
lncidence of rhegmatogenous retinal detachments is increasing in Wenzhou, China
2023-03-04 10:00MingNaXuJiaYuZhangHuiYangBenHaoSongRongHanWuZiPeiJiangKeMiFengMingXueRenKeLinZhongLin
Ming-Na Xu, Jia-Yu Zhang, Hui Yang, Ben-Hao Song, Rong-Han Wu, Zi-Pei Jiang,Ke-Mi Feng, Ming-Xue Ren, Ke Lin, Zhong Lin
1National Clinical Research Center for Ocular Diseases, Eye Hospital, Wenzhou Medical University, Wenzhou 325027,Zhejiang Province, China
2Department of Ophthalmology, the Third Affiliated Hospital of Wenzhou Medical University, Ruian 325200, Zhejiang Province, China
3Department of Ophthalmology, the Second Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang Province, China
4Department of Ophthalmology, the First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang Province, China
Abstract
● KEYWORDS: rhegmatogenous retinal detachments;retina; incidence; Chinese
INTRODUCTION
R hegmatogenous retinal detachment (RRD) is an ocular disease characterized by detachment between the retinal neuroepithelium layer and retinal pigment epithelium layer,with at least one retinal break, and which requires a confining operation to regain sight. Patients with a newly developed RRD will usually have sudden vision loss, accompanied by floaters and metamorphopsia, or a “dark curtain” blocking their vision, so would seek medical treatment immediately.The annual incidence of RRDs has been estimated in different countries and regions for a long time, ranging from 6.9-26.2 cases per 100 000 person-years[1-3]. The earliest observational report was from England, and the person-based rate of RRDs was 10.4 per 100 000 in 1968[4]. Until the late 1990s and the beginning of this century, the reported annual incidence of RRDs ranged from 7.98 to 17.9 cases per 100 000[5-7]. A recent study from The Netherlands reported a high incidence rate of 26.2 cases per 100 000[2]. Several risk factors at presentation are known, including male gender, age, myopia[2], lattice degeneration of the retina, history of intraocular surgery(e.g., cataract surgery)[8], ocular trauma[9], family history,seasonal variation[10]and race/ethnicity; Caucasian and Asian populations are at relatively higher risk[11-12].
Regarding the incidence of RRDs in the Chinese population,four previous studies, conducted in Beijing, Shanghai, Taiwan and in Singapore decades ago, reported the incidence to be 7.98-16.4 cases per 100 000[7,12-14]. Although these studies provided excellent insight into the incidence of RRDs in the Chinese population, there have been substantial economic changes and population aging since those studies were published. Furthermore, there is a lack of data on any changes in the incidence of RRDs in the Chinese population.Providing up-to-date data regarding RRD incidence and risk factors among the Chinese population has important clinical and public health value. We, therefore, performed this study to report the incidence of RRDs in Wenzhou, southeast China,from 2015 to 2019.
SUBJECTS AND METHODS
Ethical ApprovalThe study protocol was approved by the Human Ethics Review Committees of the Eye Hospital of Wenzhou Medical University. As a retrospective study,the ethics committee waived the need for written informed consent.
The Wenzhou area (simply referred to as “Wenzhou” from here down) is one of the large areas in the southeast region of China. The decision to select this district for the survey was made because of its stability, and because it has a socioeconomic profile representative of the wider population living in the Chinese hinterland. Wenzhou Prefecture includes the city of Wenzhou (4 municipal Districts: Lucheng,Longwan, Ouhai, and Dongtou) and its surrounding area includes Rui’an City (County-level city), Yueqing City(County-level city), Longgang City (County-level city),Pingyang County, Cangnan County, Yongjia County, Taishun County, and Wenchen County. According to the reports in the Wenzhou Statistical Yearbook for the correspondence year from Wenzhou Municipal Bureau of Statistics, the registered population totals (in thousands) of the area were 8112.1,8182.2, 8245.5, 8287.4, and 8323.6, in the years 2015 through 2019, respectively. RRD was diagnosed as detachment between the retinal neuroepithelium layer and the retinal pigment epithelium layer, with a definite retinal tear. The inclusion criteria for this study were: a newly developed case of RRD,with onset from January 1, 2015 to December 31, 2019; and permanent residence in Wenzhou. The exclusion criteria were:1) retina tear caused by traction (such as proliferative diabetic retinopathy), iatrogenic injury or ocular tumor; 2) subclinical RRD, which could be cured by a single retinal laser treatment;3) unclear diagnosis; 4) uncertain census registration; and 5) history of penetrating ocular trauma. Macular hole retinal detachments were not excluded from this study.
