
Comparison of the performance of four screening tools for sarcopeni a in patients with chronic liver disease
2024-02-27 11:33TingYuShanshanLiuJingZhaoYanJiangRongDeng
Ting Yu ,Shanshan Liu ,Jing Zhao ,Yan Jiang ,Rong Deng ,*
a Department of Evidence-based Nursing Center,West China Hospital,Sichuan University/West China School of Nursing,Sichuan University,Chengdu,China
b Department of Nursing,West China Hospital,Sichuan University/West China School of Nursing,Sichuan University,Chengdu,China
c Center of Infectious Diseases,West China Hospital,Sichuan University/West China School of Nursing,Sichuan University,Chengdu,China
Keywords:
ABSTRACT Objectives: Early identification of sarcopenia in patients with chronic liver disease is crucial for patient management and prevention of severe complications.We aimed to assess the effectiveness of Ishii score,Strength,Assistance with Walking,Rise from a Chair,Climb Stairs and Falls (SARC-F),SARC-F and Calf Circumference (SARC-CalF),and Mini Sarcopenia Risk Assessment-7 (MSRA-7) to screen sarcopenia in patients with chronic liver disease.Methods:This prospective study included patients with chronic liver disease in the infectious department of a tertiary hospital in Sichuan,China.Ishii score,SARC-F,SARC-CalF,and MSRA-7 were used to screen for sarcopenia risk.Sarcopenia was diagnosed according to the Asian Myometriosis Working Group (AWGS) 2019,which was used as the gold standard to compare the performance of the four screening tools.We completed clinical registration on the Chinese Clinical Trial Registration website (ChiCTR2100043910).Results:A total of 366 patients with chronic liver disease (22.4% women,mean age 48.96 ± 11.88 years)were evaluated.Based on the AWGS 2019 standard,the prevalence of sarcopenia in patients with chronic liver disease was 17.5%.Among all participants,receiver operating characteristic(ROC)produced an area under the curve (AUC) of 0.82 for Ishii score (sensitivity 85.94%,specificity 78.15%),0.53 for SARC-F (sensitivity 6.25%,specificity 99.34%),0.64 for SARC-CalF (sensitivity 45.31%,specificity 83.11%),and 0.55 for MSRA-7 (sensitivity 87.50%,specificity 22.85%).Based on AUC,decision curve analysis,and calibration curves,we concluded that Ishii score was the most accurate screening tool and was superior to the other tools.Conclusions:Ishii score is more suitable for screening sarcopenia in patients with chronic liver disease than the SARC-F,SARC-CalF,and MSRA-7,based on the AWGS 2019 criteria.Nursing professionals can use Ishii score as a clinical tool to screen for sarcopenia in patients with chronic liver disease,providing an indication cue for the final diagnosis of sarcopenia,improving diagnostic efficiency,and enabling early identification and prevention of complications resulting from sarcopenia.
What is known?
· Sarcopenia is a major public health problem worldwide and a leading cause of adverse outcomes for patients.Early diagnosis of sarcopenia is essential.There are tools available to screen for sarcopenia.
· Patients with chronic liver disease are at a higher risk of developing sarcopenia,which is often ignored.It is crucial to identify and use an effective screening tool that can detect sarcopenia in these patients at an early stage.
What is new?
· We evaluated the efficacy of Ishii score,Strength,Assistance with Walking,Rise from a Chair,Climb Stairs and Falls(SARC-F),SARC-F and Calf Circumference (SARC-CalF),and Mini Sarcopenia Risk Assessment-7 (MSRA-7) to screen for sarcopenia in patients with chronic liver disease based on the Asian Working Group for Sarcopenia (AWGS) 2019,and there were differences in the efficacy of the four tools.
· Compared with other tools,Ishii score showed higher accuracy in screening for sarcopenia in patients with chronic liver disease,and can be easily utilized by nursing staff in clinical settings.
