
Cross-sectional associations between cortical thickness and physical activity in older adults with spontaneous memory complaints:The MAPT Study
2023-06-06 13:35myRaffinYvesRollandbClaraFisherJeanFranoisManginAudreyGabelleBrunoVellasbPhilipedeSoutoBarretobfortheMAPTDSAGroup
Jérémy Raffin*,Yves Rollandb,Clara Fisher,Jean-François Mangin,Audrey Gabelle,Bruno Vellasb,Philipe de Souto Barretob,for the MAPT/DSA Group
a Gérontopôle de Toulouse,Institut du Vieillissement,Centre Hospitalo-Universitaire de Toulouse,Toulouse 31000,France
b Université Paul-Sabatier/Institut National de la Santé et de la Recherche Médicale Unité Mixte de Recherche 1027,Faculté de médecine,University of Toulouse III,Toulouse 31000,France
c Centre pour l’Acquisition et le Traitement des Images Multicenter Neuroimaging Platform,Neurospin,Université Paris-Saclay,Gif sur Yvette 91191,France
d Memory Resources and Research Center,Montpellier University Hospital,Montpellier 34295,France
e Institut National de la Santé et de la Recherche Médicale Unité 1061 i-site Montpellier Université d’Excellence,University of Montpellier,Montpellier 34090,France
Abstract Background: Age-related changes in brain structure may constitute the starting point for cerebral function alteration.Physical activity (PA)demonstrated favorable associations with total brain volume,but its relationship with cortical thickness(CT)remains unclear.We investigated the cross-sectional associations between PA level and CT in community-dwelling people aged 70 years and older.Methods: A total of 403 older adults aged 74.8±4.0 years(mean±SD)who underwent a baseline magnetic resonance imaging examination and who had data on PA and confounders were included.PA was assessed with a questionnaire.Participants were categorized according to PA levels.Multiple linear regressions were used to compare the brain CT(mm)of the inactive group(no PA at all)with 6 active groups(growing PA levels)in 34 regions of interest.Results: Compared with inactive persons,people who achieved PA at a level of 1500-1999 metabolic equivalent task-min/week (i.e.,about 6-7 h of brisk walking for exercise and those who achieved it at 2000-2999 metabolic equivalent task-min/week(i.e.,8-11 h of brisk walking for exercise) had higher CT in the fusiform gyrus and the temporal pole.Additionally,dose-response associations between PA and CT were found in the fusiform gyrus (B=0.011,SE=0.004,adj. p=0.035),the temporal pole (B=0.026,SE=0.009,adj. p=0.048),and the caudal middle frontal gyrus,the entorhinal,medial orbitofrontal,lateral occipital,and insular cortices.Conclusion: This study demonstrates a positive association between PA level and CT in temporal areas such as the fusiform gyrus,a brain region often associated to Alzheimer’s disease in people aged 70 years and older.Future investigations focusing on PA type may help to fulfil remaining knowledge gaps in this field.
Keywords: Alzheimer’s disease;Brain aging;Cortical thickness;Physical activity
1.Introduction
Cerebral aging is characterized by both macrostructural and microstructural alterations such as brain volume reduction,1-3white matter shrinkage,4β-amyloid deposition,5and cortical thinning.6-8These alterations likely impact sensory processing,9motricity,10,11or cognition.12-15Cross-sectional data suggest that cortical thickness (CT) starts reducing from the age of 30 years,particularly in the inferior parietal and in the medial and lateral frontal regions,before extending to the whole brain.16This decrease of CT accelerates after the age of 60,especially in areas prone to Alzheimer’s disease (AD),such as the entorhinal cortex,the fusiform gyrus,and the middle temporal gyrus.5,8Moreover,greater cortical thinning has been prospectively associated with subsequent onset of cognitive impairment,17indicating that developing strategies for preserving CT may help to prevent brain function alterations in older adults.In this respect,keeping a physically active lifestyle during late adulthood could represent an effective approach for maintaining cortical structure during aging.18
Both observational and interventional investigations in older people have demonstrated that regular physical exercise not only favorably affects cognitive functions19and cerebral metabolism20but also exerts a beneficial impact on brain volume and structure.21,22Magnetic resonance imaging(MRI)studies have shown that young athletes23and physically active older adults24have higher values of CT and a slower rate of cortical thinning over time25,26compared to inactive,age-matched people.However,the literature is disparate in regard to these associations in healthy older people,with some studies demonstrating favorable associations in the frontal lobes24,25and others reporting that higher levels of physical activity(PA)are associated with greater CT in the parietal and temporal areas.26Furthermore,in these studies the dichotomization of PA levels,defined as “high” or “low”,limits the recommendations that can be made concerning the dose of PA required to prevent the age-related cortical atrophy.Additionally,exercise training interventions have demonstrated positive correlations between cardiorespiratory fitness and CT,27,28suggesting a dose-response relationship between PA and CT through the mediation of cardiorespiratory capacity.Thus,evidence regarding the volume of PA needed to slow down cortical thinning during aging remains unclear,and discrepancies about which cortical regions are associated with PA in older adults persist.
