
Symptoms and symptom clusters in patients with hepatocellular carcinoma and commonly used instruments: An integrated review
2024-02-27 11:33ThitipornPthomjruwtYowrtMtchimJneArmer
Thitiporn Pthomjruwt ,Yowrt Mtchim ,* ,Jne M.Armer
a Research Unit in Palliative Care for Adults and Older Adults,Faculty of Nursing,Thammasat University,Pathum Thani,Thailand
b MU Sinclair School of Nursing,University of Missouri,Columbia,USA
Keywords:
ABSTRACT Objective:This study aimed to synthesize the available knowledge of identifying hepatocellular carcinoma (HCC) symptoms and symptom clusters in patients with HCC and instruments used for these assessments to maximize symptom management.Methods:Whittemore and Knafl’s integrative review method was employed to guide a systematic search for literature in five databases (PubMed,ScienceDirect,Scopus,CINAHL,and ThaiJO).The retrieved articles were limited to those which were peer-reviewed,published between 2005 and 2022,and had English abstracts.All of identified studies were screened,extracted,and analyzed independently by two researchers.Result:Fourteen articles were included in this review.They were grouped into three themes:symptoms,symptom assessment,and symptom clusters of HCC patients.Fatigue,lack of energy,stomach or abdominal pain/distension,loss of appetite,change in taste,sleep disturbance,distress,and sadness are the most prevalent symptoms reported in HCC patients.The different concurrent symptoms are related to the stage and treatment.Five types of symptom assessment instruments were commonly used (symptoms-specific HCC,general cancer symptom,measuring non-symptom constructs,measuring specific symptoms,such as fatigue,sleep disturbance,anxiety,and depression,and symptom assessment with clinical examination).Furthermore,the symptom clusters in HCC patients were classified into five categories: 1) pain-related symptoms,2) gastrointestinal symptoms,3) neuropsychological symptom clusters and sensory symptoms,4) liver dysfunction-related symptom clusters,and 5) others (including sickness symptom clusters,fatigue clusters,location pain symptoms,and asymptomatic or symptomatic).Conclusion:The findings of this review add to the body of knowledge on symptoms,symptom assessment,and symptom clusters in patients with HCC.Despite a variety of instruments being available,none covers all symptoms experienced by HCC patients.It is recommended that future studies should include larger and more homogenous samples to evaluate assessment instruments more precisely,avoid ambiguity in classifying symptoms into symptom clusters,and increase the effectiveness of symptom management.
What is known?
· Cancer patients experience multiple symptoms involving changes in their physical,psychological,sociocultural,behavioral,functional,sensory,and cognitive processes.
· These symptoms are related to the stages and treatment of the disease and the subsequent response.Symptom clusters are two or more concurrent symptoms that are related to each other.
What is new?
· This review provided insights into symptoms,symptom clusters,and symptom assessment instruments in patients with hepatocellular carcinoma (HCC).
· The findings summarized the characteristics of symptom assessment scales,symptom prevalence,and symptom clusters in HCC patients.
1.Introduction
Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer (PLC),accounting for 75%-85% of all liver cancer cases [1],and it is the third leading cause of cancer-related mortality worldwide [2,3].With more than 840,000 new cases detected each year,it is the sixth most common cancer across the globe [3].Increases in HCC patients’ survival rates significantly depend on early screening to detect the disease and receive appropriate treatment [4].Concurrent symptoms of HCC differ from those of other cancers,as often no physical dysfunctions and symptoms occur in the early stages,and no disease-specific symptoms appear until the condition becomes severe and advanced.Most patients with HCC are diagnosed at a late stage,resulting in short survival due to poor prognoses and limited treatment options [5].Treatment guidelines for HCC are often based on the Barcelona Clinic Liver Cancer (BCLC) staging system [3,6].Surgical cure is appropriate in very early and early stages (BCLC Stage 0 and A),when it is most effective and reduces disease recurrence.Chemoembolization and targeted therapy are appropriate for intermediate stage (BCLC Stage B) with preserved liver function and advanced stage (BCLC Stage C) in terms of extending survival [7].On the other hand,advanced-stage HCC patients develop multiple complications from progressing disease and the side effects of its treatment,resulting in a range of symptoms and signs [8,9].As time progresses to the end-stage (BCLC Stage D),physical function and multiple organs deteriorate rapidly and fail.Patients have more concurrent symptoms,leading to their severe suffering and burden during the end of their lives[10,11].
