
Improving myopia awareness via school-based myopia prevention health education among Chinese students
2023-05-15 09:20:36LuoMingHuangXianMingFanYuHongXieZhiYongMengTingChenBingFaDaiYangYuZhenZengChunYaZhouJiaJiaLinYinHeChenQianWangJianMinHu
Luo-Ming Huang, Xian-Ming Fan, Yu-Hong Xie, Zhi-Yong Meng, Ting Chen,Bing-Fa Dai, Yang Yu, Zhen Zeng, Chun-Ya Zhou, Jia-Jia Lin, Yin-He Chen,Qian Wang, Jian-Min Hu
1Department of Ophthalmology and Optometry, the School of Medical Technology and Engineering, Fujian Medical University, Fuzhou 350000, Fujian Province, China
2Department of Ophthalmology, the Second Affiliated Hospital of Fujian Medical University, Quanzhou 362000, Fujian Province, China
3Shenzhen Eye Hospital, Jinan University, Shenzhen Eye Institute, Shenzhen 518040, Guangdong Province, China
4The Research Center for Juvenile Myopia Prevention and Control of Fujian Province, Fuzhou 350000, Fujian Province,China
5Engineering Research Center of Assistive Technology forⅤisual Ⅰmpairment, Fujian Province University, Quanzhou 362000, Fujian Province, China
6Eye Institute and Affiliated Xiamen Eye Center of Xiamen University, Xiamen 361000, Fujian Province, China
7Department of Ophthalmology, Quan Zhou Women’s and Children’s Hospital, Quanzhou 362000, Fujian Province,China
Abstract
INTRODUCTION
Myopia is a global public health problem affecting both children and adolescents.Ⅰt is expected to affect more people in several decades[1-2], especially the complications caused by high myopia lead to visual impairment and even blindness[3].Although the pathogenesis of myopia is not completely clear, a large number of studies have shown that environmental factors such as long-term near work, poor eye-use habits, longer screen time, sleep disorders, and lack of outdoor activities are essential factors in the onset and development[4-7].Changes in the environment and lifestyle have led to an increased myopic prevalence and shifts in children[8-9].Compared with the period before the corona virus disease 2019(COⅤⅠD‐19) pandemic, children’s outdoor time decreased by 68.0%, and screen time for online courses increased 2.8-fold[10],leading to increased myopia rates[8].
Poor awareness of ocular diseases and their complications causes delays in seeking medical care and opportunities for early intervention and prevention.For example, due to poor awareness and understanding of glaucoma and its symptoms, it is easy to ignore its early symptoms and fail to seek treatment at the best time for glaucoma patients.One-third of patients develop blindness before seeking a doctor or receiving medical care[11].Similarly, owing to the lack of an early understanding of diabetic retinopathy, many patients develop visual impairment and even blindness[12].The level of awareness of common eye diseases has been reported worldwide.There is a deficiency in the assessment of myopia awareness, especially among children and adolescents with a high incidence of myopia.Improving public awareness of common eye diseases is vital to early diagnosis and control, reducing the burden of visual impairment[12].One effective way is to improve environmental factors and lifestyle for myopia prevention[13],for example, Singapore has implemented public education measures to effectively reduce the myopia rate in children[14].Few studies have evaluated myopia awareness, and few reports have described the level of understanding of myopia in students in China.This study investigated baseline rates of myopia knowledge, attitudes, and skills.A survey was also conducted to evaluate students’knowledge absorption and the effectiveness of myopia prevention health education.To provide a reference for the government to formulate policies for school-based myopia prevention and health education.
SUBJECTS AND METHODS
Ethical ApprovalThis study was approved by the Human Ethics Committee of Fujian Medical University (No.2021144)and followed the principles of the Declaration of Helsinki.Permission was obtained from the parents and teachers at the schools after the purpose of the study was explained.
Study PopulationConvenience sampling was used to select students from 2 middle schools in Fuzhou City to participate in myopia prevention health education, and questionnaires were administered uniformly by class and pre- and post-health education.The investigators were trained uniformly with a self-written manual to ensure the quality of the questionnaire.Before completing the questionnaire, the investigators thoroughly explained the purpose and methods of the study and the details of how to complete the questionnaire.The questionnaire was filled anonymously, and it was explained to the students that it had nothing to do with exam scores to minimize false declaration of the questionnaire.If any questions were asked, an investigator was consulted.
