
Effects of contact/collision sport history on gait in early-to mid-adulthood
2023-06-06 13:35KatherineHunzingerJalynCaeseRebekahMannixWilliamMeehanIIIJoelynHaferBuzSwanikThomasBukley
Katherine J.Hunzinger,Jalyn B.Caese,Rebekah Mannix,William P.Meehan III,Joelyn F.Hafer,C.Buz Swanik,Thomas A.Bukley,*
a Department of Biostatistics,Epidemiology,and Informatics,University of Pennsylvania Perelman School of Medicine,Philadelphia,PA 19104,USA
b Penn Injury Science Center,University of Pennsylvania,Philadelphia,PA 19104,USA
c School of Health and Rehabilitation Sciences,The Ohio State University College of Medicine,Columbus,OH 43210,USA
d Division of Emergency Medicine,Boston Children’s Hospital,Boston,MA 02115,USA
e Departments of Pediatrics and Emergency Medicine,Harvard Medical School,Boston,MA 02115,USA
f The Micheli Center for Sports Injury Prevention,Waltham,MA 02453,USA
g Division of Sports Medicine,Department of Orthopedics,Boston Children’s Hospital,Boston,MA 02453,USA
h Department of Pediatrics and Orthopedics,Harvard Medical School,Boston,MA 02453,USA
i Department of Kinesiology and Applied Physiology,University of Delaware,Newark,DE 02453,USA
j Interdisciplinary Program in Biomechanics and Movement Science,University of Delaware,Newark,DE 02453,USA
Abstract Background: To determine the effect of contact/collision sport participation on measures of single-task (ST) and dual-task (DT) gait among early-to middle-aged adults.Methods: The study recruited 113 adults(34.88±11.80 years,(mean±SD);53.0%female)representing 4 groups.Groups included(a)former non-contact/collision athletes and non-athletes who are not physically active (n=28);(b) former non-contact/collision athletes who are physically active(n=29);(c)former contact/collision sport athletes who participated in high-risk sports and are physically active(n=29);and(d)former rugby players with prolonged repetitive head impact exposure history who are physically active (n=27).Gait parameters were collected using inertial measurement units during ST and DT gait.DT cost was calculated for all gait parameters (double support,gait speed,and stride length).Groups were compared first using one-way analysis of covariance.Then a multiple regression was performed for participants in the highrisk sport athletes and repetitive head impact exposure athletes groups only to predict gait outcomes from contact/collision sport career duration.Results: There were no significant differences between groups on any ST,DT,or DT cost outcomes(p >0.05).Contact/collision sport duration did not predict any ST,DT,or DT cost gait outcomes.Conclusion: Years and history of contact/collision sport participation does not appear to negatively affect or predict neurobehavioral function in early-to mid-adulthood among physically active individuals.