A total of four hospitals in Wenzhou had the capability to treat RRD patients. Almost all patients with RRD from the area sought treatment only at those hospitals. All four of the hospitals agreed to participate in this study. Medical information, including patients’ age and gender, location, date of RRD diagnosis, eye or eyes involved and eye axial length(AL), was obtained from the electronic surgical record systems of the hospitals. The AL of the affected eye was measured using standardized A-scan ultrasonography, and the healthy fellow eye was measured with an IOL-Master (Carl Zeiss Meditec, Dublin, CA, USA).
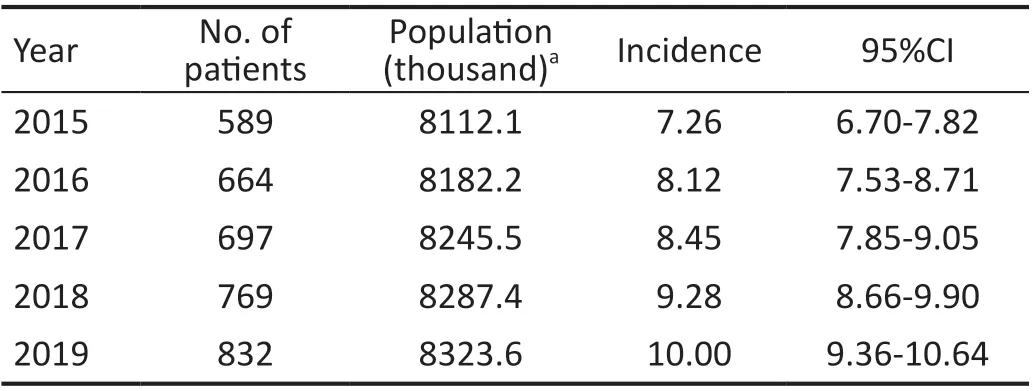
Table 1 Incidence (per 100 000 people) of RRD by year
Statistical AnalysisThe incidences of RRDs were calculated as the numbers of RRD cases divided by the population(in 100 000s). The 95% confidence intervals (CIs) of the incidences were also calculated, based on a Poisson distribution. The increase in annual incidence of RRDs was obtained by subtracting the annual incidence of the last year from that of the first year, and then dividing by 5. When further calculating the incidence by age groups, the population of each age group was obtained from the 2010 population census of China, since there were no such specific annual data for Wenzhou. It should be noted that the population from 2010 population census included both the registered population and migrant population.
RESULTS
A total of 3629 newly diagnosed RRD cases (3629 eyes)within the study period were screened from the medical systems of the four hospitals. Seventy-eight patients (156 eyes/3629, 4.30%) had bilateral RRDs. Twenty-five of those 78 patients (32.05%) developed bilateral RRDs in the same year.Ultimately, 3551 individual patients were enrolled for further analysis of incidence. The median age of the 3551 patients was 57 (range: 4-92)y. Thirty-seven cases (1.02%) were not treated by surgery. Among the 3629 cases, there were 1977 right eyes(54.48%) and 1652 left eyes (45.52%), 291 cases (8.02%)included macular hole retinal detachment.
The average incidence of RRDs was 7.79 cases per 100 000(95%CI, 7.24-8.34). There were 1916 males (53.96%) and 1635 females (46.04%). The average incidence of RRDs among males was 7.99 cases per 100 000 (95%CI, 7.22-8.76),and among females was 7.56 cases per 100 000 (95%CI, 6.77-8.35). The annual incidence increased gradually from 7.26 cases per 100 000 in 2015 to 10.00 cases per 100 000 in 2019(Table 1).
In 2019, the Wenzhou population had increased by 2.61%compared with that in 2015. In contrast, the overall RRD incidence rate in 2019 had increased by 37.74% compared with 2015. The rate of RRD increase was 0.55 cases per 100 000,and the increase among males was slightly higher than that among females (0.59vs0.49, respectively). During the 5-year survey period, the RRD incidence also displayed a year-to-year growth in both males and females, and males always had a higher annual incidence than their female counterparts (Figure 1).The overall incidence in males increased by 39.78% (10.4 per 100 000vs7.44 per 100 000) and in females by 35.22% (9.56 per 100 000vs7.07 per 100 000) from 2015 to 2019.
The distribution of incidences by age categories is presented in Table 2. Across the study population, 8.11% of individuals were less than 30y, 21.18% were 30-50y, 59.25% were 50-70y,and 11.46% were 70y or older.
