
Effects of cytoreductive surgery combined with hyperthermic perfusion chemotherapy on prognosis of patients with advanced gallbladder cancer
2023-12-10 02:23:42JinXiuWuRongHuaXiangJiLuoFengXieLiYao
Jin-Xiu Wu,Rong Hua,Xiang-Ji Luo,Feng Xie,Li Yao
Abstract BACKGROUND Gallbladder cancer (GC) is a common malignant tumor and one of the leading causes of cancer-related death worldwide.It is typically highly invasive,difficult to detect in the early stages,and has poor treatment outcomes,resulting in high mortality rates.The available treatment options for GC are relatively limited.One emerging treatment modality is hyperthermic intraperitoneal chemotherapy(HIPEC).HIPEC involves delivering heated chemotherapy directly into the abdominal cavity.It combines the strategies of surgical tumor resection and localized chemotherapy administration under hyperthermic conditions,aiming to enhance the concentration and effectiveness of drugs within the local tumor site while minimizing systemic toxicity.AIM To determine the effects of cytoreductive surgery (CRS) combined with HIPEC on the short-term prognosis of patients with advanced GC.METHODS Data from 80 patients treated at the Punan Branch of Renji Hospital,Shanghai Jiao Tong University School of Medicine between January 2018 and January 2020 were retrospectively analyzed.The control group comprised 44 patients treated with CRS,and the research group comprised 36 patients treated with CRS combined with HIPEC.Then,the survival time and prognostic factors of the two groups were compared,as well as liver and kidney function indices before and six days after surgery.Adverse reactions and complications were recorded in both groups.RESULTS The baseline data of the research and control groups were similar (P > 0.05).Six days after surgery,the alanine aminotransferase,aspartate aminotransferase,total bilirubin,and direct bilirubin levels significantly decreased compared to the preoperative levels in both groups (P < 0.05).However,the values did not differ between the two groups six days postoperatively (P > 0.05).Similarly,the postoperative creatinine and blood urea nitrogen levels were significantly lower than the preoperative levels in both groups (P < 0.05),but they did not differ between the groups six days postoperatively (P > 0.05).Furthermore,the research group had fewer postoperative adverse reactions than the control group (P=0.027).Finally,a multivariate Cox analysis identified the tumor stage,distant metastasis,and the treatment plan as independent factors affecting prognosis (P < 0.05).The three-year survival rate in the study group was higher than that in the control group (P=0.002).CONCLUSION CRS combined with HIPEC lowers the incidence of adverse reactions and improves survival in patients with advanced GC.
Key Words: Gallbladder diseases;Chemotherapy,Cancer,Regional Perfusion;Gallbladder neoplasms;Prognosis;Regression analysis;Survival rate
INTRODUCTION
The incidence of gallbladder cancer (GC) ranks first among all biliary tract tumors and is frequently observed in female patients.Additionally,cholecystolithiasis with chronic inflammation is a comorbidity considered a high-risk factor for GC[1].With symptoms similar to those of biliary colic and chronic cholecystitis,GC can easily go undiagnosed or misdiagnosed.Moreover,this type of cancer is strongly invasive and develops rapidly;therefore,patients often have middle-or late-stage disease at diagnosis[2].Approximately 30% of patients with GC in China complain of gallstones,inflammation,or polyps at the time of diagnosis,and some patients are unexpectedly diagnosed with GC on pathological examination after cholecystectomy in the hospital[3].
Surgical resection is the only curative treatment for GC.However,GC is highly malignant,can easily invade adjacent organs,and has a high lymph node metastasis rate and poor adjuvant treatment effect.Therefore,the prognosis is usually unfavorable,and the overall five-year survival rate is < 5%[4].In cases of tumor recurrence,systemic therapy can be selected based on pathological characteristics to prolong survival time[5].Therefore,close postoperative follow-up is crucial.Reoperation may not be ideal for patients with recurrent or metastatic GC.Traditional systemic chemotherapy has many side effects;therefore,it is crucial to choose postoperative adjuvant therapies with mild side effects and good curative effects[6,7].