Keywords: Exercise;Neurodegenerative disease;Postural control;Rugby;Subconcussive impacts
1.Introduction
Repetitive head impacts (RHI) are a form of neurotrauma that occur through normal participation in contact/collision sports (i.e.,American football,football/soccer,ice hockey,boxing,rugby,lacrosse,and wrestling).1,2It is theorized that RHI accumulated over years of contact/collision sports participation may have adverse effects on both short-and long-term neurobehavioral functioning and health outcomes,yet many of the existing studies are limited in generalizability and overall effect sizes of significant findings.3Moreover,controversy remains as to whether RHI exposure leads to a higher risk of neurodegenerative diseases later in life.4-6Since retrospective RHI exposure information is not available for many patients seeking evaluation,the National Institutes of Health/National Institute of Neurological Disorders and Stroke (NINDS) traumatic encephalopathy syndrome consensus statement endorsed the use of contact/collision sport career duration as a proxy measure.7However,the homogenous data that informed the traumatic encephalopathy syndrome criteria were derived mostly from male college-or middle-aged former collision sport athletes to the exclusion of females and other sport/cohort groups.3,7
Rugby is the most popular collision sport worldwide and the only collision sport where the laws are the same for both males and females,8,9thus indicating similar RHI exposure.10While most contact/collision sport athletes typically stop their careers after high school or college,many Americans only begin playing rugby at this time.Therefore,they continue to experience RHI through adulthood and often exceed the traumatic encephalopathy syndrome threshold for exposure.7,11,12Growing evidence links rugby participation and long-term physical and mental health dysfunction;however,sports participation during adulthood is associated with increased physical activity,a known positive modifier of long-term health outcomes.13-16Thus,the negative effects of RHI and the positive effects of physical activity on mid-and later-life neurobehavioral health (e.g.,gait) remain to be elucidated.15,17,18
Previous research on the long-term effects of RHI exposure has relied on self-report or on simplistic clinical measures with little to no inquiry into more objective and sensitive measures of neurobehavioral health in aging/post-collegiate populations.3,19-22Gait has been referred to as the 6th vital sign since it is an objective measure of neurological health,reflects quality of life,and is sensitive to age-and neurological impairment-related changes,with decreased performance(i.e.,conservative gait strategies) in older and neurologically compromised populations.23-25The addition of a cognitive challenge during gait,termed dual-task(DT)gait,has been utilized to identify differences between neurologically impaired populations and healthy controls.26Further,DT gait can be used to identify post-concussion and persistent subclinical deficits in executive function as well as neurophysiological impairments by calculating the DT cost (i.e.,the change from single task(ST) to DT).26Yet,because most investigations into gait abnormalities due to RHI exposure/neurotrauma have been limited to younger(e.g.,college or high school)male collision sport athletes or male and female contact/collision sport athletes and have failed to account for potential confounders(e.g.,body mass index (BMI),age,concussion history,and sex),the long-term effects of RHI on gait remain inconclusive.19,20,22
Contact/collision sport-related RHI have been associated with poorer long-term health outcomes,7,17but increased physical activity is known to improve many health outcomes.15,27Thus,the purpose of this study was to determine the relationship between contact/collision sport career duration on ST and DT gait in physically active early-to middle-aged adults.We hypothesized that individuals with a history of RHI exposure would have a conservative gait strategy,evidenced by slower gait speed,a longer percentage of time in double support,and shorter stride length compared to individuals without RHI exposure.Secondly,we hypothesized that longer career duration would be associated with a conservative gait strategy (i.e.,decreased gait speed and stride length,and increased double support) and worse DT cost in collision sport athletes.
2.Methods
2.1. Participants
Power analyses have been historically underutilized in neurotrauma and gait research.28As such,a power analysis(G*Power 3.1;https://link.springer.com/content/pdf/10.3758/BF03193146.pdf) was conducted based on the ST gait speed of 13 total subjects across the 4 groups.(The ability of ST gait to discriminate healthy from neurologically impaired individuals has been shown in previous research.29,30) Results indicated that 22 participants were needed per group to achieve 80% power for a medium effect size (Cohen’sf=0.25);31overall,113 adults were enrolled (Table 1) (Fig.1).Groups differed significantly in terms of BMI and concussion history,and thus these variables were accounted for in adjusted models.The inclusion and exclusion criteria for the 4 groups(nonathletes (NON),non-contact/collision athletes (NCA),highrisk sport athletes (HRS),and rugby/prolonged RHI exposure athletes (RUG)) are described below (Table 2).Consistent with previous studies,contact/collision sports included those with potential and/or routine RHI exposure (i.e.,American football,soccer,ice hockey,boxing,rugby,lacrosse,and wrestling).2,11Briefly,participants were recruited from 4 groups: (a) NON: individuals with no previous contact/collision sport experience who are not currently physically active(n=28);(b)NCA:non-contact/collision sport athletes/individuals with no previous contact/collision sport experience who are physically active (n=29);(c) HRS: former contact/collision sport athletes who are physically active (n=29);and (d)RUG: current/former rugby players with a history of playing rugby after age 22 who are physically active(n=27).Of note,none of the RUG group participants had actively participated in contact rugby in the 6 months prior to the study due to coronavirus disease 2019 (COVID-19) related shutdowns (years since last participating in contact/collision rugby: 8.5 ± 9.8 years;range: 0.5-36 years).Participants were recruited via word of mouth,social media,and flyers posted at various sports venues,and they were compensated for their participation in the form of an Amazon.com gift card.All participants provided oral and written informed consent in accordance with the University of Delaware’s Institutional Review Board.
