For TTFT analysis, we considered only patients treated after the second FISH sample (n = 69).Results: Considering the original cohort, patients who acquired a FISH abnormality displayed a worse outcome with a median OS of 91.9 months compared to 147.3 months for patients who did not acquire any FISH abnormalities (P = 0.007).Unmutated immunoglobulin heavy chain gene (IGHV) genes were associated with a higher probability of acquiring a FISH abnormality (P = 0.04).Turning to TTFT analysis, patients who gained at least one FISH abnormality (n = 7, 10%) were characterised by an earlier treatment requirement with a median TTFT of 1.1 months, compared to 2.7 months in patients who did not acquire any FISH abnormalities(n = 62, 90%) (P = 0.025).Conclusions: The dynamic acquisition of karyotypic abnormalities by FISH predicts poor outcomes and early treatment requirement in CLL patients.Our results suggest that FISH analysis could be integrated with other clinical and biological features to obtain dynamic scores that are able to predict outcomes at different phases of disease history.
Keywords: Chronic lymphocytic leukaemia, FISH analysis, clonal evolution
INTRODUCTION
Chronic lymphocytic leukaemia/small lymphocytic lymphoma (CLL/SLL) is the most common leukaemia in adults in Western countries, accounting for approximately 25% to 35% of all leukaemias[1-4].Most CLL patients, namely Rai 0-I and Binet A, are asymptomatic, do not require therapy, and are managed with a watch-and-wait strategy[4-6].Currently, at least two different models have been devised to identify early-stage CLL patients with a relatively short time to first treatment (TTFT).These models incorporate baseline clinical variables, namely palpable lymph nodes and lymphocyte count, as well as biological features, namely IGHV mutation status and fluorescencein situhybridization (FISH) karyotype[7,8].Since most CLL patients do not require therapy for long periods after diagnosis, this leukaemia may provide an informative model to evaluate the disease’s intrinsic mechanisms of clonal evolution in the absence of the external stimuli imposed by therapy.While the above-mentioned prognostic models consider static clinical and biological features at the time of diagnosis, they do not consider the potential clinical impact of dynamic clonal evolution over time during the watch-and-wait management in the absence of cytoreductive treatment.
The prognostic value of the most frequent CLL karyotypic abnormalities (del13q14, trisomy12, del11q23,and del17p13) identified at the time of diagnosis by FISH has already been established and confirmed by previous studies[9].However, the prognostic impact of dynamic clonal evolution detected by FISH over the course of the natural history of CLL in the absence of treatment has not been explored in detail.
METHODS
We exploited a real-life cohort of 123 consecutive CLL patients followed at our institution and satisfying the following criteria: (i) availability of at least a second FISH evaluation during the watch-and-wait management of the disease; (ii) no treatment requirement for at least 3 months after the date of first FISH analysis.The FISH karyotype was evaluated using the XCE 12 probe for tris12 detection (MetaSystems) with a cut-off for positivity of 3% of the nuclei, XL DLEU/TP53 probe for del17p detection (Cytocell Aquarius)with a cut-off of 5%, XL ATM/11cen locus-specific probe for del11q detection (Cytocell Aquarius) with a cut-off for positivity of 5%, and XL DLEU/LAMP probe for del13q detection (MetaSystems) with a cut-off for positivity of 2%.The endpoints of the study were overall survival (OS) and TTFT.For OS analysis, we considered all 123 patients of the study cohort, whereas for TTFT analysis, we considered only the cases treated after the second FISH sample, obtaining a group of 69 patients.The study was approved by the Ethical Committee of the Ospedale Maggiore della Carità di Novara associated with the Università del Piemonte Orientale (study number CE 120/19).
RESULTS
Patient characteristics are reported in Table 1 and are consistent with those derived from current real-life epidemiological data[10].The median age of the cohort at diagnosis was 68.2 years; 65 patients (53%) carried unmutated IGHV genes, 110 (90%) patients scored Rai 0-1 at diagnosis, and 99 patients (81%) scored Binet A.At the time of the first FISH evaluation, 47 (38%) patients had a normal FISH panel and 76 (62%) cases displayed at least one abnormality.In this second group, 58 patients (76%) carried del13q14, 20 (26%)patients trisomy12, 12 (16%) patients del11q23, and 3 (4%) patients del17p13 [Supplementary Figure 1].
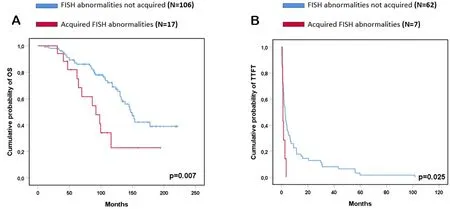
Figure 1.Kaplan-Meier estimates of OS and TTFT according to FISH clonal evolution.(A) OS analysis in patients treated at least 3 months after the first FISH sample.Patients who did not acquire karyotypic abnormalities in the second FISH panel are represented in blue.Patients who acquired karyotypic abnormalities in the second FISH panel compared to the first FISH panel are represented in red.(B) TTFT analysis in patients treated after the second FISH sample.Patients who did not acquire karyotypic abnormalities in the second FISH panel are represented in blue.Patients who acquired karyotypic abnormalities in the second FISH panel compared to the first FISH panel are represented in red.P-value is represented by adjacent curves.
