
Is hamstrings-to-quadriceps torque ratio useful for predicting anterior cruciate ligament and hamstring injuries?A systematic and critical review
2023-06-06 13:35EleftheriosKellisChrysostomosShinisVsiliosBltzopoulos
Eleftherios Kellis *,Chrysostomos Shinis ,Vsilios Bltzopoulos
a Laboratory of Neuromechanics,Department of Physical Education and Sport Sciences at Serres,Aristotle University of Thessaloniki,Serres 62100,Greece
b Research Institute for Sport and Exercise Sciences(RISES),Faculty of Science,Liverpool John Moores University,Liverpool L3 5UX,UK
Abstract Background: For the past 30 years,the hamstring (H)-to-quadriceps (Q) (H:Q) torque ratio has been considered an important index of muscle strength imbalance around the knee joint.The purpose of this systematic review was to examine the value of H:Q torque ratio as an independent risk factor for hamstring and anterior cruciate ligament(ACL)injuries.Methods: Database searches were performed to identify all relevant articles in PubMed,MEDLINE,Cochrane Library,and Scopus.Prospective studies evaluating the conventional (concentric H:Q),functional (eccentric H: concentric Q),and mixed (eccentric H at 30°/s: concentric Q at 240°/s)H:Q ratios as risk factors for occurrence of hamstring muscle strain or ACL injury were considered.Risk of bias was assessed using the Quality In Prognosis Studies tool.Results: Eighteen included studies reported 585 hamstrings injuries in 2945 participants,and 5 studies documented 128 ACL injuries in 2772 participants.Best evidence synthesis analysis indicated that there is very limited evidence that H:Q strength ratio is an independent risk factor for hamstring and ACL injury,and this was not different between various ratio types.Methodological limitations and limited evidence for ACL injuries and some ratio types might have influenced these results.Conclusion: The H:Q ratio has limited value for the prediction of ACL and hamstring injuries.Monitoring strength imbalances along with other modifiable factors during the entire competitive season may provide a better understanding of the association between H:Q ratio and injury.
Keywords: ACL;Isokinetic;Prospective;Strains;Strength imbalance
1.Introducti on
Muscle strength evaluation is an integral part of the fitness assessment of athletes or rehabilitation of individuals with various pathologies or injuries.One of the key parameters in these applications is the hamstrings (H)-toquadriceps (Q) (H:Q) torque ratio as an index of a strength imbalance between antagonistic muscle groups around the knee joint.1,2Identification of relative weakness in one muscle relative to the other can serve 2 main purposes:first,to identify athletes with strength imbalance in the pre-season period and then use this information to design appropriate training programs to restore H:Q ratio to“normal” levels3and improve their performance;4,5second,to identify imbalances after injury or other pathological conditions and use this information to design appropriate rehabilitation programs.6-8
The H:Q ratio can be calculated using various combinations of contraction types (concentric,eccentric,and isometric),angular velocities,and type of torque (peak or angle-specific torque).9The conventional ratio is calculated using torque values of the same contraction type for both antagonistic muscle groups.These include the concentric H:concentric Q (QCON);the eccentric H (HECC):eccentric Q;and the H:Q torque ratio.9It has been proposed that an isometric H:Q ratio of approximately 0.66 represents the average value in a typical population sample.10This is partly confirmed by a recent systematic review of evidence showing that the isokinetic conventional ratio,when tested at slow (12°/s) to intermediate (180°/s) angular velocities,is in the range of 0.52-0.67 and that it increases further at faster angular velocities.8
When the quadriceps produce force by shortening(concentric contraction),the hamstrings are activated as antagonists while lengthening (eccentric contraction).9For this reason,several authors have proposed that a more functional approach should be taken in the calculation of H:Q ratio1,11,12by considering the typical muscle actions during a knee extension.Therefore,the dynamic control12or functional11torque ratio has been established as the ratio of eccentric hamstrings torque over concentric quadriceps torque (HECC/QCON).Normative values for the functional ratio also vary depending on test angular velocity,being around 0.79 at 60°/s and exceeding 1 at angular velocities greater than 240°/s.8Another modification of the functional ratio is the mixed ratio,which is calculated by dividing the HECCtorque at an angular velocity of 30°/s by the QCONtorque at 240°/s.13Hence,by taking the HECCtorque at a slow speed and the QCONat a faster speed,the resultant H:Q ratio for the typical sport population would be centered around a value of 1.13According to the authors who proposed the mixed ratio,13,14the main advantage of this ratio is its greater experimental validity(i.e.,it is less affected by inertial artifacts).This is because the recorded torque at fast angular velocity tests shows better experimental validity in isokinetic fast angular velocity concentric contraction tests (QCONtorque at 240°/s) than in eccentric contraction tests,while eccentric torque values at a slow angular velocity(HECCtorque at 30°/s)have better validity than fast velocity tests.A recent review has examined the associations between different types of H:Q ratios,15but they did not systematically review the association of H:Q ratio with injury.
One important application of the H:Q ratio has been to monitor strength imbalances in individuals with anterior cruciate ligament (ACL) deficiency12,16or reconstruction.17,18This is based on the observation that the hamstrings co-contract near full extension and generate an opposing force to the anterior component of the quadriceps force.19,20This reduces anterior shear loading and contributes to a physiological range of motion and safer relative position of the femur and tibia bones in the knee joint,thus maintaining knee joint stability and reducing ACL load.19,20Consequently,it has been proposed that a low force generating capacity of the hamstrings relative to the quadriceps may be related to ACL injury and re-injury,especially in female athletes.21To our knowledge,published evidence on the association between H:Q ratio and ACL injury has not been reviewed.
An altered H:Q ratio is also frequently considered a risk factor for hamstring strains.22This is often attributed to a reduced relative ability of the hamstrings to control combined hip flexion and knee extension during dynamic movements such as sprinting or stretching.23,24Systematic reviews have shown that there is strong evidence that strength variables,including H:Q ratio,are not independent risk factors for hamstring injury.7,25However,these studies have examined H:Q ratio generically together with various other potential risk factors and,hence,specific issues that may influence H:Q ratio measurement and its relation to injury have not been considered.These include torque ratio measurement issues(e.g.,reliability,gravity correction,validity),calculation method and the type of ratio (e.g.,conventional,dynamic,mixed),and interpretation(e.g.,the determination of cut-off values).These considerations are very important because previous studies have identified methodological limitations and issues with the experimental protocol that influence the calculation of H:Q ratio.1,2These limitations are often underestimated,which may lead to erroneous interpretation of the obtained H:Q ratio values.While studies have advocated the use of one type of ratio over another for different applications,there is still confusion about which type of H:Q ratio is better for predicting or preventing injury.8The use of various types of H:Q ratios in combination with limitations in injury survey data collection and analysis may also influence conclusions regarding the usefulness of H:Q ratio for injury prevention.Three recent reviews6-8have shown that it is unclear whether H:Q ratio is sensitive enough to detect differences between injured and non-injured legs or between injured and non-injured individuals suffering from hamstring strains;these studies,however,did not examine the association between H:Q ratio and future injury.
