
Agreements’ profile of Scheimpflug-based optical biometer with gold standard partial coherence interferometry
2023-12-14 08:52SaraSardariAkbarFotouhiEbrahimJafarzadehpurMehdiKhabazkhoob
Sara Sardari, Akbar Fotouhi, Ebrahim Jafarzadehpur, Mehdi Khabazkhoob
1Research and Technology Deputy, Tehran University of Medical Sciences, Tehran 1417653761, Iran
2Noor Ophthalmology Research Center, Noor Eye Hospital,Tehran 1968653111, Iran
3Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran 1417653761, Iran
4Noor Research Center for Ophthalmic Epidemiology, Noor Eye Hospital, Tehran 1968653111, Iran
5Department of Basic Sciences, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences,Tehran 1968653111, Iran
Abstract
● KEYWORDS: ocular biometry; optical biometer;Pentacam AXL
INTRODUCTION
Ocular biometric measurements are of great importance in ophthalmic studies as well as clinical practice.These measurements are used for the intraocular lens (IOL)power calculation before cataract surgery, screening of refractive surgery candidates, diagnosing and monitoring primary angle-closure glaucoma, and monitoring the progression of ametropia[1-2].According to the previous studies, optical biometry has higher accuracy and safety compared to ultrasound biometry[3].The IOL Master 500 is an optical biometer based on the principle of partial coherence interferometry (PCI)[4].Various studies have confirmed the high accuracy, reliability, and repeatability of this device; so it is known as a gold standard for optical biometry[5-7].
In recent years, various ocular biometric parameters and the anterior segment status have received attention due to the introduction of the newer generation IOL power calculation formulas, the widespread use of premium IOLs, and the increased number of cataract surgery candidates with a history of refractive surgery[1,8-10].This has led to the emergence of new multi-tasking devices that are capable of providing comprehensive information about the cornea and anterior segment in addition to measuring conventional biometric parameters such as axial length (AL) and anterior chamber depth (ACD).The Pentacam is a corneal topographer that uses a rotating scheimpflug camera to provide a three-dimensional scan of the anterior segment of the eye.The new version of this device (Pentacam AXL) utilizes PCI technology to perform non-contact optical biometry along with routine topographic measurements[1,11].
Limited studies have examined the agreement between Pentacam AXL biometric measurements with well-known and valid optical biometric systems[1,8,12-17].Pereiraet al[18]studied the agreement between the Pentacam AXL and the Lenstar LS900 in biometric measurements and the calculated IOL power.According to the results of this study, the AL measurements of the two devices were interchangeable, but there were significant differences in the ACD, keratometric readings, and calculated IOL power by all formulas between the two instruments.In another study, Wanget al[13]studied the agreement of ocular biometric measurements between Pentacam AXL, IOL Master 500, and IOL Master 700.The results of this study showed that these three devices were not significantly different in biometric measurements including AL, keratometry, and ACD, and had a high agreement in this regard.Another study by Muzyka-Wozniak and Oleszko[11]evaluated the agreement of the anterior segment and AL measurements between the Pentacam AXL and the IOL Master 500.The results of this study indicated significant differences in the AL, horizontal corneal diameter, and keratometric measurements between the two devices.Moreover, the calculated IOL power was significantly different between the two instruments, so that the Pentacam AXL overestimated the IOL power in 62% of the eyes based on the SRK/T formula.Due to the limitations and inconsistencies between the previous studies as well as the lack of reporting results according to different ocular conditions such as the presence or absence of cataracts, further studies are necessary on this subject.These additional studies will help to use the biometric capability of Pentacam AXL in clinical practice with more confidence.The present study aimed to investigate the agreement between Pentacam AXL and a reference optical biometer (IOL Master 500) in measuring the AL and other biometric indices according to some contributing parameters.
SUBJECTS AND METHODS
Ethical ApprovalThe Ethics Committee of Tehran University of Medical Sciences approved the study protocol, which was conducted in accordance with the tenets of the Helsinki Declaration.All participants signed a written informed consent.(National Ethics Code: IR.TUMS.FARABIH.REC.1399.010).The present report is part of a large cross-sectional populationbased study (Tehran Geriatric Eye Study) conducted from Jan.2019 to Jan.2020.The target population was all residents of Tehran, Iran aged 60y and above.In this study, sampling was performed using a multi-stage stratified random cluster sampling method.The 22 municipality districts of Tehran were considered as strata.A total of 160 clusters were randomly selected proportional to size (each cluster contained 20 individuals) from 22 strata of Tehran city.All people aged 60y and above were invited to participate in the study after explaining the study objectives and ensuring the confidentiality of information.
