
Acute heart failure as an adverse event of tumor necrosis factor inhibitor therapy in inflammatory bowel disease: A review of the literature
2023-05-25 02:44ThaisGagnoGrilloCarolineFerreiradaSilvaMazetoPupoSilveiraAnaElisaValenciseQuaglioRenatadeMedeirosDutraJulioPinheiroBaimaSilmeiaGarciaZanatiBazanLigiaYukieSassaki
World Journal of Cardiology 2023年5期
Thais Gagno Grillo,Caroline Ferreira da Silva Mazeto Pupo Silveira,Ana Elisa Valencise Quaglio,Renata de Medeiros Dutra,Julio Pinheiro Baima,Silmeia Garcia Zanati Bazan,Ligia Yukie Sassaki
Thais Gagno Grillo,Caroline Ferreira da Silva Mazeto Pupo Silveira,Renata de Medeiros Dutra,Julio Pinheiro Baima,Silmeia Garcia Zanati Bazan,Ligia Yukie Sassaki,Department of Internal Medicine,Medical School,São Paulo State University,Botucatu,Botucatu 18618686,Brazil
Ana Elisa Valencise Quaglio,Department of Biophysics and Pharmacology,Institute of Biosciences,São Paulo State University,Botucatu,Botucatu 18618689,Brazil
Abstract Tumor necrosis factor inhibitors (anti-TNFs) are widely used therapies for the treatment of inflammatory bowel diseases (IBD); however,their administration is not risk-free.Heart failure (HF),although rare,is a potential adverse event related to administration of these medications.However,the exact mechanism of development of HF remains obscure.TNFα is found in both healthy and damaged hearts.Its effects are concentration- and receptor-dependent,promoting either cardio-protection or cardiomyocyte apoptosis.Experimental rat models with TNF α receptor knockout showed increased survival rates,less reactive oxygen species formation,and improved diastolic left ventricle pressure.However,clinical trials employing anti-TNF therapy to treat HF had disappointing results,suggesting abolishment of the cardioprotective properties of TNFα,making cardiomyocytes susceptible to apoptosis and oxidation.Thus,patients with IBD who have risk factors should be screened for HF before initiating anti-TNF therapy.This review aims to discuss adverse events associated with the administration of anti-TNF therapy,with a focus on HF,and propose some approaches to avoid cardiac adverse events in patients with IBD.
Key Words: Tumor necrosis factor inhibitors; Inflammatory bowel disease; Heart failure; Adverse event; TNFα receptor
INTRODUCTION
Inflammatory bowel disease (IBD),including Crohn's disease (CD) and ulcerative colitis (UC),presents with chronic and progressive intestinal inflammation with periods of remission and activity,affecting mainly young people,with a peak of incidence between the third and fourth decades of life[1].The etiopathology of IBD is poorly established,but it is believed to be related to an inappropriate inflammatory response to gut microbes in predisposed individuals[2].There is still no curative therapy for IBD.Thus,treatment aims to alleviate symptoms,restore quality of life,and delay the progression and development of complications[3].The choice of therapy depends on the location,activity,and severity of the disease,along with previous response to therapy and presence of complications.Evaluation of individual patient characteristics and the cost/benefit ratio of medications are also considered[4].The therapeutic arsenal currently includes aminosalicylates (mesalazine and sulfasalazine); local and systemic corticosteroids (budesonide,prednisone,methylprednisolone,and hydrocortisone); immunosuppressants (azathioprine and 6-mercaptopurine); JAK inhibitors (tofacitinib); and biological therapies such as tumor necrosis factor inhibitors (anti-TNFs; infliximab,adalimumab,certolizumab pegol,and golimumab),anti-integrin antibody (vedolizumab),and anti-IL-12/23 antibody (ustekinumab)[4].As anti-TNFs are widely used therapies,their adverse effects should be recognized in a timely manner to avoid patient morbidity and mortality.They are administered for the induction and maintenance of therapy in patients who fail to respond to conventional therapy.Infliximab,adalimumab,and certolizumab pegol are approved for use in CD.and infliximab,adalimumab,and golimumab,in UC[4].Contraindications to their use include active infection,demyelinating disease,cancer,and heart failure (HF) [absolute in the New York Heart Association (NYHA) functional classification III-IV][5].This review aims to discuss adverse events due to the use of anti-TNF therapy,with a focus on HF.Additionally,we performed a literature review on cases of HF secondary to the use of anti-TNFs in patients with IBD.