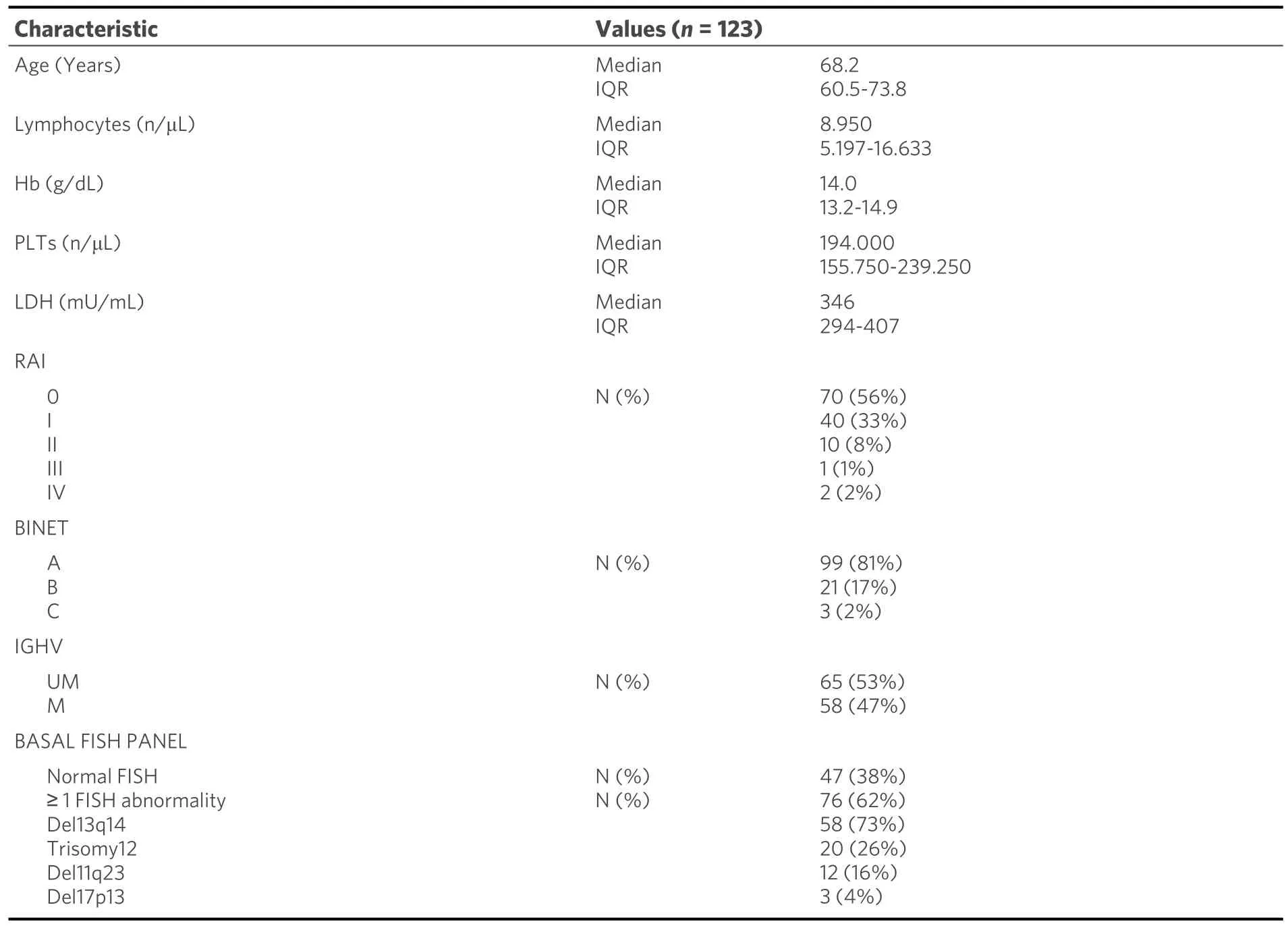
Table 1.Patients characteristics
After a median follow-up of 14.6 years, the median number of sequential FISH evaluations in each patient before the initiation of treatment was 2.7 (range 2-7).During the watch-and-wait management, seventeen patients (14%) acquired a FISH abnormality that was not detectable at the time of diagnosis.Some patients acquired more than one FISH abnormality and a total of 20 abnormalities were detected and distributed as follows: 5 (25%) patients acquired del17p13, 9 (45%) patients acquired del13q14, 3 (15.0%) patients acquired trisomy12, and 3 (15.0%) patients acquired del11q23 [Supplementary Figure 2].In contrast, 97 (79%)patients did not acquire any abnormality and 9 (7%) cases lost at least one FISH alteration that had been previously identified.