The main objective of our cross-sectional study was to determine the minimal amount of PA that is significantly associated with higher CT,as well as the PA-CT dose-response association,in adults aged 70 years and older with spontaneous memory complaints.Secondly,we aimed to identify the cortical regions that are related to PA in this population.
2.Methods
The MRI ancillary study data from the randomized controlled Multidomain Alzheimer’s Preventive Trial(MAPT)(clinicaltrials.gov;NCT00672685) were used.29The parent MAPT study demonstrated no significant effect of 3 years of omega-3 polyunsaturated fatty acid (PUFA) supplementation with or without multidomain intervention(consisting of nutritional and PA counseling plus cognitive training,)on cognition in adults aged 70 years and older who were free from dementia,compared to a placebo control group.30The MAPT study,as well as the MRI ancillary study,were approved by the Advisory Committee for the Protection of Persons Participating in Biomedical Research of Toulouse.Written informed consent was provided by all participants.
2.1. Study population
Participants in the MAPT study(n=1679)were dementia-free older adults aged 70 years and older and met one or more of the following criteria: spontaneous memory complaint,limitation in 1 instrumental daily-living activity,and slow gait speed (≤0.8 m/s).Individuals were not included if they had a Mini-Mental State Examination score lower than 24,a diagnosed dementia,difficulties in carrying out basic activities of daily living,or supplementation in PUFA.The subpopulation used in this study was restricted to the 501 volunteers who had baseline MRI assessment.MRI assessments were performed throughout the first year of MAPT.The PA data,as well as information regarding confounders,were obtained at the clinical visit closest to the MRI scan.The mean time interval between the baseline MRI scan and the closest clinical visit was 41± 25 days(mean±SD).
2.2. MRI acquisition and analyses
Baseline brain MRI scans (Philips Achieva 3T;Philips,Amsterdam,Netherlands;Siemens Avanto 1.5T and Trio Tim 3T;Siemens Healthcare,Erlangen,Germany;and GE Signa 1.5T;GE Healthcare,Chicago,IL,USA)were performed in 9 city centers(Bordeaux,Dijon,Foix,Limoges,Lyon,Montpellier,Nice,Tarbes,and Toulouse) through a standardized protocol that was first tested on volunteers.The protocol included 3-dimensional T1-weighted,T2-turbo spin echo,T2-weighted gradient-echo,and T2-weighted fluid-attenuated inversion recovery sequences.T1-weighted images were processed using the open source software Freesurfer (Version 6.0.0;downloadable at https://surfer.nmr.mgh.harvard.edu/fswiki/DownloadAndInstall).Briefly,CT was estimated at each location of the cortex as the mean distance between vertices of grey-white matter boundary and grey matter/cerebrospinal fluid interface (pial) surfaces.This method has been previously detailed elsewhere.31,32Visual quality control was performed from 3D visualization of the surface models.An automatic parcellation of the cortical surface into 34 regions of interest (ROIs) in each hemisphere (Desikan-Killiany atlas) led to an aggregation of the thickness measurements.33Images assessed as being of poor or unreliable quality were excluded from the analysis.