ADVERSE EVENTS WITH USE OF ANTI-TNF THERAPY
Infliximab is a human-mouse chimeric monoclonal antibody administered intravenously.Adalimumab and golimumab are fully humanized monoclonal antibodies that are injected subcutaneously.Certolizumab pegol is a conjugated Fab antibody fragment administered subcutaneously.In CD,anti-TNFs (infliximab,adalimumab,and certolizumab pegol) are indicated for inducing remission in moderate-tosevere disease with inadequate response or intolerance to conventional therapy (steroids and/or thiopurines).They are effective in patients who are biological therapy-naive and biological therapyrefractive.Patients who achieved remission with anti-TNF agents need to continue the maintenance treatment.The effects of suspending anti-TNF therapy after long-term remission are not established; therefore,the decision must be individualized.In cases of complex perianal fistulas,the use of infliximab or adalimumab is recommended for induction and maintenance[4].In UC,anti-TNFs are recommended in cases of moderate-to-severe active colitis,along with adalimumab,golimumab,or infliximab for inducing remission[6].These drugs are recommended as maintenance therapy with or without thiopurines in patients who attained remission.In severe acute colitis refractory to intravenous steroids,infliximab may be a therapeutic rescue therapy[6,7].Hypersensitivity reactions are among the most common adverse events with administration of anti-TNFs; they are either acute (during or within 24 h of the infusion) or delayed (24 h to 14 d after the infusion)[8].The acute reactions are rapid in approximately 2% of the reactions,but < 1% lead to a severe reaction[9].The presence of antibodies against infliximab increases the risk of infusion reactions[10],and case studies suggest that hypersensitivity to adalimumab is also due to the presence of anti-drug antibodies[11].
Neutropenia,thrombocytopenia,and anemia are also observed.Neutropenia may occur due to a blockade of TNFα (regulates proinflammatory factors involved in the differentiation and maturation of hematopoietic progenitor cells) that may mediate marrow failure due to inhibition of stem cell differentiation[12,13].Isolated thrombocytopenia after administration of anti-TNF therapy has been reported by Salaretal[14] in 2007 and Casanovaetal[15] in 2012,respectively; however,the cause/effect mechanism remains unclear.It may be related to autoimmune platelet destruction secondary to antiplatelet antibodies,immune complexes,or an idiosyncratic reaction.Anemia related to the use of anti-TNF remains debatable.Some studies have reported aplastic anemia due to administration of infliximab in rheumatoid arthritis[16] and infliximab-induced autoimmune hemolytic anemia[17].
Further,dermatological manifestations,such as eczema,psoriasis,infections,acne,dermatitis,and other erythema,are also reported.Psoriasis is a common adverse effect of anti-TNF therapy,occurring in approximately 1.5%-5% of the patients,mostly women,within an average of 2-6 mo after starting the therapy[18,19].Autoimmune disorders,such as lupus-like syndrome,vasculitis,antiphospholipid syndrome,sarcoidosis,interstitial lung disease,optic neuritis,inflammatory eye disease,central nervous system demyelination,and peripheral neuropathies,are also reported[20].Demyelination may occur,but it is unclear whether there is a causal relationship[21].As anti-TNFs are immunosuppressive agents,they can increase the risk of infections of bacterial,viral,or fungal origin.Uncommon infections,such as listeriosis,have also been linked to the administration of anti-TNF therapy,with a higher risk in the first year of therapy[22,23].Anti-TNFs can reactivate latent tuberculosis in immunocompromised individuals,emphasizing the importance of screening with clinical history,chest X-rays,and tuberculin tests before initiation of the therapy[24,25].A high risk of infection with varicella zoster virus is observed in patients with IBD,and those receiving anti-TNF have a high risk of herpes zoster[26].However,screening for a herpes virus infection is not required before the initiation of therapy[25].Hepatitis B virus reactivation can also occur during anti-TNF therapy or after its withdrawal[27].In the case of hepatitis C,biological agents do not present with a contraindication during concomitant infection and have a good safety profile; however,they are contraindicated in acute infections[28].In patients with human immunodeficiency virus (HIV) infection,the risk/benefit of administering anti-TNFs should be weighed due to the increased risk of opportunistic infections[29].Screening for hepatitis B and C viruses and HIV with serological tests is also recommended[25].The possibility of cytomegalovirus infection recurrence by reactivation of latent infection is low after the use of biological therapy in most cases[8].Screening before therapy is not required[25].Fungal infections related to anti-TNF use are also reported,particularly in those with risk factors,such as opioid use,leukopenia,advanced age,and more severe disease[30].The blocking of TNFα possibly alters the cytotoxic immune response to fungal infections[31].Warrisetal[32] reported a case of pulmonary aspergillosis in a patient with CD receiving infliximab.Histoplasmosis was also reported in a case series by Leeetal[33] after infliximab infusions in immunocompromised patients.