The purpose of this systematic review was to examine the ability of different types of H:Q strength ratios to prospectively predict hamstrings and ACL injuries in athletes.Two specific questions were addressed in this review: (a) Is the H:Q ratio a significant risk factor for ACL and hamstring strains and,if so,which type of H:Q ratio shows a greater association with injury?and (b) do methodological issues and limitations influence the association between H:Q ratio and ACL or hamstring injuries?
2.Methods
2.1. Search strategy and selection of studies
This review was not registered.A comprehensive,multistep search strategy using Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)guidelines was performed in June 2021 using the (Population,Intervention,Comparison,Outcomes of interest;PICO)framework for prognostic studies to identify all relevant articles in 4 electronic databases:26PubMed,MEDLINE,Cochrane Library,and Scopus.Population:sport athletes;problem:hamstrings or ACL injury;prognostic factor: ipsilateral strength ratios;comparison: prospective comparison of injured and uninjured groups;and outcome:hamstrings or ACL injury and associated risk estimates.The electronic databases were searched independently by 2 authors(EK and CS),to reduce the probability of study selection bias,with no limit for year of publication.The following combination of terms with the proper Boolean(“AND”,“OR”,and “NOT”) operators were used: “isokinetic strength” or “strength ratio” or “strength balance” or“hamstrings to quadriceps ratio” or “knee flexors to knee extensors ratio” or “hamstrings injury” or “posterior thigh injury” or “hamstring strain” or “hamstring tear” or “anterior cruciate ligament injury” or “anterior cruciate ligament rupture” or “risk factors” or “predictor” or “prediction” or“prevention”.Additionally,secondary searches were conducted by screening the reference list of the selected studies and by evaluating the reference list of previous related reviews.After duplicates were removed,2 independent reviewers (EK and CS)assessed the potential studies by comparing the lists of included and excluded studies.Any discrepancies between the 2 authors(EK and CS) with regard to the included and excluded studies were resolved through discussion and consensus.
2.2. Eligibility criteria
Studies that satisfied the following criteria were included in the review: (a) publications in international English-language peer-reviewed journals,(b)studies that examined healthy individuals of any age and playing level (ex-athletes or athletic populations) with subsequent occurrence of hamstring muscle or ACL injury during either a sport and competition-related activity or training period,and (c) studies that employed any type of H:Q strength ratio (conventional,functional,and mixed) as a measurement outcome to investigate the risk of injury.Reviews,case and brief reports,letters to editors,thesis,and conference abstracts were excluded.
2.3. Risk of bias assessment
The methodological quality of the included studies was independently examined by 2 reviewers (CS and EK) using a modified version of the Quality In Prognosis Studies tool described by Hayden et al.27This risk of bias assessment tool examines 6 potential bias domains (study participation,study attrition,prognostic factor measurement,outcome measurement,study confounding,and statistical analysis and reporting) to evaluate different aspects of the potential risk of bias in prognostic studies.7Each of the 6 study design elements contain 5-7 items of potential bias that were evaluated according to specific criteria used to examine the degree of risk with a score of“yes”or“no”.If fewer than 75%of the items within a single category were scored with a “yes”,this domain was determined to have a “High risk” of bias,while“Low risk” of bias was considered if the number of items scored with“yes”was greater than or equal to 75%.To obtain an overall low risk of bias,a study should have a low bias on at least 5 of the 6 domains and the outcome measurement.The domain “outcome measurement” (Domain 4) refers to 3 criteria: first,whether the study provides a clear definition of the outcome measurement;second,whether information about the validity and reliability of the measurements is provided;and,finally,whether the same methodology was applied for all participants.
2.4. Data extraction
Two authors (EK and VB) independently extracted the following data from each study to an Excel spreadsheet(Microsoft Office Excel 2016;Microsoft,Redmond,WA,USA): (a)authors and year of publication,(b)details regarding the characteristics of participants who underwent isokinetic evaluation(such as sample size,sport,and sex),(c)methodological characteristics(test angular velocity,types of ratios,gravity correction,participant position,and reliability measures),(d)study duration,(e) strength ratio data,and (f) key findings related to injury prediction.
2.5. Data synthesis and analysis
Preliminary evaluation of the identified literature indicated relatively few studies examining different versions of the H:Q ratio.Further,the data from various studies originated from different sports,and this might have influenced the heterogeneity of the sample for each specific ratio type.For this reason,the final number of studies for each type of H:Q ratio was considered insufficient for meta-analysis.Therefore,a best evidence synthesis7was used to facilitate the interpretation of data derived from included studies.It consisted of a 5 levels of evidence-based qualitative analysis:
1.Strong evidence:consistent results in 2 or more low risk of bias studies (high quality),with generally consistent findings in ≥75%of studies.
2.Moderate evidence: provided by 1 low risk of bias study(high quality)and/or 2 or more studies with high risk of bias(low quality) and by generally consistent results across all studies(≥75%of the studies reported consistent findings).
3.Limited evidence: provided by single-study findings from high risk of bias study(low quality).
4.Conflicting evidence: inconsistent findings in multiple studies(<75%of the studies reported consistent findings).
5.No evidence:no studies(randomized controlled trials or nonrandomized controlled trials)available for assessment.
Best evidence synthesis of the included studies was applied twice: first,to examine the association of each H:Q ratio type and injury across all sports;and second,to examine the association of H:Q ratio and injury in each sport.
3.Results
3.1. Search results
A total of 10,154 potentially relevant published studies were identified through the electronic search (Fig.1).Of these,4032 duplicate articles were removed,while after title and abstract screening,6083 documents were excluded.Of the remaining 41 articles,18 additional studies were excluded on the basis of fulltext screening.Therefore,23 articles were retained.
