
Recovery shape of physical activity after COVID-19 pandemic
2023-08-02 04:00PiyawatKatewongsaDyahAnantaliaWidyastariNarumolHaemathulinAunyaratKhanawapeeSurasakPenmai
Piyawat Katewongsa ,Dyah Anantalia Widyastari, *,Narumol Haemathulin ,Aunyarat Khanawapee ,Surasak Penmai
a Institute for Population and Social Research,Mahidol University,Salaya,Phutthamonthon,Nakhon Pathom 73170,Thailand
b Thailand Physical Activity Knowledge Development Centre(TPAK),Salaya,Phutthamonthon,Nakhon Pathom 73170,Thailand
Abstract Background:Since the shutdowns associated with the coronavirus disease 2019 pandemic,there has been limited discourse on physical activity(PA)recovery(i.e.,the ability of individuals to resume PA at pre-pandemic levels),including recovery rate,speed of recovery,which individuals are able to return quickly,who is left behind,and what are the causes of those differences.This study aimed to estimate the level and shape of PA recovery rate in Thailand.Methods: This study employed 2 rounds (2020 and 2021) of Thailand’s Surveillance on Physical Activity dataset for the analysis.Each round included over 6600 samples from individuals aged 18 years or older.PA was assessed subjectively.Recovery rate was calculated from the relative difference in the cumulative minutes of moderate-to-vigorous PA(MVPA)from 2 different periods.Results:The Thai population experienced a medium level of recession of PA(-26.1%)and a moderate level of recovery of PA(37.44%).PA recovery in the Thai population resembled an imperfect V shape,reflecting a sharp decline followed by an immediate upturn;still,recovered PA remained lower than pre-pandemic levels.The quickest recovery was found among older adults,whereas students,young adults,residents of Bangkok,the unemployed,and those who had a negative attitude toward PA experienced the highest recession of PA and were among the slowest to recover.Conclusion:The level of recovery of PA among Thai adults is largely determined by the preventive behaviors demonstrated by groups within the population who have a higher awareness of their health.The effect of the mandatory coronavirus disease 2019 containment measures on PA was temporary.However,the slower recovery rate of PA among some individuals was caused by a combination of restrictive measures and socioeconomic inequality,which required more time and effort to overcome.
Keywords: Health promotion;Preventive behavior;Resilience;Surveillance
1.Introduction
The importance of physical activity (PA) for health has been documented worldwide.Engaging in regular adequate PA may lower the risk of getting a non-communicable disease(NCD),prevent individuals from becoming overweight or obese,and also improve mental health and well-being.1It is concerning,then,that studies have documented a significant reduction in PA levels during the coronavirus disease 2019(COVID-19) pandemic,both in terms of cumulative minutes and the prevalence of sufficient moderate-to-vigorous PA(MVPA).2,3
Scholars have expressed a growing concern that the reduction in PA following the COVID-19 pandemic and restrictions in many countries may result in an increase in long-term sedentary behavior among their populations.However,evidence is limited,as global PA surveillance has been constrained by national and local pandemic containment measures.Among the existing studies,there are inconsistent results on the change and recovery rate for PA.Longitudinal observations of PA during several periods of state-ordered measures(lockdowns,curfews,border closures,etc.) showed that 12%-18% of the population remained inactive even after the restrictive measures were lifted.2,4However,there is also a growing body of literature showing that the decrease in PA during the COVID-19 pandemic rebounded shortly afterwards for certain group of individuals,even while it persists for other groups.3,5,6
Heterogeneity and inequality in PA are established facts worldwide.Studies show that PA participation is largely determined by the differences in individual-biological (i.e.,age,sex),7-9socioeconomic,10and community-environmental factors.11,12Inequalities in access and PA opportunity are consistently found to be the predominant factors affecting an individual’s participation in PA.13-18A bulk of evidence also documents the adverse effects of the COVID-19 pandemic on a population’s PA.3,19-21However,there is a lack of evidence regarding how and to what extent PA inequality may affect PA recovery.
At present,there has been limited discourse on PA recovery(i.e.,the ability of individuals to return to PA at pre-pandemic levels),including the recovery rate (the proportion who can resume),the speed of recovery (how fast individuals resume their regular PA),which individuals are able to resume quickly,who is left behind,and what are the causes of those differences.The current literature on post-COVID-19 recovery is mostly reported by economists who study the shape of economic recovery.22-24The shapes(which economists use as shorthand) are often depicted by letters in the Latin alphabet that reflect the duration,rate,and magnitude of changes following a shock (i.e.,COVID-19).A V-shaped response depicts a steep decline followed by a quick recovery with minimal long-term damage,whereas a U shape portrays a longer period of recovery.25The W shape represents a rapid recovery followed by a second period of decline,and an L shape depicts a downturn in which growth falls precipitously and does not recover for an extended period.25A K shape depicts a situation where the recovery rate is not uniform and a part of the population experiences a speedy recovery while the rest is stalling.22
For this study,we adapted these recovery shapes from the field of economics to portray the recovery rate in PA in Thailand in the wake of the COVID pandemic.Data are extracted from nationally representative surveys at 3 different periods:before the COVID-19 pandemic (2019),during the stateordered containment measures (2020),and after certain COVID-related restrictions were lifted (2021).The results of this study are meant to be beneficial for the government and policy makers as they assist the population in resuming their PA at pre-pandemic levels.The study also adds to the body of knowledge on PA recovery by documenting recession and recovery patterns of PA at different time periods.The simplicity of the analysis also enables countries to adopt the methodology by using widely available PA data.
2.Methods
2.1.Population and sample
This study utilized 2 rounds(2020 and 2021)of Thailand’s Surveillance on Physical Activity(SPA)dataset for the analysis.We also collected 2019 data by asking the participants of the SPA2020 to recall their PA level prior to the COVID-19 pandemic.The SPA is a series of national surveys that are conducted annually by the Thailand Physical Activity Knowledge Development Centre,Institute for Population and Social Research of Mahidol University in Thailand.Usually,the SPA collects data on PA by using face-to-face interviews with Thais 5 years of age or older who are selected by multi-stage random sampling.However,during periods of COVID-19 restrictions,the SPA surveys were conducted online.