Malignancies (mainly non-melanoma skin cancer,melanoma,and lymphomas) are reported in patients with IBD due to chronic intestinal inflammation and the carcinogenic effects of immunosuppressive drugs[8,34,35].TNF can trigger apoptosis by activating caspases,and its inhibition can lead to growth and/or metastases and tumor recurrence[36].However,whether the use of anti-TNF monotherapy increases the overall risk of cancer in patients with IBD remains unclear[37].Studies conducted by Bianconeetal[38,39],Caspersenetal[40],and Fidderetal[41] failed to observe an increased risk of lymphoma,leukemia,or other hematologic malignancies with the use of anti-TNF monotherapy.Cardiovascular effects have also been reported,including HF,as discussed below.
HEART FAILURE
HF is a clinical syndrome secondary to the inability of the heart to pump sufficient blood to supply peripheral metabolic demands or to do so under increased filling pressures.Acute HF (AHF) has been increasingly described as a condition with unique pathophysiology,distinct from that of chronic heart failure,and is among the most common causes of hospitalization in the elderly[42].The patients can be categorized into new-onset (denovo) HF and worsening chronic HF.The latter accounts for the greater number of hospitalizations.Patients withdenovoHF may have no prior risk factors,such as in myocarditis,but more commonly have preexisting conditions that favor the development of HF,or present with structural heart diseases without overt symptoms.Those with chronic HF may have precipitating factors for decompensation,including infections,poor adherence to treatment,and medications for other comorbidities[42,43].Data on pathophysiology of AHF suggests that,apart from the architectural changes in the left ventricle due to increasing filling pressure and activation of the renin-angiotensin-aldosterone system,the inflammatory activation plays a pathogenic role in the progression of HF due to association with increasing stiffness of the vessels that leads to HF decompensation[42-48].Several conditions may be classified as risk factors for HF,including ischemic heart disease,hypertension,hyperlipidemia,diabetes,smoking,hypertensive heart disease,valvular heart disease,Chagas disease,congenital heart disease,and deposit diseases[49].
HF is diagnosed after thorough anamnesis,investigation of personal risk factors,family history,and current symptoms,such as dyspnea,edema of the lower extremities,orthopnea,paroxysmal night dyspnea,and palpitations[42].The general clinical examination may indicate an increase in the respiratory rate and a decrease in oxygenation levels,edema,cachexia,and signs of poor perfusion,such as altered mental status.A detailed examination may indicate an increased jugular pulse,reflecting the increased left ventricle filling pressure,auscultation of the S3 and S4,along with mitral regurgitation murmur due to dilation of the left ventricle.The signs of pulmonary congestion include crackling sound on inspiration and dullness of the lung bases on percussion due to pleural effusion.The abdominal examination may show hepatomegaly due to an increase in central venous pressure,along with ascites due to right HF[50-52].Patients should also be assessed using complementary tests,including renal function,levels of N-terminal-pro hormone B-type natriuretic peptide (NT-pro BNP),and electrolytes.The imaging examinations include electrocardiogram,chest radiography,and echocardiogram[53-56].The treatment for AHF depends on whether the patient presents with congestion,low output,or both.Four hemodynamical profiles have been postulated for better organization of the medications employed in the early management of AHF,as demonstrated below and summarized in Figure 1[57,58].