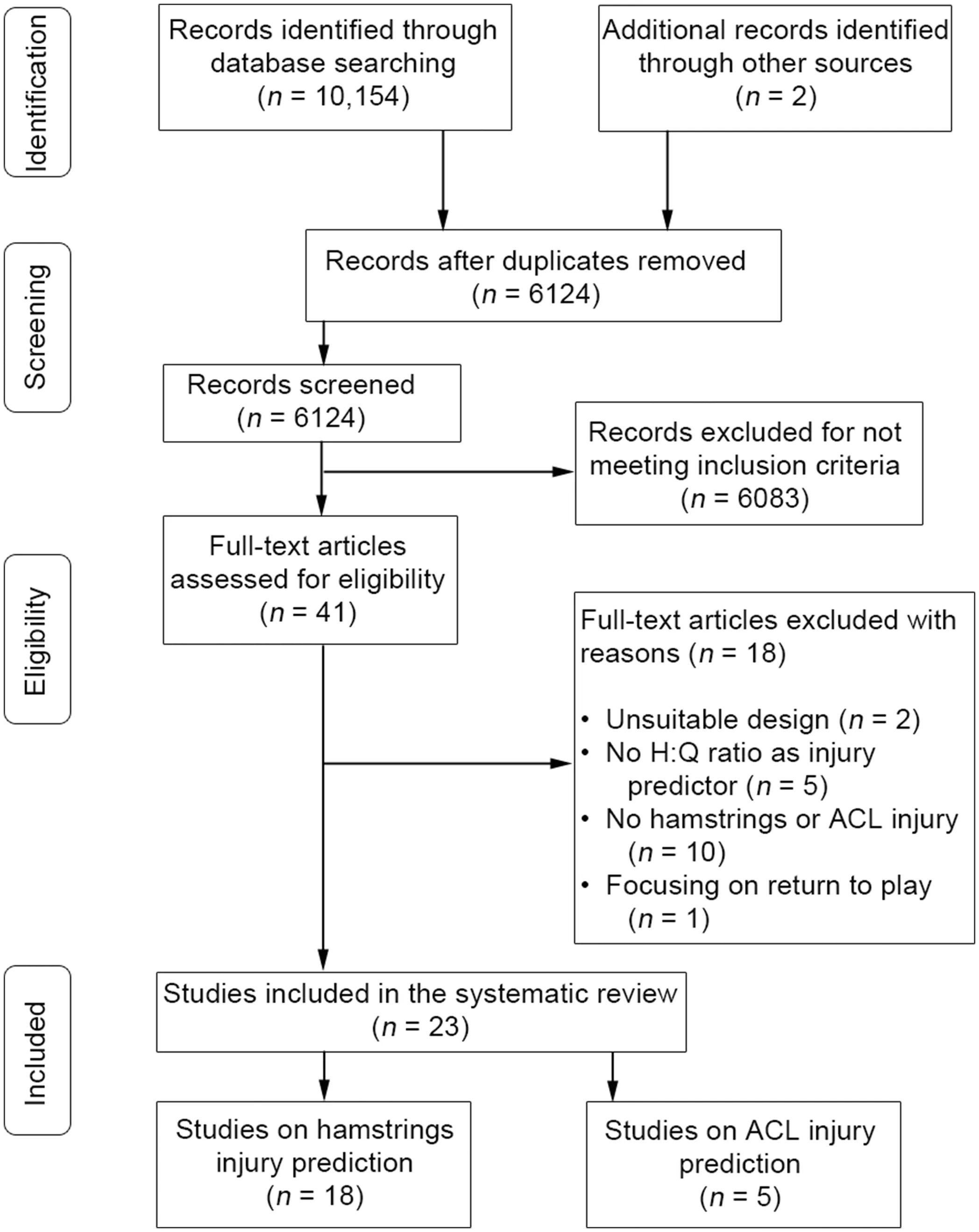
Fig.1.Search flow diagram.ACL=anterior cruciate ligament;H:Q=hamstrings-to-quadriceps torque ratio.TagedEnd
3.2. Description of the included studies
Of the 23 studies included in this review,18 studies examined hamstring injuries and 5 studies examined ACL injuries.These studies documented 585 hamstrings injuries in 2945 participants across football (soccer),3,13,28-36Australian rules football,37-39sprinting,40,41American football,42and Rugby.43Additionally,128 ACL injuries in 2772 participants across football (soccer),44,45basketball,44,46,47handball,45floorball,46and in military academy cadets.48
From the included studies,demographics,strength measurement methodology,and main data treatment techniques were tabulated.Further,H:Q torque ratio values (mean and SD) for injured and control groups were visualized according to type of H:Q ratio as well as type of injury.
3.3. Methodological characteristics of the included studies
The details of prospective studies are presented in Table 1.Some studies on hamstring injury have examined more than 1 type of ratio.Hence,14 studies3,13,28,31,33-39,41-43measured the conventional H:Q ratio,6 studies3,29,32,37,40,41used the functional H:Q ratio,and 5 studies3,13,33-35examined the mixed ratio,while there were some studies that calculated a different version of the strength imbalance between the 2 muscle groups.30,40Of the 5 included studies on ACL injury,all of them examined the conventional ratio,44,45-48only 1 examined the functional ratio,48and none of them assessed the mixed ratio(Table 1).All studies except for 232,44used a slow angular velocity (60°/s),7 studies3,31,32,37,38,41,43used a 180°/s test,7 studies3,13,33-36,41used a 240°/s test,4 studies used a 300°/s test,29-31,38while only one3used a 120°/s angular velocity test.
Twelve of the included studies3,13,28-30,37-40,44,45,47evaluated strength from a seated position (hip angle range 80°-105°),while the remaining 11 studies31-36,41-43,46,48did not specify the participant testing position(Table 1).Additionally,only 9 studies3,13,31,33,34,37,38,40,48included information regarding gravity correction procedure,and only 4 studies3,41,45,46reported the reliability of their H:Q ratio measurements.Twenty-one studies calculated H:Q ratio using peak torque values,and only 2 studies29,41used both peak and angle-specific H:Q ratios.
3.4. Risk of bias assessment
The scores on the potential risk of bias domains of the included studies are presented in Fig.2.Particularly,11 studies on hamstring injury were scored as low risk,while the remaining 7 studies had a high risk (Fig.2).Of the 5 studies that examined ACL injury risk,3 were rated as low risk of bias and 2 were rated as high risk of bias(Fig.2).
3.5. Main findings
Fig.3 presents the reported conventional H:Q ratios for groups with and without hamstring and ACL injury,while the corresponding data for the functional,mixed,and other ratio types are presented in Fig.4.Of the 18 studies,non-significant differences between injured and uninjured groups or legs were reported by 14 studies on hamstring injury,while none of the included studies reported differences between ACL injured and non-injured athletes.