ExaminationsThe preliminary ocular examinations were performed in the next stage including the measurement of visual acuity, refraction, and anterior and posterior segment ocular examination.The uncorrected visual acuity and presenting visual acuity were measured using an LED visual acuity chart (Smart LC 13, Medizs Inc., Republic of Korea)at 6 m.The objective refraction was done using an autorefractometer (ARK510A, Nidek Co.42 LTD, Aichi, Japan).The subjective refraction was then performed to determine the optimal distance optical correction and the best-corrected distance visual acuity was recorded.Finally, all participants underwent an ocular health examination using a slit-lamp biomicroscope (Slit-lamp B900, Haag-Streit AG, Bern,Switzerland) by an ophthalmologist.The posterior segment examination was undertaken using a +90 D lens.
In the next step, all study participants underwent ocular biometry using IOL Master 500 and Pentacam AXL.There was a random order of biometric measurements by the two devices.The IOL Master 500 is the first generation of optical biometric devices that measure the AL using PCI.In addition to the Pentacam HR properties, the Pentacam AXL also measures the AL using PCI.All biometric measurements were performed by the same experienced optometrist on both eyes.An interval of 10min was considered between ocular biometry by the two devices.To account for diurnal variations, all biometric measurements were performed between 10a.m.and 4p.m.at least 2h after waking up.The exclusion criteria were dense corneal opacities preventing reliable measurement, macular pathologies causing fixation loss, a history of vitrectomy and other intraocular surgery, meibomian gland dysfunction,pterygium, high corneal astigmatism, poor image quality of Pentacam, ocular biometric signal to noise ratio less than 6.3 for Pentacam AXL and less than 2 for IOL Master 500.
DefinitionsThe cataracts were diagnosed and classified according to the World Health Organization grading system.Nuclear, cortical, and posterior sub-capsular (PSC) cataracts were defined based on the lens opacities grade 2 or more[19].The ALs 22 mm and less, 22 to 24.5 mm, and above 24.50 mm were defined as short, medium, and long, respectively.
Statistical AnalysisThe indices that were analyzed to examine the agreement between Pentacam AXL and IOL Master 500 were AL, ACD, horizontal corneal diameter, and flat and steep keratometric readings (K1 and K2).The mean±standard deviation (SD), median, and interquartile range (IQR)of these indices measured by the two devices were reported.The Pearson correlation coefficient was used to show the correlation of measurements.To assess the agreement of the measurements between the two instruments, the intraclass correlation coefficient (ICC) was reported.The Bland-Altman plots with 95% limits of agreement (LoA) were also used to illustrate the agreement of biometric measurements between the two devices[20].In the Bland-Altman diagram,the y-axis and x-axis represent the difference between the two measurements and the average of the two measurements,respectively.The 95% LoA was calculated according to this formula: “mean difference±1.96×SD”.P<0.05 was considered statistically significant.
RESULTS
Of 3791 invitees, 3310 participated in the study (response rate: 87.3 percent).After applying the exclusion criteria, 2411 eyes from 2411 individuals were analyzed for this report.Of these, 1485 (61.6%) were female and the mean age of the participants was 67.01±5.80y (60 to 95y).The frequency of normal, pseudophakic and cataractous eyes were 916 449, and 1046, respectively.