This study uses a nationally representative sample of Thais who have access to the internet (85% of Thai population).To reduce bias occurring due to under-representation of the population who cannot access the internet,the proportion of samples in this study was designed to be similar to the general Thai population.The online population was estimated using data from the National Statistical Office and classified by province of residence.The study population was drawn from Facebook members using probability random sampling,with inclusion criteria of having discrete gender/sex on their profile page.We also considered the representativeness of Thais from different occupations and levels of education.The research team sampled Facebook open groups and invited participants to join the study.A total of 6756 individuals from SPA2019-2020 and 6620 from SPA2021,all of whom were 18 years of age or older,were included in the analysis.
2.2.Measurement
PA was assessed subjectively by asking respondents to estimate the level and intensity of their PA and enter their responses into a LimeSurvey web application.The online questionnaire was adapted from the Global Physical Activity Questionnaire(Version 2.0)26and translated into Thai.For the main analysis,PA in this study is expressed as the average cumulative minutes of MVPA weekly.
PA recovery was defined as the ability of individuals to return to their pre-pandemic levels of PA.This variable,called the“recovery rate”,was calculated from the relative difference in the cumulative minutes of MVPA in 2 different periods,i.e.,2021 compared to the base year(2019).We also calculated the“recession rate” by subtracting cumulative absolute minutes of MVPA in 2020 from the base year (2019).The year 2020 was selected for comparison to the baseline because PA significantly dropped during this period due to the harsh,mandatory measures ordered by the Thai government to contain COVID-19.4The grouping and categorization of recession (high,medium,and low) and recovery (fast,medium,and slow) were made based on the distribution of cumulative minutes MVPA data.We also drew the interaction between recession and recovery rates and plotted them into the following 9 zones:(I)low recession and fast recovery,(II)medium recession and fast recovery,(III) high recession and fast recovery,(IV) low recession and moderate recovery and (V) medium recession and moderate recovery,(VI) high recession and medium recovery,(VII) low recession and slow recovery,(VIII)medium recession and slow recovery,as well as(IX)high recession and slow recovery.The higher zones were designated to the critical groups,indicated by a higher level of recession and slower speed of recovery.
2.3.Data analysis
To analyze temporal variation of PA in different periods,we compared the PA level between 2019 and 2021 and categorized the changes into 4 trajectories: (1) improved PA,(2) remained active,(3) remained inactive,and (4) declined PA.Correlates included in the analysis are comprised of sociodemographic characteristics,e.g.,sex(male or female),education (primary or less,secondary,or post-secondary);occupation (student,agriculture,private enterprise,formal sector,informal sector,or unemployed);monthly income;residential area (urban or rural);and region of residence (North,Central,Northeast,South,or capital/Bangkok).We defined urban as municipal areas and rural as local administrative areas (non-municipal areas).While sociodemographic characteristics refer to the current situation (at the time the survey was undertaken),we also collected information on respondents’health status from the prior year.We asked them whether they had a debilitating NCD or condition in the present (2020) and whether they also had it in the previous year (2019).Similarly,for mental health status,we asked the respondents to rate their current anxiety level,ranging from 0(no anxiety) to 5 (very severe anxiety),then asked them to compare that retrospectively to the past year(prior to the emergence of the COVID-19 pandemic).We also asked respondents(in 2021 only)whether they had ever been diagnosed with COVID-19.We included 3 enabling factors of PA participation: whether the respondent has a positive attitude towards PA (meaning they perceive PA as important for their health),whether they have been exposed to the government’s “Fit from Home”campaign,and whether they have a built environment for PA available in their neighborhood.
Descriptive analysis was used to illustrate the recovery shape and the interaction between recession and recovery rate.To identify the depth of recession in PA and the speed of recovery for each group,multivariate analysis with binary logistic regression was employed to determine factors correlated with PA changes in 4 trajectories.We included sociodemographic characteristics,health status (whether respondents have NCDs and have been infected with COVID-19),anxiety,and enabling factors of PA participation in 2020 as correlates in the models.
All participants provided informed consent prior to their involvement in the study.The research team ensured the confidentiality of the information provided by participants and explained the right of each individual to participate or withdraw from the study at their convenience.The protocol of the study followed local government regulations and was approved by the ethical review board of the Institute for Population and Social Research of Mahidol University,Certificate of Ethical Approval(COA),No.2020/04-190(SPA2020),and 2021/05-114(SPA2021).
3.Results
In all rounds of the SPA,the study population was a nationally representative sample with over 6000 individuals.The proportion of sexes was almost equal in SPA2019-2020,but a slightly higher proportion of females (51.7%) was found in SPA2021.The vast majority of the sample in SPA2019-2020 were young adults (52.3%) and middle-aged adults (44.4%),with a low proportion of older adults(3.3%).SPA2021,on the other hand,contained a larger proportion of older adults (i.e.,aged 65 years or over)(14.4%).About half the sample in each of the 3 rounds attained some formal education,but the proportion with primary education was the highest (17.4%) in SPA2021.Around one-third of the sample (32.3%-33.8%)was employed in the formal sector,whereas 17.1%-21.2% was employed in the informal sector and private enterprises(Table 1).