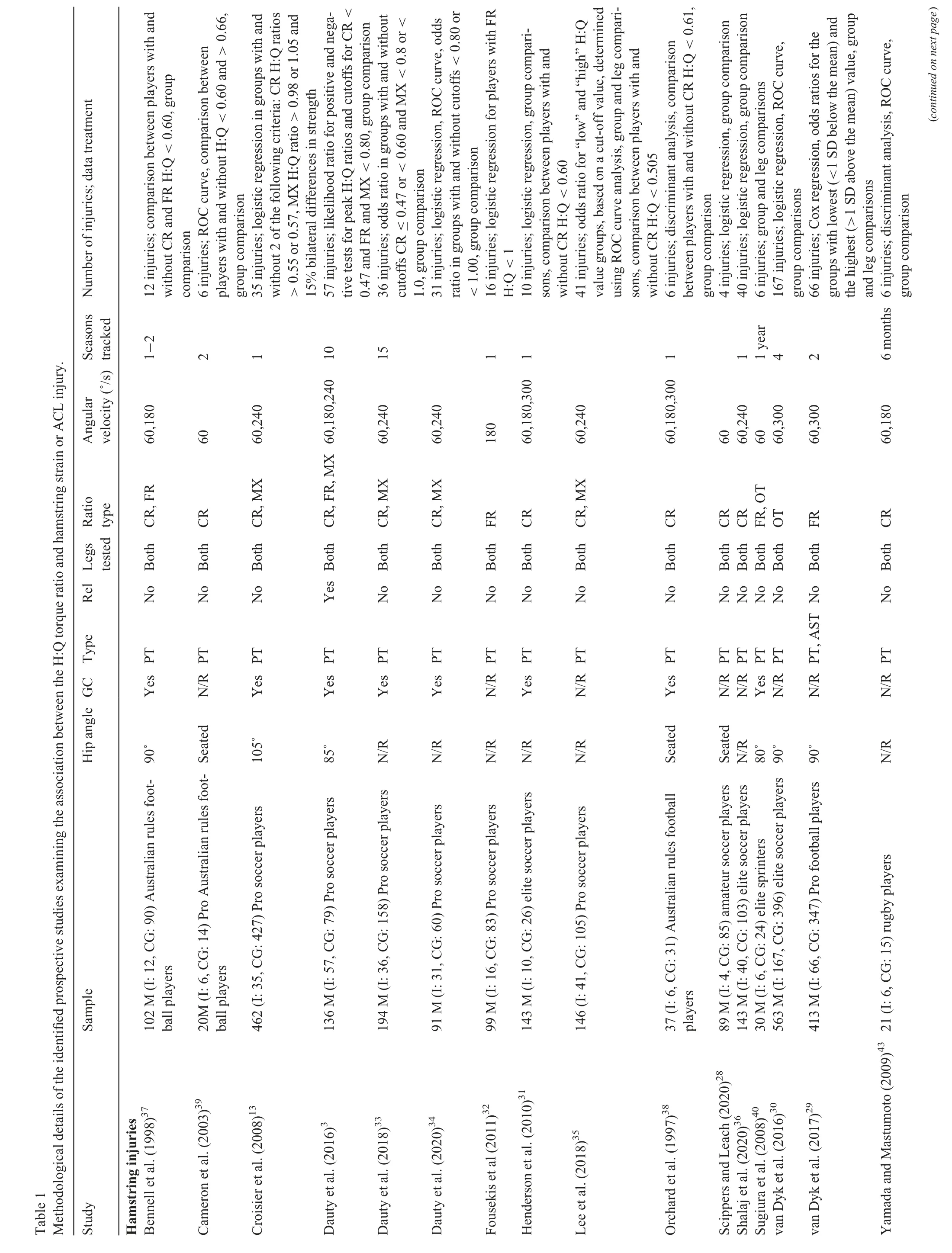
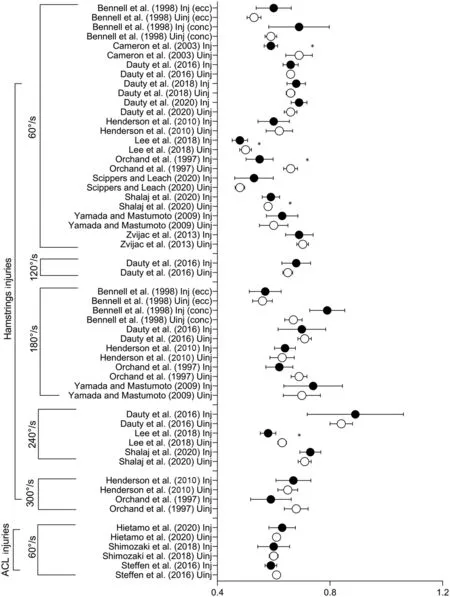
Fig.3.Mean conventional H:Q torque ratio values of Inj and Uinj groups reported by the studies included in this review.For all studies but that of Sugiura et al.,40 95%CI were estimated based on the reported means,SDs,and study sample sizes.Solid circle means injured and circle means uninjured.*p <0.05,significant differences between groups.95%CI=95%confidence interval;ACL=anterior cruciate ligament;conc=concentric;ecc=eccentric;H:Q=hamstrings-to-quadriceps;Inj=injured;Uinj=uninjured.
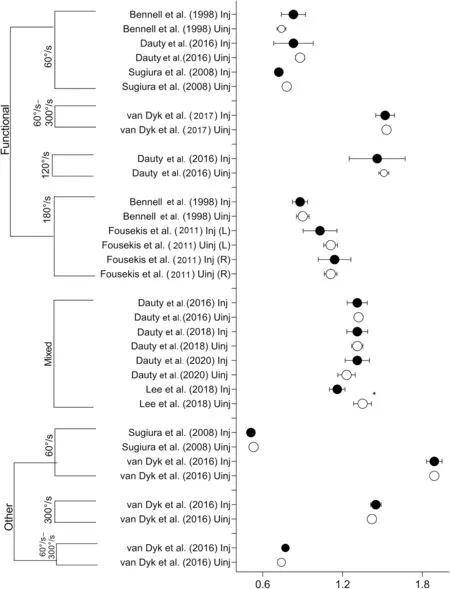
Fig.4.Mean (95%CIs) functional,mixed,and other type of H:Q torque ratio values of groups with (Inj) and without (Uinj) hamstring injury reported by the studies included in this review.For all studies but that of Sugiura et al.,40 95%CIs were estimated based on the reported means,SDs,and study sample sizes.Solid circle means injured and circle means uninjured.*p <0.05,significant differences between groups.95%CI=95%confidence interval;H:Q=hamstrings-to-quadriceps;Inj=injured;L=left;R=right;Uinj=uninjured.
The main findings of the included studies are presented in Table 2.Of the 14 studies,11 reported no association between conventional H:Q ratio measurements at 60°/s and hamstring injury,3,13,28,31,33,34,36,37,41-43while 4 studies31,37,38,43reached a similar conclusion using an H:Q ratio at 180°/s.Similarly,non-significant associations with hamstring injury were reported by 5 (out of 6)studies3,29,32,37,41for the functional ratio and by 4 (out of 5)studies for the mixed ratio.13,33-35Of the studies listed above,only 4 showed a high risk of bias.3,32,37,43In contrast,of the 18 total studies that examined the H:Q ratio following hamstring injury,only 53,35,38-40reported a significant association,of which,3 were rated as having a high risk of bias.35,38,39None of the prospective studies reported a significant association between H:Q ratio and ACL injury.Of the 5 studies44,45-48that looked at this potential association,2 studies44,45had a high risk of bias(Table 2).