1.Introduction
Sarcopenia is a progressive and generalized skeletal muscle disorder that is associated with increased adverse outcomes,including falls,fractures,frailty,physical disability,and mortality [1-3],and has been officially classified as a disease under a specific code (FB32.Y) in the WHO Eleventh Revision of the International Classification of Diseases (ICD-11).Sarcopenia has been attracting increasing attention from researchers[4].In Asia,the prevalence of sarcopenia in older adults is 2.5%-45.7%,and the incidence increases with age [5].Moreover,the prevalence of sarcopenia is expected to increase by 72.4% between 2016 and 2045 in Europe [6].An early study in the United States found that the direct medical costs associated with the disease were estimated at $18.5 billion [7].Hence,the development of sarcopenia and its associated consequences cannot be overlooked.
In recent years,the impact of sarcopenia on patients with chronic liver disease has received increasing attention.Patients with chronic liver disease have decreased appetite,inadequate protein intake,dyspepsia caused by portal hypertension,and a high metabolic state,which accelerates skeletal muscle consumption [8].At present,sarcopenia is recognized as a risk factor closely related to complications and death,which seriously affects the quality of life of patients with chronic liver disease [9,10].Importantly,sarcopenia has a prevalence of 22%-70% in patients with chronic liver disease [11].Compared with patients without sarcopenia,patients with sarcopenia have increased health care costs while waiting for liver transplantation,resulting in a significant economic burden [8].However,scholars have pointed out that sarcopenia is not easy to detect in the early stage,and patients often seek rehabilitation guidance when severe physical function decline or disability occurs[12,13].It is easily overlooked and has not been applied to routine clinical prognostic assessment,and its evaluation and diagnosis methods are still not uniform [14,15].Nursing staff,who had the most frequent contact with patients,were key to identifying patients with chronic liver disease at high risk for sarcopenia.Therefore,an easy-to-use screening tool could be helpful,thereby enabling nursing staff to identify sarcopenia early,provide possibilities for the early diagnosis and rehabilitation of sarcopenia,and then prevent or delay the progression of sarcopenia,reducing the occurrence of disability and even death [16].
To improve the consistency of sarcopenia screening results,the Asian Working Group for Sarcopenia (AWGS) 2019 proposed criteria for diagnosing and screening and revising the diagnostic process,standard cutoffs,and treatment regimen[17,18].However,accurate identifying sarcopenia early is challenging due to the complex operation involved and the need to use advanced equipment like CT scans,magnetic resonance imaging,dual-energy X-ray bone density meters,and biological electroresistive analyzers,which are not suitable for large-scale screening in clinical practice.Considering the lack of equipment in primary medical institutions,the AWGS 2019 recommended different diagnostic strategies for sarcopenia at different levels of medical institutions,and proposed the concept of“sarcopenia possibility”to provide primary medical institutions with a more practical diagnosis and treatment process and early identification and intervention for people at risk of sarcopenia.The concept of “sarcopenia possibility” emphasizes simple,effective screening prior to gold standard diagnosis using complex instruments and procedures[3].Therefore,identifying an effective,practical,and operable screening method for sarcopenia has become an urgent issue in the management of patients with chronic liver disease.
Many sarcopenia screening tools have been used thus far.Based on a previous literature review,the questionnaires most widely used include Ishii score [19],Strength,Assistance with Walking,Rise from a Chair,Climb Stairs and Falls (SARC-F)[20],SARC-F and Calf Circumference (SARC-CalF) [21],and Mini Sarcopenia Risk Assessment-7 (MSRA-7) [22].Among them,the SARC-F questionnaire is easy to perform and has high specificity,but its sensitivity is low,and it lacks the assessment of muscle mass.Barbosa-Silva et al.combined the SARC-F questionnaire with the calf circumference measurement,which is related to muscle mass,to form the SARCCalF.Although the sensitivity of the SARC-Calf has been improved,the calf circumference test is susceptible to fat mass and edema,and the measurement results are affected [16,23,24].The MSRA-7 showed high sensitivity and low specificity in patients with stomach cancer and was mostly used for older individuals in the community or nursing homes [23].Ishii score derived a sexstratified formula based on three variables: age,grip strength,and calf circumference [19].One study noted that Ishii score was appropriate for hemodialysis patients,with a sensitivity and specificity of 94.8% and 73.6%,respectively [24].Li et al.evaluated the accuracy of Ishii score screening for sarcopenia in older people in Chinese communities,and the results showed that Ishii score has a high screening ability[25],but there were still no research reports on the accuracy and cutoff value of screening for sarcopenia in patients with chronic liver disease.