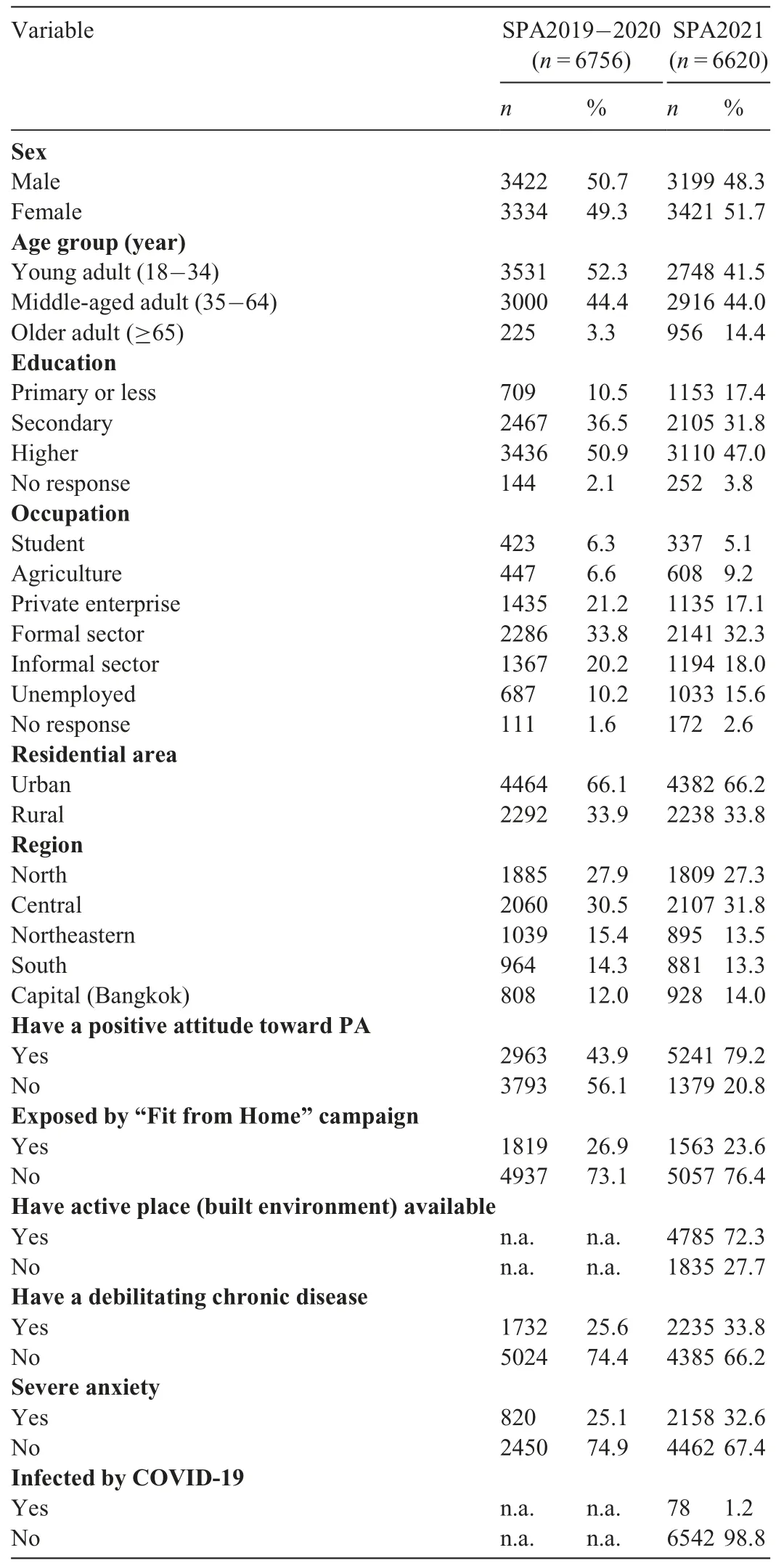
Table 1 Sample characteristics of SPA2019-2021.
The proportion of the sample by residence (urban/rural,region)was similar across the 3 rounds.However,there was a significant difference in the proportion of the sample with a positive attitude toward PA (79.2% in SPA2021vs.43.9% in SPA2019-2020).The proportion of the sample exposed to the government’s PA awareness campaign across the 3 rounds was also quite similar(26.9%in SPA2019-2020vs.23.6%in SPA2021).Nevertheless,only SPA2021 collected information on the availability of a built environment for PA.A slightly higher proportion of the sample reported an NCD or other debilitating condition in SPA2021 (33.8%) as compared to previous rounds (25.6%).Similarly,the proportion of the sample with a severe level of anxiety was also slightly higher(32.6%) in SPA2021 than in the previous 2 rounds (25.1%).Only 1.2% of the sample reported ever being diagnosed with COVID-19 as of SPA2021(Table 1).
3.1.PA recovery shape
The average cumulative minutes (min) of MVPA dropped significantly,from 685 min in 2019 to 506 min in 2020,and remained low,at 513 min,in 2021.The proportion of the population with sufficient MVPA also declined from 69.7%in 2019 to 56.7% in 2020.With an intensified health promotion campaign in the later period,the proportion of the population with adequate MVPA bounced back to 65.3% in 2021,whereas the rest(4.4%)were unable to resume their PA to prepandemic levels(Table 2).
PA recovery in the Thai population resembles an imperfect V shape,indicating a sharp decline followed by an immediate upturn.Despite the recovery,PA has not been resumed at prepandemic levels.The overall and recovery rate classified by population characteristics (Fig.1) showed a similarity in pattern (V-shaped) but differed in the level of recession and recovery.
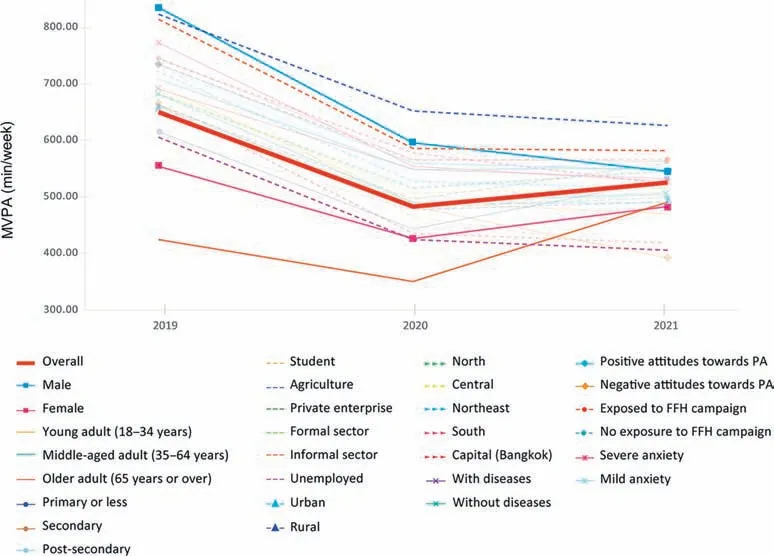
Fig.1.PA recovery shape.FFH=Fit from Home;PA=physical activity.