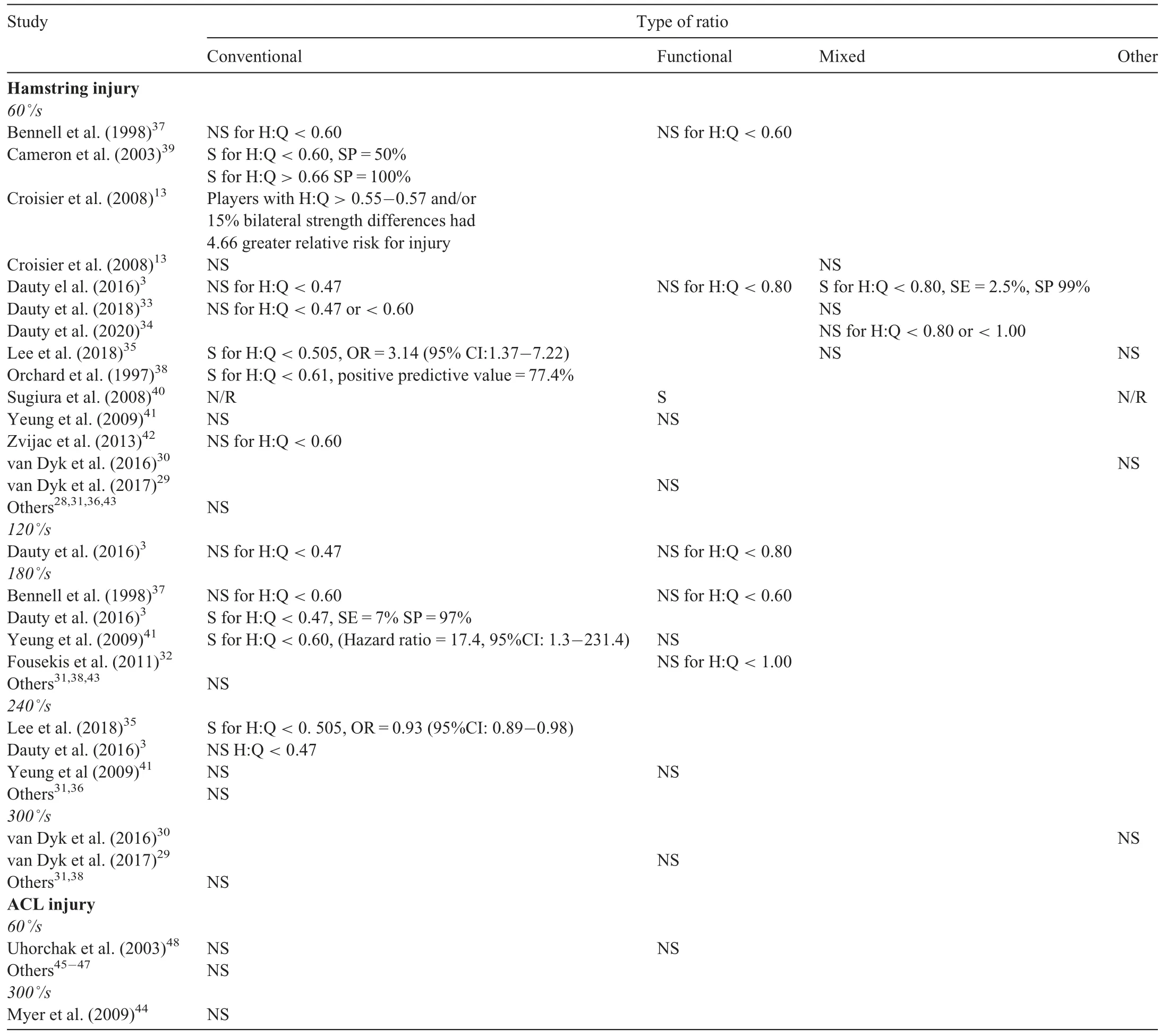
Table 2 Results of the included studies on the association between the H:Q ratio and hamstring or ACL injury.
Summarizing the results for each individual sport indicates that 11 studies3,13,28-36examined soccer players,of which,9 reported a non-significant association.13,28-34,36There was also no association reported for American football42and rugby43players.Out of the 3 studies37-39that examined Australian rules football athletes,2 reported a significant association between a different type of H:Q ratio and hamstring injury.38,39In addition,2 studies in sprinters40,41reported significant associations between injury and a specific H:Q ratio type.As for ACL injuries,no association with injury was reported by all included studies.
3.6. Best evidence synthesis
Best evidence synthesis strongly indicated that neither the conventional ratio at 60°/s and 240°/s,the functional ratio at 60°/s,nor other strength ratios were associated with hamstring injury risk (Table 3).Moderate evidence for no association was found for the conventional H:Q ratio at 300°/s and the functional H:Q ratio at 180°/s.There was also limited evidence for no association with injury for the conventional H:Q ratio at 120°/s,the functional H:Q ratio at 60°/s,120°/s,240°/s,and 300°/s.Finally,evidence for the conventional H:Q ratio at 180°/s and the mixed ratio was conflicting.For ACL injuries,there is strong (conventional ratio) or limited (conventional ratio at 300°/s and functional ratio) evidence that the H:Q ratio is not associated with injury (Table 3).