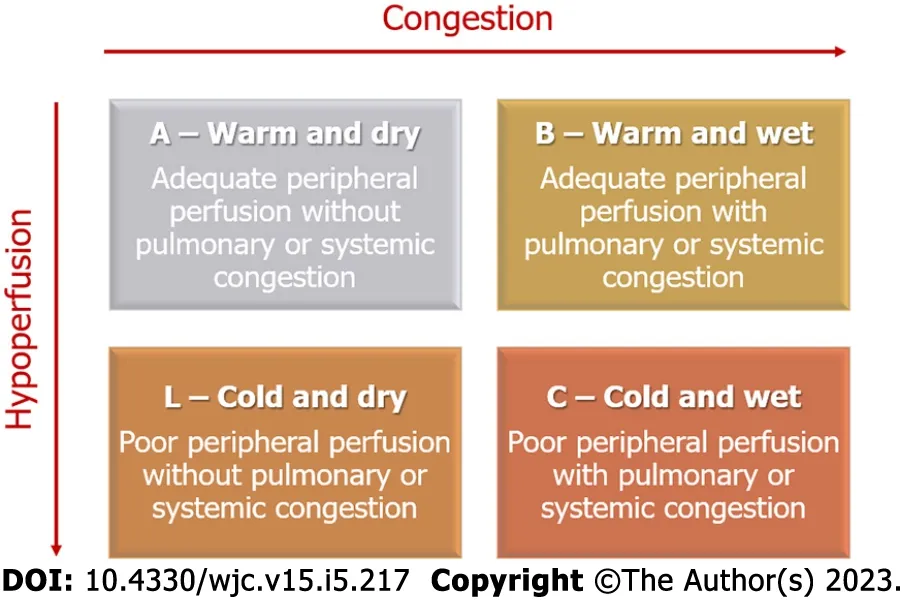
Figure 1 Clinical profiles of acute heart failure.
It is also important to assess patient’s prognosis on admission to determine the requirement of advanced HF therapy,such as implantable cardiac devices or heart transplant[59].Patients are considered to have worst prognosis if they are aged > 65 years; have a history of multiple hospitalizations; fail to adhere to treatment; present with functional classification NYHA III or IV; and have cachexia,syncope,sleep apnea,type II diabetes,or depression.Other factors include having had a reversed cardiac arrest; having pulmonary disease or cognitive dysfunction; having poor perfusion,congestion,tachycardia,persistent hypotension or low tolerance to exercise; having altered electrolyte levels,such as sodium < 130; having elevated BNP,troponin,or cytokines; having hemoglobin < 11 g/dL,creatine > 2.75 mg/dL,or urea 92 mg/dL; and showing atrial fibrillation in electrocardiogram,complete left bundle block,alternating T wave,long QT,low heart rate variability,progressive left ventricle dilatation,ejection fraction < 30%,right ventricle dysfunction,mitral or tricuspid regurgitation,restrictive pattern or decreased cardiac output,increase in pulmonary pressures,and peripheral vascular resistance[59].
HEART FAILURE AS AN ADVERSE EVENT OF ANTI-TNF USE
TNFα is found in both healthy and damaged hearts.Thus,it is challenging to understand its mechanisms of action.It binds to two different receptors: TNFα receptor-1 (TNFR1) and -2 (TNFR2) that are generally expressed on the heart cells[60,61].In HF,TNFα induces β-adrenergic receptor uncoupling,increases oxidation and formation of nitric oxide,increases levels of inflammatory cytokines,and downregulates levels of contractile proteins,thus contributing to myocardial dysfunction.Long-term TNFα signaling leads to alterations in the heart geometry due to hypertrophy,apoptosis,and fibrosis[62].The role of TNFα in HF pathophysiology is complex.Its effects are concentration-dependent and functionviatwo different pathways: Survivor activating factor enhancement (SAFE) pathway functioning under low TNFα concentrations,and death-promoting pathway functioning in high TNFα concentrations.The SAFE pathway involves stimulation of other cytokines,such as cardiotrophin-1,that act on glycoprotein 130 receptor,leading to eccentric hypertrophy due to sarcomere organization in series.This pathway is observed in athletes with left ventricle hypertrophy[63-65].In addition to the concentration of TNFα,its repercussion on the cardiac muscle depends on the receptor that it binds to as binding to TNFR1 may be cardio-damaging and binding to TNFR2 may be cardioprotective[60,66,67].The mechanisms of HF caused by the use of anti-TNF are summarized in Figure 2.