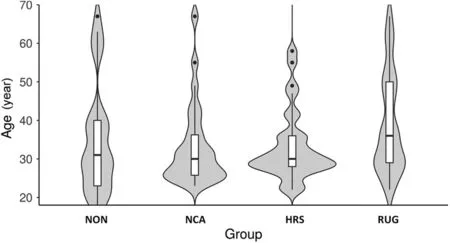
Fig.1.Violin plot of age distribution by group with box and whisker plot overlay.Groups were not significantly different by age (p=0.319).HRS=high-risk sport athletes;NCA=non-contact athletes;NON=non-athletes;RUG=rugby/prolonged RHI exposure athletes.
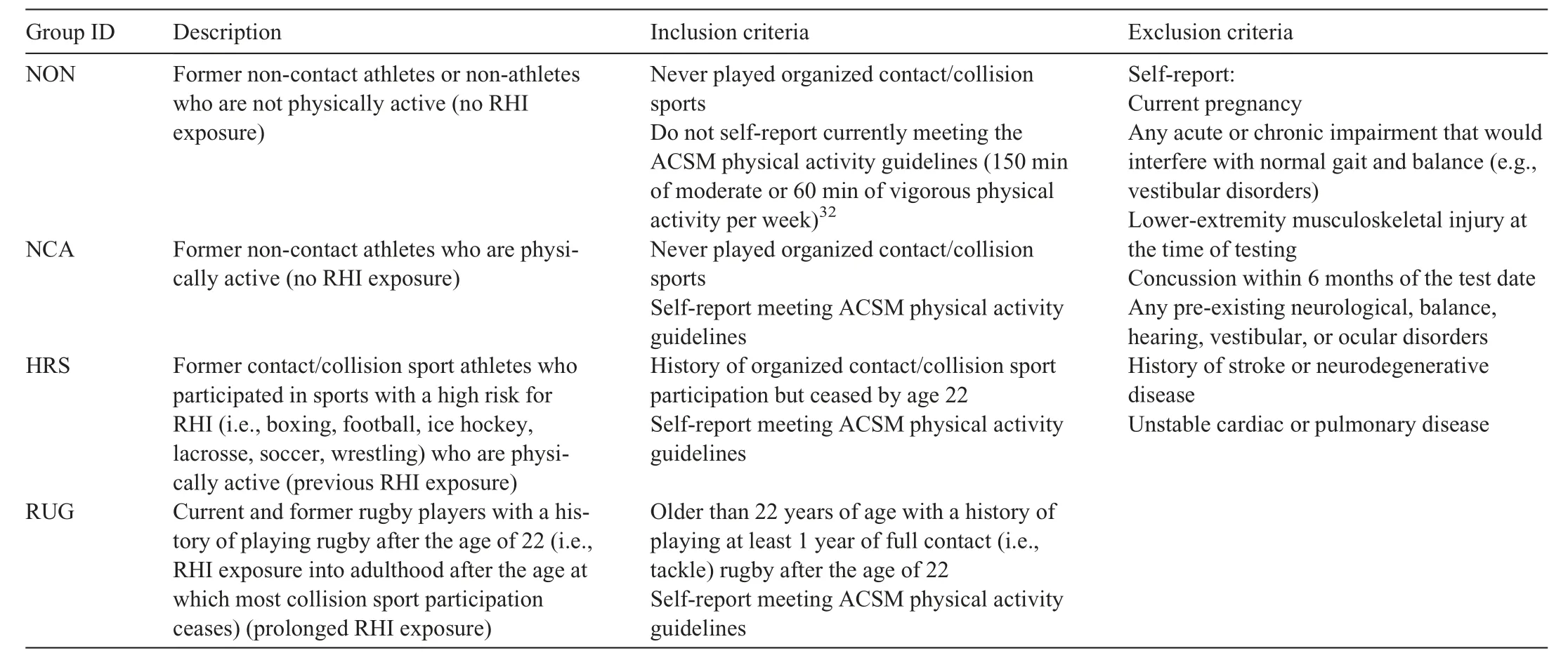
Table 2 Inclusion and exclusion criteria by group.