In HCC,multiple co-occurring symptoms are caused by the disease,treatment,and complications associated with clinical features that impact the patient’s functional status,quality of life,and disease progression [3].Symptom clusters,which are classified as two or more concurrent symptoms that are related to each other,require efficient symptom management [12].Managing one symptom may not lead to an improvement in other symptoms;therefore,all symptoms in the symptom cluster should be considered,not just a single symptom.
Understanding the evidence regarding symptom assessment,symptom prevalence,and symptom clusters in HCC patients will allow nurses to assess patients with concurrent symptoms and identified clusters and to develop appropriate symptom management.Although the literature has reported symptom prevalence and symptom clusters in HCC patients,limitations exist in summarizing this important topic and comparing various symptom assessment instruments.
Therefore,this study used the integrative literature review method to synthesize the literature examining instruments used to assess symptoms and symptom clusters in HCC patients and report on these symptoms and symptom clusters.It aimed to systematically identify HCC symptoms and symptom clusters and instruments used for these assessments,in order to maximize symptom management.
2.Methods
This literature review was conducted using Whittemore and Knafl’s (2005) framework for integrative reviews [13].The methodological approach comprised five consecutive stages:1) problem identification,2)systematic literature search,3)data evaluation,4)data analysis,and 5) presentation of the fin dings.
2.1.Problem identification
This review guide presented two questions as follow.1) What symptom assessment instruments have been used in HCC patients?And 2) What symptom prevalence and symptom clusters are reported among HCC patients?
2.2.Literature search
A comprehensive search of five relevant databases (PubMed,ScienceDirect,Scopus,CINAHL,and ThaiJO) was conducted in August 2023.The inclusion criteria of the studies were as follows:1) original quantitative and qualitative literature published between January 2005 and December 2022,and 2) Literature with English abstracts published in peer-reviewed journals,including selected Chinese and Korean articles with English abstracts.We searched articles using the PICo framework [14]: P (Population or Problem)=what characteristics of symptom assessment,symptom prevalence,and symptom clusters were reported in patients with HCC or liver cancer;I (Interest)=symptom experience;and Co(Context)=global setting regarding the preceding issues.The central terms for combined searches included “symptom assessment” AND “symptom prevalence” AND “symptom cluster” AND“hepatocellular carcinoma” OR “liver cancer.” Studies were excluded if they analyzed mixed cancer types,did not explicitly report subjects of interest,were of insufficient quality,or were reviews,editorials,or comments.The initial search revealed 616 articles,of which 330 duplicates were excluded.An additional 159 articles were excluded based on their titles and abstracts.Further screening excluded those that analyzed mixed cancer types(n=58),lacked the terms of assessment symptoms,symptom prevalence,and symptom cluster(n=45),or for which full text was unavailable(n=10).After selecting studies by reviewing titles and abstracts,full texts were retrieved and read in full to include suitable studies.Fourteen studies that met the inclusion criteria were included in the analysis(Fig.1).No articles were excluded after the quality appraisal.
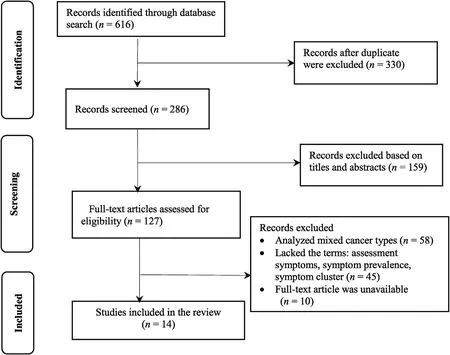
Fig.1. Flowchart of the study selection in this review.
2.3.Data evaluation
A review rubric for the critical appraisal of the literature was introduced to assess the methodological rigor.The Joanna Briggs Institute(JBI)critical appraisal tools[15]were employed to evaluate the methodological quality of the articles.The total number of rating criteria assigned by the papers was calculated using the JBI critical appraisal tools for a systematic review.A quality rating of 70%or higher indicated high and very high quality.Two researchers (T.Pathomjaruwat &Y.Matchim) independently assessed the articles and discussed the quality scores using the JBI critical appraisal tools.Any discrepancies in scores were decided by the third researcher(J.M.Armer).
