
Application of femtosecond laser in assisted cataract after lCL implantation with different vault
2023-03-04 10:00YanLiCongYiWangLiAnWuBoMaGuanXingDang
Yan Li, Cong-Yi Wang, Li-An Wu, Bo Ma, Guan-Xing Dang
Shaanxi Eye Hospital, Xi’an People’s Hospital (Xi’an Fourth
Hospital), Affiliated Guangren Hospital, School of Medicine,
Xi’an Jiaotong University, Xi’an 710004, Shaanxi Province,China
Dear Editor,
We are writing this letter to report two unusual cases of femtosecond laser-assisted cataract surgery (FLACS)in two ICL-implanted patients with significant different vault.FLACS has been confirmed by accumulating evidence to improve the safety and precision of surgery from common cases to complicated cases in treating cataracts[1-3]. Implantable collamer lens (ICL) implantation possesses a good performance in its predictability, reversibility, and the rapid visual recovery.It has become a new tendency in the correction of ametropia,but complicated cataract is the most common complication after ICL implantation[4-5]. We report two cases of FLACS with the ICL implantation, and the vaults of two cases are greatly different, one is 287 μm and the other is 975 μm. Furthermore,the differences of FLACS were compared.
Case PresentationCase 1, a 54-year-old female with progressive blurred vision in her left eye for 2y, who underwent ICL (ICL V4, STAAR Surgical Company, CA, USA) implantation in her left eye 11 years ago, and carried out the cataract extraction combined with single focus intraocular lens (IOL)implantation in her right eye by reason of traumatic cataract in the same year. Her uncorrected distance visual acuity (UDVA)of the right eye was 20/30 (Snellen visual acuity chart), and her corrected distance visual acuity (CDVA) was reached at 20/20 with -0.75 diopter phere (DS). For the left eye, her UDVA was 20/200 and her CDVA with -3.75 DS was 20/30.The corneal endothelial cell count of the left eye was 2384.5/mm2.Under the slit-lamp biomicroscope, there was no central hole of ICL in the left eye, and the laser peripheral incision of the iris at 11 o’clock was unobstructed. In addition, the ICL was not in contact with the anterior capsule of lens, and the nuclear cataract was found (Figure 1A). The vault was 287 μm by anterior segment optical coherence tomography (AS-OCT;Japan TOMEY; Figure 1B).
Since the patient’s right eye was implanted with a monofocal IOL, and the diopter was -0.75 DS and UDVA was 20/30,the monovision design was implanted in the left eye with a monofocal IOL. After the patient signed the informed consent,the left eye underwent FLACS combined with ICL extraction.The femtosecond laser machine was a GAUSH LENSAR 3D laser machine, and the diameter of capsulotomy was 5.3 millimeter (mm), and the chop nuclear pretreatment was designed as 6 pieces. When scanning the anterior capsule of lens, the posterior surface of the ICL was mistaken for the anterior capsule, and the manual adjustment of the anterior capsule was performed by surgeon. Besides, the capsulotomy appearance was good, and many small cavitation bubbles gathered between the ICL and the lens, hindering the nuclear pre-fragmentation. During the phacoemulsification step, a large number of small cavitation bubbles were observed below the ICL (Figure 2A). A conventional 3.0 mm corneal incision at 135 degrees for phacoemulsification was used, and the ICL was taken out by alternating hands perpendicular to the long axis of the ICL directly. The posterior surface of the ICL was examined for circular laser damage marks (Figure 2B).The anterior capsular flap was successfully removed along the trajectory of the laser anterior capsulotomy. The anterior capsule flap of the lens was completely free, but the nuclear pre-fragmentation was unsuccessful (Figure 2C). Conventional phacoemulsification and IOL implantation were successfully completed, the anterior capsule orifice was perfect (Figure 2D). The patient’s UDVA 1wk after surgery was 20/20.
Case 2, a 51-year-old female with progressive blurring of vision in her right eye for 1y, then undergone ICL (ICL V4,STAAR Surgical Company, CA, USA) implantation in both eyes due to high myopia 11 years ago. Her UDVA was 20/66 in the right eye and 20/30 of the left eye. The corneal endothelial cell count was 2183.9/mm2in the right eye and 2432.1/mm2in the left eye. With the slit-lamp examination, there was no central hole in the ICL of both eyes under slit-lamp, the distance from the posterior surface of the ICL to the anterior surface of the lens was about 2.0 corneal thickness (CT), and the peripheral anterior chamber was about 1/2 CT. The iris laser peripheral incision was unobstructed, and the anterior capsule of the lens’s optical axis area was opaque. The vault of the right eye was 975 μm by optical coherence tomography(Japan TOMEY), the depth of the anterior chamber was 2187 μm (Figure 3A), the vault of the left eye was 641 μm by optical coherence tomography (Japan TOMEY), and the depth of the anterior chamber was 2285 μm (Figure 3B).