2.3. Outcome measure
CT (mm) was the main outcome measure.Based on previously published works demonstrating significant associations between PA and CT in older adults,24,26,34we selected 10 primary ROIs according the Desikan-Killiany classification:35the superior frontal gyrus,the rostral middle frontal gyrus,the caudal middle frontal gyrus,the inferior parietal cortex,the precuneus cortex,the inferior temporal gyrus,the fusiform gyrus,the entorhinal cortex,the lateral occipital cortex,and the insula.For exploratory analyses,the remaining 24 supplementary areas were defined as secondary ROIs: the pars opercularis,the pars triangularis,the pars orbitalis,the lateral orbitofrontal cortex,the medial orbitofrontal cortex,the precentral gyrus,the paracentral lobule,the frontal pole,the superior parietal cortex,the supramarginal gyrus,the postcentral gyrus,the superior temporal gyrus,the middle temporal gyrus,the banks of the superior temporal sulcus,the transverse temporal cortex,the temporal pole,the parahippocampal gyrus,the lingual gyrus,the cuneus cortex,the pericalcarine cortex,the rostral anterior cingulate cortex,the caudal anterior cingulate cortex,the posterior cingulate cortex,and the isthmus cingulate cortex.The averaged values of the left and right hemispheres in each ROI were used for the analyses,as was previously done in recent studies using similar populations of subjects,whose average age was 70 years or older.26,36
2.4. PA assessment
PA levels were assessed using the Minnesota Leisure Time Activities questionnaire,37,38in which participants informed about the frequency and the duration of their household and leisure time physical activities performed during the previous 2 weeks.This questionnaire was validated against fitness tests(e.g.,maximal oxygen uptake and submaximal treadmill tests)in men and women,39-41with correlation coefficients between total PA volume and fitness test performance ranging from 0.39 for women41to 0.57 for men.40Test-retest reliability(correlation coefficients) for total PA ranged from 0.92(1-month reliability) to 0.69 (1-year reliability).39,42The weekly volume of PA was reported in metabolic equivalent task (MET) minutes per week (MET-min/week) and was calculated as follows:First,2 experienced raters independently estimated the intensity (in MET) of each reported PA based on the Compendium of Physical Activities.26Then,any moderate-to-vigorous-intensity PA (MVPA,≥3 METs) was multiplied by its frequency and duration,divided by 2 (METmin/week),and summed together to obtain the overall amount of PA (continuous variable).Low-intensity activities(<3 METs) were excluded from the computation because of their unsettled role in improving health in elderly people.43Participants were then classified into 7 categories according to their PA level: 0 MET-min/week,1-499 MET-min/week,500-999 MET-min/week,1000-1499 MET-min/week,1500-1999 MET-min/week,2000-2999 MET-min/week,and ≥3000 MET-min/week.
2.5. Confounders
Based on the literature,we selected the following as confounding variables: intracranial volume,age (continuous),sex,body mass index(continuous),cardiovascular risk factors(defined as having at least one of the following conditions—type 2 diabetes mellitus,hypertension,hypocholesterolemia,ischemic heart disease,and stroke history),apolipoprotein E(APOE) genotype (APOEε4 allele carrier or not),level of education (ordinal;no diploma,primary education,middle school education,high school education,or university diploma),and MAPT group allocation.
2.6. Statistical analyses
Descriptive statistics were provided in mean ± SD for continuous variables,while absolute numbers and percentages were used for categorical variables.Multiple linear regressions,providing unstandardized coefficients (B) and SE,were performed in order to investigate the associations between PA groups (reference category: inactive) and CT in each ROI.Additionally,the dose-response relationship between PA and CT was assessed with tests for linear trend by establishing PA level as an ordinal variable.Similar supplementary analyses were also performed separately in each hemisphere in order to explore any potential lateralization effect.The previously identified confounders were included in each model.All analyses were corrected for multiple comparisons using the Benjamin-Hochberg false discovery rate procedure,andpvalues were presented before and after adjustement.44All statistical analyses were performed using SPSS Statistics Version 23.0(IBM Corp.,Armonk,NY,USA),with a level of significance defined at adjustedp(adj.p)<0.05.
3.Results
3.1. Characteristics of the participants
A total of 501 participants in MAPT had a baseline MRI.Among these participants,21 presented poor or unreliable image quality and 77 had missing values in PA,CT,or confounding variables,leading to a total of 403 subjects with fully documented data.The demographic and clinical characteristics of the subjects are shown for the whole sample as well as for each group in Table 1.Significant differences were found in terms of sex,body mass index,and intracranial volume between the inactive group and the PA groups.