Many years of research have resulted in hyperthermic intraperitoneal chemotherapy (HIPEC),a relatively new technology that has become crucial for treating intra-abdominal tumors[8].After more than 40 years of clinical application and the continual development of perfusion technology,the consensus is that HIPEC significantly affects peritoneal cavity metastasis in patients with digestive tract tumors[9].Existing level I evidence shows that HIPEC can treat and prevent peritoneal implantation of malignant peritoneal tumors and reduce the incidence of peritoneal metastasis[10].Over time,HIPEC has been gradually applied to the gastrointestinal tract,gynecological tumors,and other fields,and its clinical efficacy and safety have been widely recognized[11].Most studies on gynecological malignant tumors,especially advanced ovarian cancer[12],have reported good curative effects;thus,HIPEC has become the firstline treatment for gynecological malignant tumors.Since GC has a high degree of malignancy and metastasis rate,it requires further postoperative consolidation or adjuvant therapy to prolong survival and improve the patient’s quality of life[11].Currently,postoperative adjuvant therapy is mainly systemic chemotherapy;however,some patients experience many intolerable side effects,compromising their quality of life.HIPEC for gastrointestinal and gynecological malignant tumors has delivered good results;therefore,we speculate that it is feasible to adopt HIPEC as an auxiliary treatment after GC surgery.The curative effects of HIPEC after GC surgery need to be clarified.Therefore,this study analyzed the short-term effects of cytoreductive surgery (CRS) combined with HIPEC in patients with advanced GC to provide a new,alternative treatment plan.
MATERIALS AND METHODS
Participant source
Data from 122 patients with advanced GC treated at the Punan Branch of Renji Hospital,Shanghai Jiao Tong University School of Medicine between January 2018 and January 2020 were analyzed retrospectively.Our hospital’s medical ethics committee approved this study.
Inclusion and exclusion criteria
The inclusion criteria were patients: (1) With confirmed GC through postoperative pathology;(2) With tumor,node,metastasis (TNM) stage III or IV disease;(3) Between 18 and 80 years old;(4) Who had not received radiotherapy,chemotherapy,and other adjuvant therapies before surgery;(5) Without abnormalities of the heart,lung,brain,kidney,or other important organs;and (6) With a Karnofsky Performance Scale score of ≥ 70 points[13].
The exclusion criteria were patients: (1) With TNM stage I or II disease;(2) With abnormalities in the heart,lung,brain,liver,kidney,or other important organs;(3) With severe abdominal adhesion;(4) With other malignant tumors;(5) With blood system diseases or blood coagulation insufficiency;(6) With intestinal obstruction;(7) With cachexia;and (8) Who had received chemotherapy,radiotherapy or other adjuvant therapy after surgery.
Participant screening
Eighty patients who met these requirements were screened based on their electronic medical records.Among them,44 patients treated with CRS were enrolled in the control group,and 36 patients treated with CRS combined with HIPEC were enrolled in the research group.
Clinical data collection
Clinical data of the patients were collected,including age,sex,tumor stage,degree of differentiation,comorbidities,tumor size,lymph node metastasis,nerve invasion,distal metastasis,and vascular invasion.In addition,changes in liver function indices before and after surgery were collected.
Outcome measures
The primary outcome measures were survival time and prognosis.The secondary outcome measures were comparisons of the clinical data between the two groups,including indices related to liver and kidney function before surgery and six days after surgery.Adverse reactions and complications were also recorded in both groups.
Follow-up
Re check the patient in the outpatient department according to the doctor’s suggestion,or follow up the patient through telephone communication after discharge.The patients were followed up at 1,2,3,6,9,12,18,24,30 and 36 mo after operation.Patients who could not return to the hospital on time or regularly were followed up by telephone,and the circumstances of their recent situation were noted.This study followed each patient for three years or until death.
Statistical analyses
All statistical analyses were performed with SPSS version 26.0 (IBM SPSS Inc.,Chicago,United States).Measurement data are presented as means ± SD.All data were subjected to normality tests and analyzed using independent-samplet-tests.Countable data were analyzed usingχ2tests.Survival time was analyzed based on the follow-up results,and the survival rates of the two groups were compared using the log-rank method.Survival curves of the two groups were plotted using the Kaplan-Meier method.Multivariate Cox regression analysis was performed to identify independent risk factors affecting patient prognosis.P-vales of < 0.05 were considered significant.
RESULTS
Baseline data
The research and control groups had similar baseline data (P> 0.05,Table 1).