Considering the willing of this patient prefer to drive, use computer and read books, and hoped to take off the glasses after surgery. After the preoperative communication, she was recommended to implant a trifocal intraocular lens (Alcon PanOptix TFNT00 intraocular lens). When measuring the biological parameters with IOL-Master 700 before surgery, it was found that the posterior surface of the ICL was mistakenly identified as the anterior surface of the lens (Figure 4A, 4B).Therefore, the measured anterior chamber depth became smaller, and it was 2.87 mm including the corneal thickness,but the actual anterior chamber depth was 3.91 mm. However,the lens thickness (LT) was increased to 4.55 mm, but the actual LT was 3.50 mm. Meanwhile, the calculation of the IOL refractive power was consistent for both measurements, and both calculations of the IOL refractive power using Barrett Universal II formula[6]were 2 diopter (D) when the target refractive power was close to emmetropia.
After the patient signed the informed consent, the right eye underwent FLACS combined with trifocal IOL implantation,and ICL was removed. The femtosecond laser machine was also the GAUSH LENSAR 3D laser machine. The diameter of capsulotomy was 5.3 mm and the nuclear pre-fragmentation was designed as 6 pieces. When the laser machine scanned,the distance between the posterior surface of the ICL and the anterior capsule was high, and the anterior capsule was scanned accurately without manual adjustment (Figure 5A). But the posterior capsule couldn’t be scanned accurately, and the preset distance of nuclear pre-fragmentation was 200 μm from the posterior capsule. The capsulotomy appearance was successful and small cavitation bubbles gathered in the surrounding area between the posterior ICL and the lens (Figure 5B), meanwhile the nuclear pre-fragmentation was performed normally. During the process of phacoemulsification, there was no accumulation of cavitation bubbles below the ICL (Figure 5C). The ICL was successfully removed by the same operation method as the same incision in case 1 (Figure 5D). After examination of the ICL lens, there was no laser damage on the posterior surface.The nuclear pre-fragmentation was done but the depth was shallow (Figure 5C). The nucleus material was removed using phacoemulsification and the trifocal IOL was successfully implanted into the capsular bag. One week after the operation,the patient’s UDVA was 20/20.
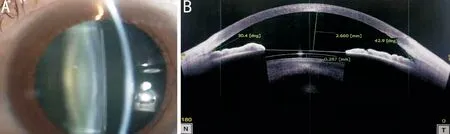
Figure 1 Anterior segment optical coherence tomography image and slit-lamp photographs of the left eye.
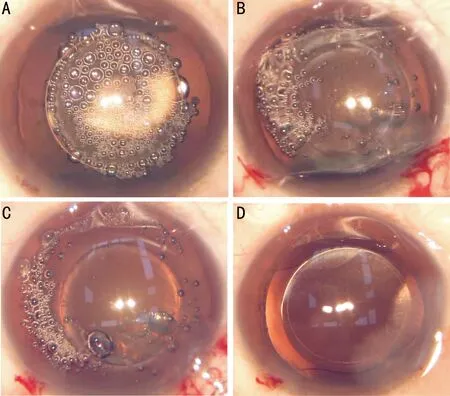
Figure 2 Process of capsulotomy by femtosecond laser and phacoemulsification in the left eye.

Figure 3 Anterior segment optical coherence tomography image of both eyes.