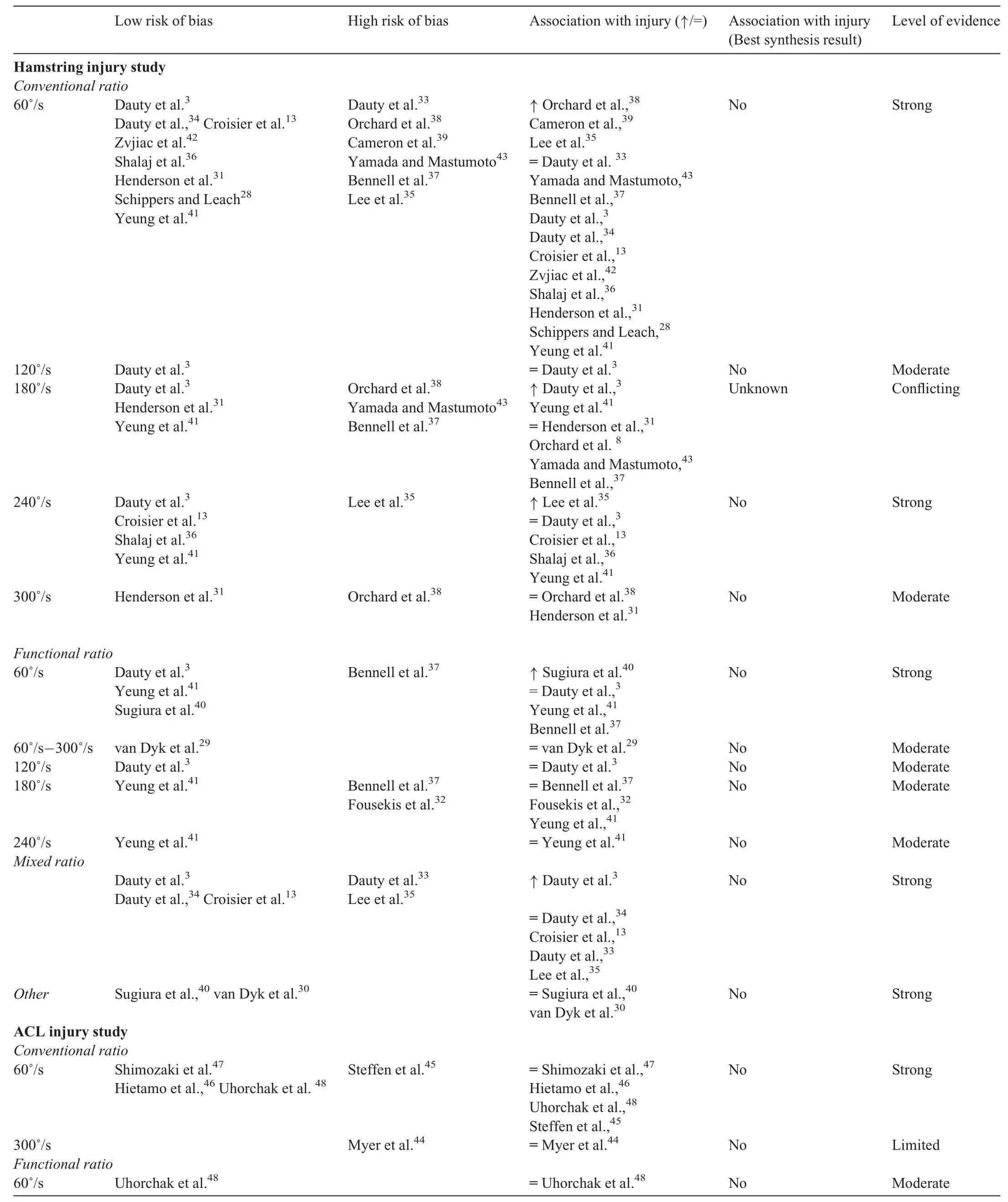
Table 3 Results of best evidence synthesis of studies for each H:Q ratio.
Table 4 presents the results of best evidence synthesis analysis for each sport.For Australian footballers,there was limited to moderate evidence that H:Q ratios are not associated with hamstring injury;exception was the conventional H:Q ratio at 60°/s,where the evidence was conflicting.Similar results were also found for soccer players.For sprinters,there was conflicting evidence for one H:Q ratio type,moderate evidence for no association with injury for 2 ratio types,and moderate evidence for an association between injury and the conventional H:Q ratio at 180°/s.As for ACL injuries,there was limited to strong evidence of no association with H:Q ratio for all sports.
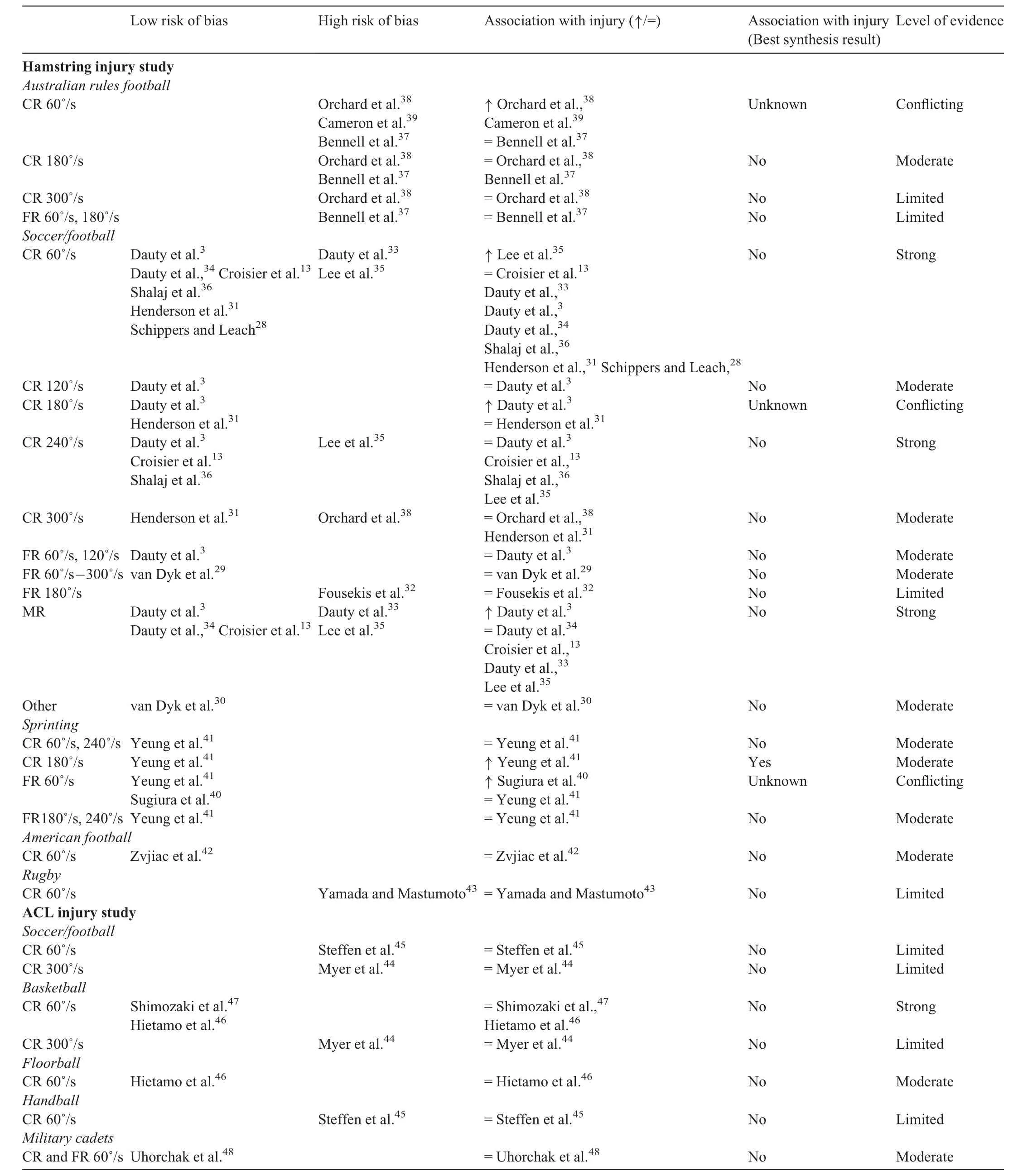
Table 4 Results of best evidence synthesis analysis of studies that examined the association of injury and H:Q ratio for each sport.
4.Discussion
The results of this review indicate that there is moderate-tostrong evidence that the H:Q strength ratio is not an independent risk factor for either hamstring or ACL injury.This result applies for both the conventional and functional H:Q ratio,while evidence for the mixed H:Q ratio is conflicting.Several methodological limitations and differences between studies might have influenced these results.