2.4.Data analysis
Considering the heterogeneity of the studies,thematic analysis was chosen for the integrative review[13].Data reduction,display,comparison,conclusion drawing,and verification were performed.The findings were structured into subsections in a data matrix template based on research and location and the study's aims,design,methods,sample,key findings,and quality score.Data were extracted and coded according to the research questions addressed in this review and were sorted into a manageable framework to integrate the results for all included studies.The data were assembled around corresponding subgroups based on the research topic.Similar data were compared and grouped until the final themes were refined.
3.Results
3.1.Study characteristics
The included studies were from the United States(n=4),China(n=6),Korea (n=2),Thailand (n=1),and Uganda (n=1).Categorization of the key findings permitted the identification of two general themes: symptom and symptom clusters of HCC patients.The studies focused on symptom prevalence and severity.Prevalent physical symptoms included fatigue,lack of energy,stomach pain/distension,loss of appetite,changes in taste,and sleep disturbance.Most prevalent psychological symptoms were distress and sadness.More severe symptoms included fatigue,loss of energy,and sadness.Symptoms involved the disease stage,treatment,and impact on quality of life.Pain-appetite,fatiguerelated symptoms,gastrointestinal symptoms,neuropsychological symptoms,liver dysfunction,itching,constipation,and sickness symptoms cluster were the occurring symptom clusters.The data collection methods used in the included studies were questionnaires,interviews,and clinical examinations (Table 1).
3.2.Identified themes
The studies were grouped into “symptoms,” “symptom assessment,” and “symptom clusters.” The subthemes identified from“symptoms in HCC patients” were symptom prevalence and severity in patients during each stage of HCC and patients who underwent several treatments.The subthemes identified from the“symptom assessment”were the characteristics of the instruments and validation.The subthemes identified from“symptom clusters”were the classification methods and components of the symptom clusters.
3.2.1.Symptoms in HCC patients
Ten studies focused on symptom prevalence and symptom severity primarily occurring in HCC patients [8,9,11,16-20,23,25].Three studies focused on the specific symptoms which occurred,including sleep disturbance [24],fatigue,depression [22,24],and pain[21,22].Two studies focused on symptoms related to quality of life [22,23].One study focused on symptoms related to adverse drug-related events [26].Patients with different stages and treatments had different concurrent symptoms.Five studies explored the symptom prevalence in patients with early to advanced stage HCC receiving multiple active HCC treatments[9,16-19].The most prevalent symptoms included fatigue,lack of energy,stomach or abdominal pain/distension,loss of appetite,change in taste,sleep disturbance,distress,and sadness [9,16-19].One study explored the symptom prevalence in patients with end-stage liver disease who had short-term mortality.Pain,lack of energy,drowsiness,difficulty concentrating,irritability,itching,dry mouth,lack of appetite,nausea,problems with sexual interest or activity,swelling of arms or legs,bloating,and sadness occurred at a rate of >60%in these patients [11].
Two studies examined symptom prevalence in patients receiving transarterial chemoembolization(TACE).Fatigue,distress,sleep disturbance,sadness,lack of appetite,weight loss,and pain (abdominal,back,and shoulder) occurred at a rate of 80% [9,21].One study examined symptom prevalence in patients receiving molecular-targeted therapy with lenvatinib.Hypertension,proteinuria,diarrhea,hepatic encephalopathy,anorexia,fatigue,hand-foot syndrome,hoarseness,and weight loss were adverse drug events,occurring at a rate of >20%[26].

Two studies focused on the characteristics of pain symptoms [21,23].Pain symptoms were described related to site,such as abdominal/stomach/belly pain [23],back pain,upper-back pain,lower-back pain,shoulder pain [21,23],pain in the liver area,diaphragm pinching,pain in the spleen area,pain from itching,breathing pain,and pain at the chemoembolization incision site [23].