DISCUSSION
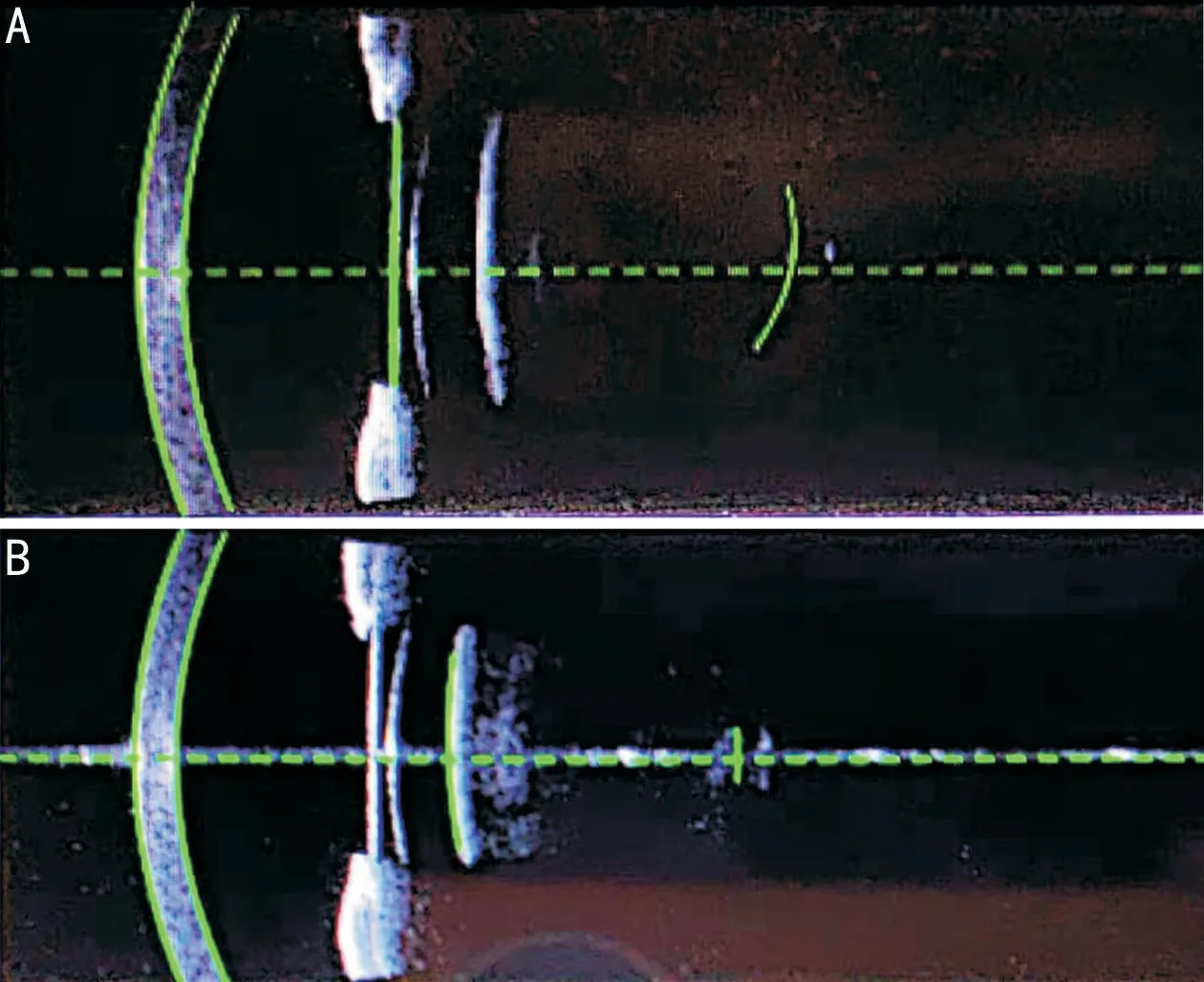
Figure 4 Measured biological parameters with IOL-Master 700.

Figure 5 Accurate scanning of lens anterior capsule with femtosecond laser A: Rear surface of implantable collamer lens(ICL) was visible; B: No cavitation bubbles in the central area between the ICL and the lens; C: The capsulotomy and the nuclear pre-fragmentation were complete; D: The ICL was extracted by alternating hands in the direction perpendicular to the long axis of ICL with supratemporal phacoemulsification incision.
Complicated cataract is the most common complication after ICL surgery, characterized by the major anterior subcapsular opacity[7-8], which is related to the design methods of ICL,vault and other patient’s related factors. In case 1, it was the nuclear cataract, and the vault was 287 μm. In case 2,the vault was 975 μm, which exceeded the ideal vault range of 250-750 μm reported by literatures[9]. The occurrence of anterior subcapsular cataract suggested that vault was not the only factor for the complicated cataract. ICL of both cases was V4 type without central hole, which may be related to complicated cataract. In recent years, with the improvement of ICL design and increased experience of surgeon, the incidence of postoperative complications of cataract was decreased, with the incidence of 7%-13% in 5y[10-11]and 28%-58.4% in 10y[12-13].In both cases, the patient underwent ICL surgery 11 years ago had both developed cataracts almost 10y after surgery.