4.1. Association of H:Q ratio with injury
With respect to the first question raised in this study,bestevidence-synthesis analysis has shown that the H:Q ratio is not associated with hamstring and ACL injury (Table 3).Overall,of the 15 studies with low risk of bias,only 33,13,41reported that the H:Q ratio is a significant risk factor for hamstring strain,while all studies found that there is no association of H:Q ratio and ACL injury (Table 3).The mean group values reported by various studies show some similarity.In particular,the conventional ratio values at 60°/s are centered around 0.60 (Fig.2),the functional ratios at 60°/s around 0.80,and the mixed ratios around 1.30(Fig.3).Nevertheless,the variability in each measurement in both injured and non-injured groups prevents users from deciding which value should be considered as typical and which ones might be indicative of injury risk.Therefore,it is not certain that an individual who has an H:Q ratio that is almost 2 SDs less than the average group value is at increased risk for injury.On the other hand,it is also not certain that an individual who displays an H:Q ratio that is similar to the average group value has a lower risk for sustaining an injury.This substantial overlap between players with high and low risk of injury is seen in almost all existing screening tests.49
This study also explored whether different types of H:Q ratio have greater association with injury.However,current evidence indicates that the functional ratio does not offer a greater injury predictive capacity than the conventional one,while evidence on the value of the mixed ratio is conflicting(Table 3).It should be mentioned,however,that of the total 15 studies with lower risk bias,only 5 examined the functional ratio and 2 examined the mixed ratio (Table 1).This indicates that there is much more evidence available for the conventional ratio than for the other ratio types.Furthermore,no studies have examined the association of the mixed H:Q ratio and ACL injury (Table 1).Collectively,these results indicate that the limitations of the conventional ratio as an injury screening tool are not overcome if a more “functional” approach in the H:Q ratio calculation is followed.
There are various factors that may have influenced these results.In particular,studies used different H:Q cutoff values to discriminate the sample (Table 2).The cutoff values varied from 0.47 to 0.66 for the conventional ratio at 60°/s,from 0.78 to 1.05 for the functional H:Q ratio (across speeds),and from 0.80 to 1 for the mixed H:Q ratio.This could be attributed mainly to differences in the method used to determine these cutoff values as well as to the size of the sample examined in each study.Some studies tested the idea that the optimum value of the conventional H:Q should be 0.60;37,42others determined cutoff values by calculating the area under the curve of receiver operating characteristics based on the raw data29,30,34,35,39,41,43(Table 1);still others tested the cutoff values reported by previous experiments.3,32,33Perhaps the most influential study is that done by Croisier et al.,13which examined an almost 4 times greater number of players than all other studies.13These authors did not find a significant association between the conventional H:Q ratio at a specific angular velocity and injury (Table 2).They observed,however,that injured athletes showed a much greater deficit in HECCtorque at 30°/s than that observed for QCONtorque at 240°/s.Hence,they were able to show that soccer players had a 4.66 times greater risk of sustain a hamstring injury if they met 2 of the following criteria:a conventional ratio less than 0.55,a mixed ratio greater than 0.98,and/or 15% bilateral differences in strength when compared with players showing no imbalance in the preseason.Based on the suggestions made by these authors,the H:Q ratio should be combined with bilateral differences in strength to detect players who are at greater injury risk.The use of these specific cutoff values,however,was based on previous experiments in a very small number of players,14and hence,it has been criticized.50,51In addition,the cutoff values proposed by Croisier et al.13were tested by other studies,3,32,33which reported a non-significant association between H:Q ratio and hamstring injury.In the most recent of those prospective studies,Dauty et al.33failed to find a significant prediction of hamstring injury for a wide range of the conventional and mixed H:Q ratio cutoff values.
Another factor that contributed to the present findings is that the conditions at which the H:Q ratio is measured have limited association with muscle function at the instant of injury.Hamstring injuries are frequently attributed to different mechanisms,one occurring during high-speed sprinting and the other occurring during excessive stretching.23,24ACL injuries occur during the deceleration phase of dynamic movements,such as landing from jumping or change of direction,while the knee is near full extension,frequently in combination with knee valgus and internal/external tibial rotation.52In these movements,the hamstrings work at relatively long muscle lengths.Evidence indicates that isokinetic strength has moderate correlation with kicking53or sprinting,54but this relationship is lower between H:Q ratio and performance,55obviously,because H:Q ratio is an expression of the relative maximum strength when each muscle works as agonist and not the torque that is exerted simultaneously by the 2 antagonist muscles.56Related to this is the criticism that the position and speed of testing do not resemble actual conditions,such as sprinting or change in direction.7In the included studies,isokinetic testing angular velocities ranged from 60°/s to 300°/s (Table 1),which are lower than those developed during fast sport movements,such as fast kicking (~550°/s-1720°/s,57sprinting(~500°/s-800°/s),58or landing (~78°/s-570°/s).59,60This may also explain the observation that angular velocity does not influence the association of H:Q ratio with injury (Table 2).For this reason,evaluation of the conventional or functional H:Q at a slow angular velocity,such as 60°/s,is recommended.
An important contributor to the low predictive capacity of the H:Q ratio is the multifactorial origin of both hamstring22and ACL61,62injuries.Although various factors are often considered to increase the risk for sustaining an injury,very few of them have been identified as independent risk factors for hamstring22or ACL61,62injury.Hence,preseason evaluation of strength imbalances between antagonistic muscle groups may not identify all players who are at a greater risk for sustaining an injury unless it is part of a wider screening program with a broader range of risk factors examined.Future studies that use multifactorial designs that incorporate measurements of various modifiable factors may assist in this direction.63
Another observation is that all included studies have calculated H:Q ratio using peak torque during the test (Table 1).The H:Q ratio changes throughout the range of motion due to differences in torque-joint angular position curves between the quadriceps and the hamstrings.Hamstrings torque is generally greater near full extension,reaching peak values at 40°of knee flexion.56In contrast,peak quadriceps torque is smaller near full extension,reaching its peak at 60° of knee flexion.56Hence,starting from 90° of knee flexion,the H:Q torque ratio is very low,and it increases almost linearly,reaching its peak at approximately 30°-20° of knee flexion with values around 1.56,64Taking the peak torque provides an index of the maximum strength generation capacity of each muscle,but it may not reflect the instantaneous relationship between hamstrings and quadriceps torque that occurs at a specific joint position.In theory,the use of anglespecific H:Q torque is ecologically more valid as it is closer to the injury mechanism of the ACL64,65as well as the hamstrings muscles.66,67Nevertheless,only 2 low-risk studies29,41examined angle-specific strength values,and they reported that the resulting H:Q ratio has no association with hamstrings injury.