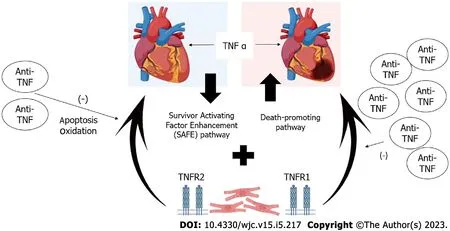
Figure 2 Mechanisms of heart failure caused by the use of anti-tumor necrosis factor agents.
Studies with animal models have suggested that TNFR1 Levels are upregulated after myocardial infarction without change in TNFR2 Levels.Other studies showed an absence of cardio-protection in acute ischemic models of TNFR1- and TNFR2-knockout rats,suggesting the involvement of both the receptors for maintaining a healthy heart[68,69].In another knockout model study,Hamidetal[70] explored the left ventricle remodeling after myocardial infarction; the study indicated that TNFR1 knockout improved the left ventricle ejection fraction,reduced left ventricle dilatation through cardiomyocyte hypertrophy and apoptosis,and also decreased fibrosis and inflammation.In contrast,knockout of TNFR2 reversed the effects,suggesting a strong protective role of TNFR2.However,knockout of both the receptors increased survival rates,reduced reactive oxygen species formation,and improved diastolic left ventricle pressure; thus,this indicated the ambivalence of role of TNFRs on the heart health[68-70].Further,Cacciapagliaetal[5] developed aninvitromodel for TNFα preconditioning,exposing the cardiac cells to a lower dose of TNFα.The results suggested that the cells developed more resistance to subsequent TNFα toxic dose exposure and conferred more protection against oxidation and apoptosis.
From animal models to human randomized control trials,the concept of cardiac detrimental effects of TNFRs inspired the studies ATTACH,RECOVER,and RENAISSANCE (the last two are combined as RENEWAL) that were designed to understand the effects of infliximab and etanercept on HF with optimized clinical treatment.The ATTACH study failed to observe improvement and,surprisingly,indicated worsening of HF after therapy discontinuation.The RENAISSANCE study also showed an increased hazard ratio for the worsening of HF in the treatment group than that in the control group[71].The disappointing clinical results,along with evidence from experimental models,suggest that the current rationale for the worsening of HF while administering anti-TNFα is that the dose employed in the randomized controlled trials abolishes the cardioprotective concentration of TNFα,therefore making the cardiomyocytes susceptible to apoptosis and oxidation[5].A consensus is lacking on whether TNFα functions as a parallel phenomenon to,and not the cause for,HF,along with a possible selective cytotoxicity of anti-TNFα on cardiomyocytes in HF[62].A study by Chungetal[72] evaluated the safety of infliximab in patients (n= 150) with moderate-to-severe HF (NYHA III or IV).The patients randomly received placebo,infliximab 5 mg/kg,and infliximab 10 mg/kg at 0,2 and 6 wk and were followed for 28 wk.There was no improvement in the clinical status of patients who received infliximab at 14 wk,and after 28 wk,there were more hospitalizations in the infliximab 10 mg/kg group (n= 20) due to worsening of the HF condition,along with adverse clinical events persisting for up to 5 mo after discontinuation of therapy.Abedinetal[73] reported a case of acute coronary syndrome after infliximab infusion in a patient without previous heart disease.The patient was a 49-year-old Hispanic woman with rheumatoid arthritis and previously well-controlled hypertension.She presented to the emergency department 10 min after the start of infliximab infusion (20 mg had been infused).The patient had no other risk factors and no family history of coronary artery disease.