Most studies reporting fatigue,lack of energy,sadness,loss of appetite,pain,and sleep disturbance reported high scores in severity of symptoms in HCC patients in all stages receiving multiple treatments [8,9,11,16-20,23,25].One study examined symptoms and health-related quality of life (HRQoL) [22].Pain and fatigue had significantly negative associations with HRQoL.Pain and fatigue were negatively correlated and changed in the Emotional Well-Being (EWB) [22].
3.2.2.Symptom assessment instruments in HCC patients
Fourteen symptom assessment instruments were commonly used in HCC patients.These instruments were classified based on the aim to measure,is shown in Appendix A.
3.2.2.1.Symptom-specific assessment instruments.Specific HCC symptom assessment instruments measured two characteristic features were amounts of symptoms and their severity.These features initially aimed to measure all symptoms,both physical and psychological,of HCC or hepatobiliary cancer such as HCC symptom checklist consisting of 20-21 symptom items,respectively[16,17].These instruments were validated through internal consistency by the Cronbach’s α coefficient symptom checklist,20 items=0.901[17]and 21 items=0.892[16].6-Items HCC symptom checklist[9]or the 6-items symptom checklist specifically for PLC [19],the content validity index (CVI)=0.911 [9].
3.2.2.2.General cancer symptom assessment instruments.General symptom assessment instruments for cancer patients aimed at measuring the amount and severity of most cancer patients’ symptoms,both related and unrelated to treatment.For example,1) The M.D.Anderson Symptom Inventory (MDASI) (13 items related to cancer) was the most frequently used in these patients[9,18-20].However,symptoms associated with HCC were absent.The MDASI was used with the 6-item HCC symptom checklist [9,19].Internal consistency for MDASI was validated through Cronbach's α coefficient for English version(0.82)[18]and Chinese version(0.92 and 0.98)[18,19].Furthermore,validation by construct validity was checked by factor analysis and concurrent validity[18].Reliability was checked by test-retest reliability(0.97)[18].Two other tools are: 2) The Edmonton Symptom Assessment Scale (ESAS) (10 items) [21];and 3) the Memorial Symptom Assessment Scale (MSAS) (32 items) [11].These were validated through Cronbach’s α (0.89 for ESAS [21] and 0.93 for MSAS [11],respectively).MSAS differed from MDASI and ESAS as it aimed to measure the symptom frequency,symptom severity,and additional distress-related symptoms [11].
3.2.2.3.Instruments measuring non-symptom constructs.Certain instruments have a primary aim other than to assess symptoms.Rather,these were used to assess variables related to concepts or theories,such as quality of life,function status,and health-related quality of life.These instruments included the Functional Assessment of Cancer Therapy-Hepatobiliary (FACTHep) [16,22,23] and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Hepatocellular-18 (EORTC QLQ-HCC18) [23].FACT-Hep had a Cronbach’s α coefficient of 0.935[10]and >0.7[22].The validity of EORTC QLQHCC18 was not reported in the included study [23].
3.2.2.4.Instruments measuring specific symptoms.Some instruments assessed specific symptoms,such as symptom interference [18],the Brief Fatigue Inventory (BFI) [24],the Sleep Quality Index (SQI) [24],and the Hospital Anxiety and Depression Scale (HADS)[24],the most specific symptoms reported in HCC patients.These instruments had reliability through Cronbach’s α coefficient (0.89 for symptom interference [18],091 for BFI,0.83 for SQI,0.96 for HADS-depression [24],and >0.80 for HADS [16,24],respectively).
3.2.2.5.Symptom assessment and clinical examination.These instruments for symptom assessment with clinical examination consist of two parts:symptom assessment by patients’reports and signs as clinical examination reported by physicians who underwent standardized training.These instruments aimed to assess both symptoms and signs.However,these questionnaires were not validated by internal consistency [25,26].These instruments were commonly used in the assessment of complex cases based on the expertise in symptom assessment skills,for example,the occurrence of HCC symptoms in AIDs patients[25]or the complications of HCC patient outcomes after chemotherapy or targeted therapy [26].
3.3.Symptom clusters in HCC patients
Six studies used factor analysis to classify symptom clusters [9,16-19,21] and only one study used cluster analysis[22].