Before the pandemic(2019),males accumulated the highest MVPA,followed by individuals who were employed in the agricultural sector (Fig.1).In general,Thai males have a higher level of PA,both in terms of the proportion of sufficient MVPA and average cumulative MVPA per week.Compared to females,the proportion of males with sufficient MVPA was higher in all 3 rounds of SPA.Nevertheless,males also experienced a drastic drop in their average cumulative MVPA,from 834.47 min in Retrospective 2019 to 594.51 min in SPA2020 and 544.15 min in SPA2021(Table 2).
Individuals employed in the agricultural sector ranked second highest in PA levels before the COVID-19 pandemic.They experienced the slightest decline during the harshcontainment measures in 2020 and attained the top PA level by 2021 (Fig.1).Among individuals with different occupations,those who worked in the agricultural sector accumulated the greatest amount of MVPA in all 3 rounds of SPA(822.24 min,651.08 min,and 625.59 min per week in 2019,2020,and 2021,respectively)(Table 2).
A V shape pattern with a narrow slope for older Thai adults(i.e.,≥65 years of age) indicates an immediate upturn or recovery.Although seniors were ranked last during 2019-2020,this group experienced a significant and immediate increase in 2021(Fig.1).Compared to other age groups,older adults accumulated the lowest amount of MVPA in 2019-2020 (423.56 min and 349.25 min,respectively) but were able to recover more than young adults in 2021(Table 2).Females were initially at the lowest end of the groups for baseline PA.Although they also experienced a decline in PA during the COVID-19 pandemic,the recession slope was not as sharp as for males(Fig.1).Average cumulative MVPA for females declined from 555.87 min in 2019 to 428.29 min in 2020 and slightly increased to 484.40 min in 2021(Table 2).
3.2.Recession and recovery rate of PA in the Thai population:Levels and patterns
In this study,the PA recession rate was calculated from the difference of cumulative minutes of MVPA between 2020 and 2019.The PA recovery rate was calculated from the relative difference in the average cumulative minutes of MVPA between 2021 and the base year(2019).Overall,Thais experienced a medium level of recession (-26.1%) and moderate level of recovery (37.44%) (Table 3).The highest recession rate was experienced by students (-36.9%) and residents of Bangkok (-34.4%).Older adults,individuals with an NCD,and those who were employed in agriculture experienced the lowest recession rates (-17.5%,-20.5%,and -20.8%,respectively).Older adults were the only group to experience a fast recovery rate (57.75%).Students,those with a negative attitude toward PA,and residents of Bangkok were among the slowest to recover,with rates of 27.09%,29.46%,and 31.51%,respectively(Table 3).
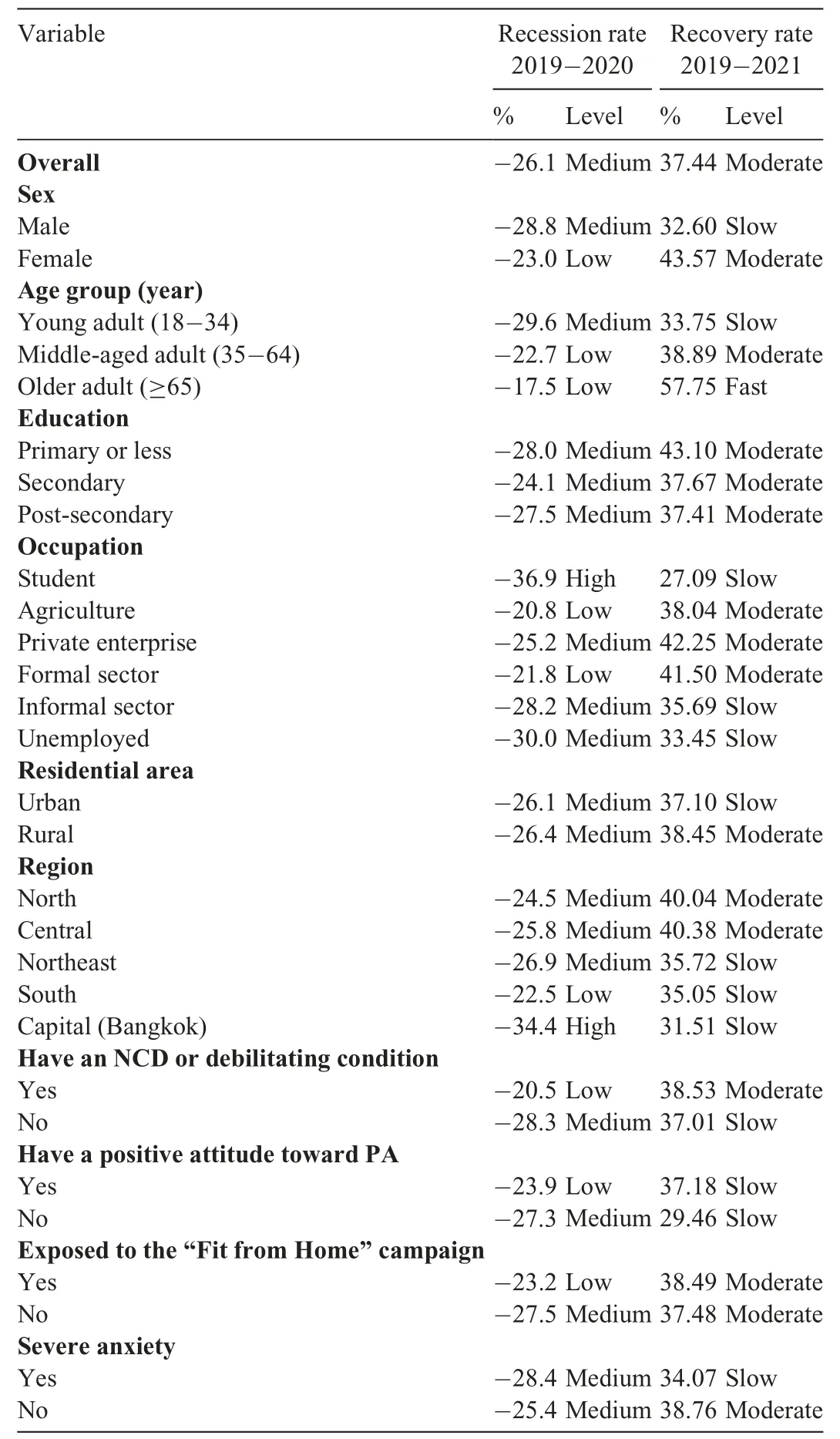
Table 3 Recession and recovery rate in PA of the Thai population:2019-2021.