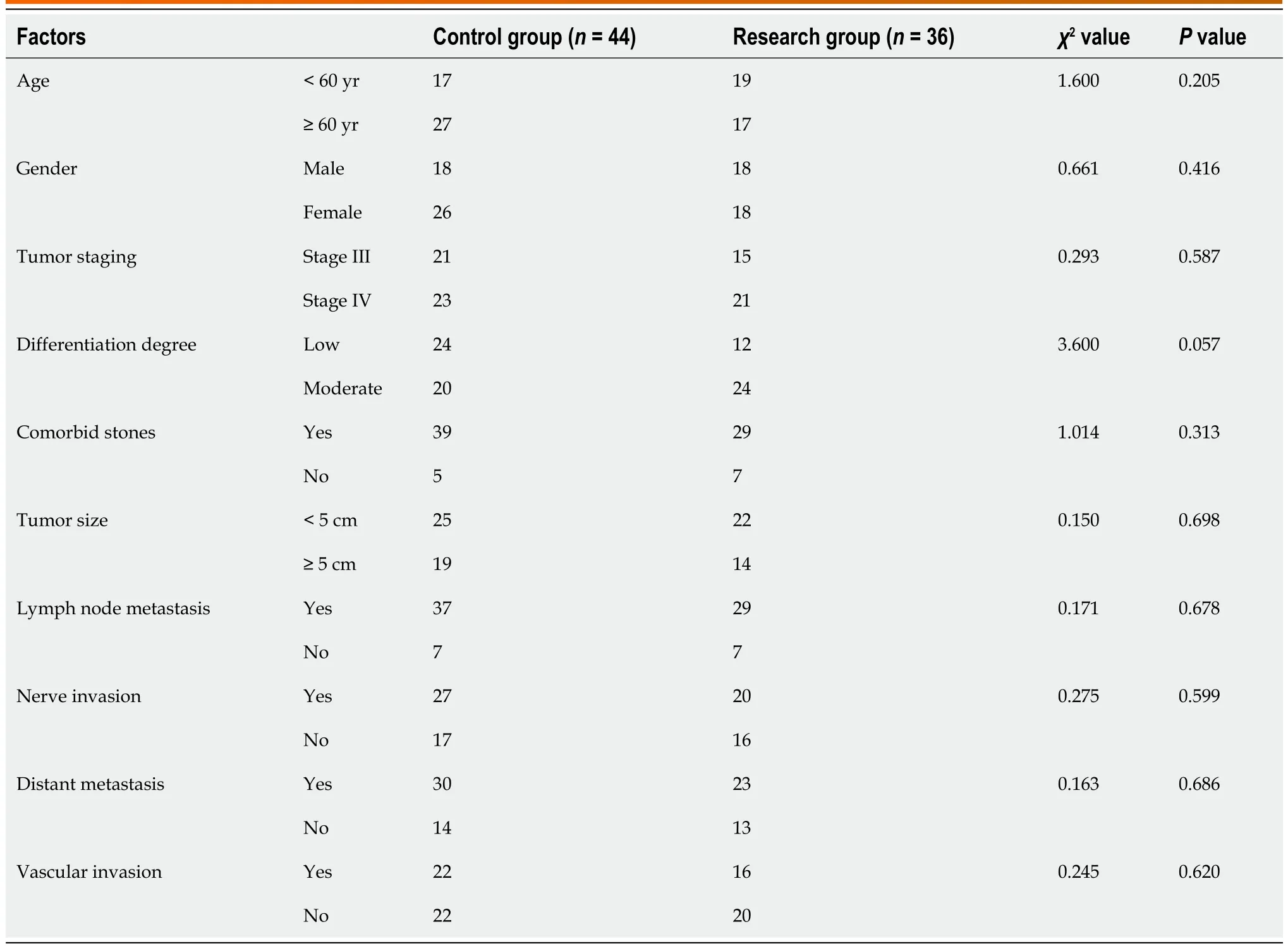
Table 1 Baseline data
Liver function indices before and after surgery
Liver function-related indices were compared between the two groups before and six days after surgery.The alanine aminotransferase,aspartate aminotransferase,total bilirubin,and direct bilirubin levels were significantly lower after surgery than before surgery in both groups (P< 0.05,Figure 1).However,after surgery,the levels did not differ between the two groups (P> 0.05,Figure 1).

Figure 1 Liver function indices before and after surgery. A: Alanine aminotransferase;B: Aspartate aminotransferase;C: Total bilirubin;D: Direct bilirubin concentrations before (orange) and after (green) surgery.aP < 0.05;bP < 0.01;dP < 0.0001.ALT: Alanine aminotransferase;AST: Aspartate aminotransferase;TBIL:Total bilirubin;DBIL: Direct bilirubin.
Renal function indices before and after surgery
The renal function-related indices were compared between the two groups before and six days after surgery.The creatinine and blood urea nitrogen levels were significantly lower after surgery than before surgery in both groups (P<0.05,Figure 2).However,after surgery,the levels did not differ between the two groups (P> 0.05,Figure 2).