AssessmentMembers of the Research Center for Juvenile Myopia Prevention and Control of Fujian Province conducted health education lectures using the 2020 version of Myopia Prevention and Control for Children and Adolescents issued by the Chinese Ministry of Education[15].The health education courseware included basic knowledge of eyes, myopia onset and development, myopia health risks and complications,myopia prevention and control, a healthy diet, and nutrition.The questionnaire was designed based on the courseware content and relevant literature[16-17], including general information such as sex, age, myopia knowledge, myopia prevention behaviors, and attitudes toward myopia prevention.Statistical AnalysisAccording to previous studies, the awareness rate of myopia knowledge among students is approximately 70%[18].This study hypothesized that it could be increased by 10% post-health education.A twosidedαof 0.05 and a power level of 95% were assumed.The assumption of an intervention loss to follow-up of 15%and a baseline participation rate of 80% led to baseline and post-sample sizes of 580 and 650, respectively.The integrity and effectiveness of the questionnaires were checked, and incomplete questionnaires were eliminated.For unqualified standardization, if the data integrity of the questionnaire was less than 80%, the questionnaire was considered invalid and destroyed.Statistical software SPSS 26.0 (SPSS Inc., version 26, Chicago, IL, USA) was used for analyses.Categorical variables were summarized using descriptive frequencies and percentages and analyzed using the Chi-squared test.Statistical significance was set atP<0.05.
RESULTS
The mean age of the participants was 13.6±0.7y.Totally 957 valid questionnaires were collected pre-health education,with an effective rate of 95.7% and 850 valid questionnaires were collected post‐health education, with an effective rate of 85.0%.
As shown in Table 1, the awareness rates about myopia knowledge questions, such as “do you know the symptoms of myopia?”, “do you think myopia is a high-risk ocular disease?”, “do you think myopia can be prevented?”, and “do you think increasing levels of myopia are associated with age?”were 87.5%, 72.9%, 91.3%, and 86.7% at baseline,respectively.After health education, the awareness rates of these questions significantly increased to 95.2% (χ2=33.10),89.0% (χ2=74.37), 96.5% (χ2=20.31), and 94.1% (χ2=27.96)respectively (allP<0.001).Regarding whether they thought that myopia could be cured, 51.5% of the participants believed that it could be cured, and this belief significantly decreased to 38.3% after health education (χ2=31.77,P<0.001).At baseline,awareness rates of myopia prevention and control questions,such as “do you think it is necessary to perform periodic eyeexaminations?”, “do you know the‘one fist, one foot, one‐inch’rule?”(one foot: maintaining a distance of > 30 cm between the eyes and book while reading and writing; one inch: keeping a distance of 3 cm between the finger and a pen while writing;one fist: maintaining a distance of 7 cm between the body and table when reading and writing), “do you know that outdoor activities can prevent myopia onset and development?”, and“do you know that taking breaks for 10min after 30-40min continuously near work is important?”were 92.8%, 84.8%,85.6%, and 59.2%, respectively.Post-health education, the awareness rates of these questions significantly increased to 97.6% (χ2=22.67), 96.2% (χ2=66.28), 96.5% (χ2=63.45),and 73.00% (χ2=37.99) respectively (allP<0.001).Posthealth education: “do you think conducting health education on myopia prevention and control in schools is necessary?”significantly increased from 91.6% to 98.1% (χ2=37.80,P<0.001).

Table 1 Comparison of the awareness rate of myopia pre- and post-health education n (%)
Figure 1 shows the percentage of ways to obtain knowledge on myopia prevention and control.Those that accounted for more than 70.0% were television and the internet (80.8%), doctors(79.7%), school health education (78.9%), teachers (76.4%),and parents (73.1%).The lowest selection rate was “other”,accounting for 43.7%.
Figure 2 shows that 94.9% of students were willing to spread myopia prevention and control knowledge to others, and 93.8% were determined to correct their unhealthy eye-use behavior in post-health education.
DISCUSSION
We investigated the rate of myopia awareness, knowledge,attitudes, and skills in school-based health education among Chinese middle school students.