In this review,the number of symptom clusters was extracted using statistical analysis,ranging from two to four symptom clusters,which are shown in Table 1 and Appendix B.We observed five major symptom clusters as follow.Symptom clusters were classified depending on the pain symptoms at each location.Moreover,symptoms were classified as asymptomatic or symptomatic,depending on the symptom prevalence.
1)Pain-related symptom clustersincluded pain,lack of appetite[16-18],change in taste,nausea [16,17],stomach pain/discomfort [17,21],abdominal distension [21],feeling ill [11],fatigue,sadness,distress,drowsiness,sleep disturbance,dry mouth[18],and fever[16].Pain-related symptoms before TACE were caused by visceral involvement originating from the primary or metastatic lesion in the abdomen and resulting in concurrent pain at multiple body sites in the form of abdominal distension,upperback pain,and shoulder pain [9,21].In patients receiving HCC treatment[16-19,21],pain incidence of 45%-81%was reported.Pain was associated with and contributed to many concurrent symptoms.For example,pain,nausea,stomach pain,discomfort,feeling ill,loss of appetite,and change in taste were often associated with pain reports [17].See Appendix B.Due to liver damage after TACE,oxygen-rich blood supply to the tumor and other surrounding tissues was reduced.Furthermore,pain in any tissue,such as abdominal or back pain,may have occurred from the position attained during the procedure or at rest[21].
2)Gastrointestinal-related symptom clustersincluded uppergastrointestinal tract symptoms,such as nausea and vomiting[9,18,19],stomach pain/swelling/cramps [16],dry mouth,poor appetite,pain,fatigue,fever [16],jaundice,diarrhea,and other side effects [17].In the included studies,gastrointestinal symptoms related to the physiological mechanism of nausea and vomiting due to liver dysfunction were most commonly reported in patients with primary or advanced HCC stage.Patients with a treatment history of chemotherapy or TACE may have reported an adverse reaction to chemotherapy drugs which activated the vomiting center in the brain[18].
3)Neuropsychological symptoms or sensation-related symptom clustersThe neuropsychological symptom cluster included sadness and distress [9,19],which were reported both before and after TACE.Difficulty remembering [18,19],shortness of breath[18],sleep disturbance,drowsiness[19],and sensationalrelated symptoms such as numbness were reported in patients receiving multiple HCC treatment [19].
4)Liver dysfunction-related symptom clustersincluded jaundice [9,16,19],itching/pruritus [17-19],constipation [16-19],abdominal distension,diarrhea,poor appetite,and abnormal liver function [19].These cluster were reported after TACE and active HCC treatment.In the included studies,TACE procedures resulted in abnormal liver function due to a damaged liver[9].
5)Other symptom clustersinvolved the following.Sickness symptom clusters included pain,fatigue,sleep disturbance,lack of appetite,dry mouth,abdominal distention,and weight loss,which were reported in HCC patients both receiving and not receiving TACE [9].Fatigue-related symptom clusters included fatigue,lack of energy,sadness[16,17],weight loss,spending all day in bed [17],and back pain [16].Other clusters included asymptomatic,symptomatic[22],and fatigue-related symptom and pain-related symptom clusters [18,22].Particularly,HCC patients experiencing fatigue-and pain-related symptom clusters concurrently reported a greater frequency and severity of symptoms than those who had a single symptom or no symptoms [18].This relationship was described through a pathogenesis of inflammation throughout the HCC disease,coupled with treatment-related (chemotherapy and TACE) elevated cytokine levels (IL-6,IL1-β,tumor necrosis factor (TNF)-α,and interferons (IFN)),which typically induce fatigue,drowsiness,and distress[18].Patients with HCC often experienced a variety of psychological symptoms,including fatigue,sleep disturbance,and depression [24].It has been reported that patients with a high prevalence and severity of sleep disturbance were likelier to be depressed [24].Sleep disturbance has been recognized as one of the early signs of HCC with hepatic encephalopathy.It was a primary diagnosis that could develop into a depressive disorder or other mental disorder[24].Mood and depression are common causes of fatigue,and depression and fatigue in HCC patients may share a common cause that is due to cytokines [22,24].One study described a relationship between fatigue and the release of activated cytokines from the liver or neoplastic tissue [21].Fatigue in HCC patients was found to be associated with elevated serum TNF-α,IL-1,and IL-6 levels [22].