Therefore,to our knowledge,these criteria have not yet been evaluated in patients with chronic liver disease,and their external validity needs to be further verified.In this study,we compared four sarcopenia screening tools(Ishii score,SARC-F,SARC-Calf,and MSRA-7) using the AWGS 2019 diagnostic criteria as the gold standard to diagnose sarcopenia.Our objective was to evaluate the effectiveness of these four tools for screening sarcopenia in patients with chronic liver disease and to provide nursing staff with the best one for detecting sarcopenia in this population.
2.Patients and methods
2.1.Patients
We recruited patients with chronic liver disease who were admitted to the Infectious Diseases Department of a general hospital in Sichuan Province between September 2020 and December 2021.The prospective study included patients: (a) over 18 years old;(b) had chronic liver disease,which refers to chronic and persistent liver damage that leads to progressive deterioration of liver function for more than six months,including viral hepatitis,alcoholic liver disease,metabolic fatty liver disease,autoimmune liver disease,and cirrhosis (These patients were mainly middleand advanced-stage patients,with Child-Pugh grade B and C with liver function [26,27]);(c) had normal limb movements and were able to cooperate with the researchers;and (d) voluntarily participated in the study with informed consent.Patients were excluded if they had any uncontrolled comorbidities such as uncontrolled diabetes,tuberculosis,AIDS,chronic renal failure,muscle disease,rheumatism,digestive disease,parasitic disease,or active drug abuse.Patients with uncontrolled joint disease and neuropathy were also excluded.
2.2.Measuring tools
2.2.1.Diagnosis of sarcopenia
AWGS 2019: The diagnostic criteria of sarcopenia followed the AWGS 2019 “age-related loss of muscle mass,plus low muscle
strength,and/or low physical performance”,which needed measurements of both muscle quality and quantity and defined people with low muscle mass,low muscle strength,and low physical performance as having severe sarcopenia.Specific measures included muscle mass,grip strength,and walking speed[17,18].In this study,the definite diagnosis of sarcopenia was made according to AWGS 2019 criteria by a clinician,who was blinded to the results of the screening tools.
2.2.2.Screening tools of sarcopenia
Ishii score:It was compiled by Japanese scholar Ishii[19],which used a score derived from a formula based on three variables(age,grip strength,and calf circumference)to estimate the probability of sarcopenia.These three variables are used to derive the sex-specific sarcopenia calculation formula.The higher the scale score is,the higher the sarcopenia risk.In the study population,the recommended cutoff points for sarcopenia diagnosis are a sum score of≥105 in males and ≥120 in females.The score for males is calculated as follows: 0.62 × (age -64) -3.09 × (grip strength -50) -4.64 × (calf circumference -42).The score for females is calculated as follows: 0.8 × (age -64) -5.09 × (grip strength-34) -3.28 × (calf circumference -42).
SARC-F:The SARC-F score was developed by American scholars Malmstrom and Morley in 2013 [20] and included five variables (strength,assistance with walking,rising from a chair,climbing stairs,and falls).The scores range from 0 to 10,with 0 to 2 points for each component (0=suffciiently possible,1=possible,and 2=somehow possible/impossible).A diagnosis of sarcopenia is made for a total score of 4 or higher.The score contains only five questions that are closely related to the functional status of older adults,and no cumbersome measurement is required.
SARC-CalF:The SARC-CalF is a screening method combining the SARC-F questionnaire and calf circumference formed by Brazilian scholar Barbosa-Silva Tequal in 2016[21].In addition to the SARC-F score,the calf circumference score is 0 points for males and females with >34 and >33 cm calf circumference,respectively,and 10 points for males and females with ≤34 and ≤33 cm calf circumference,respectively.The total score ranges from 0 to 20;a sum score ≥11 indicates possible sarcopenia.