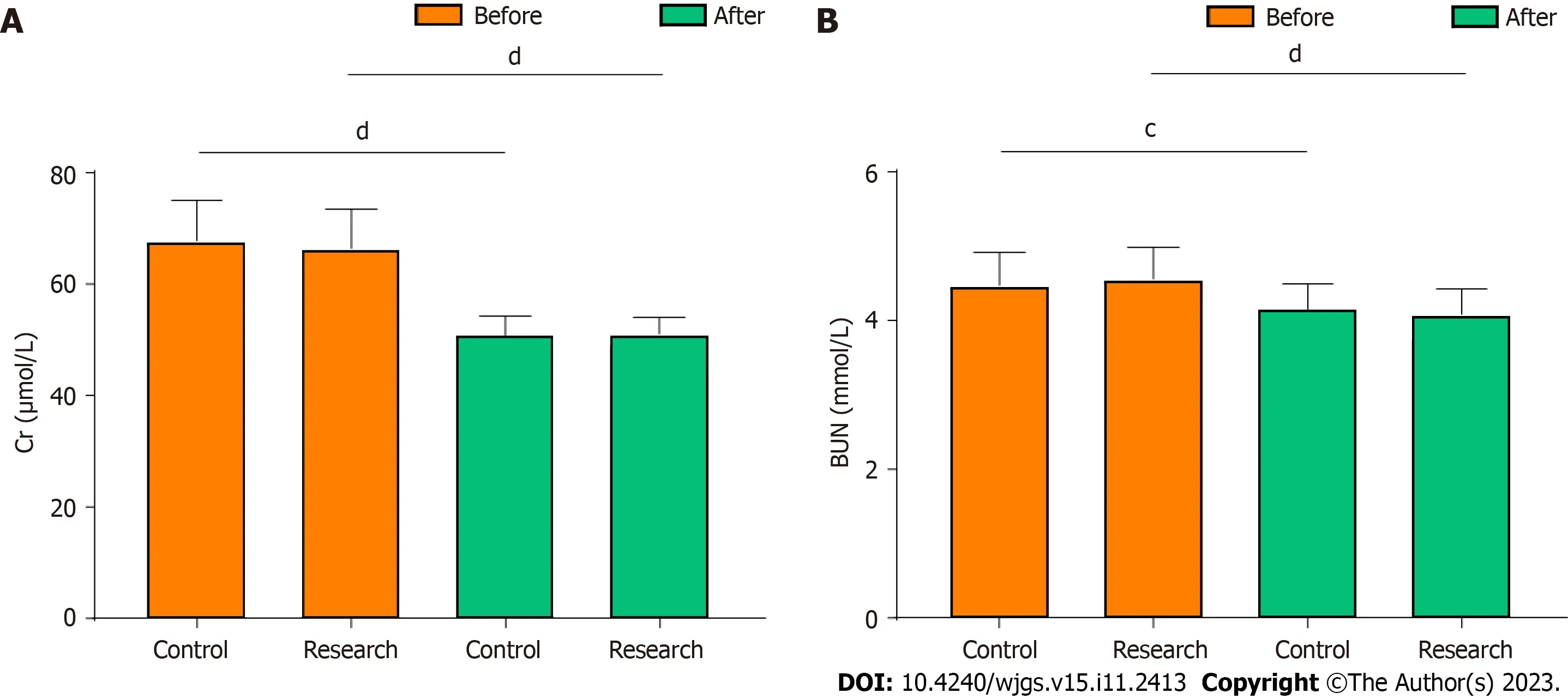
Figure 2 Renal function markers before and after surgery. A: Creatinine;B: Blood urea nitrogen concentrations before (orange) and after (green) surgery.cP < 0.001,dP < 0.0001.Cr: Creatinine;BUN: Blood urea nitrogen.
Adverse reactions
The research group has notably fewer adverse reactions than the control group after surgery (P=0.027,Table 2).

Table 2 Adverse reaction statistics
Prognostic factors
Patient survival was analyzed by Cox regression analysis;the univariate analysis identified the treatment plan,tumor stage,lymph node metastasis,distant metastasis,and vascular invasion as factors affecting prognosis (P< 0.05,Table 3).However,the multivariate analysis only identified the tumor stage,distant metastasis,and treatment plan as independent prognostic factors (P< 0.05,Table 4).