Furthermore,the included qualitative studies classified eight symptom categories: 1) eating behavior/weight change,2) extremities,3) fatigue/strength,4) gastrointestinal,5) pain,6) sensory,7) skin,and 8) other.Four categories were different from the previously explained clusters in quantitative studies seen in Table 1: 1) symptoms in extremities (arms,legs),including neuropathy,numbness,tingling,and swollen ankles,arms,and legs;2)fatigue and strength,including fatigue,lack of energy,and loss of muscle strength;3) sensory,including change in sense of smell;and 4) other symptoms,including difficulty concentrating,dizziness,vertigo,dry mouth,shortness of breath,dry eyes,fainting,fever,hallucination,and urogenital problems [8].
4.Discussion
This review synthesized existing knowledge to provide insights into symptoms and symptom clusters in HCC patients.Despite general similarities in some symptoms,patients reported different symptoms related to characteristic symptom items,disease stage,and cancer-related treatment due to different symptom assessment instruments and their symptom items.
Most of the included studies examined the prevalence and severity of symptoms and the symptom classifications,which allowed for the assumption that individuals belonged to underlying subgroups.Most patients with HCC were likely to have multiple concurrent symptoms.The early-stage patients tended to report fewer accounts and less-severe symptoms.In addition to fatigue,lack of energy,stomach pain/discomfort,sleep disturbance,loss of appetite,and sadness were the most common symptoms occurring in the intermediate and advanced stages[9,16,17].These symptom relationships were explained through pain-related symptom clusters[18],fatigue-related symptom clusters[16],and pain-appetiterelated symptom clusters[16,17].Sadness,anxiety,and depression were psychological symptoms found in the early stage of the disease and that,over time,would lead to physical problems(fatigue,loss of energy)and worsening of disease progression[18,24].In the end stage of the disease,patients most often suffered from multiple and severe symptoms.However,some patients at this stage did not self-report symptoms due to cognitive function impairment,such as difficulty concentrating and feeling irritable due to hepatic encephalopathy [11].
Among HCC patients who underwent TACE,most reported a significant increase in pain [9,21],fatigue,sleep disturbance,jaundice,fever [9],and itching [23] due to this procedure,which was meant to retain the chemotherapeutic and embolization agents within the tumor,and the damage it caused the normal liver parenchymal tissue surrounding the tumor[9,21].These symptoms occur within 24 h to over a week after TACE[23].In addition,some chemotherapy drugs entered the gastric blood vessels,inducing nausea and vomiting [9].Hypertension,diarrhea,hepatic encephalopathy,anorexia,fatigue,and hand-foot syndrome were symptom-related adverse events in patients with HCC associated with molecular-targeted therapy,with differences based on related types of drugs.These symptoms sometimes compromised the response to treatment and led to treatment termination [26].Patients and healthcare providers should prioritize assessment of the patients’ concurrent symptoms and managing these symptoms appropriately.
Most of the included studies examined symptom prevalence and severity using symptom assessment instruments to collect data.The results revealed various instruments were used for different aims.General symptom assessment instruments for cancer patients consist of the patient’s self-report symptom assessment,including symptom amounts,frequency,severity [9,18-20],and distress [11].Self-assessment of symptoms helps the patient understand and manage their symptoms.Conversely,patients with severe symptoms or cognitive impairment due to hepatic encephalopathy had difficulty reporting the symptom experience.Assessing the patient’s condition requires the use of appropriate symptom assessment tools by caregivers and nurses.This helps to identify the need for prompt management of symptoms that interfere with QOL and cause the patient’s discomfort and distress.On the other hand,the results showed that some symptoms were more frequent and severe according to the caregiver’s assessment [20].Some instruments like the MDASI were standard[9,18-20].It had high validity and is used with cancer patients.However,symptom checklists specific to HCC could be used to assess HCC patient's specific symptoms.It was also noted that there were tools that were used together.Quality of life-related symptoms and treatment could be assessed by using the FACT-Hep [16,22,23] or the EORT QLQ-HCC18 [23].Nurses and healthcare providers working in this area should select appropriate instruments based on the aim of use and their quality performance measurement.