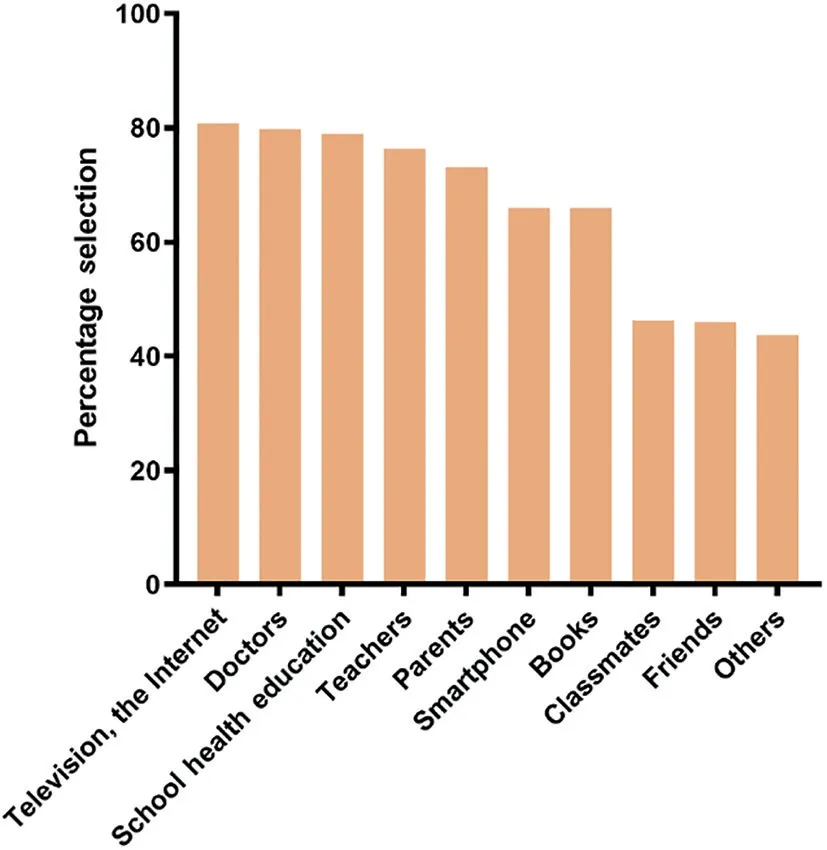
Figure 1 The percentage of selection in ways to obtain knowledge of myopia.
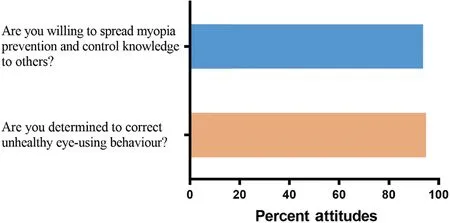
Figure 2 Attitudes of participants towards health education in posthealth education.
This study found that Chinese middle school students have a good level of myopia knowledge, prevention, and control,with awareness rates exceeding 70%.This result was similar to the high level of myopia awareness rate shown in primary school students in Wenzhou[18-19].This may be related to the Chinese government’s focus on myopia prevention and control among children and adolescents, which has promoted a series of health education[20].Although, the awareness rate for all the questions increased significantly after health education,the percentage of students who still did not think it necessary to take breaks after 30-40min of continuous near work was 27.0%.Taking breaks after near work is a vital eye care practice that has been shown to be effective against myopia in both cross-sectional and longitudinal studies[21-22].To explain in detail the mechanism and the importance of “taking breaks after continuous near work”is necessary for health education and to encourage students to perform outdoor activities during recess to reduce myopia[23].Besides, the incorrect opinion that“myopia can be cured”was held by 38.3% of participants.The explanation might be that students interpret low-dose atropine[24]and orthokeratology[25], and refractive surgery as curable treatments for myopia.Health education has corrected students’incorrect views to some extent.There is still a need to optimize the content and format, such as the side effects and complications of various interventions, to improve awareness of myopia control techniques.Thus, maintaining good eyeuse habits and behavior should be taught, and health education should also focus on myopia control techniques.
The top-ranked methods for students to obtain knowledge about myopia prevention and control were television and the internet, indicating the effectiveness of these health education methods.Health education on myopia prevention should be combined with social media, which has proven to be a practical way to educate and raise awareness[26].The secondranking method was from doctors, which aligns with the fact that 92.8% of students have periodic eye examinations.They may have received professional guidance and education from doctors while performing these examinations.The participation of doctors in myopia prevention health education can ensure the authority of content, and doctors should actively participate in health education.More than 70% of students chose school health education, teachers, and parents as methods to obtain knowledge, indicating that school and family play a vital role in myopia prevention health education.Schools and families providing myopia prevention and control education are crucial.Previous studies have shown that the lack of myopia knowledge, risk factors, and control techniques among eye care practitioners, parents, teachers, and students is detrimental to myopia prevention and control[27-28].If teachers and parents lack knowledge about myopia, they cannot educate and supervise children with poor eye-use behaviors.Parents influence children’s lifestyle choices, and they must hold positive attitudes toward managing myopia prevention and control to reduce myopia[29-30].A randomized clinical trial showed that improving parental myopia awareness could reduce the 2-year cumulative incidence of myopia[31].Changes in children’s lifestyle behaviors and the choice of prevention and control methods depend on parents’awareness of the disease and their acceptance of the available interventions as necessary treatments.Among other existing public health domains, parents have been evidenced to play a critical role in understanding new treatments for diseases and their curative effects.Health education should not only be geared toward students but also raise awareness and participation of teachers and parents in myopia prevention and control, and they should assume the responsibility and supervisory role in protecting children’s vision in schools and families[17,32].Family education is the beginning of children’s health education.Improving parental awareness of myopia is the foundation for cultivating healthy behaviors in children.It is also necessary to ensure that myopic interventions are effectively implemented.The popularization of health education and participation of the entire society (government, doctors, schools, children, and parents) can promote the sustainable development of myopia prevention and control management measures[9,29].