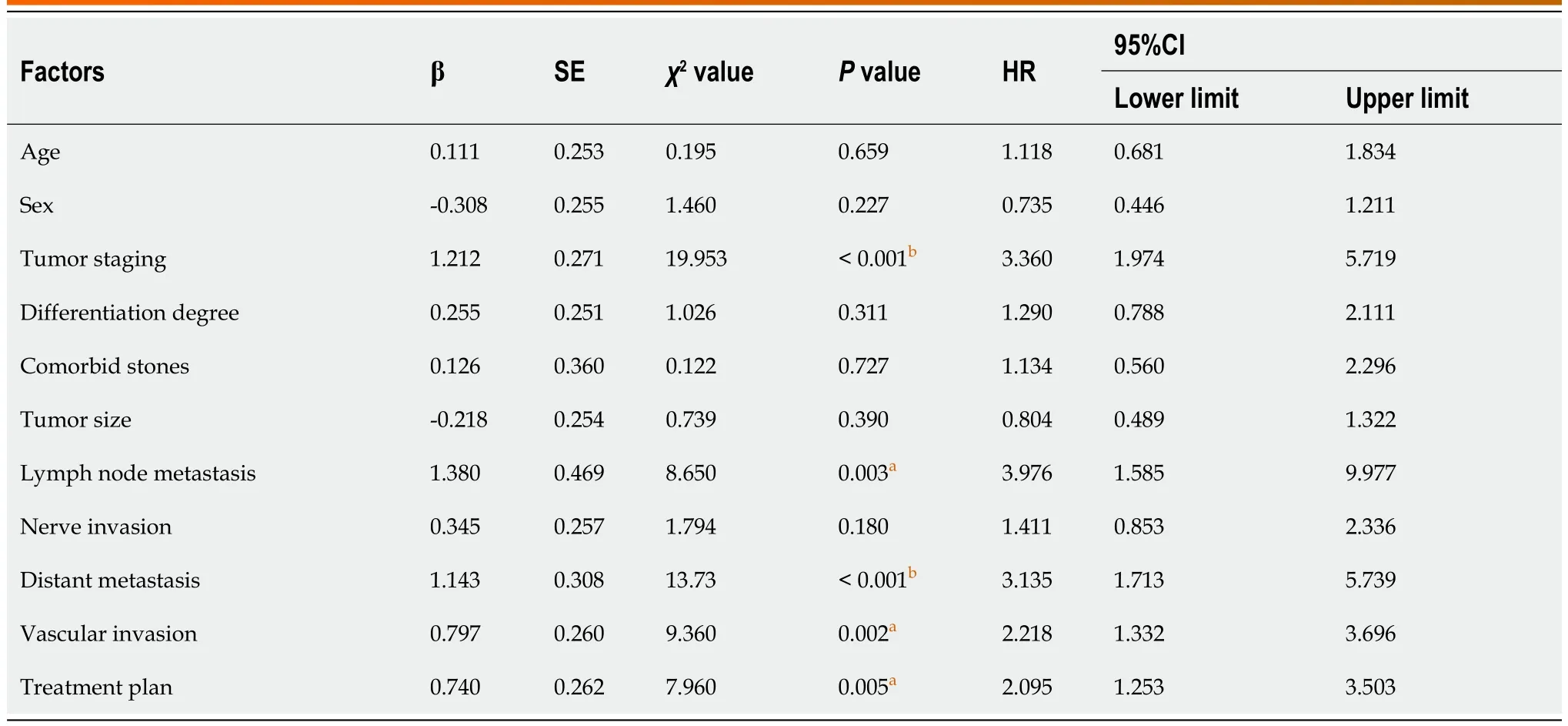
Table 3 Univariate Cox regression analysis results
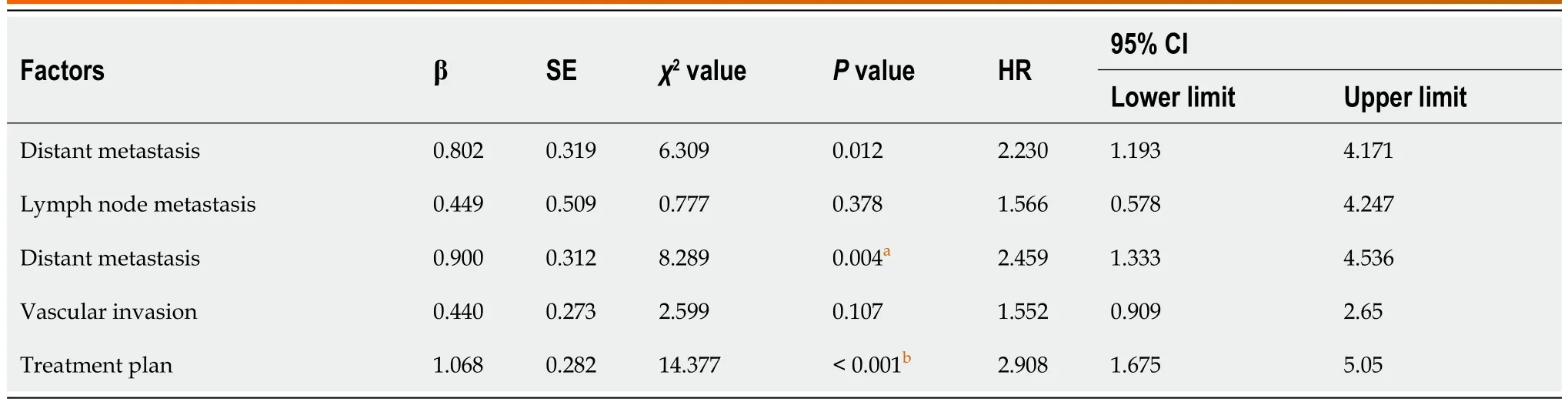
Table 4 Multivariate Cox regression analysis results
The relationship between prognostic indicators and patient survival
In the final analysis of the study,Cox regression analysis was performed to examine prognostic indicators related to patient outcomes.The results indicated that patients