Unmutated IGHV genes were associated with a higher probability of acquiring a FISH abnormality.More precisely, 21% of patients with unmutated IGHV genes acquired a FISH abnormality compared to 8% of patients with mutated IGHV genes (P= 0.04).One patient was excluded from this analysis because of a lack of information about IGHV status.Other genetic features investigated at CLL diagnosis in this cohort(mutations ofTP53,NOTCH1,SF3B1, andBIRC3) did not show any significant association with clonal evolution of the FISH karyotype.
In order to evaluate the clinical impact of acquiring clonal evolution by FISH, we evaluated the OS in patients who acquired a FISH abnormality (n= 17, 14%) compared to patients with unchanged FISH or who had lost any abnormality that had been previously detected (n= 106, 86%).By survival analysis [Figure 1A],patients who acquired a FISH abnormality displayed a worse outcome with a median OS of 91.9 months compared to 147.3 months for patients who did not acquire any FISH abnormalities (P= 0.007).The acquisition of at least one FISH abnormality maintained an independent association with OS when adjusted for IGHV mutational status [Table 2].

Table 2.Multivariate analysis
In order to evaluate the impact of FISH evolution on treatment requirement, TTFT analysis was performed considering the 69 patients treated after the second FISH sample [Figure 1B].Seven (10%) patients gained at least one abnormality that was not present in the first FISH panel.More precisely, a total number of 8 gained abnormalities were detected and distributed as follows: 2 (25%) patients gained del17p13, 4 (50%)patients del13q14, 1 (12.5%) patient trisomy12, and 1 (12.5%) patient del11q23.In contrast, 56 (81%)patients did not acquire any abnormalities and 6 (9%) cases lost at least one FISH alteration.Patients who gained at least one FISH abnormality (n= 7, 10%) were characterised by an earlier treatment requirement with a median TTFT of 1.1 months, compared to 2.7 months in patients who did not acquire any FISH abnormalities (n= 62, 90%) (P= 0.025).
DISCUSSION
Overall, this study shows that the acquisition of karyotypic abnormalities by FISH predicts poor outcomes in CLL patients, underscoring the negative prognostic impact of clonal evolution in CLL patients initially managed with a watch-and-wait strategy[11,12].In fact, although the prognostic impact of clonal evolution has already been demonstrated in previous studies, in this work, we analyse a cohort of untreated CLL patients,emphasizing the value of clonal evolution in the absence of the selective pressure induced by therapy[13].In addition, our findings reinforce the notion that molecular predictors should be tested at different times during the course of the disease to ensure correct treatment tailoring[13-15].The retrospective nature of the study and the fact that serial FISH sampling was not pre-scheduled but was decided by clinicians according to the clinical course may represent limitations of the analysis.However, the criteria for sequential FISH sampling were uniform across this monocentric cohort that was managed according to pre-planned diagnostic strategies of the hematological center.Importantly, despite these potential limitations, the acquisition of clonal evolution retained its prognostic value.Future analyses in prospective CLL series should integrate FISH clonal evolution with the investigation of gene mutations and other biological features in order to create a dynamic score that can predict outcomes at different time points of the natural history and clinical course of the disease.
DECLARATIONS
Authors’ contributions
Designed the study, interpreted the data, and wrote the manuscript: Dondolin R, Bellia M, Gaidano G, Moia R
Performed biological studies: Rasi S, Talotta D, Deambrogi C
Contributed to data collection and analysis: Mouhssine S, Al Essa W, Mahmoud AM, Faraci D
Availability of data and materials
Data will be available upon dedicated request.
Financial support and sponsorship
This work was supported by: Molecular bases of disease dissemination in lymphoid malignancies to optimize curative therapeutic strategies (51000 No.21198), Associazione Italiana per la Ricerca sul Cancro Foundation Milan, Italy; PNRR-MAD-2022-12375673 (Next Generation EU, M6/C2_CALL 2022), Italian MoH, Rome, Italy; the AGING Project (Department of Excellence), DIMET, Università del Piemonte Orientale, Novara, Italy.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
The study was approved by the Ethical Committee of the Ospedale Maggiore della Carità di Novara associated with the Università del Piemonte Orientale (study number CE 120/19).
Consent for publication
Not applicable.
Copyright
© The Author(s) 2024.
 Journal of Cancer Metastasis and Treatment2024年1期
Journal of Cancer Metastasis and Treatment2024年1期
- Journal of Cancer Metastasis and Treatment的其它文章
- Feature interview with Dr.William C.CHO -“Clarivate 2023 Highly Cited Researcher”
- Fast-tracking drug development with biomarkers and companion diagnostics
- Mechanical force-mediated interactions between cancer cells and fibroblasts and their role in the progression of hepatocellular carcinoma
- Leveraging metformin to combat hepatocellular carcinoma: its therapeutic promise against hepatitis viral infections
- Regulation and function of the RSK family in colorectal cancer