Table 1 shows the mean±SD and median (IQR) of the measured AL by the Pentacam AXL and IOL Master 500 according to the crystalline lens status, AL, and mean keratometry.Table 2 shows the differences between the two devices.According to the results, the lowest mean difference of the AL between the two devices was seen in pseudophakic eyes and the mean difference±SD was almost similar in normal and cataractous eyes.The ICC values for the AL measurements of the two instruments are shown in Table 2.As seen in Table 2, all ICC values in all three studied groups were higher than 0.995.The 95% LoA between the two devices were -0.13 to 0.19, -0.15 to 0.17, and -0.13 to 0.19 in normal,pseudophakic, and cataractous eyes, respectively.Figure 1 illustrates the Bland-Altman plots for the agreement of the two devices in measuring the AL according to the crystalline lens status.As seen in Figure 1, the dispersion of measurement differences (spread of outliers) was greater in eyes with cataracts.Figure 2 shows the mean difference of the AL measurements by the two devices in different groups of AL.As shown in Figure 2, the greatest difference was found in eyes with an AL longer than 24.5 mm.According to the post-hoc test,the mean difference of the AL was significantly different between eyes with an AL of more than 24.5 mm and eyes with an AL less than 24.5 mm.The results of the present study showed that in eyes with an AL of less than 22 mm,the lowest mean difference of AL measurements was related to pseudophakic eyes and the mean difference was similar in cataractous and normal eyes.The best agreement between the AL measurements of the two devices was also seen in the pseudophakic eyes.Similar findings were also observed in eyes with an AL of 22 to 24.5 mm.

Table 1 Mean, SD and median (IQR) of axial length measured with Pentacam AXL and IOL Master 500 according lens, axial length and mean keratometry

Table 2 Mean and standard deviation, rang and median (IQR) of paired differences, 95% limit of agreement and intraclass correlation coefficient of axial length measured with Pentacam AXL and IOL Master 500

Figure 1 Bland-Altman plots illustrating 95% limits of agreement between IOL Master 500 and Pentacam AXL in measuring the axial length in normal (A), pseuodophakic (B) and cataractous (C) eyes The middle line indicates the mean difference and the two dashed side lines show the 95% limits of agreement.Dashed lines in middle show trend.

Figure 2 The mean difference of the axial length measurements by IOL Master 500 and Pentacam AXL in different groups of axial length values.

Figure 3 Bland-Altman plots illustrating 95% limits of agreement between IOL Master 500 and Pentacam AXL in measuring the average keratometery in normal (A), pseuodophakic (B) and cataractous (C) eyes The middle line indicates the mean difference and the two dashed side lines show the 95% limits of agreement.Dashed lines in middle show trend.
In eyes with a mean keratometry<42 D, the mean difference of the AL between the two devices was 0.03, 0.01, and 0.02 mm, in normal, pseudophakic, and cataractous eyes,respectively.In this group of mean keratometry, the narrowest and widest LoAs were related to normal (-0.01 to 0.07) and pseudophakic (-0.05 to 0.07) eyes, respectively.In eyes with a mean keratometry of 42 to 46 D, the mean difference of the AL was the least in pseudophakic eyes; however, as shown in Table 2, the LoA was narrower than in cataractous eyes.In eyes with a mean keratometry above 46 D, the lowest and highest differences between the two devices were related to the pseudophakic and cataractous eyes, respectively.The LoA was also narrower in the pseudophakic than in other groups.The comparison of the two instruments in measuring other biometric components is shown in Table 3.Regarding the mean keratometry, as shown in Table 3, the lowest difference between the two devices was observed in the pseudophakic eyes and the highest difference was related to the normal eyes.Moreover, the IOL Master’s measurements were steeper than Pentacam’s measurements in all cases.The LoA between the two devices regarding the mean keratometry shows that the best LoAs were seen in cataractous and followed by normal eyes and the pseudophakic eyes had the widest LoA (Figure 3).As seen in Table 3, the IOL Master 500 measured the mean horizontal corneal diameter about 0.39, 0.40, and 0.40 mm higher than the Pentacam AXL in normal, pseudophakic, and cataractous eyes, respectively.The ICC values for horizontal corneal diameter measurements by the two devices were 0.802,0.823 and 0.817 in normal, pseudophakic and cataractous eyes,respectively.The 95% LoA between the two devices is shown in Figure 4.As shown in Figure 4, the narrowest LoAs was related to the pseudophakic eyes.According to the results, the mean difference of ACD measurements between the two devices was -0.1 and -0.12 in normal and cataractous eyes, respectively.The ICC of the ACD measurements was 0.886 in normal and 0.924 in cataractous eyes.Figure 5 shows the agreement of the two devices in cataractous and normal eyes.As seen, the agreement in the two groups is relatively close to each other.