2.2. Procedures
Participants completed online questionnaires to ascertain relevant demographic information,physical activity status(yes/no meeting American College of Sports Medicine guidelines of 150 min/week of moderate or 60 min/week of vigorous physical activity32),sport history,and career duration of contact/collision sports via Qualtrics (Qualtrics,Provo,UT,USA).Consistent with traumatic encephalopathy syndrome guidelines,career duration was calculated for each participant as the sum of each year played in each contact/collision sport(e.g.,2 years of ice hockey and 2 years of American football=4 years career duration).7
Participants completed 5 ST walking trials and 5 DT walking trials with a cognitive task (i.e.,spelling 5-letter words backwards,serial 6 s/7 s,or naming the months in reverse order) while wearing 3 inertial measurement units on the dorsal surface of each foot and L5 vertebrae (Opal Sensor-V1,APDM,Portland,OR,USA).33,34Data were collected at 128 Hz and analyzed using Mobility Lab software(APDM).35Walking trials consisted of the participant traversing a 7-m walkway at a self-selected pace.Dependent variables were double support (% of gait cycle),gait speed (m/s),and stride length (m) for ST,DT,and the associated DT cost for each.These variables were chosen because they differ the most between neurologically impaired populations and healthy controls,with negative changes being indicative of a conservative gait.26DT cost was calculated as a percentage change between ST and DT conditions:(DT-ST)/(ST)×100%.36
2.3. Statistical analysis
Group demographics were compared using either a oneway analysis of variance when comparing all 4 groups or a Mann-WhitneyU-test when comparing the collision groups only(i.e.,HRS and RUG),due to the violation of normality.
Unadjusted models can be found in Supplementary Table 1.To determine the effect of group on gait outcomes,groups were compared using an analysis of covariance adjusted for known covariates (i.e.,age,sex,concussion history,and BMI)26,37that may affect gait performance.All test assumptions of linearity,outliers,and homogeneity were met.Post hocanalyses were performed for significant outcomes,with a Bonferroni test for multiple comparisons.Effect sizes are reported as η2and interpreted as small=0.01-<0.06;medium=0.06-<0.14;large=≥0.14.31
To investigate the relationship between contact/collision career duration(years)and gait outcomes,we performed a linear regression using the enter method to predict ST,DT,and DT cost for gait outcomes (i.e.,gait speed,stride length,double support) in collision sport athletes (i.e.,HRS and RUG groups)(Supplementary Table 2).We also used a multiple linear regression with Bonferroni adjustment for multiple comparisons to adjust analyses for sex (M/F),concussion history,age,and BMI (kg/m2).All assumptions of linearity,independence of residuals,homoscedasticity,and multicollinearity were met.All analyses were run using SPSS Version 26(SPSS,IBM,Armonk,NY,USA).