Fig.2 shows the 9 zones of recession and recovery based on population characteristics.Zoning was aimed at identifying groups in the population who would require assistance in resuming their baseline levels of PA.The higher zones indicate where assistance is needed most,i.e.,those who experienced the greatest recession and slowest recovery.Attention should be paid to the bottom left(high recession,slow recovery,Zone IX) as this group experienced a significant drop in their PA followed by a sluggish recovery.Students and residents of Bangkok(Zone IX)were shown to be the most affected populations and the ones who experienced greater difficulty in attaining their pre-pandemic PA levels (Fig.2).Those who were on the borderline between Zones VIII and IX (young adults,unemployed) were also among the disadvantaged groups.Males experienced a medium recession and slow recovery rate (Zone VIII),as did residents of the Northeast region and individuals working in the informal sector.
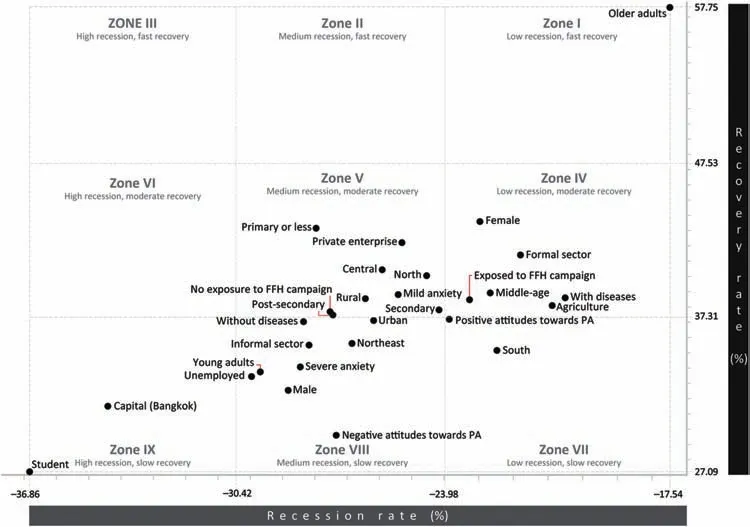
Fig.2.Zoning the recession and recovery rates of PA in the Thai population.(I)Low recession and fast recovery,(II)medium recession and fast recovery,(III)high recession and fast recovery,(IV) low recession and moderate recovery,(V) medium recession and moderate recovery,(VI) high recession and medium recovery,(VII)low recession and slow recovery,(VIII)medium recession and slow recovery,and(IX)high recession and slow recovery.FFH=Fit from Home;PA=physical activity.
Recession and recovery rates also corresponded with health-related and information factors.The COVID-19 pandemic showed a more adverse impact on the PA of those with severe levels of anxiety,shown by a medium level of recession and slow recovery rate (Zone VIII).Compared to those without,individuals with a debilitating NCD showed a better PA level with low recession and moderate recovery(Zone IV),likely because they were more concerned with their health than were healthy individuals (Zone VIII).Individuals with a positive attitude toward PA who were exposed to training/PA campaigns seem to have benefited from the information,as their PA declined less than those with a negative attitude who had no PA promotion exposure.Both positive and negative attitudes were associated with a slow recovery rate,and these individuals saw a moderate level of recovery whether or not they were exposed to PA training guidelines.
Most Thai adults were concentrated around medium recession (between -24.0% and -30.4%) and moderate recovery(between 37.3% and 47.5%).Middle-aged adults,females,those who work in the agricultural or formal sectors,and those with an NCD were among the groups located in Zone IV (low recession and moderate recovery).The central zone (medium recession and moderate recovery,or Zone V) was occupied by those who had attained a primary education or less,who were employed in private enterprise,or who resided in a rural area or the North or Central regions of Thailand.Those who attained secondary or post-secondary education or who resided in an urban area were on the border between Zones V and VIII,indicating that their PA dropped to a medium level but recovered at a moderate or slow pace.The group of older adults was the only group in the study population assigned to Zone I.They experienced the lowest recession and fastest recovery.No subgroup of the sample in this study occupied Zones II or III.
3.3.Factors associated with PA transition in 4 trajectories
Binary logistic regression was employed to determine factors associated with the PA transition in 4 trajectories: (1)improved PA,(2) remained active,(3) remained inactive,and(4) declined PA.The determination of trajectories was made by calculating the changes in PA level from 2 different periods(2019-2021).We included the identical covariates from 2020 and tested the associations of those factors with the 4 PA trajectories as dependent variables.