Kwonetal[74] followed patients with rheumatoid arthritis,psoriatic arthritis,and CD who were treated with an anti-TNF agent (etanercept or infliximab).A total of 47 patients developed HF; of these,81% had no previous symptoms and 19% had worsening of preexisting symptoms.Among those who developed HF,50% had no risk factors.The median interval between the first infusion of anti-TNF and diagnosis of HF was 3.5 mo (24 h to 24 mo).Keatingetal[75] reported a case of anti-TNF-induced AHF.The 32-year-old patient had hypothyroidism and a bicuspid aortic valve and presented with Turner syndrome and CD.Biological therapy with adalimumab was initiated due to no response to budesonide.Examination indicated a transthoracic echocardiogram with normal ejection classification (> 55%).Eighteen weeks after administering adalimumab,the patient was admitted to the emergency department with edema and dyspnea.Further,we reported a case of AHF 6 mo after administering infliximab in a 50-year-old woman with CD and diabetes and a previous history of arterial hypertension.The patient presented with cardiac symptoms after optimization of the infliximab dose (10 mg/kg)[76].The standard treatment is administered after diagnosis of HF due to anti-TNFα therapy.The current guidelines show evidence of the best prognosis for therapy for HF with low ejection fraction,while specific treatment for preserved ejection HF is unavailable.Treatment for low ejection fraction HF includes angiotensin-converting enzyme inhibitors,angiotensin receptor blockers,angiotensin receptor neprilysin inhibitor,beta-blockers,aldosterone inhibitor,and,more recently,sodium-glucose cotransporter-2 inhibitors.Symptomatic medication includes diuretics,vasodilators,and digoxin.AHF may require intravenous administration of inotropes and vasopressors[77].Studies have suggested that the use of anti-TNFs should be discontinued,and a new class of medication should be selected for treatment of the primary disease; these studies also highlighted a lack of specific guidelines for the management of cardiovascular disease in patients with IBD[8,78,79].Some therapeutic options for the treatment of IBD in case of adverse reactions to anti-TNFs include Janus kinase (JAK) inhibitors (tofacitinib),anti-IL-12/23 antibody (ustekinumab),and anti-integrin antibody (vedolizumab).
Tofacitinib can be used in patients with moderate-to-severe UC who are intolerant or refractory to treatment with anti-TNFs.Despite its ease of rapid onset of action,oral administration,and low immunogenicity,it is also having risks such as venous thromboembolism and hyperlipidemia[80].However,long-term data on adverse cardiovascular events with tofacitinib are lacking in patients with IBD,and it remains unclear whether the risk of venous thromboembolism is disease- or drug-related [79].Ustekinumab,a monoclonal antibody,is an option in patients with CD and with moderate-tosevere UC intolerant or refractory to anti-TNFs.In IBD,the relationship of cardiovascular events in these patients is unclear[81,82].Vedolizumab,a humanized monoclonal antibody,is also an option in patients with CD and with moderate-to-severe UC refractory or intolerant to anti-TNFs,with better outcomes in patients not treated with anti-TNFs[83,84].Randomized and observational studies have not reported an increase in cardiovascular events in patients with IBD[85-88]; however,an increase in cerebrovascular events,such as stroke and cerebral hemorrhage,is reported[79].The selection of the most appropriate medication in this scenario is challenging.The clinicians should carefully analyze the different medication classes available,with their safety and efficacy profiles,to define a personalized treatment strategy for each patient,considering risk factors inherent to the patient and the proposed medication,while aiming for the best outcome.