3.Results
3.1. Instrumented gait parameters by group
Means,standard errors,range,and 95% confidence intervals(95%CIs)for each gait variable of interest(i.e.,gait speed,stride length,double support) are presented in Table 3 along with their associated DT cost outcomes.There were no significant differences between groups in adjusted models for all gait outcomes and DT costs for each variable(p>0.05)(Table 3).Of note,none of the groups differed by the clinically meaningful change for ST gait speed(0.09 m/s)in adjusted models,further indicating no clinical significance.38
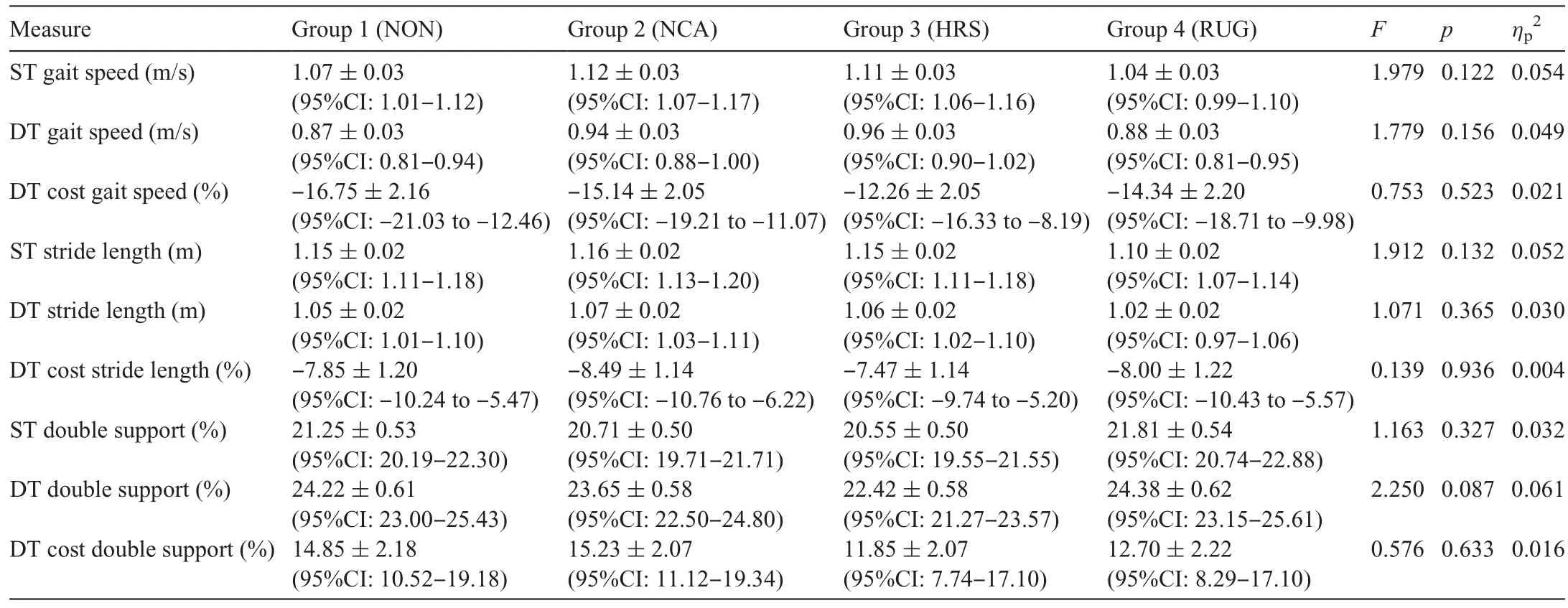
Table 3 Adjusted single-and dual-task gait outcomes by groups.
3.2. Career duration and gait parameters
Only the adjusted model for ST double support was significant (p=0.009);however,career duration did not add significantly to this model (p=0.058) (Table 4).None of the other models significantly predicted any of the gait outcomes in contact/collision sport athletes (i.e.,HRS and RUG groups) (p>0.05)(Table 4).