MSRA-7: The MSRA-7 questionnaire was designed by Italian scholar Rossi in 2017 [22].It consists of 7 questions that assess various factors related to sarcopenia: age,number of hospitalizations in the past year,physical activity level,number of meals eaten per day,weight loss in the past year,increased dairy consumption,and protein consumption.Each question is scored on a scale of 0 to 5 or 0 to 10,and the total score ranges from 0 to 40.A score of 30 or less indicates the presence of sarcopenia.
2.3.Medical assessment
Disease-related medical information was obtained from routine clinical laboratory measurements in the Department of Clinical Laboratory of West China Hospital,Sichuan University.
The grip strength measurement was conducted using a professional handheld electronic grip device(Addison Electronic Grip,No.TXUT-013) to assess the dominant hand’s grip strength.The test was pre-calibrated,and the patient was familiar with using the grip device.The patient was seated with their lower legs bent to the floor and their knees and hips bent at a 90°angle.The upper arm was pressed against the chest wall,the forearm was in a neutral position,and the wrist was extended 0-30°.The grip strength of both the left and right hands was recorded,and the maximum value of the two measurements was taken,with a precision of 0.1 kg.The cutoff values for sarcopenia diagnosis were <28 kg for males and<18 kg for females.
Limb muscle mass was measured using bioelectrical impedance analysis (Body Composition Analyzer,BIA,In Body 770,Korea)following an 8 h period of fasting.Measurements were taken in the morning after the patient had urinated or defecated.The patient was positioned in a supine position with shoes and socks removed,and devoid of any metallic objects.BIA lead wires were connected to the limbs,and the researchers input the patient’s basic information before starting the measurement,which took approximately 1-2 min to complete.The cutoff values for sarcopenia diagnosis were <7.0 kg/m2for males and <5.7 kg/m2for females.
The physical function test was conducted five times to measure the time it took for the patient to rise from the chair.A stopwatch was used for measurement.During the test,the patient was positioned on a chair with the back against the wall at a height of approximately 40 cm from the ground.The patients were asked to keep their hands on their chest,feet flat on the floor,and avoid leaning back in the chair.They were then instructed to stand up and sit down five times as quickly as possible,while the time taken for each repetition was recorded.The mean time was calculated and adopted.
Walking speed measurement(m/s).In order to measure walking speed,the researchers selected a flat and empty ground and marked the starting point,3 m,9 m,and the endpoint.The patients were instructed to walk forward from the starting point at their usual walking speed.The researchers initiated the timing when a patient reached 3 m and concluded at 9 m,recording the walking time.The cutoff value for diagnosing sarcopenia was 6 m pace<1 m/s.
Calf circumference was measured by taking the maximum calf circumference using an inelastic tape measure.The patient received instructions to stand with their feet apart at shoulder width,ensuring that the center of gravity was evenly distributed on the foot and the body was relaxed.The tester used an inelastic tape measure to measure the circumference of the patient’s right calf,ensuring a snug fit without any gaps.
2.4.Data collection
To ensure that the data collected is valid and free from bias,the research team followed strict and standardized methods for data collection.We provided training to all the nurses who participated in the study to improve the accuracy of the data collected.At each participating site,data was collected by an assigned trained nurse who met specific criteria (registered nurse with at least 3 years of working experience and more than 1 year of experience in the relevant department).Patients’ socio-demographic information was collected using a self-designed questionnaire,which included details such as gender,age,profession,education level,smoking,and alcohol consumption.The smoking index was calculated by multiplying the number of cigarettes smoked per day by the number of years of smoking:Level 1 indicated never smoked or had quit;Level 2,less than 400;and Level 3,at least 400.Different levels of alcohol consumption were identified based on the average daily intake: Level 1 indicated never drunk or abstained from alcohol;Level 2,<25 g/day;Level 3,25-59 g/day;Level 4,≥60 g/day.Subsequently,nurses and researchers reviewed and signed off on the collected data.The entire survey and measurement process was completed in approximately 30 min,and all participants received small gifts as compensation for their time and effort.