Most individual factors (biology or socioeconomic) had no significant correlation with improved PA in the post-COVID period.In Model 1 (improved PA),most of the significant correlates were related to health status,attitude toward PA,and region of residence as proxy for local government policy to control the spread of COVID.Relative to those with negative attitudes towards PA,individuals with a positive attitude toward PA were more likely to improve their PA in 2021(odds ratio (OR)=6.895,95% confidence interval (95% CI):5.287-8.993;p=0.000).Individuals who had ever been diagnosed with COVID-19 (compared to those who had never been) were also more likely to have an improved PA(OR=2.089,95% CI: 1.287-3.413;p=0.003).Individuals who resided in Northeast (OR=1.494,95% CI:1.165-1.915;p=0.002),North (OR=1.465,95% CI: 1.174-1.829;p=0.001),South (OR=1.462,95%CI: 1.142-1.873;p=0.003),or Central (OR=1.331,95%CI: 1.072-1.653;p=0.010)Thailand were more likely to improve their PA than those who lived in Bangkok.The chances of having better PAin 2021 were also higher among individuals who were exposed to PA campaigns/training guidelines (OR=1.400,95% CI:1.222-1.605;p=0.000),those who had PA facilities/built environments available in their neighborhood (OR=1.263,95% CI:1.090-1.462;p=0.002),and those who suffered from a debilitating NCD (OR=1.179,95% CI: 1.032-1.347;p=0.015).One of the barriers to improving PA(as captured in Model 1) is mental health status.Individuals with severe levels of anxiety were 26% less likely to have better PA(OR=0.740,95% CI:0.647-0.847;p=0.000)than those who had mild or no anxiety.
In Model 2,the likelihood of remaining active in 2021 was highest among individuals with a positive attitude toward PA(OR=2.093,95% CI: 1.819-2.408;p=0.000),followed by those whose occupation was in agriculture (OR=1.294,95% CI:1.049-1.597;p=0.016)and those who resided in the South (OR=1.513,95% CI 1.235-1.854;p=0.000),Northeast(OR=1.305,95% CI:1.064-1.601;p=0.011),and North(OR=1.259,95%CI: 1.052-1.507;p=0.012) of the country.The availability of built environments (i.e.,PA facilities) also helped individuals stay active (OR=1.230,95% CI:1.093-1.385;p=0.001).Individual factors such as age,educational attainment,anxiety,and having a debilitating NCD served as barriers to staying active(Model 2).
The likelihood of remaining in an inactive state (Model 3)was higher among individuals with severe levels of anxiety(OR=1.700,95% CI: 1.502-1.952;p=0.000),a postsecondary education (OR=1.484,95% CI: 1.217-1.809;p=0.000)or a secondary education only(OR=1.297,95% CI:1.067-1.575;p=0.009),and among those who were middleaged adults (OR=1.172,95% CI: 1.022-1.343;p=0.023).In the fourth trajectory (Model 4),declined PA was positively associated with anxiety,attaining post-secondary education,and being middle-aged.Conversely,declined PA was negatively associated with occupation (agriculture,informal sector),region of residence,positive attitude toward PA,availability of PA facilities,history of COVID-19 diagnosis,and suffering with a debilitating NCD.
Age,educational attainment,and mental health status are among the consistent predictors of PA in 3 trajectories(Models 2-4).Middle-aged adults,individuals who attained post-secondary education,and those with severe levels of anxiety were less likely to stay active,more likely to remain inactive,or more likely to have declined PA in 2021 (Fig.3).Region of residence and positive attitude toward PA were positive determinants for an improved or stable active state(Models 1 and 2,respectively).Region of residence and positive attitude toward PA were negative determinants for remaining inactive (Model 3) and declining PA (Model 4).Individuals who resided in the North,Northeast,or South and those who had a positive attitude toward PA were more likely to improve their PA or stay active during COVID-19 containment measures in 2021,and they were less likely to be inactive compared to their counterparts who resided in the capital city(Bangkok) or who had a negative attitude toward PA.Having a debilitating NCD was not a consistent predictor of PA;it served as a positive correlate for being in an improved state but a negative correlate for remaining active.The built environment served as a positive correlate for being in an improved-or remained-active state,a negative correlate with declined PA,and it was not a significant predictor for remaining in an inactive state.COVID-19 status (having ever been diagnosed with the infection),on the other hand,was a significant predictor of improved and declined PA (Models 1 and 4)but was not significant in the other models.Area of residence(urban/rural)was not a significant factor in any of the 4 trajectories.