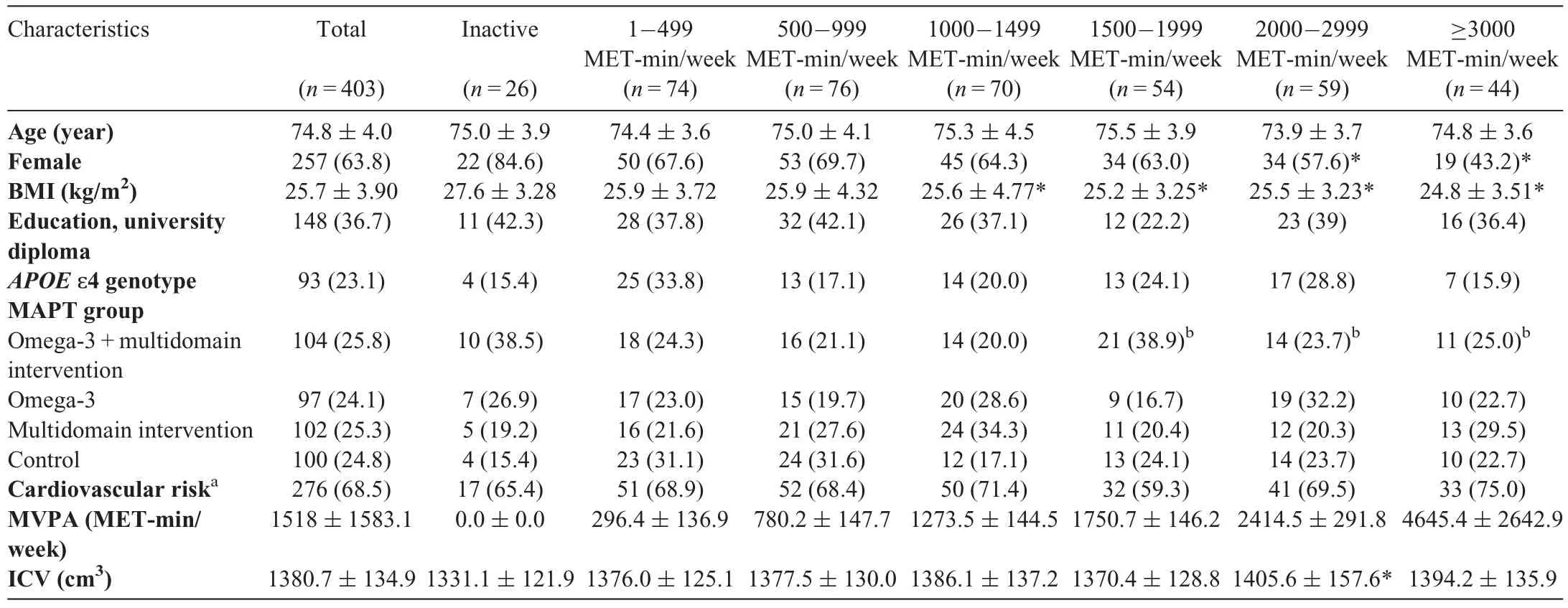
Table 1 Participants characteristics.
3.2. Association between PA levels and CT
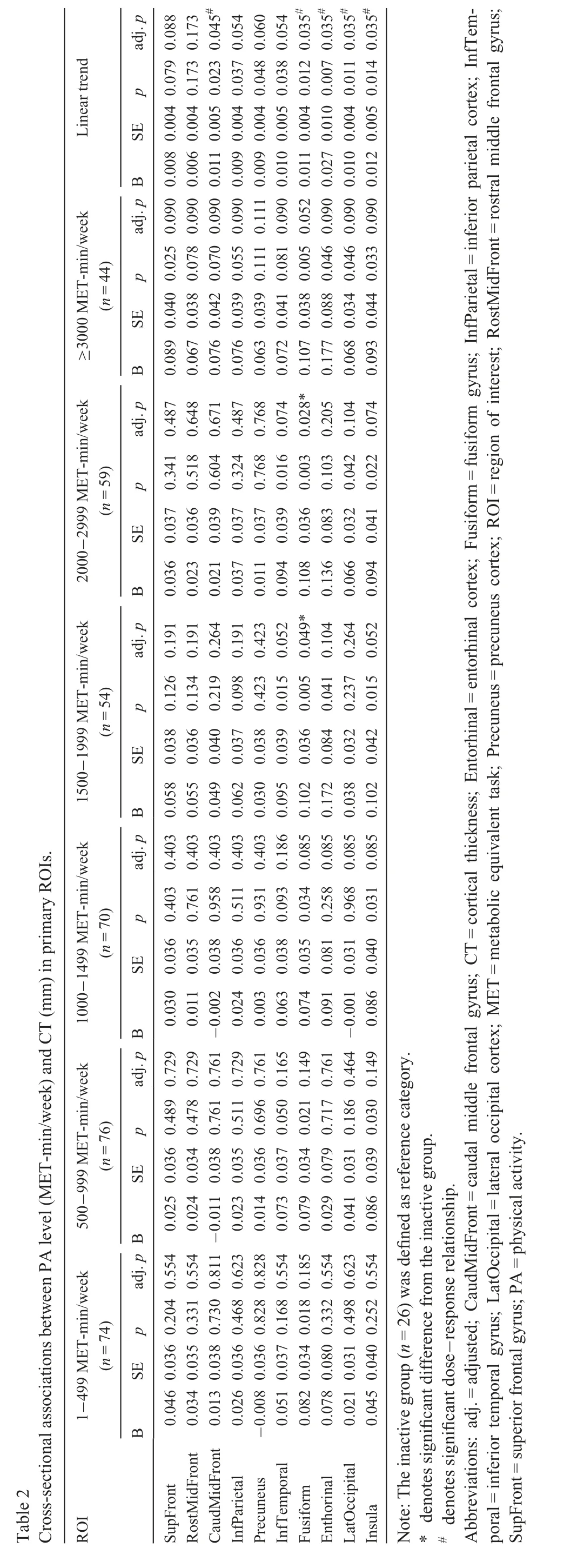
Multiple linear regressions demonstrated significant associations between PA level and CT in the superior frontal,inferior temporal,fusiform,entorhinal,lateral occipital,and insula cortices.However,after false discovery rate correction for multiple comparisons,only the association of PA with the fusiform gyrus remained significant.In this region,PA groups of 1500-1999 MET-min/week (B=0.102,SE=0.036,adj.p=0.049) and 2000-2999 MET-min/week (B=0.108,SE=0.036,adj.p=0.028) had significantly greater CT than the sedentary group.A trend toward significance was also found for the ≥3000 MET-min/week group in this region(B=0.107,SE=0.038,adj.p=0.052).Tests for linear trend(dose-response association) revealed positive associations between increasing PA levels and the fusiform CT(B=0.011,SE=0.004,adj.p=0.035).The test for linear trend was also significant for the caudal middle frontal (B=0.011,SE=0.005,adj.p=0.045),entorhinal (B=0.027,SE=0.010,adj.p=0.035),lateral occipital (B=0.010,SE=0.004,adj.p=0.035),and insula(B=0.012,SE=0.005,adj.p=0.035)cortices.No further significant associations were found for the other primary brain ROIs.These results are presented in Table 2.