2.5.Statistical analyses
The statistical methods employed in this study were guided by biostatisticians from West China Hospital of Sichuan University.Statistical analyses were conducted using SPSS 26.0 and MedCalc 19.0.4.Continuous variables were presented as mean values and standard deviations (SD),while nominal variables were described in terms of frequencies or percentages.The differences were assessed using Student’s t-tests or Pearson’s χ2test.
The receiver operating characteristic(ROC) curve was analyzed using AWGS 2019 as a reference to determine whether patients had sarcopenia based on the criteria for sarcopenia provided by the tools mentioned above.For each tool,the following conditions were used to judge if a patient had sarcopenia.Ishii: male ≥105 points and female ≥120 points;SARC-F:≥4 points;SARC-CalF: ≥11 points;MSRA-7:≤30 points.The application of each tool has been described in detail previously,resulting in a categorical variable as the final result.The predictive accuracy of the tools was evaluated using the area under the curve (AUC) and calibration curve.The clinical effectiveness of the tool was further confirmed using the decision curve analysis (DCA).Additionally,the sensitivity,specificity,positive predictive value (PPV),negative predictive value(NPV),and 95%confidence interval(CI)of each screening tool were compared.The DeLong test was used for pairwise comparison of the area under the ROC.The optimal cutoff value for each screening tool was determined using the Youden index.Differences were considered significant at P <0.1 for the ROC curve analysis and P <0.05 for the other analyses.
2.6.Ethical consideration
This study was approved by the ethics committee of West China Hospital,Sichuan University [No.2019 (803)].The researcher adhered to the following ethical principles throughout the study:respect for autonomy,beneficence,nonmaleficence,and justice throughout the study.Participants received information letters with instructions on the study’s aims,objectives,and potential risks.Their voluntary written consent was obtained before data collection.Participants were assured that their participation was voluntary and that they had a right to withdraw at any time.We completed clinical registration on the Chinese Clinical Trial Registration website (ChiCTR2100043910).
3.Results
3.1.General characteristics of patients
A total of 366 patients were eventually enrolled in our study(82 females,22.4%;284 males,77.6%),and the mean age was 48.96(SD 11.88).The majority of the patients were infected with hepatitis B virus (HBV) (293/366,80.1%),4.6% (17/366) of the patients were affected by alcohol-related cirrhosis,and 4.4% (16/366) were affected by immunity-related cirrhosis.The remaining causes included but were not limited to hepatitis C virus (HCV) or drugrelated.The main patient characteristics are presented in Table 1.

Table 1 Patients’ characteristics (n=366).
According to AWGS 2019,17.5% (64/366) of patients had sarcopenia,while 82.5% (302/366) did not.The results of the four screening tools according to AWGS 2019 are shown in Table 2.
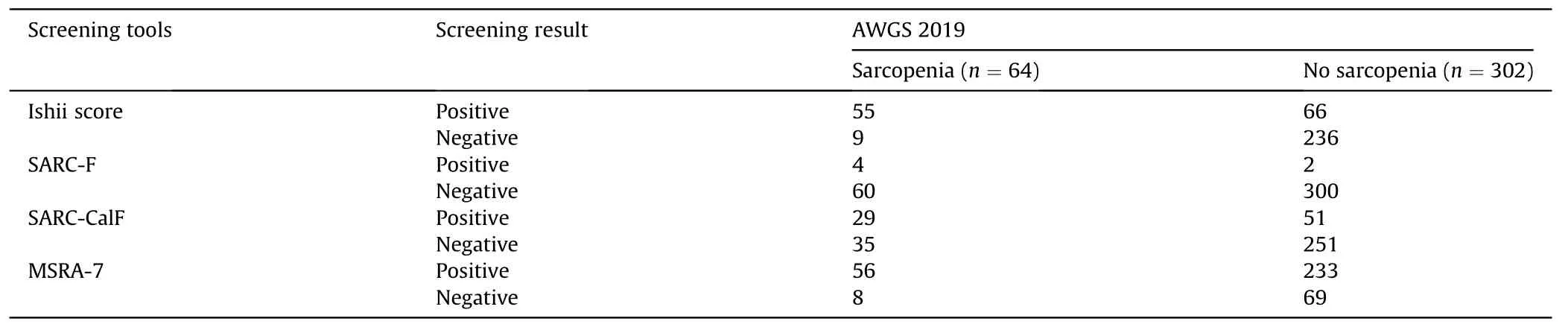
Table 2 Results of four screening tools for sarcopenia in patients with chronic liver disease,using the AWGS 2019 as gold standard.