Ten years after ICL implantation, phacoemulsification and IOL implantation was often required in 17%-18.7%[12-13]of patients. The introduction of the femtosecond laser system has extended the develop of cataract extraction surgery, especially in the capsulotomy and the nuclear pre-fragmentation[14].The femtosecond laser platform uses image and software technology to scan and 3D to reconstruct the cornea and lens.After collecting images, the capsulotomy and the nuclear pre-fragmentation can be completed. The cavitation bubbles generated during the femtosecond laser process need to be diffused[15]. The existence of ICL and the change of ICL high refractive index may lead to the impact of FLACS on scan imaging and laser transmission, blocking the diffusion of cavitation bubbles in the anterior chamber space. It induced the generated cavitation bubbles to accumulate in the below,interfering the laser delivery and resulting in an incomplete treatment step. Indian scholars Nathet al[16]and Chinese scholars Yuet al[17]reported that in patients with low vault and “0” vault, the capsulotomy may be incomplete and the cavitation bubbles was not performed. In our reported cases,the difference of vault was significant, and there were different appearances about the laser scanning of the anterior capsule,the capsulotomy, and the nuclear pre-fragmentation. In case 1, the vault was 287 μm and it was low. When scanning the anterior capsule, it was wrongly focused on the posterior surface of the ICL. Therefore, it must be identified carefully,and the anterior capsule surface needs to be manually corrected. During the capsulotomy, a large number of dense cavitation bubbles gathered between the entire posterior surface of the ICL and the lens and they couldn’t be diffused,which blocked the laser delivery and interfered the nuclear prefragmentation step[18]. In case 2, the vault was 975 μm and it was a little high. The laser scanning was accurately positioned on the anterior lens capsule, and the pre-fragmentation process was successfully completed. However, in the process of phacoemulsification, it was found that the nuclear prefragmentation was weakened. The subcapsular opacity area of lens weakened the laser delivery, which may be one of the reasons for the weakening of the effect of lens nuclear prefragmentation[17]. In some reports, Diakoniset al[19], suggested that the setting parameters of capsulotomy can be optimized to successfully complete the surgical steps.
Most cataract patients with ICL implantation hope to implant multifocal IOLs to take off glasses, and the accuracy of biological parameter measurement is particularly important.During the measurement with IOL-Master 700, the anterior surface of the ICL will be mistakenly identified as the anterior surface of the lens, resulting in an underestimation of the anterior chamber depth and an overestimation of the LT. This may be related to the light reflection on the ICL surface. But the errors in the measurement of anterior chamber depth and LT did not impact on IOL prediction accuracy. This is also proved by the excellent UDCA after operation in case 2, which is consistent with the view of Zhanget al[20]. Some literatures suggest that the same temporal incision should be used when removing the ICL[20-22]along the long axis direction of ICL, without rotating the ICL. When the ICL was removed in the presented two cases, the 135 degree phacoemulsification corneal incision of Chinese traditional surgical method was adopted, and the ICL was directly taken out by alternating hands without rotating the ICL. In addition,it is not recommended to use a micro-incision, and Chinese scholars Yuet al[17]reported that ICL required a large incision to extract with 3 mm incision. The dissociation of capsulotomy should be carefully identified during the operation. It is still recommended to complete the capsulorhexis along the femtosecond laser trajectory for the removal of anterior capsule, so as to avoid the incomplete capsulotomy and the occurrence of capsulorhexis accidents.
Our reports confirm that FLACS is feasible in cataract after ICL implantation, but it may be more challenging than the conventional cataract cases without ICL implantation, while showing different results for different vaults. The surgeon should pay attention to every step during the surgery,especially for cases with low vault. It may be possible to select patients with high vault for FLACS, the whole surgery can complete successfully. At present, there are not a large number of cases to analyze that the FLACS will bring more safeties and benefits to such special patients. However, by the sufficient preoperative preparation and the optimization of surgical equipment parameters, the effect of surgery can fully achieve the expectation. We should have more prospective studies to observe the safety and feasibility.
ACKNOWLEDGEMENTS
Foundations:Supported by Key Research and Development Program of Shaanxi Province (No.2020SF-271;No.2017SF-273).
Conflicts of Interest:Li Y,None;Wang CY,None;Wu LA,None;Ma B,None;Dang GX,None.
 International Journal of Ophthalmology2023年2期
International Journal of Ophthalmology2023年2期
- International Journal of Ophthalmology的其它文章
- Perspectives and clinical practices of optometrists in Saudi Arabia concerning myopia in children
- Progression of myopia among undergraduate students in central China
- Flipped classroom approach to global outreach: crosscultural teaching of horizontal strabismus to Chinese ophthalmology residents
- Topical ketotifen treatment for allergic conjunctivitis: a systematic review and Meta-analysis
- Pseudomembranous conjunctivitis in a patient with DRESS syndrome
- Two cases of persistent shallow anterior chamber after cataract surgery combined with goniosynechialysis