Analyses in secondary brain ROIs are presented in Table 3.Significant positive associations were found in the temporal pole,the frontal pole,and the supramarginal gyrus.Compared with sedentary people,individuals who achieved either 1500-1999 MET-min/week (B=0.221,SE=0.072,adj.p=0.035) or 2000-2999 MET-min/week (B=0.225,SE=0.072,adj.p=0.043) displayed higher CT in the temporal pole.People achieving 3000 MET-min/week or more also tended to have greater temporal pole CT than sedentary older adults(B=0.192,SE=0.76,adj.p=0.096).In addition,the group of 1500-1999 MET-min/week also had higher CT in the frontal pole (B=0.190,SE=0.064,adj.p=0.035) and the supramarginal gyrus (B=0.100,SE=0.036,adj.p=0.049),compared with the inactive group.Tests for linear trend were significant in the temporal pole (B=0.026,SE=0.009,adj.p=0.048) as well as in the medial orbitofrontal cortex(B=0.015,SE=0.005,adj.p=0.048).No other significant associations were found for the secondary ROIs.
Supplementary analyses,performed separately on each hemisphere,revealed that most of the associations were located in the right hemisphere.These analyses are provided in Supplementary Tables 1-4.
4.Discussion
This study investigated the cross-sectional associations between PA level and brain CT in community-dwelling adults aged 70 years and older with spontaneous memory complaints.The study demonstrates that higher levels of PA were mainly associated with greater CT in the fusiform gyrus and the temporal pole,especially for participants performing at least 1500 MET-min/week of MVPA.It also showed a positive dose-response relationship of PA level with CT in the caudal middle frontal gyrus,the medial orbitofrontal cortex,the fusiform gyrus,the entorhinal cortex,the temporal pole,the lateral occipital cortex,and the insula.