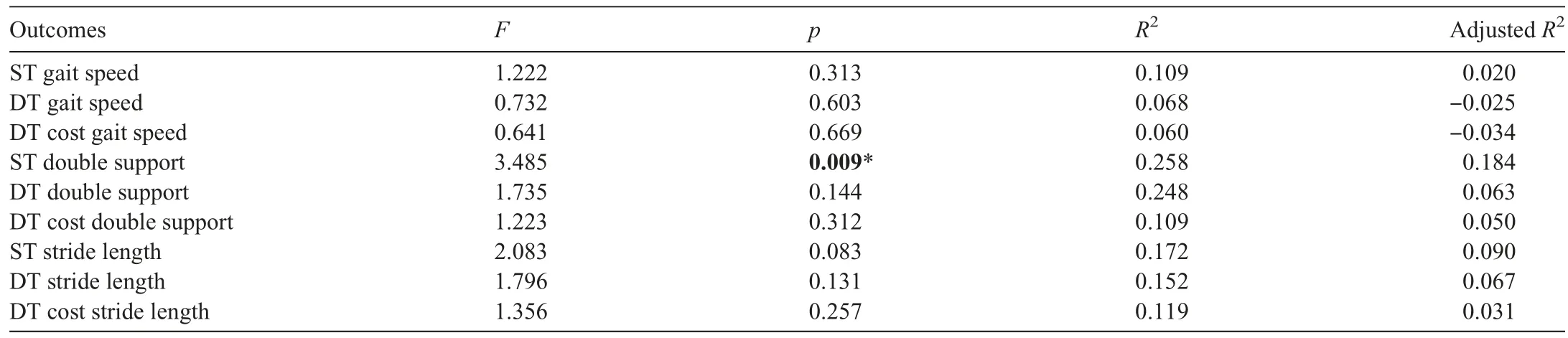
Table 4 Adjusted multiple linear regression:Collision sport athletes and gait.
4.Discussion
RHI exposure may put individuals at risk for subtle acute and chronic neurophysiological deficits;3,19,20however,prior studies have focused primarily on current collegiate or former professional American football players.3,19,20,39,40We addressed this limitation by including male and female athletes from a variety of sports,with a special emphasis on rugby—a sport representative of prolonged RHI exposure into adulthood across the sexes.Contrary to our hypothesis,the primary finding of this study was that participation in contact/collision sports,including prolonged rugby participation into early adulthood and middle age,was not associated with impaired postural control.Further,career duration of contact/collision sport was unrelated to postural control outcomes in physically active contact/collision sport athletes.Collectively,these findings suggest that previous and/or prolonged RHI exposure may not negatively impact gait in early-to mid-adulthood in individuals who report being physically active.
Gait was not impaired in early-to mid-adulthood in selfreported physically active individuals with a history of sportsrelated RHI exposure compared to both physically active and inactive individuals without a history of RHI.This is consistent with a 2021 review of current adolescent and collegiate athletes that identified limited effects of acute RHI on gait across a variety of measures.19Similarly,recent investigations of middle-aged former American football players and American amateur rugby players (male and female) reported that career duration was unrelated to later-life or mid-life health conditions and dysfunction.11,39,41Taken together,data among physically active early-to mid-adult collision sport athletes(i.e.,aged 22-50 years) suggest that RHI exposure does not adversely affect objective measures of neurobehavioral health;3however,the later-life effects (i.e.,older adults aged>65 years) and the effects in physically inactive individuals with histories of prolonged RHI exposure (e.g.,former adult rugby players who are inactive)remain unknown.