3.2.Effectiveness of sarcopenia risk screening tools based on the AWGS 2019
To compare the performance of different sarcopenia screening tools,we used the AWGS 2019 as the standard for analysis.In terms of screening tools,the MSRA-7 had the highest sensitivity(87.50%)and the lowest specificity(22.85%).On the other hand,the SARC-F had the lowest sensitivity (6.25%) but the highest specificity (99.34%).The SARC-CalF showed a sensitivity of 45.31% and a specificity of 83.11%.Additionally,Ishii score was found to be effective in predicting sarcopenia risk in patients with chronic liver disease,with an AUC of 0.82 and a Youden Index of 0.64 (Table 3,Fig.1).By observing the calibration curve,the observed result of Ishii score was highly consistent with the predicted results(Fig.2).In addition,DCA showed that Ishii score was best effective to screen for sarcopenia in patients with chronic liver disease (Fig.3).
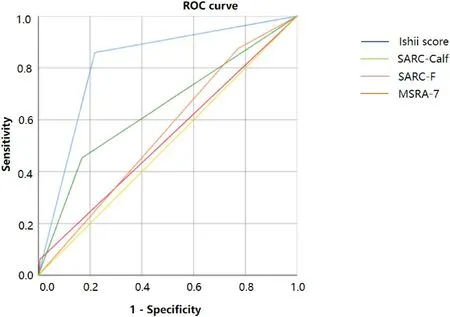
Fig.1. ROC curves analysis for the screening tools for the prediction of sarcopenia risk with the AWGS 2019 as a criterion.Diagonal segments are produced by sites.
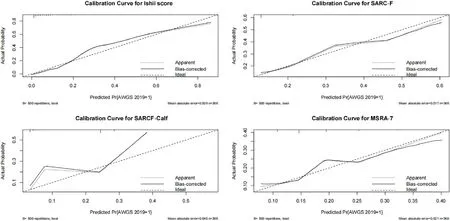
Fig.2.Calibration curves analysis for the screening tools to predict the risk of sarcopenia.
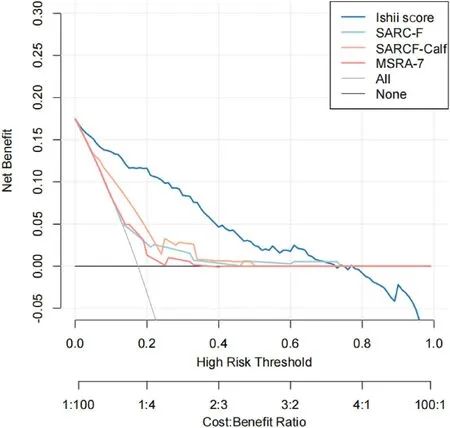
Fig.3. Decision curves analysis for the screening tools to predict the risk of sarcopenia.Comparison of the performance of 4 screening tools for sarcopenia in patients with chronic liver disease.

Table 3 Diagnostic value of the four sarcopenia screening tools,using the AWGS 2019 as gold tandard.
3.3.Comparison of the area under the ROC curve of different sarcopenia screening tools
We observed a statistically significant disagreement between Ishii score and MSRA-7(95%CI 0.21 to 0.34,P<0.001),SARC-F(95%CI 0.23 to 0.35,P<0.001),and SARC-CalF (95% CI 0.11 to 0.25,P<0.001).Comparison of the area under the ROC curve of different sarcopenia screening tools is shown in Table 4.