The incidence rate increased considerably after age 50 and decreased after age 80. We also found that the highest peak occurred in the age group from 60-69y, with an incidence of 42.61 per 100 000 (95%CI, 38.33-46.89). The age-specific incidence rates for males and females are shown in Figure 2.The incidence peaks for both males and females were also in the 60-69y age group. Males had a higher incidence than females across most age categories, except for the age groups from 50-69y. In the past 5y, the increase in annual incidence of RRDs was largest in the age group from 60-69y (2.81 cases per 100 000 per year), followed by the age group from 70-79y(2.16; Table 3).
Because high myopia carries a high risk of developing an RRD, we also conducted analysis of ALs. AL information was available for a total of 2750 eyes (77.4%). Of those,1675 (60.91%) had an AL greater than 24 mm. The mean ALs were 25.28±2.50 (range: 16.06-37.34) mm overall, and 25.35±2.52 (n=1558, range: 20.38-35.63) mm and 25.19±2.48(n=1192, range: 16.06-37.34) mm for the right and left eyes,respectively. The mean AL was 25.28±2.31 mm in men and 25.28±2.70 mm in women. Furthermore, males had a higher percentage of ALs greater than 24 mm than did their female counterparts (65.08%vs56.24%). Individuals younger than 50y had both longer ALs (26.37±2.51 mm versus 24.82±2.35 mm,P<0.001) and a higher proportion of ALs greater than 24 mm(82.67%vs51.85%,P<0.001) than did those ≥50y. There were no significant changes in ALs over time (Table 4).
The monthly numbers of RRD cases are presented in Figure 3.The maximum number of cases were observed in April (n=334,9.20%) and August (n=316, 8.72%). The minimum number of cases was recorded in November (n=265, 7.31%).
DISCUSSION
The population-based incidence of retinal detachments has been reported in many areas (Table 5)[2,5,7,13,15-23]. In China,population-based data investigating the incidence of RRDs are scarce, especially regarding any trend in variation of the incidence. The present study provides data on the 5-year incidence in Wenzhou, southeast China. Importantly, we provide a comprehensive review of RRD incidence, as well as its recent 5-year trend in Wenzhou, home to more than 8 million residents. In this study, we found that the incidence of RRDs in Wenzhou gradually increased from 7.26 cases per 100 000 in 2015 to 10.0 cases per 100 000 in 2019. The incidence of RRD in Wenzhou is similar to that reported in Beijing[7](7.98 per 100 000) and among Chinese people in Singapore[12](11.6 per 100 000), but is lower than that reported in Taiwan[15](16.4 per 100 000) and Shanghai (14.4 per 100 000)[13]. The incidence was also lower than that reported in developed countries (14.81-26.2)[2,16].
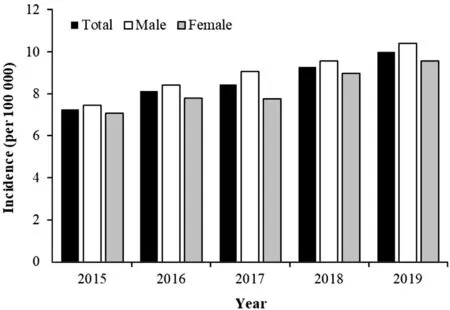
Figure 1 Incidence of RRDs by year and gender RRD: Rhegmatogenous retinal detachment.

Figure 2 Incidence of RRDs by age RRD: Rhegmatogenous retinal detachment.
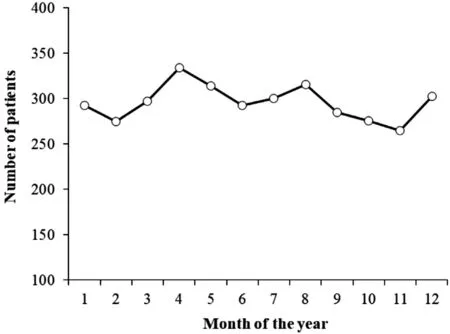
Figure 3 The number of cases of RRDs by month of the year RRD:Rhegmatogenous retinal detachment.