CONCLUSION
The recommendations for HF screening prior to IBD treatment with anti-TNFα drugs are lacking.Some guidelines suggest screening,while others only mention avoidance of biological drugs when a patient presents with class III/IV HF.The European Crohn's and Colitis Organization (ECCO) reports that patients with IBD have a modest increase in the risk of ischemic heart disease,especially in women; however,they have not mentioned requirement of screening tests for cardiovascular diseases before administration of biological therapy[1,4,7,89,90].The guidelines of the American College of Gastroenterology and the Brazilian Consensus on Inflammatory Bowel Diseases have also not provided recommendations for screening these patients[6,91,92].The guidelines of the British Society of Gastroenterology recommend that the use of anti-TNFs be contraindicated in cases of congestive HF and that screening be performed before starting treatment; however,they have no suggestions on the best strategies for screening[93].Considering the indication of anti-TNFα drugs for other immune mediated diseases,although with a very low certainty,guidelines on rheumatoid arthritis recommend the following strategies: Inclusion of a non-TNF inhibitor in place of a TNF inhibitor for patients with NYHA class III or IV HF and also switching to a non-TNF inhibitor instead of a TNF inhibitor for patients who develop HF[94].The stratification of patients with HF should not be challenging as a simple clinical examination is sufficient to identify patients with NYHA classes III and IV disease.However,issues arise when the patients present with severe HF and are oligosymptomatic,especially if they are not accustomed to exerting themselves on a regular basis.As patients may develop HF after pregnancy,viral infections,or alcohol abuse,yet not present with any symptoms consistent with NYHA III or IV,this makes them susceptible to underdiagnosis.Taken together,in the absence of evidence supporting heart disease screening prior to initiating anti-TNFα drugs,and considering the current availability of a low-cost,radiation-free test that can easily assess the patient’s heart function,such as echocardiogram,we recommend that an initial cardiac evaluation be a part of the patients’ routine care.We suggest increasing employment of an echocardiogram for diagnosing HF prior to initiating treatment.This strategy may prevent the incidence of adverse events in patients receiving this treatment.We hope that this review highlights this topic and would encourage future studies to clarify the benefits of using HF screening tools in patients with IBD prior to the use of anti-TNF medications to control inflammatory processes and restore quality of life,without causing further damage to the patients.It is reinforced that anti-TNF therapy has changed the course of treatment for IBD and other immune-mediated diseases in recent decades,altering its progressive and disabling course.Due to the more frequent use of these therapies,concerns about safety arise,and this article reinforces the importance of studying the subject in greater depth,including investigating the role of cardiac receptors and their relationship with the appearance of adverse events in these patients.Another point worth mentioning is the need for new algorithms and protocols,especially for populations at risk,in order to avoid the unwanted effects of the prescribed therapy.
FOOTNOTES
Author contributions:Grillo TG,Silveira CFDSMP,Quaglio AEV,Dutra RM,Baima JP,and Bazan SGZ undertook the majority of the writing; Sassaki LY designed the outline and coordinated the writing of the paper; all authors revised the manuscript for important intellectual content and approved the final version.
Conflict-of-interest statement:The authors have no conflicts of interest to declare.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Brazil
ORCID number:Thais Gagno Grillo 0000-0002-4351-5034; Caroline Ferreira da Silva Mazeto Pupo Silveira 0000-0001-7132-2654; Ana Elisa Valencise Quaglio 0000-0002-5998-2382; Renata de Medeiros Dutra 0000-0002-0060-6155; Julio Pinheiro Baima 0000-0002-4035-3113; Silmeia Garcia Zanati Bazan 0000-0002-0607-8189; Ligia Yukie Sassaki 0000-0002-7319-8906.
S-Editor:Xing YX
L-Editor:Wang TQ
P-Editor:Yu HG
 World Journal of Cardiology2023年5期
World Journal of Cardiology2023年5期
- World Journal of Cardiology的其它文章
- Atrial fibrillation and coronary artery disease: An integrative review focusing on therapeutic implications of this relationship
- Current knowledge and contemporary management of non-A non-B aortic dissections
- Importance of concomitant functional mitral regurgitation on survival in severe aortic stenosis patients undergoing aortic valve replacement
- Impact of erythropoietin therapy on cardiorenal syndrome: A systematic review with meta-analysis
- Extracorporeal veno-venous ultrafiltration in congestive heart failure: What’s the state of the art? A mini-review
- Pharmacoepidemiologic study of association between apparent treatment resistant hypertension,cardiovascular disease and interaction effect by sex and age