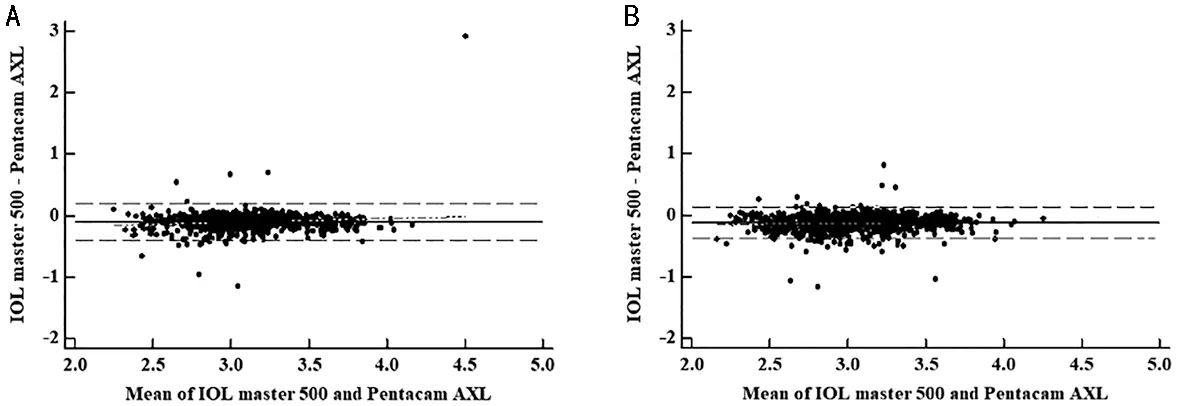
Figure 5 Bland-Altman plots illustrating 95% limits of agreement between IOL Master 500 and Pentacam AXL in measuring the anterior chamber depth in normal (A) and cataractous (B) eyes The middle line indicates the mean difference and the two dashed side lines show the 95% limits of agreement.Dashed lines in middle show trend.

Table 3 Mean, SD and median (IQR) of K1, K2, mean K, WTW and ACD measured with Pentacam AXL and IOL Master 500 and their 95%limit of agreement and intraclass correlation coefficient

Table 4 Literature review on the agreement between the Pentacam AXL and other devices in the measuring axial length
DISCUSSION
Since the introduction of the Pentacam AXL, several studies have examined the validity and reliability of its measurements[1,8,11-12,14-17,21-25].The most important application of the AL measurement is to calculate the IOL power; these calculations are strongly influenced by different values of the AL and keratometry[14,25].Therefore, it is important to know the validity of Pentacam AXL in measuring the AL in different values of AL and keratometry.On the other hand, most previous studies were performed in eyes with cataracts.This report investigated the agreement of Pentacam AXL with the IOL Master 500 (a gold standard optical biometer) in a large sample size in a variety of crystalline lens conditions according to the different ocular parameters.
It should be noted that the newer version of the IOL Master(IOL Master 700) has been introduced in recent years.This device measures the AL using swept-source optical coherence tomography (SS-OCT) with a wavelength of 1050 nm and its most important difference with the IOL Master 500 is the ability to measure crystalline lens thickness, vitreous length,and central corneal thickness[26].However, due to the fact that IOL Master 500 has longer history and used in more centers than its new version, we used it in this study.
Based on the results of the present study, the Pentacam AXL and IOL Master 500 had a high agreement in measuring the AL.
The 95% LoAs of AL measurements in three crystalline lens conditions were almost the same from -0.13 to 0.19.Although the mean difference between the two devices in the three groups was very low, paying attention to the LoA is also important from a clinical point of view.Olsen considered an error of up to 0.1 mm in measuring AL, which may be associated with 0.27 D post-operative refraction error, as ideal[27].Therefore, the results obtained in the present study are slightly different from this value.It should be noted that Pentacam AXL slightly underestimated the AL and the upper limit of the LoA also indicates a possible error up to 0.19 mm.So, in some biometric measurements with Pentacam AXL,about 0.5 D of myopia may occur after the surgery, which should be taken into account.
Table 4 shows a summary of the findings of the previous studies in this regard.As seen in Table 4, the difference between Pentacam AXL and other biometric devices has been reported in a range of 0.002 to 0.08 mm[1,8,11-12,14-16,18,22,24,28-30].