with stage III tumors,no distal metastases and those who received CRS had significantly higher 3-year survival rates compared to their respective control groups (P< 0.01,Figure 3).
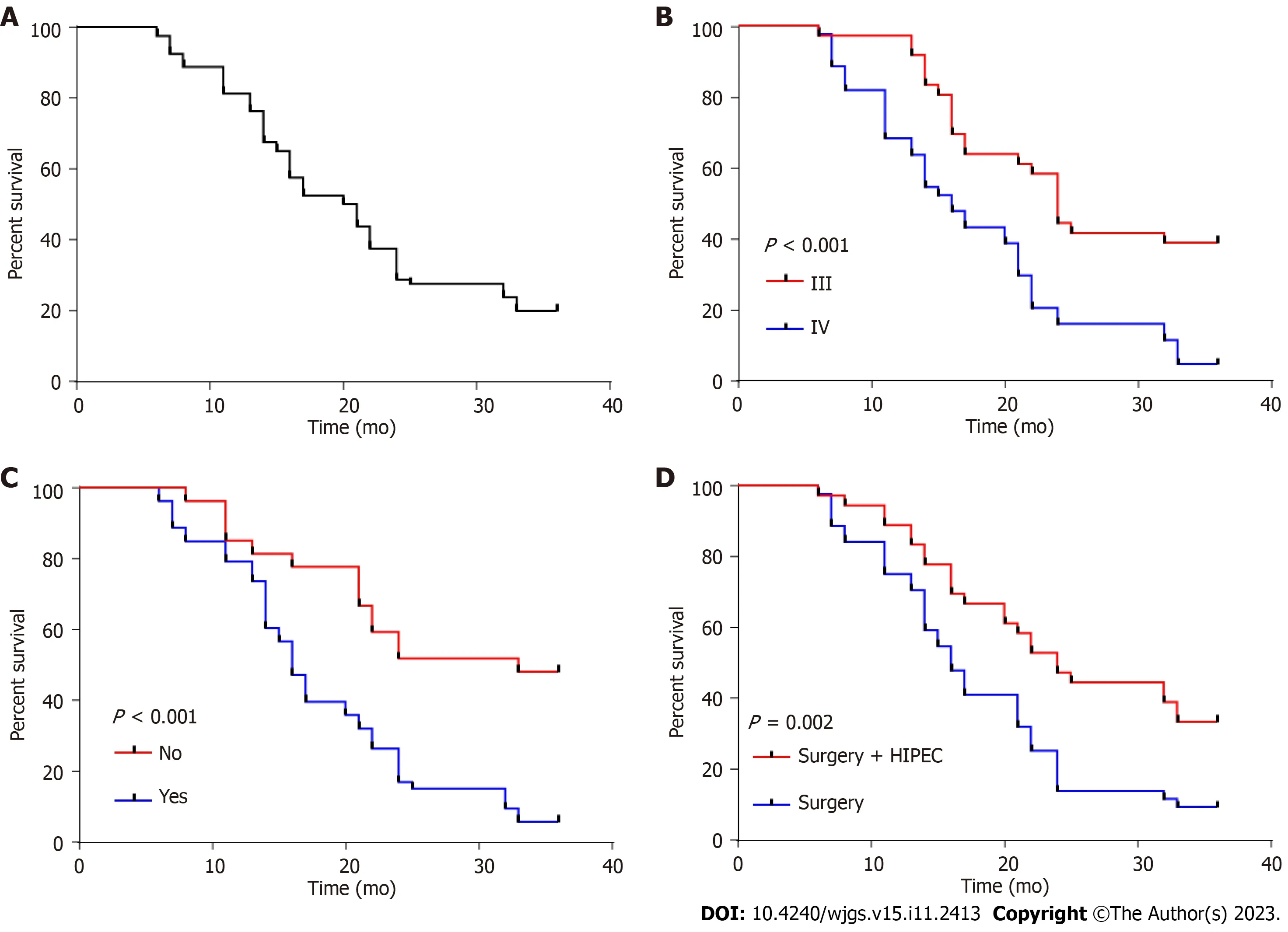
Figure 3 Three-year survival curves of independent prognostic factors. A: Overall survival;B: Tumor stage;C: Distant metastasis;D: Treatment plan.HIPEC: Hyperthermic intraperitoneal chemotherapy.