The lack of differences between the collision sport athletes and the non-contact/collision sport athletes herein may be the result of the neuroprotective effects of exercising outweighing the potential negative consequences of RHI exposure on postural control.42-44Rugby is a multi-activity sport consisting ofrepeated high-intensity sprint efforts separated by variable rest durations,jogging,and dynamic exertion(e.g.,scrum,ruck,or tackle);moreover,the average rugby player covers between 4200-6500 m per 80-min match and spends 42%of the match above 85% of their maximum heart rate.45As such,physical activity from contact/collision sport participation provides players with improved cardiovascular and physical health in later life,reducing risk of chronic disease and increasing lifespan compared to the general population,which may be a result of the cumulative effects of increased levels of lifetime physical activity.15,46-48This may partially explain our lack of group differences.Since the HRS and RUG groups were physically active,the chronic benefits of exercise may outweigh the negative consequences,if any,of RHI.Of note,these participants were generally young (~35 years old;87%were under 50 years old)compared to other cohorts of middleaged adults,meaning it is possible that the negative consequences of RHI may not have manifested yet among the HRS and RUG groups.Indeed,self-reported head trauma is related to worse DT gait in middle-aged former professional American football players,independent of career duration,age,and BMI.49Furthermore,physical inactivity,which usually indicates low levels of cardiorespiratory fitness,is a risk factor for many diseases.43,50,51Indeed,among former professional American football players,declines in physical activity were related to increased neuropsychiatric dysfunction,52which has been linked to worse gait performance.53However,many of these chronic conditions result from chronic physical inactivity and poor lifestyle choices,which,again,may not yet have manifested negative consequences in our young cohort.In addition,our measurement of physical activity was based upon current physical activity status and did not account for previous regular physical activity throughout one’s lifespan.Taken together,these findings suggest that RHI history and physical activity status in early-to mid-adulthood are unrelated to gait performance.
A secondary finding of this study,contrary to our hypothesis,was that contact/collision sport career duration was unrelated to gait performance in current and former contact/collision sport athletes(HRS and RUG groups).Again,gait—particularly DT gait—is an important marker of neurobehavioral health that is sensitive to changes in neurological function and aging.23,25To our knowledge,this was the first study to investigate the relationship between RHI and gait in early-to mid-life(i.e.,aged 30-50 years)across a variety of RHI exposure history.19Concussion leads to a more conservative gait strategy acutely post-injury,with DT gait highlighting impairments,yet the literature on the effects of RHI on gait remain mixed.19,26Herein,our data suggest that neither career duration,sex,age,BMI,nor concussion history added significantly to the prediction of ST and DT gait performance.This is consistent with a recent finding by Oldham et al.21whereby career duration in collision and contact sports was unrelated to ST,DT,and DT cost for gait speed or stride length in a younger cohort of collegiate athletes with shorter career duration.Further,the finding that career duration,age,and BMI were unrelated to gait performance is consistent with Manor et al.’s49finding that these factors did not influence the relationship between self-reported symptomatic head trauma and walking performance in middle-aged American football players.This finding could also be the result of any negative consequences not yet having manifested.Additionally,it could be that the RHI experienced by these individuals were not sufficient to warrant any changes in gait.Thus,consistent with previous data among contact/collision sport athletes in college,our data suggest that RHI history is unrelated to gait performance in early-to mid-adulthood.19,21
A primary limitation of this study was that this heterogeneous sample had a relatively small proportion of older adults,which may contribute additional confounders that were not accounted for and limit extrapolation to older cohorts.Our sample may have been susceptible to survivor or respondent bias as individuals with neurophysiological dysfunction may have removed themselves from participation in contact/collision sports or failed to volunteer for the study while healthy and resilient individuals continued to participate in sport and subsequently volunteered for study participation.However,it should be noted that our study is different from previous research that limited itself by enrolling only symptomatic RHI-exposed individuals,which potentially biased the results.3Furthermore,there were considerable differences in the sex composition of each group,which although not statistically significant,may have introduced further bias into our analyses.We addressed this difference in sex composition (which may be a result of the varying availability of contact/collision sports for females compared to males2)by accounting for sex in all adjusted models.Another limitation was the use of career duration as a metric for RHI exposure,which may not be sensitive to the effects of playing style,culture,and competition levels.However,this method was chosen based on the recommendation of the NINDS traumatic encephalopathy syndrome consensus statement and has been previously utilized in other research as a measure of RHI exposure because it permits a rough estimation in the absence of biomechanical data,which is not feasible to collect across the lifespan.3,7,11Lastly,this study relied on self-reported measures of physical activity as a dichotomous outcome(yes/no for meeting American College of Sports Medicine physical activity guidelines).Although self-reported measures of physical activity have been used in previous research,54they may fail to capture the accuracy and precision needed to detect the true effects of exercise (i.e.,frequency,intensity,type,time) on the included outcomes.Furthermore,our cohort did not have an HRS or RUG group that was not currently physically active,thereby preventing analysis of the effects of physical activity and RHI on gait.Future studies should further explore both current and prior exercise habits (i.e.,the chronicity of regular physical activity)across the sporting spectrum.