However, the LoA is diverse among previous studies,possibly due to different sample characteristics, measurement conditions, or measurement devices.For example, the narrowest LoA is related to the Tañá-Riveroet al[1]study,which compared the Anterion with the Pentacam AXL, and the widest LoA was reported by Pereiraet al[18]using Lenstar.
The results of the present study showed that in normal,pseudophakic, and cataractous eyes, the average AL measured by IOL Master 500 was longer than Pentacam AXL.Most previous studies have similarly reported that the average AL measured by the Pentacam AXL was shorter than that of the IOL Master 500.Compared to most other biometric devices, the findings of previous studies also indicate the shorter AL measurements by the Pentacam AXL.However,four studies reported longer AL measurements by Pentacam AXL compared to the recent biometers of Anterion (mean difference: -0.0083), Galilei G6 (mean difference: -0.04), and IOL Master 700 (mean difference: -0.019 and -0.05).Since the biometric technology of the Pentacam AXL and IOL Master 500 follows the same principle (PCI), this difference could be due to differences in the light source.
The highlight of the present study was the investigation of the agreement of AL measurements in the three crystalline lens statuses in a large sample.The comparison of the AL measurements according to the crystalline lens status showed that the lowest mean difference of the two devices was related to the pseudophakic eyes and the difference was almost similar in cataractous and normal eyes.This finding seems to be due to the homogeneity of the refractive index of the IOL.So far,no study has evaluated this agreement in pseudophakic eyes.Such evaluation is important considering biometry may be required in pseudophakic eyes.The backscattering from the crystalline lens acts as a source of noise in imaging and increases the variance of the measurements.In a more homogeneous environment such as pseudophakic eyes, the amount of scattering and consequently the noise would be reduced[31].
Although the mean difference of the AL measurements was almost similar in normal and cataractous eyes, the agreement data were more dispersed in eyes with cataracts.This finding seems logical considering the opacity of the crystalline lens with subsequent increased light scattering in eyes with cataracts and the difference in the amount of light scattering in the two devices[31].Moreover, in eyes with cataracts, increasing the crystalline lens refractive index and the difference in the refractive index distribution in different parts of the crystalline lens could make the AL measurement unpredictable and decrease the agreement.In normal eyes, the crystalline lens is not completely clear compared to IOL, and due to the age distribution of the study participants; small degrees of crystalline lens opacity are expected.Considering the definition of cataracts in the present study which included crystalline lens opacities grade 2 and above, minor opacities were considered normal.It should also be noted that some severe cases of cataracts were excluded because the two devices could not measure the AL, or only the IOL Master 500 could measure,and the Pentacam AXL’s SNR was not acceptable.Therefore,considering the dispersion of the agreement data (spread of outliers), it seems that the Pentacam AXL is less predictable in severe cases of cataracts.In the present study, 27 cataractous eyes whose measured AL values despite good SNR were significantly different between the two devices were excluded.In these cases, the Pentacam AXL measured the AL from 5.9 to 18.54 mm longer than the IOL Master 500.
A similar finding was previously reported in a study by Kim and Han[28]In that study; the authors attributed this discrepancy to the error of the Pentacam AXL and recommended that it is necessary to check the extra-ordinary AL values measured by the Pentacam AXL with another device.
In all three groups of normal, pseudophakic, and cataractous eyes, the mean difference of the AL between the two devices increased with increasing AL.Rodrigueset al[32]similarly reported that the agreement between the two instruments decreases with increasing the AL.The increase in the AL is often accompanied by ocular comorbidities, which could cause variable and unsteady fixation and affect the accuracy and predictability of the measurement.
The mean difference of the average keratometry reading between devices ranged from 0.20 D in pseudophakic eyes to 0.26 D in normal eyes.Other studies also showed these differences between 0.11 to 0.2 D[11,14,16].There was a high agreement between the two instruments in keratometric measurements.However, Pentacam AXL measured keratometry slightly flatter than the IOL Master 500, which is in line with the results of previous studies[11,14,16].Even studies comparing the keratometric measurements of the Pentacam AXL with the IOL Master 700[1], Anterion[1], Argos[15], Galilei G6[8], and Lenstar LS 900[18], reported flatter keratometric findings for the Pentacam AXL.The IOL Master 500 measures the radius of curvature of the cornea in a 2.3 mm diameter zone, while the Pentacam AXL measures simulated keratometry over 3 mm area around the corneal apex.Given that the periphery of the cornea is flatter than that of its center,it makes sense for keratometric measurements of the Pentacam AXL to be flatter.