DISCUSSION
GC has an extremely low incidence (less than 4%);however,its five-year survival rate does not exceed 5%[14].Mostpatients have middle-or late-stage disease at the first visit;thus,their survival time does not exceed one year[15].Surgical resection is the only treatment option for GC.A simple cholecystectomy is feasible in the early stages without obvious metastasis[16].However,surgery is more complicated for patients with metastasis regardless of the stage;if the imaging examination determines that the tumor is resectable and there are no absolute surgical contraindications,then organs with a possible correlation with tumor invasion should also be resected to ensure complete resection of the tumor[17].In these cases,extended CRS of the GC,including the gallbladder,tumor,adjacent organs,lymph nodes,ligaments,and bile duct,is required.Additionally,the lymph nodes around the bile duct,portal vein,and duodenum should be resected as much as possible[4].However,less than 10% of patients undergo tumor resection through surgery,and nearly 50% have lymph node metastasis[18].
During surgery,instruments may touch cancer cells at the margin,causing them to fall off and form an implantation metastasis[19].Additionally,tumor dissection can sometimes increase intraperitoneal spread and growth of GC cells owing to their aggressive invasion and adhesion or growth variation.Systemic chemotherapy is frequently administered to patients with unresectable tumors or surgical contraindications.However,the effect of radiotherapy and chemotherapy in most advanced-stage patients is poor;it may prolong progression-free survival,but the five-year survival rate for those with malignant biliary tumors remains at less than 5%[20].Furthermore,intravenous chemotherapeutic drugs do not easily infiltrate the abdominal cavity;therefore,their effect on tumors is not ideal[21].Consequently,even if the tumor can be surgically removed,most GCs still progress and metastasize after surgery,highlighting the importance of finding an adjuvant therapy to improve prognosis.
HIPEC is a novel method that combines chemical and physical therapy[22].This treatment takes advantage of the destructive effect of high temperature on tumor cells,killing them by adding heated chemotherapy drugs into the abdominal cavity[23].Additionally,high temperatures promote the diffusion of chemotherapy drugs,so the drugs act on tumor cells more effectively.HIPEC treatment can also involve continuous washing through a power pump to increase the probability of contact between the chemotherapeutic drugs and tumor cells.As a result,the chemotherapeutic drugs are maintained at an effective concentration and produce stronger lethality.Compared with intravenous chemotherapy,HIPEC treatment alleviates adverse reactions and improves patient tolerance,delivering a more effective treatment for malignant abdominal tumors[24].Therefore,HIPEC therapy is a safe and effective treatment suitable for malignant abdominal tumors.In the present study,the incidence of adverse reactions was notably lower in the research group than in the control group.However,liver and kidney function did not differ between the two groups after treatment.Nonetheless,considering this study’s small sample size and short observation time,observing and analyzing more cases is necessary.
Finally,we analyzed the prognostic factors affecting three-year patient survival.The tumor stage,distant metastasis,and treatment plan were independent factors affecting prognosis.Many reports have suggested a correlation between tumor stage,distant metastasis,and prognosis in patients with advanced GC[19,25,26].This study found that CRS combined with HIPEC improves the survival time,indicating that this combination is safe and effective.
Although this study confirmed that CRS combined with HIPEC improves the survival time of patients with advanced GC,there are some limitations.First,this was a single-center study with limited data,which may have resulted in bias in the analysis.Second,this study did not obtain long-term follow-up data from the patients.Therefore,whether the surgical plan affects the long-term prognosis requires further verification.We hope to conduct a prospective study with a longer follow-up period to improve our conclusions.