Our findings are consistent with previous cross-sectional studies demonstrating that a higher amount of PA was associated with a thicker brain cortex in older adults.24We found that a minimal dose of 1500 MET-min/week of PA may be necessary to provide benefits on CT.This PA amount,which is roughly equivalent to 6 h/week of brisk walking,represents almost thrice the current recommended weekly volume of PA for adults,which is at least 150 min of moderate-intensity PA.43Regarding the cortical regions associated with PA,our findings showed associations mainly in temporal regions while Lee et al.24found positive associations in the frontal and parietal lobes.Such disparities might come from the age and clinical differences between Lee et al.’s24sample and ours.Indeed,while Lee et al.’s population24was composed of cognitively normal individuals aged less than 65 years on average,MAPT subjects were aged about 75 years and had spontaneous memory complaints.It has been demonstrated that cortical atrophy mostly occurs in the frontal lobe before 60 years of age,after which it extends to the temporal areas,where it becomes more pronounced.8,16In addition,this phenomenon could be coupled with AD mechanisms that mainly affect the temporal lobes,8,45making the latter particularly vulnerable to cortical thinning from the age of 60 years.Of note,the fusiform gyrus cortex,along with the middle temporal,inferior temporal,and entorhinal cortices,have been defined as the AD signature because of their vulnerability toward this pathology.46The temporal lobe structures are also the first affected regions in mild cognitive impairment (MCI)that precedes the conversion to AD.47,48Similar regional differences in the CT-PA relationships can also be consistently observed across longitudinal studies in which slower PA-related cortical thinning was reported in the prefrontal cortex in people aged around 60 years25but in the parietal and temporal lobes in people aged 70 years.26Taken together,these data suggest that the relationship between CT and PA may be dependent on brain status in the sense that PA might be preferentially associated with CT in the most vulnerable areas at a given time point in the life course.Similarly,some authors have demonstrated that,in older adults,cardiorespiratory fitness was positively associated with CT in regions showing significant age-related atrophy.49Thus,the association between PA and CT might follow the age-related pattern of cortical thinning described above,with a shift from the frontal to the temporal lobes after the age of 60 years.One possible mechanism underlying this relationship is that PA may protect the brain from cortical thinning related to β-amyloid accumulation,which is supported by a recent longitudinal study.26Further investigations,including wide ranges of age,are needed to test the hypothesis of an age-dependent association between regional CT and PA.
Additionally,it is worth noticing that despite the associations of the PA active groups,compared to the inactive group,with CT were not significant for most of the ROIs,we have found significant dose-response relationships between PA level and CT in several regions,such as the caudal middle frontal,medial orbitofrontal,entorhinal,temporal pole,lateral occipital,and insula cortices.Given the close associations between PA and cardiorespiratory fitness50found both in observational49and exercise intervention studies51that have reported similar dose-response relationships between cardiorespiratory fitness and CT,it is possible that cardiorespiratory fitness may represent a mediator linking PA to CT in older adults.Moreover,our supplementary analyses demonstrated that PA was mainly associated with CT in the right hemisphere.It has been recently demonstrated that aging affects the right and left cortices differently.52Such lateralization effect requires further investigations since previous studies on populations with a mean age of 70 years or more used CT values that were averaged across left and right hemispheres,26,36which impeded us from comparing our lateralization findings with prior works.
Last,it is possible that the type of PA could also play a role in cortical thickening,as suggested by CT increases following 6 months of a dancing intervention in old adults.34Compared with endurance exercise,which implies rather repetitive movements,dancing involves more complex body movements and hence may require a greater mental challenge than aerobic activities.Thus,while CT may benefit from aerobic exercise through metabolic pathways,53more complex types of exercise may also increase CT through neurocognitive mechanisms.However,we could not test the association between the type of PA and CT based on the questionnaire we used.