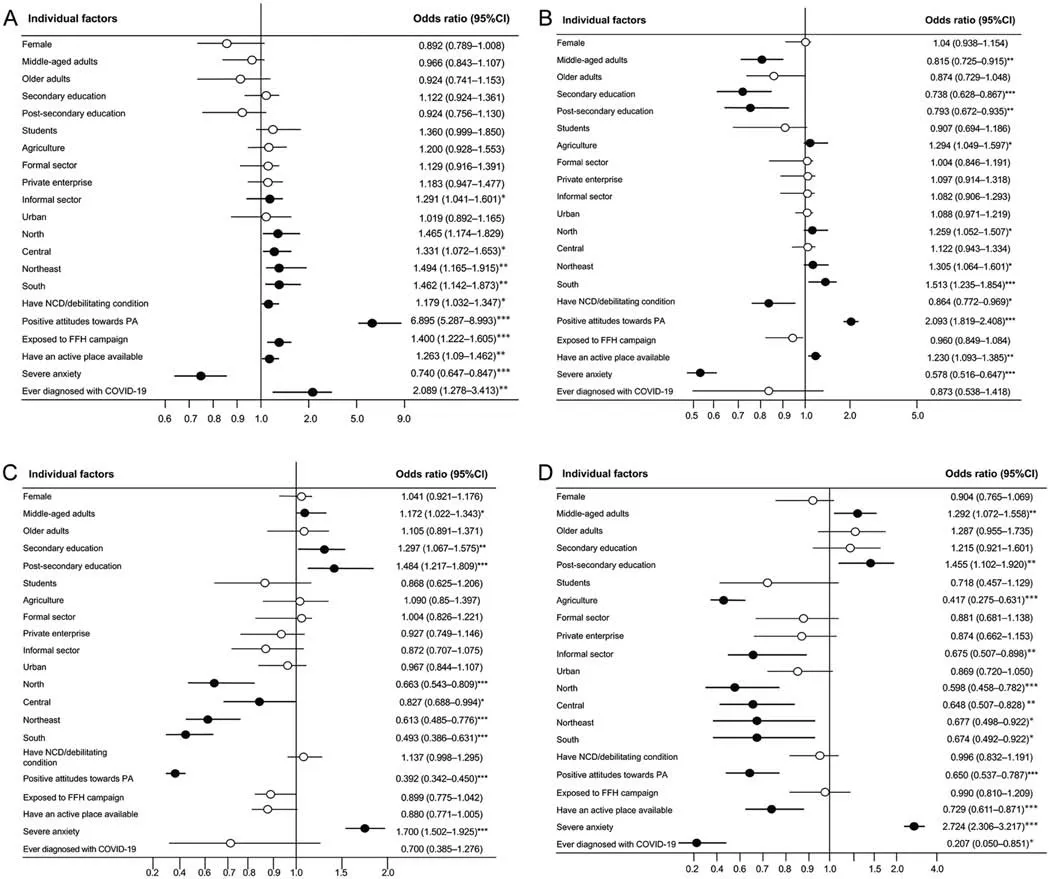
Fig.3.Factors associated with PA transition in 4 trajectories:(A)improved PA,(B)remained active,(C)remained inactive,and(D)declined PA.Reference group are males,young adults,primary education or lower,unemployed,rural,Bangkok,without NCD,negative attitudes towards PA,no exposure to“Fit from Home”campaign,built environment(place to be active)is not available,no or with mild level of anxiety,and never been infected with COVID-19,respectively.○means insignificant and · means significant.* p=0.05,** p=0.001,*** p<0.001,compared with reference group.95% CI=95% confidence interval;COVID-19=coronavirus disease 2019;FFH=Fit from Home;NCD=non-communicable disease;PA=physical activity.
4.Discussion
With COVID-related restrictions ordered by central and local governments,the Thai population experienced a significant decrease in their PA in the wake of the pandemic.The average reduction in cumulative MVPA per week during 2020-2021 was 3 h;this was accompanied by a decline in the proportion of the population with sufficient PA.A decline in PA during the COVID-19 pandemic was also reported worldwide,with a wide range of reductions(e.g.,from 30 min to >3 h).2,6,19,27With a medium level of recession (-26.1%) and a moderate recovery speed (37.44%),PA recovery in the Thai population resembled a V shape,with a sharp decline followed by an immediate upturn.It should be noted,however,the current figure does not depict a perfect V shape with a narrow slope.This means the recovery of the state of PA in 2021 was incomplete.The imperfect V shape also suggests the future of PA recovery is indeterminate: it may complete a perfect V shape or we may see another downturn,resulting in a W shape.
The quick recovery among older adults was somewhat surprising because many studies have found seniors to be the most vulnerable sub-group of the population to COVID-19.In other countries,older adults experienced a significant decline in PA28,29and were at higher risk for anxiety and other mental health problems due to COVID containment measures,which restricted movement and increased social isolation.30-32In the case of older Thai persons,however,there are several possibilities that might explain their quick recovery.
4.1.Resilience
Older Thai adults practiced good COVID prevention and had an overall sense of well-being,economic security,and life satisfaction during the pandemic.Studies found that older persons who had good social capital and a supportive environment found alternatives to their larger social network by engaging with family more and limiting themselves to neighborhood activities,home-based/indoor PA,gardening,etc.33,34
4.2.Community support
There is evidence that targeted government/community support helped older Thai adults adapt and cope with the COVID containment measures.35,36As a country with a rapidly aging society,Thailand has been preparing its health system to provide more assistance to older persons and designated seniors,and they were a priority group during the COVID-19 pandemic.
Students,young adults,residents of Bangkok,the unemployed,and those who had a negative attitude toward PA experienced the highest recession and were among the slowest to recover.Students and young adults were severely affected by the mandatory shift from classroom to online learning and the work-from-home edicts,which forced individuals to spend more time sitting at a desk and focusing on a computer screen.27,37However,it should be noted that,even before the pandemic,adolescents were considered the least active group of the population.38Working from home also reduced PA opportunities for working-age young adults who usually collected most of their daily PA minutes from work-and commuter-related activities.39Failure to adjust to the “new normal” has further delayed the recovery of these 2 groups.Although the national health promotion campaign(“Fit from Home”)was intensified,the PA of these 2 groups had not returned to pre-pandemic levels by the 2021 round of the survey.4
Bangkok residents were also among those most affected by stringent COVID containment measures,as several outbreaks were traced to various entertainment and shopping venues in and around the capital city.4The high recession of PA and slow recovery were generally caused by harsh measures meant to contain the virus and the closure of PA amenities.18Unemployed individuals were among the most vulnerable during the pandemic(high recession and slow recovery),as they suffered from economic deprivation and were exposed to an elevated risk of infection due to their crowded living conditions.PA was likely not a priority for this group given their struggle to survive and cover daily expenses.18Finally,those who already had a negative attitude toward PA were further demotivated during the COVID-19 pandemic.40,41
While many older adults were able to bounce back immediately after restrictions on movement and socialization were relaxed,middle-aged adults,individuals with secondary or post-secondary education,and those with severe anxiety were less likely to stay active,more likely to remain inactive,or more likely to have declined PA in 2021.With the closure of non-essential businesses,office workers relied on screen-mediated meetings and remote work,which involved long periods of stationary sitting.39Even after work-from-home edicts were lifted,this group of sedentary working-age adults still relied on work-related PA (i.e.,commuting) as the main contributor to their daily PA minutes.39Individuals with severe anxiety had more trouble bouncing back because their fear of COVID deterred them from engaging in PA outside the home or neighborhood.Most probably did not have PA facilities or equipment in their home environment and,thus,self-isolation due to COVID thwarted PA,even if those persons were motivated to be more active.Studies found that individuals with severe anxiety or depression had a low level of PA during the COVID pandemic and that individuals with a low level of anxiety demonstrated a stronger motivation for PA.42,43
Individuals employed in agriculture are among those who successfully maintained their PA level during the COVID pandemic.Rural areas had less restriction of movement than Bangkok and many other urban areas,which increased confinement measures due to high infection rates.4,18In addition,individuals who worked in agriculture were more likely to be able to carry out their routine farming and maintain their work-related PA during 2020-2021.