CONCLUSION
In summary,CRS combined with HIPEC decreases the incidence of adverse reactions and improves survival in patients with advanced GC.Although our study shows the encouraging results of CRS-HIPEC treatment for GC treatment,however,we understand that as a new therapeutic strategy,the long-term impact and efficacy of it need to be verified by further clinical studies.
ARTICLE HIGHLIGHTS
Research background
Gallbladder cancer (GC) is one of the most deadly malignancies worldwide,with a high incidence of peritoneal metastasis,leading to poor prognosis.Despite advances in systemic chemotherapy,survival outcomes remain unsatisfactory.Cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) has been proposed as a promising approach to improve survival and reduce postoperative complications;however,its benefits and risks remain under investigation.
Research motivation
The primary research question was: Is CRS combined with HIPEC efficient and safe for managing GC? The key issues for resolution are the benefits and risks of this combined approach,including its effect on survival rates and postoperative complications compared with CRS.Addressing these questions is paramount to providing evidence-based guidance for clinicians for GC management;it could also potentially revolutionize the treatment paradigm and improve survival rates and quality of life for these patients.Moreover,it opens avenues for further research to optimize CRS-HIPEC protocols and identify patient subgroups that could benefit the most from this approach.
Research objectives
The main objective of this study was to evaluate the efficacy and safety of CRS combined with HIPEC for managing GC.We aimed to comprehensively understand the impact of CRS-HIPEC on survival rates and postoperative complications,which is crucial for future research as it informs clinical decision-making and establishes a foundation for refining treatment protocols.
Research methods
This study employed a retrospective analysis of the medical records of patients with GC treated with CRS-HIPEC.This method allows for a thorough examination of patient outcomes and treatment complications.Additionally,this study includes a comparative analysis of patients receiving CRS,highlighting the novel aspects of the CRS-HIPEC approach.
Research results
CRS-HIPEC significantly improved the survival rates of patients with GC.This study also highlighted an increased risk of certain postoperative complications.These results contribute to the field by providing empirical evidence for the efficacy and safety of CRS-HIPEC.
Research conclusions
CRS-HIPEC significantly improves survival rates but with certain risks.Furthermore,the results of this study underscore the need for personalized patient selection to maximize benefits and minimize complications.
Research perspectives
Future research should focus on optimizing CRS-HIPEC protocols and developing criteria for patient selection,which would enhance the benefits of this approach and mitigate the potential risks.Prospective,randomized controlled trials are also needed to corroborate these findings.
FOOTNOTES
Author contributions:Wu JX,Yao L,and Hua R designed the manuscript;Wu JX performed the study and wrote the manuscript;Yao L supervised the report writing;Hua R contributed to the analysis;Luo XJ and Xie F supervised the report.
Supported byShanghai Pudong New Area Health Commission’s Excellent Young Medical Talent Training Plan,No.PWRq2020-68;Shanghai Pudong New Area Health Commission Discipline Leader Training Project,No.PWRd2020-16;and Shanghai Pudong New Area Science and Technology Development Fund,No.PKJ2020-Y36.
Institutional review board statement:The Punan Branch of Renji Hospital,Shanghai Jiao Tong University School of Medicine reviewed and approved this study.
Informed consent statement:All study participants and their legal guardians provided written informed consent.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:The dataset is available from the corresponding author at yaolibestpn@sina.com.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Jin-Xiu Wu 0009-0000-9816-5599;Rong Hua 0009-0000-4521-3761;Xiang-Ji Luo 0009-0007-3534-1437;Feng Xie 0009-0009-3800-764X;Li Yao 0009-0005-4726-2387.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Wang JJ
 World Journal of Gastrointestinal Surgery2023年11期
World Journal of Gastrointestinal Surgery2023年11期
- World Journal of Gastrointestinal Surgery的其它文章
- Systematic sequential therapy for ex vivo liver resection and autotransplantation: A case report and review of literature
- Gastric inflammatory myofibroblastic tumor,a rare mesenchymal neoplasm: A case report
- Comprehensive treatment and a rare presentation of Cronkhite-Canada syndrome: Two case reports and review of literature
- Isolated traumatic gallbladder injury: A case report
- Metachronous primary esophageal squamous cell carcinoma and duodenal adenocarcinoma: A case report and review of literature
- Organ sparing to cure stage IV rectal cancer: A case report and review of literature