Our study is one of the few that have investigated CT and PA associations in a population aged 70 years and older at risk for cognitive decline.Except for the study published by Rabin et al.,26previous observational publications were based on middle-aged people and people with a mean age around 60 years.24,25The brains of people 60 years old may differ from the brains of people 75 years old (the mean age of the population in our study),for example,due to the acceleration of β-amyloid deposition and cortical thinning that is more marked in individuals aged over 60 years.8,45Another important aspect of our study lies in the fact that we stratified PA levels into a rather large number of subcategories.Our subcategories included very inactive individuals (people reporting doing no PA at all) as well as active and very active people,which allowed for a more precise quantification of the associations between PA and CT than could be expected from previous investigations that used a simple “lowvs.high”dichotomization of PA levels.24,26
One limitation of our study is its cross-sectional design,which precludes any causal and longitudinal inferences from the observed associations.A second limitation is the absence of vertex-based analyses,which would have provided a reliable way to correct for multiple comparisons.However,the ROI-based approach was chosen because of the hypothesis-driven nature of our work.Indeed,10 primary ROIs were pre-specified because they were previously associated with PA in several publications.24,26,34Using an ROI system provided a way to perform a simple aggregation of the results reported in these different papers.Also,the use of fully automated techniques for CT computation represents a limitation because it could lead to errors when delineating greywhite and grey-cerebrospinal fluid boundaries.Manual intervention can be used to overcome such errors,54but was beyond reach given the scale of our large dataset.Therefore,we relied on careful visual inspection of the FreeSurfer results performed by imaging operators55to discard problematic subjects,which has been shown to largely increase the reliability of the final analysis.56Another weakness lies in the method used for assessing PA (i.e.,a self-reported questionnaire),which may have overestimated the true levels of PA,especially in men.57For this reason,it is possible that the PA threshold of significance for CT we found in our study was higher than the threshold that could be found in studies that measured PA with accelerometers.Additionally,the PA questionnaire used in our study was validated against fitness tests in people aged 20-60 years only,and it demonstrated poor validity values against accelerometers.39It should also be mentioned that the number of participants in our study was smaller in the groups with high PA levels,thus reducing the statistical power to detect significant associations in these groups.
5.Conclusion
This study demonstr ates positive associations between PA level and CT in temporal cortical areas prone to AD among people aged 70 years and older.In this population,the persons who achieved at least 1500 MET-min/week of MVPA had higher CT in the fusiform gyrus and the temporal pole than their inactive peers.Moreover,other regions,such as the entorhinal cortex,the caudal middle frontal gyrus,the medial orbitofrontal cortex,the lateral occipital cortex,and the insula,were associated with PA in a dose-response manner.Future investigations that focus on the type of PA achieved,that use accelerometers for better quantification of PA,and that measure cardiorespiratory fitness may add to our understanding of the relationship between PA and CT.Studies that assess sedentary time could also make an important contribution to the field,given its independent deleterious effect on health.58
Acknowledgments
The present work was performed in the context of the Inspire Program,a research platform supported by grants from the Region Occitanie/Pyrénées-Méditerranée (No.1901175)and the European Regional Development Fund (ERDF)(project No.MP0022856).This study also received funds from Alzheimer Prevention in Occitania and Catalonia (APOC Chair of Excellence-Inspire Program).The MAPT study was supported by grants from the Gérontopôle of Toulouse,French Ministry of Health (PHRC 2008 and PHRC 2009),Pierre Fabre Research Institute(manufacturer of the omega-3 supplement),Exonhit Therapeutics SA,and Avid Radiopharmaceuticals Inc.The promotion of this study was supported by the University Hospital Center of Toulouse.The data-sharing activity was supported by the Association Monegasque pour la Recherche sur la maladie d’Alzheimer (AMPA) and the INSERM-University of Toulouse III UMR 1027 Unit.The members of MAPT/DSA Group are listed in the Supplementary materials.
Authors’contributions
JR conceptualized and designed the study,analyzed the data,performed statistical analyses,and wrote the manuscript;PSB conceptualized and designed the study,analyzed the data,and revised the manuscript critically for intellectual content;YR and BV revised the manuscript for intellectual content;CF,JFM,and AG played a major role in data acquisition and revised the manuscript for intellectual content.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2021.01.011.
 Journal of Sport and Health Science2023年3期
Journal of Sport and Health Science2023年3期
- Journal of Sport and Health Science的其它文章
- Impact loading in female runners with single and multiple bone stress injuries during fresh and exerted conditions
- Are EPB41 and alpha-synuclein diagnostic biomarkers of sport-related concussion?Findings from the NCAA and Department of Defense CARE Consortium
- Factors and expectations influencing concussion disclosure within NCAA Division I athletes:A mixed methodological approach
- Effects of contact/collision sport history on gait in early-to mid-adulthood
- Refinement of saliva microRNA biomarkers for sports-related concussion
- Lacrosse-related injuries in boys and girls treated in U.S.emergency departments,2000-2016