5.Conclusion
Prolonged participation in contact/collision sports in physically active individuals is unrelated to postural control in early-to mid-adulthood.Further,RHI exposure,assessed by career duration,does not appear to negatively affect postural control in early-to mid-adulthood.These findings add to the growing body of literature showing that exposure to RHI through routine contact/collision sport participation,assessed by career duration,is unrelated to neurological dysfunction in early-to mid-adulthood.This study fills a gap in the literature among female and male collision sport athletes in early-to mid-adulthood who participated in prolonged contact/collision sports.However,consistent with the NINDS traumatic encephalopathy syndrome call to action,future research should seek to expand on these findings by conducting more research in older adults and utilizing more specific measures of RHI exposure and physical activity.
Acknowledgments
The authors thank all the participants who participated in this study and all the collaborators and friends who helped share our study flyers to promote participant recruitment.This study and publication were made possible and funded in part by the University of Delaware Unidel Distinguished Graduate Scholars Fellowship and Department of Kinesiology and Applied Physiology Doctoral Research Fund.Additionally,Dr.Hunzinger acknowledges funding support in part by the Department of Defense grant W81XWH-21-1-0590,the Penn Injury Science Center,and National Institutes of Health/National Institute of Neurological Disorders and Stroke brain injury training grant T32 NS043126.Opinions,interpretations,conclusions,and recommendations are those of the authors and are not necessarily endorsed by the Department of Defense.
Authors’contributions
KJH conceived the study and study design,recruited all participants,performed statistical analysis,and drafted the manuscript;JBC,RM,WPM,and JFH participated in study design,assisted in statistical analysis,and reviewed manuscript drafts;CBS and TAB assisted with study design,study resource allocation,assisted with data interpretation,and reviewed all manuscript drafts.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
Dr.Hunzinger is an independent contractor with USA Rugby as a World Rugby Educator for the Strength and Conditioning and Referee Strands.Dr.Meehan receives royalties from (1) ABC-Clio publishing for the sale of his books,Kids,sports,and concussion:A guide for coaches and parents,andconcussions;(2)Springer International for the bookHead and neck injuries in young athlete,and (3) Wolters Kluwer for working as an author forUpToDate.His research is funded,in part,by philanthropic support from the National Hockey League Alumni Association through the Corey C.Griffin Pro-Am Tournament,and a grant from the National Football League.All the supporting entities had no involvement in the study design and writing of the manuscript or the decision to submit it for publication.The other authors have nothing to disclose.
Supplementary materials
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2022.12.004.
 Journal of Sport and Health Science2023年3期
Journal of Sport and Health Science2023年3期
- Journal of Sport and Health Science的其它文章
- Impact loading in female runners with single and multiple bone stress injuries during fresh and exerted conditions
- Refinement of saliva microRNA biomarkers for sports-related concussion
- Are EPB41 and alpha-synuclein diagnostic biomarkers of sport-related concussion?Findings from the NCAA and Department of Defense CARE Consortium
- Factors and expectations influencing concussion disclosure within NCAA Division I athletes:A mixed methodological approach
- Association between ACTN3 R577X genotype and risk of non-contact injury in trained athletes:A systematic review
- Lacrosse-related injuries in boys and girls treated in U.S.emergency departments,2000-2016