According to the study by Ladi[33], a 0.5 D error in keratometry measurement will be associated with a 0.5 D post-operative refractive error.However, comparing this value with the LoA in the present study indicates that the agreement of these two devices in keratometry may be associated with a residual refractive error greater than 0.5 D.The results of Pentacam could be more trusted in this regard, as most studies showed Pentacam’s topography and keratometry measurements to be very valid even in pathologic corneas such as keratoconus[34].According to the results, the Pentacam AXL measured on average about 0.4 mm shorter horizontal corneal diameter than the IOL Master 500.In addition, the LoA and ICC values for horizontal corneal diameter measurements indicate less agreement for this index compared to other parameters.This finding was in line with the results of the studies by Wanget al[16]and Muzyka-Woźniaket al[11]Moreover, studies comparing the Pentacam AXL with other biometric devices have also shown that horizontal corneal diameter distance is underestimated by the Pentacam AXL[8,15].Tuet al[15]also found that the Pentacam AXL measured a horizontal corneal diameter of more than 1 mm shorter than the Argos.The reason for this difference may be due to the difference between the iris margin recognition algorithm and different digital processing to define the limbus in the two devices.
According to our results, the Pentacam AXL measured the ACD about 0.1 mm deeper than the IOL Master 500 in both normal and cataractous eyes.Tuet al[15]reported that the difference of less than 0.1 mm in measuring the ACD is not clinically significant.However, we believe that 95%LoA between the two devices should also be considered in addition to this difference.This LoA indicates that the difference between the two devices, especially in individuals with cataracts, can reach up to 0.37 mm.Therefore, the interchangeability of the ACD measurements of the two devices should be judged with caution.
Previous studies examining the agreement of ACD measurements between the Pentacam (both HR and AXL) and the IOL Master 500 confirm this finding[11,14,16].Comparing the ACD measurements of the Pentacam AXL with different devices is associated with contradictory results in the literature[1,8,15].Some studies showed the higher accuracy of ACD measurements by the Pentacam in unusual corneas.Given that the Pentacam AXL derives ACD values from the scheimflug data which is independent of subject’s fixation,it seems to provide a more accurate measurement of ACD compared to the IOL Master 500[16].
Norrby[35]showed that each millimeter error in ACD measurement can be associated with about 1.44 D residual refractive error.According to the LoA between the two devices in measuring ACD, there may be a difference of about 0.4 mm between the two devices, which is equivalent to a residual refractive error of about 0.6 D.In this regard, previous studies reported very accurate measurement of the ACD by Pentacam.In general, the agreement of Pentacam AXL and IOL Master 500 in measuring the AL was excellent.However,in cataractous eyes as well as eyes with long AL, the AL measurements of this two devices were slightly different.The two instruments agreed weak in ACD measurements and they were not interchangeable for keratometry and horizontal corneal diameter measurement.
ACKNOWLEDGEMENTS
Foundation:Supported by the Deputy of Research and Technology of Tehran University of Medical Sciences as a PhD Thesis.
Conflicts of Interest:Sardari S,None;Fotouhi A,None;Jafarzadehpur E,None;Khabazkhoob M,None.
 International Journal of Ophthalmology2023年12期
International Journal of Ophthalmology2023年12期
- International Journal of Ophthalmology的其它文章
- Dynamic tear meniscus parameters in complete blinking:insights into dry eye assessment
- Effects of diquafosol sodium in povidone iodine-induced dry eye model
- Morroniside ameliorates lipopolysaccharide-induced inflammatory damage in iris pigment epithelial cells through inhibition of TLR4/JAK2/STAT3 pathway
- Role of reactive oxygen species in epithelial-mesenchymal transition and apoptosis of human lens epithelial cells
- Electroacupuncture alleviates ciliary muscle cell apoptosis in lens-induced myopic guinea pigs through inhibiting the mitochondrial signaling pathway
- De novel heterozygous copy number deletion on 7q31.31-7q31.32 involving TSPAN12 gene with familial exudative vitreoretinopathy in a Chinese family