High-quality education on myopia prevention can promote students’self-health management.Regarding pre-health education, 91.6% of the students thought myopia prevention health education in schools was necessary.This shows that students lack ways to obtain myopia knowledge, but they realize the importance of eye care and are eager to change their daily behaviors.This may be due to concerns that changes in lifestyle and conduct may lead to a potential myopia boom during the COⅤⅠD‐19 pandemic[27,33]without knowing the methods of eye care.Post-health education, students were determined to change their poor eye-use habits and were willing to spread myopia knowledge in health education to others.This indicates that they were inclined towards health education and benefited from it.Improving myopia knowledge and modifying its risk factors can prevent myopia epidemics[13].The health belief model, that is, knowing health information, recognizing health beliefs, changing health information, and adopting healthy behavior, can measure the effectiveness of health education[34].Health education aims to raise disease awareness, improve health beliefs, and promote healthy behavior[35].Therefore, enhancing health education and increasing awareness among students and parents are key strategies to prevent myopia.
The strength of our study is that it provides the latest data on student awareness of myopia, filling a gap for which no data are currently available in China.This study also assessed the effectiveness of increasing students’awareness of myopia through health education.Baseline knowledge and evaluation results can provide the government with information on improving health education content based on student preferences and needs.Courseware content is authoritative and representative and can be generalized to a certain extent in China.This study had some limitations.First, only the basic concepts of myopia prevention and control were taught and evaluated because of the brevity of this study and its shortterm follow-up period.To further increase student mastery,it is essential to implement longitudinal health education and evaluate retention over time.The absorption of health education in myopia prevention does not reflect students’applications in daily life.Second, because the refraction of the students was not measured in this study, the effect of health education on this parameter could not be evaluated.Third, the questionnaire failed to quantify the knowledge students gained from health education.
In conclusion, Chinese middle school students had a good understanding of myopia.Implementing school-based myopia prevention education improved the baseline knowledge,attitudes, and skills regarding myopia.To raise student awareness of eye care, the government, society, schools, and families must participate in myopia prevention and health education.Health education should be widely disseminated in schools, emphasizing myopia prevention and control techniques to improve dissemination efficiency.
ACKNOWLEDGEMENTS
Authors’contributions:Huang LM and Hu JM designed the study.Huang LM, Fan XM and Xie YH drafted the initial manuscript.Yu Y, Zeng Z, Zhou CY, Lin JJ, Chen YH, and Wang Q collected the data.Huang LM, Meng ZY, Xie YH,Lin JJ, and Zhou CY analyzed the data.Huang LM, Meng ZY,Xie YH, Chen T, Dai BF, and Hu JM reviewed and edited the manuscript.Hu JM, Fan XM, Dai BF, and Huang LM obtained funding.Hu JM acts as a guarantor of the study.All authors reviewed and approved the final version of the manuscript.
Foundations:Supported by National Key R&D Programmes of China (No.2018YFC2002602); Special Task of the Ministry of Education of the People’s Republic of China(No.087280); Sanming Project of Medicine in Shenzhen (No.SZSM201812090); Startup Fund for Scientific Research,Fujian Medical University (No.2020QH1109); Fujian Medical University High‐level Talents Scientific Research Launch Fund(No.XRCZX2021011).
Conflicts of Interest: Huang LM,None;Fan XM,None;Xie YH,None;Meng ZY,None;Chen T,None;Dai BF,None;Yu Y,None;Zeng Z,None;Zhou CY,None;Lin JJ,None;Chen YH,None;Wang Q,None;Hu JM,None.
 International Journal of Ophthalmology2023年5期
International Journal of Ophthalmology2023年5期
- International Journal of Ophthalmology的其它文章
- Comment on “Factors affecting single-step transepithelial photorefractive keratectomy outcome in the treatment of mild, moderate, and high myopia: a cohort study”
- Visual function and biofeedback training of patients with central vision loss: a review
- A case of Posner-Schlossman syndrome treated by gonioscopy-assisted transluminal trabeculotomy
- Mitochondrial dysfunction in glaucomatous degeneration
- Publication trends of primary angle-closure disease during 1991-2022: a bibliometric analysis
- Ocular manifestations of children with atopic dermatitis in Saudi Arabia