Gender inequality in PA is a worldwide phenomenon,as previously established.16,44Compared to women,men generally have a higher level of PA,both in terms of cumulative MVPA per week and in terms of the proportion meeting a sufficient quota of PA.As expected,men in this study accumulated more minutes of MVPA than women in all 3 survey rounds,but they also experienced a higher recession in their average cumulative MVPA in 2020-2021.This finding indicates that men were more adversely affected by the pandemic restrictions with respect to PA,as they lost access to gyms,organized/team sports,and other outdoor PA opportunities.Men may have been especially slow to recover because of their “outdoor nature”—that is,because they are more likely to look for outdoor PA opportunities,which were limited by periods of confinement and the need to practice social distancing.18
The findings of this study suggest that more attention should be paid to the groups in Zones IX and VIII (highest drop in the PA level and the slowest to recover).These groups include students,young adults,residents of Bangkok,the unemployed,and those who had a negative attitude toward PA.It also should be noted that a substantial portion of the population were unable to resume their PA even after government restriction measures were eased or lifted altogether.2,4Previous findings also found a weak positive association between prolonged sedentary behavior and lower levels of PA among adults.45Without a proper program and intervention,individuals who became accustomed to pandemic control measures may have lost the motivation or habit to resume their pre-pandemic PA routine.
This study owes its strength to the time series of data.The recession and recovery rates were observed over 3 rounds of collection.This enabled us to compare a pre-COVID assessment (2019) with PA during periods of intense state-ordered containment(2020)and then with the period of gradual easing of restrictions on travel and social distancing (2021).The national representativeness of the sample is also a strong point of this study.The conclusions of this study can be generalized to represent the PA recovery rate of adults in Thailand and,perhaps,other countries with similar characteristics.More important,the findings of the study showed which groups in the population are at a disadvantage,which ones experienced significant barriers to resuming their PA,and which would require assistance in returning to their pre-COVID PA levels.Despite these strong points,several weaknesses from the study should also be acknowledged.PA was measured subjectively by self-reported information and could be biased.However,it is not possible to say whether the findings are an over-or under-estimation of PA levels.In addition,the sample was limited to persons 18 years of age or older who have access to the Internet.Also,the built environment could not be assessed in 2020 due to the heightened pandemic measures.Finally,PA was not differentiated by its domains(work-related,transport,or recreational) and,therefore,the recommendations provided only address declines in overall PA.
5.Conclusion
While most Thai adults experienced a moderate level of recession in PA and a moderate speed of recovery,a substantial proportion of Thais experienced significant barriers in returning to their pre-COVID level of PA.Biological and socioeconomic inequality (e.g.,age,education,occupation)contribute to some variance in the recovery rate of the population,as do differences in local government mandates,employer requirements,and social norms.While the effect of the COVID containment measures on PA was temporary,the slow recovery rate was caused by a combination of lingering restrictions and socioeconomic inequalities that require more time and effort to overcome.
The findings of the study indicate that changes in the PA of Thai adults during the pandemic were largely determined by preventive behaviors demonstrated by certain groups within the population who have higher awareness and concern about their health.The members of the population who improved their PA are those with a high level of resilience (e.g.,older adults),and those who remained active despite the lockdowns and curfews are most likely those who have higher self-efficacy and awareness of the importance of PA as a health-promoting activity(i.e.,those with a positive attitude toward PA).This is especially important for the more vulnerable populations (e.g.,persons with an NCD or other debilitating condition).Individuals who remained inactive before and during the COVID pandemic are most likely those with less health awareness.Those who experienced PA declines are also those who were most adversely affected by the COVID containment measures,those who had lower adaptability,and those who had less exposure to health information.The findings of the study suggest that these latter groups (highest recession and slowest recovery,Zones VIII and IX) are the ones who need immediate and sustained assistance to restore their PA to pre-pandemic levels or better.
Acknowledgment
The authors gratefully acknowledge funding support from the Thai Health Promotion Foundation with grant numbers 63-00030 and 64-00139.
Authors’contributions
PK conceptualized and designed the study,performed formal data analysis,interpreted the findings,and drafted the manuscript;DAW conceptualized and designed the study,interpreted the findings,drafted the manuscript,and finalized the manuscript;NH performed formal data analysis;AK performed data analysis;SP designed the visualization of the findings.All authors reviewed and contributed to the final manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
 Journal of Sport and Health Science2023年4期
Journal of Sport and Health Science2023年4期
- Journal of Sport and Health Science的其它文章
- Beyond cardiomyocytes:Cellular diversity in the heart’s response to exercise
- COVID-19:Insights into long-term manifestations and lockdown impacts
- Exercise training attenuates angiotensin II-induced cardiac fibrosis by reducing POU2F1 expression
- Specific alterations of regional myocardial work in strength-trained athletes using anabolic androgenic steroids compared to athletes with genetic hypertrophic cardiomyopathy
- Effects of exercise by type and duration on quality of life in patients with digestive system cancers:A systematic review and network meta-analysis
- Sports compression garments improve resting markers of venous return and muscle blood flow in male basketball players