Different symptom clusters were investigated using factor and cluster analyses based on symptom prevalence.The main influencing factors for the symptom cluster classification were the differences among the measuring instrument,the disease stage,and the treatment.Cao et al.(2013) [9] found a difference in symptom clusters between patients before and after TACE.The two symptom clusters were psychological symptom and sickness symptom clusters.Patients presenting with symptom-related liver damage after TACE experienced an increase in two symptom clusters:the uppergastrointestinal symptom cluster and the liver dysfunction symptom cluster,which includes jaundice and itching [9].The various symptom assessment instruments were major factors influencing symptom cluster classification.The results revealed that the included studies used a combination of two instruments (MDASI-13 symptom items and additional symptoms for PLC/HCC-6 symptom items) to collect symptom data [9,19].The results also showed three general symptom clusters for cancer patients,including pain-related symptom or sickness symptom clusters,gastrointestinal-related symptom clusters,neuropsychological symptom clusters,and a specific symptom cluster related to liver dysfunction.In contrast,using only the MDASI-13 symptom items,the classified symptom clusters had the same three general symptom clusters,with no liver dysfunction symptom cluster[18].Furthermore,the use of different instruments resulted in differing symptom prevalence,which affected the symptom cluster classification in Appendix B.Instruments are a key factor that can help complete symptom data,as they ensure that the data are suitable for statistical analysis.
5.Strengths and limitations
This review has certain strengths.First,this is one of the few studies to synthesize the available knowledge about symptoms,symptom clusters,and symptom assessment instruments among patients with HCC,identifying the most common symptoms and symptom clusters and comparing symptom assessment instruments and validation.Second,the Whittemore and Knafl’s integrative reviews method was adopted to reduce potential bias.Some limitations should be acknowledged in this review.First,database searches were limited to PubMed,ScienceDirect,Scopus,CINAHL,and ThaiJO.Second,only peer-reviewed papers with abstracts published in English were included,which may have impacted the generalization of the results.
6.Conclusion
This review summarized symptom prevalence,concurrent symptoms,and symptom clusters among HCC patients.Concurrent symptoms with different characteristics related to the stage of the disease and associated treatment were noted in these patients.An appropriate symptom assessment instrument is important to understand the prevalence and severity of symptoms and symptom distress.This assessment is the most important influencing factor in the multiple symptoms management.Understanding the relationships between and among concurrent symptoms in the same cluster enhances strategies for symptom management.
Future studies are needed to examine how concurrent symptom characteristics and associations are amenable to guiding symptom management interventions that can contribute to the short-term and long-term quality of life of patients with HCC.
Funding
This study was supported by the Research Unit in Palliative Care for Adults and Older Adults,Faculty of Nursing,Thammasat University,Thailand and Bualuang ASEAN Chair Professor Fund for the project leading to this publication.
Data availability statement
All data used for analysis and discussion in this manuscript can be checked from the reference lists.
CRediT authorship contribution statement
Thitiporn Pathomjaruwat:Conceptualization,Methodology,Validation,Formal analysis,Investigation,Data curation,Writingoriginal draft,Visualization.Yaowarat Matchim:Conceptualization,Validation,Investigation,Writing-review&editing.Jane M.Armer:Writing -review &editing.
Declaration of competing interest
The authors declare that they have no conflict of interest.
Appendices.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.09.009.
 International Journal of Nursing Sciences2024年1期
International Journal of Nursing Sciences2024年1期
- International Journal of Nursing Sciences的其它文章
- Nursing leadership: Key element of professional development☆
- Comparison of the performance of four screening tools for sarcopeni a in patients with chronic liver disease
- Associations among frailty status,hypertension,and fall risk in community-dwelling older adults
- Facilitators and barriers to the implementation of dietary nutrition interventions for community-dwelling older adults with physical frailty and sarcopenia: A qualitative meta-synthesis
- The prevalence and factors associated with sarcopenia in Thai older adults: A systematic review and meta-analysis Phatcharaphon Whaikid,Noppawan Piaseu*
- Air quality self-management in asthmatic patients with COPD: An integrative review for developing nursing interventions to prevent exacerbations