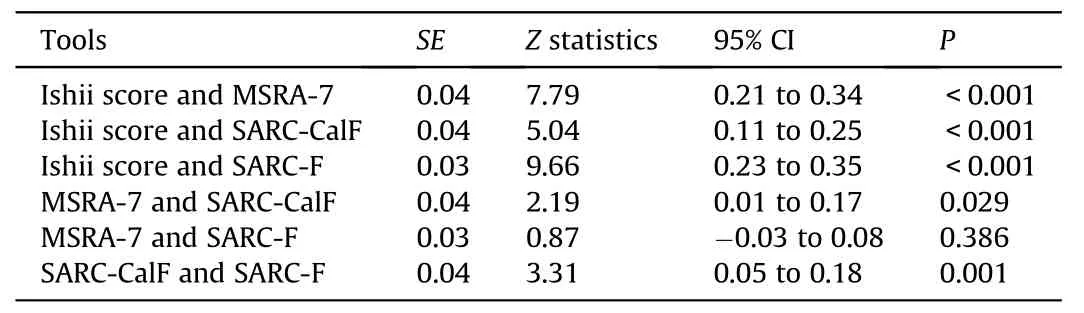
Table 4 Pairwise comparison on ROC curves of different sarcopenia screening tools.
4.Discussions
Using the AWGS 2019 criteria,we found that 17.5% of patients with chronic liver disease had sarcopenia.This prevalence rate is slightly lower than what has been reported in previous studies,possibly due to variations in the populations studied and the screening tools used,as well as the improved awareness of patients regarding their health [4].
International organizations have proposed diagnostic criteria for sarcopenia,such as the European Working Group on Sarcopenia in Older People (EWGSOP) and the AWGS,and different criteria have different focuses[17,28].Because the gold standard diagnostic standard requires specialized equipment and personnel,its wide application is limited [29,30].It is pertinent to conduct screenings for sarcopenia and its potential manifestation in order to accurately diagnose patients who are at risk.This approach serves two purposes:first,it helps to raise awareness about sarcopenia and reduce its incidence;second,it helps to avoid or minimize the expenses associated with expensive diagnostic procedures,thereby saving medical costs.In recent years,several screening tools,such as Ishii score and SARC-F,have been developed and validated for sarcopenia screening.These tools offer advantages such as time and cost efficiency.However,it is important to note that these tools vary in terms of accuracy and duration of measurement[31].Furthermore,their efficacy in patients with chronic liver disease remains unknown.
Our study compared different screening tools for sarcopenia in patients with chronic liver disease using the AWGS 2019 criteria.We found that Ishii score had the highest predictive value compared to the SARC-F,SARC-CalF,and MSRA-7 tools.Ishii score had a statistically superior sensitivity (85.94%) and specificity (78.15%),with the best AUC (0.82) and Youden index (0.64).Therefore,we recommend using Ishii score as the preferred screening tool for sarcopenia in patients with chronic liver disease.This is consistent with the views of earlier scholars that Ishii score provided a more objective risk assessment of the probability of sarcopenia compared to other tools [31,32].The advantage of Ishii score is that it directly assesses calf circumference and muscle mass,both of which are objective and important indicators of sarcopenia [33,34].The EWGSOP recommends screening patients for sarcopenia using Ishii score [33].Additionally,Ishii score was developed based on Asian populations[35],which aligns with our study population and may yield more accurate results.
In this study,the SARC-CalF showed better performance in screening patients with chronic liver disease for sarcopenia thanthe SARC-F,with a low sensitivity of 45.31%and a high specificity of 83.11%.