Rhegmatogenous Retinal Detachment Incidence IncreasingPrevious studies have reported an increase in RRD incidence.Hajariet al[17]observed that the incidence of RRD increased in Denmark at a rate of 0.40±0.04 cases per 100 000 during the period 2000 to 2011. Another study, also conducted in Denmark, showed that the age- and sex-standardized RRD incidence rate had sharply increased, by more than 50%,between 2000 and 2016[1]. In the Netherlands, it was also found that a 44% increase in incidence of primary RRDs occurred over a 7-year period, which may be explained by the simultaneous myopic shift in the population[2]. Conversely, a population-based study in Taiwan did not found a change in age-standardized incidence of RRDs from 2000 to 2012[15]. In our study, the incidence of RRD apparently also increased, by 37.74%, in Wenzhou during the past 5y.Several factors may underlie this significant increase. Rapid population aging is likely to result in greater numbers of RRDs[16]. China’s population has the following characteristics:a high speed of aging, a high level of aging population and massive size. China’s population is aging faster than that in other countries, which may be associated with the birth control policy, and also attributed to the decrease in the desire for children among the Chinese. It has been predicted that the proportion of elderly people in China’s population will reach 19.25% in 2030[24]. By 2010, the proportion of children(aged 0-14y) among the whole population in Wenzhou had decreased by 5.49%, relative to 2000, whereas the proportion of those older than 60y had increased by 0.71%[25]. Older age is an important risk factor for RRDs[26]. The highest RRD incidence in our study was observed in the age group of 60 to 69y. We did not observe a bimodal distribution according to age groups, as described in some studies from Asia[15,18]. We found that the fastest rate of incidence increase occurred in the 60-69-year-old group. Other studies have described similar findings regarding this peak age[16]. With increasing age,vitreous humor liquefaction and posterior vitreous detachmentprogress gradually. Posterior vitreous detachment increases rapidly around age 60 to 70y[27], which may contribute to the occurrence of RRDs[16].
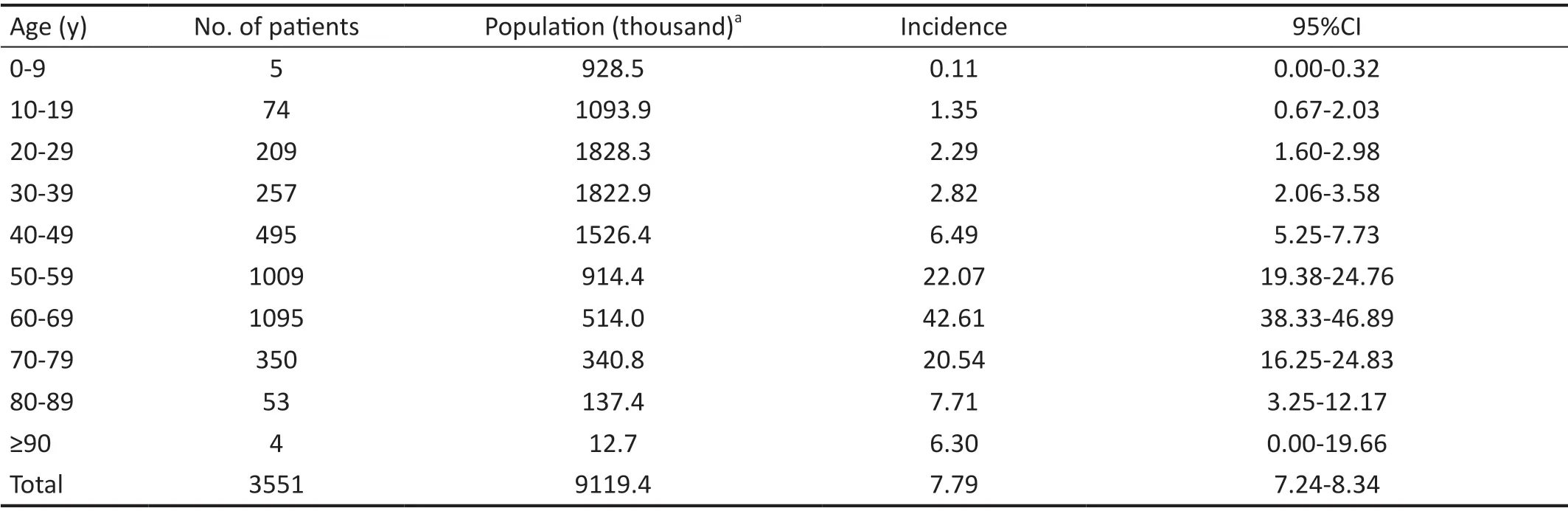
Table 2 Incidence (per 100 000 people) of RRD by age

Table 3 Number and incidence (per 100 000 people) of RRD by age and year n (%)

Table 4 Mean ocular AL (mm) by year

Table 5 Summary of incidence of RRDs reported in the previous 2 decades
Another important factor may be the drastic growth of the cataract-surgery rate in the elderly population. For example,phacoemulsification increases the risk of RRD by at least 1.7 times[1]. In China, as the largest developing country in the world, the rate of cataract surgeries has dramatically increased in recent decades[28-29]. It has been reported that there is a 58.6%-78.7% rate of posterior vitreous detachment after cataract surgery[8,30], which may be a major promotor of pseudophakic retinal detachment[9,27]. Petousiset al[31]found that male gender, longer AL (>25 mm) and posterior capsular rupture, with vitreous loss during cataract surgery, carries an increased incidence of RRD.