4.2. Methodological issues
The second aim of this study was to identify methodological aspects of the included studies that may have had an influence on the results(Table 1).First,it was observed that only 3 low-risk studies3,41,46examined the reliability of measurements,which appeared to be moderate or high (intraclass correlation coefficients: 0.80-0.98 for peak torque values).Studies have shown a moderate reliability of H:Q ratios in repeated sessions.68-70Impellizzeri et al.70noticed lower H:Q values for the first session as compared with the second and third sessions,suggesting a learning effect.Neuromuscular inhibition,which often takes place during eccentric testing,has also been considered as an important threat to the reliability and validity of the functional or mixed H:Q ratio.33In fact,these studies have shown that percentage changes in H:Q should be greater than 18%68or even 28%69to detect real changes.None of the included studies have identified such large differences in any type of ratio (Figs.3-4) between injured and non-injured athletes.This represents an important limitation of most studies,and it should be taken into consideration when interpreting the results of this review.In addition,threats to the validity of the H:Q ratio,such as gravitational torque1and inertial force,71are often not considered.Using the peak torque value during the non-isokinetic phase of the torque-angle curve,for example,may lead to an error of up to 16%at an angular velocity of 300°/s.71This may influence the association of H:Q ratio with injury in a specific cohort,and it also provides erroneous conclusions regarding the extent of muscle imbalances in these particular athletes.
Differences in injury recording methodology between studies might also have had an influence on the results of this review.First,several studies examined a relatively small sample of players reporting a low number of injuries.For example,5 out of 15 studies with low risk of bias reported less than 16 injuries each (Table 1).In this case,comparisons between injured and uninjured players is based on unequal sample sizes,and this can dramatically influence the statistical power of the results.72More important,with a small sample size,the validity of using specific cutoff values to discriminate the sample is questionable.Second,concerns have been raised regarding the definition,type,and severity of injury in various studies.13For example,hamstring muscle strains can be mild,moderate,or severe,73or they may be sprint-type or stretchtype.23,24Studies included in this systematic review did not identify the mechanism that led to the registered injury.One may hypothesize that sprint-type and stretch-type injuries exhibit differences in muscle function and that,hence,a single preseason measurement of H:Q ratio is inadequate for predicting both injury types.Third,inclusion of athletes with a history of injury may also influence the results as previous injury history may increase injury risk.33All but 2 studies31,44included in this review excluded individuals with a previous injury incident from their sample.Finally,the reviewed literature provided evidence for the association of H:Q ratio with injury in a specific sample.Based on Bahr,49this is only the first step for an effective screening strategy.The next step is validating the cutoff values using a new sample and the final step is to test whether a prevention program can reduce risk of injury in those athletes who are classified as high risk based on their screening results.
An additional factor related to the heterogeneity of the samples’characteristics is that the participants were athletes from various sports,each with different performance demands (Table 1).Re-examination of our data collected on ACL injuries indicates it is unlikely that the type of sport influenced the results,as all studies failed to show an association between ACL injury and H:Q ratio(Table 4).As for the hamstring injuries,studies in American football,rugby,and soccer athletes indicated no association with H:Q ratio (Table 4).Interestingly,for Australian rules football athletes37-39and sprinters,38,39there was evidence that supports a significant association,but this originates from studies with high risk of bias.38,39For this reason,there was moderate evidence for a significant association with injury in only 1 case(Table 4).Overall,based on the collected evidence,it appears that the absence of association between H:Q ratio and hamstring injury is common in all sports.Nevertheless,subject to more evidence,the possibility that a different association exists for sports such as sprinting or Australian rules football cannot be excluded.
4.3. Implications
There are important implications to be gleaned from the findings of this review.First,due to the low association between H:Q ratio and injury,one may suggest that preseason evaluation of muscle strength imbalance is not useful for identifying players with a greater risk potential.This does not indicate that preseason evaluation of strength should not be performed.Previous studies have shown that strength training may prevent hamstring injuries and,therefore,monitoring of strength is necessary.74There have been suggestions that other tests such as Nordics,hand-held dynamometers,or force plates may substitute or complement isokinetic testing for better injury prediction results.7,75However,it should be stressed that these tests have no76or only moderate correlation with performance,77and there is no evidence that they are associated with injury.29Isokinetic dynamometers offer maximum resistance throughout the movement at both concentric and eccentric conditions,and they can be used to monitor strength progress of players effectively,safely,and correctly.Obviously,any test that is performed under controlled laboratory conditions is not expected to have a direct association with muscle function during movements that lead to injury.This observation aligns with the latest research by Bahr,49who commented that “any existing screening test is unlikely to be able to predict injury with sufficient accuracy”.
Strength levels are greater in the preseason period and tend to decrease over the in-season period.78It is possible that some players display greater strength losses than others and that this may influence their performance and injury risk.Further,while preseason evaluation levels provide an evaluation of strength imbalances,it is unclear how in-season training influences strength imbalances.For example,it has been shown that preseason strength was reduced after a 12-week in-season soccer training period without any strength training.78Performance of one strength training session per week during the in-season period maintained strength,79while strength training twice a week may decrease strength due to overtraining.80This indicates that injury epidemiology studies should monitor strength sessions adopted by players during the in-season period as they may affect strength imbalances relative to the preseason measurements.In addition,monitoring strength imbalances at selected time instances during both the preseason and in-season periods will allow for a closer examination of the association between injury and strength imbalance by using strength values obtained during the specific period when the injury occurs.
Limitations of this review are acknowledged.First,we restricted eligibility to studies in English only while we searched 2 of the 4 databases.Second,we did not contact study authors to request clarifications where needed;instead,we extracted information from the published data and cross-checked our results with those reported by previous meta-analysis studies.
5.Conclusion
Preseason evaluation of H:Q ratio has limited value for the prediction of hamstring and ACL injuries.The type of H:Q ratio does not influence the association with injury.Monitoring strength imbalances along with other modifiable factors during the entire competitive season may provide a better understanding of the association between H:Q ratio and injury.
Authors’contributions
EK conceived the idea for the manuscript and wrote the first versions of the manuscript;CS and VB provided intellectual contribution as part of the redrafting process within their areas of expertise.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Data availability
https://data.mendeley.com/datasets/vpp87gykvh/draft?a=9f05cca6-878c-4aa0-9808-7cbcb1171246
 Journal of Sport and Health Science2023年3期
Journal of Sport and Health Science2023年3期
- Journal of Sport and Health Science的其它文章
- Impact loading in female runners with single and multiple bone stress injuries during fresh and exerted conditions
- Are EPB41 and alpha-synuclein diagnostic biomarkers of sport-related concussion?Findings from the NCAA and Department of Defense CARE Consortium
- Factors and expectations influencing concussion disclosure within NCAA Division I athletes:A mixed methodological approach
- Effects of contact/collision sport history on gait in early-to mid-adulthood
- Refinement of saliva microRNA biomarkers for sports-related concussion
- Lacrosse-related injuries in boys and girls treated in U.S.emergency departments,2000-2016