SARC-F was a highly recommended screening tool for sarcopenia,although it has been criticized for its low to moderate sensitivity [32],which aligns with the findings of our study.This limitation makes it unsuitable for general screening but suitable for evaluating severe cases,limiting its widespread use [3,36].However,evidence suggests that the diagnostic performance of SARC-F can be improved by incorporating additional variables,such as calf circumference [37,38].One study demonstrated that SARC-CalF could enhance the sensitivity of SARC-F while maintaining its original specificity,either by adding age and BMI or by optimizing the low sensitivity.The results also indicated increased sensitivity [38].Nevertheless,further studies are required to validate its external effectiveness.
In our study,we found that the MSRA-7 had a different performance compared to the SARC-F in screening patients with chronic liver disease for sarcopenia.The MSRA-7 showed high sensitivity (87.50%) and low specificity (22.85%),with an overall diagnostic performance(AUC=0.552)that was slightly better than the SARC-F (AUC=0.528),although the difference was not statistically significant.These findings were consistent with previous studies conducted on hospitalized older individuals [39,40].The advantage of the MSRA-7 over the SARC-F lay in its ability to assess risk factors beyond sarcopenia,such as regular eating habits and adequate protein intake for muscle tissue maintenance.Additionally,the MSRA-7 took into account the negative effects of weight loss and frequent hospitalizations [41].A 5.5-year follow-up study on the predictive role of the MSRA-7 in screening for sarcopenia in older adults in the community further supported its high sensitivity and low specificity,indicating that the MSRA-7 was suitable for general screening purposes and should not be used exclusively for assessing high-risk patients [29].
This study has some limitations.The first is that the sample size is relatively small,especially for subgroup analysis,and a larger cohort is needed to confirm the outcomes.Second,the study population consisted of patients with chronic liver disease in the hospital,and the findings may not be applicable to screening other adults in the community.
5.Conclusions
This study was conducted to compare the performance of four screening tools (Ishii score,SARC-F,SARC-CalF,MSRA-7) for sarcopenia screening in patients with chronic liver disease,based on the AWGS 2019 diagnostic gold standard.In our study,the prevalence of sarcopenia in patients with chronic liver disease was 17.5%.Among various screening tools for sarcopenia,Ishii score proved to be the most efficient tool for nursing staff to assess the risk of sarcopenia in patients with chronic liver disease,as it only required age,calf circumference,and grip strength for screening.Larger studies should be conducted to validate these results.Furthermore,future studies can focus on enhancing the accuracy of sarcopenia screening by refining the existing scoring formula or developing a more precise sarcopenia risk prediction model to enhance muscle health management in patients with chronic liver disease.
CRediT authorship contribution statement
Ting Yu:Methodology,Data curation,Investigation,Validation,Writing-original draft,Writing-review and editing,Conceptualization.Shanshan Liu:Methodology,Data curation,Investigation,Validation,Writing-review and editing,Conceptualization.Jing Zhao:Methodology,Data curation,Investigation,Validation,Writing-review and editing,Conceptualization.Yan Jiang:Conceptualization,Methodology,Validation,Supervision,Writingreview and editing.Rong Deng:Conceptualization,Methodology,Validation,Supervision,Writing-review and editing.
Funding
Nothing to declare.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Competing interest
The authors declare that they have no conflicts of interest.
Acknowledgments
All patients with chronic liver diseases,health care staff,and statisticians participating in this study are gratefully acknowledged.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.12.014.
 International Journal of Nursing Sciences2024年1期
International Journal of Nursing Sciences2024年1期
- International Journal of Nursing Sciences的其它文章
- Nursing leadership: Key element of professional development☆
- Associations among frailty status,hypertension,and fall risk in community-dwelling older adults
- Facilitators and barriers to the implementation of dietary nutrition interventions for community-dwelling older adults with physical frailty and sarcopenia: A qualitative meta-synthesis
- The prevalence and factors associated with sarcopenia in Thai older adults: A systematic review and meta-analysis Phatcharaphon Whaikid,Noppawan Piaseu*
- Air quality self-management in asthmatic patients with COPD: An integrative review for developing nursing interventions to prevent exacerbations
- Measurement properties of assessment tools of Kinesophobia in patients with cardiovascular disease: A systematic review