Myopia or longer AL are well-established risk factors for RRD, and the impact of long AL is especially great in young individuals[2,14-15,32-33]. van Leeuweenet al[2]found a myopia shift in Dutch individuals aged 55 to 75y, through a populationbased study. In the current study, the young patients with RRDs had relatively longer ALs. Among the elderly, the proportion with a long AL was lower, which suggests that senile vitreous liquefaction and detachment is the main mechanism of RRD in old age[32]. It was found that 66.5% of eyes in RRD patients in Beijing were myopic[7,14]. Similarly, the majority of the RRD cases (60.91%) in the present study had an AL greater than 24 mm. However, we did not observe an increase in average AL from 2015 to 2019 in this study. Hence, further studies are warranted.
GenderConsistent with other reports[34], RRDs occurred more frequently in males than females in this study. A higher incidence of RRDs was found in males in each year of our study and in almost every age group. Male gender is a wellrecognized risk factor for RRDs[16]. Long AL may be a reason for the higher incidence of RRD in males[15]. Indeed, our data showed that the males had a higher proportion of longer ALs (>24 mm) then did the females (65.08% versus 56.24%,respectively). Furthermore, higher likelihoods of physical labor and trauma in men may also contribute[15,17].
Disease LateralityA higher incidence of RRDs was observed among right eyes than left eyes. Similar phenomena were reported in previous studies[17]. Mitryet al[26]hypothesized that this might be because right eyes are more commonly dominant,and dominant eyes are frequently more myopic, although the difference in AL and spherical equivalent refraction between right and left eyes was not statistically significant in their study.Our data show that the mean AL in the right eye was slightly longer than in the left eye. Sevillano Torradoet al[35]proposed another hypothesis, one about solar radiation: ultraviolet radiation might promote the formation of a posterior vitreous detachment in dominant eyes.
Seasonal VariationSeveral studies have observed seasonal variation in the occurrence of RRDs[35-37]. In our study, a seasonal distribution was detected, with the maxima in April and August, and minimum in November. These results align with the previous articles that reported a maximum at the end of the spring[35]and in summer months[36-37], and a minimum in the winter months. Nevertheless, an explicit reason for the phenomenon is not yet clear. The impact of climate might be an important factor. In the summer months, there are more hours of sunshine, which means greater radiation intensity,higher temperature[10,38]and lower rainfall than in the winter months, which may be associated with a higher incidence of RRDs. We believe that this seasonal variation may also be due to variations in outdoor physical labor,e.g., a reduction in winter months. However, seasonality had no association with RRD in some other studies[7,16].
There were some limitations in this study. First, we may have underestimated the RRD incidence in Wenzhou. Some patients with an RRD may not have undergone surgery or may have visited a hospital outside the area, due to population movement. The second limitation relates to information bias,as follows. In the subgroup analyses of the age-specified population, we choose the national census age data from 2010,owing to the lack of corresponding annual data for Wenzhou.This national census indicated a larger population, hence there was an underestimation of RRD incidence in the age groups.Third, the AL measurements may have been inaccurate after the detachments developed, especially in cases of macular detachment.
In conclusion, the incidence of RRDs has increased by 37.74%in Wenzhou during the past 5y. Higher incidences of RRDs in older patients (60-69y), in male patients, and in right eyes were observed. We also found that RRDs in the Wenzhou area show seasonal variation, peaking at the end of spring and in the summer months.
ACKNOWLEDGEMENTS
Foundations:Supported by Zhejiang Provincial Highlevel Health Talents Training Project (No.CZ-RC2022010);Wenzhou Basic Medical and Health Technology Project (No.Y20220779).
Conflicts of Interest: Xu MN,None;Zhang JY,None;Yang H,None;Song BH,None;Wu RH,None;Jiang ZP,None;Feng KM,None;Ren MX,None;Lin K,None;Lin Z,None.
 International Journal of Ophthalmology2023年2期
International Journal of Ophthalmology2023年2期
- International Journal of Ophthalmology的其它文章
- Perspectives and clinical practices of optometrists in Saudi Arabia concerning myopia in children
- Progression of myopia among undergraduate students in central China
- Flipped classroom approach to global outreach: crosscultural teaching of horizontal strabismus to Chinese ophthalmology residents
- Topical ketotifen treatment for allergic conjunctivitis: a systematic review and Meta-analysis
- Pseudomembranous conjunctivitis in a patient with DRESS syndrome
- Two cases of persistent shallow anterior chamber after cataract surgery combined with goniosynechialysis