
A canine model of aortic arch aneurysm created with autologous pericardium
2022-10-18 08:30:38WixioLiJunLiQingliMingzhCuiRutoXuShuitingZhiChshirNikTinxioLiJingboChnWnliZho
Wixio Li, Jun Li, Qing li, Mingzh Cui, Ruto Xu, Shuiting Zhi, Chshir Nik,Tinxio Li, Jingbo Chn, Wnli Zho
a Department of Vascular and Endovascular Surgery, Zhengzhou University People's Hospital, Henan Provincial People's Hospital, Zhenghou, China
b Operation Department, Zhengzhou University People's Hospital, Henan Provincial People's Hospital, Zhenghou, China
c Department of Medical Imaging, Zhengzhou University People's Hospital, Henan Provincial People's Hospital, Zhenghou, China
d Department of Vascular Surgery, Royal Brompton and Harefield Hospital, London, UK
e Department of Cerebrovascular Disease, Zhengzhou University People's Hospital, Henan Provincial People's Hospital, Zhenghou, China
Keywords:Aortic aneurysm Pericardium patch Ascending aorta Aortic arch Animal model
ABSTRACT
1. Introduction
The incidence of thoracic aortic aneurysms appears to be increasing.1,2Currently, the treatments for thoracic aortic aneurysms include open surgery, hybrid surgery, and endovascular repair.Compared to open surgery and hybrid surgery, endovascular repair has lower rates of procedure-related mortality and morbidity.3–5However,the aortic arch is still a challenge when performing endovascular repair because the supra-aortic vessels cannot be covered by stent grafts.4New endovascular devices and techniques should be investigated to overcome this challenge. To date, there has been no animal model suitable for studying these new endovascular devices and techniques applied to the aortic arch.In this article, we describe a canine model of an aortic arch aneurysm created using an autologous pericardial patch.
2. Materials and methods
This study was approved by the Animal Care and Use Committee of Zhengzhou University. Fifteen adult female mongrel dogs weighing 20.0–33.0 kg were provided by the Laboratory Animal Center of Zhengzhou University.
All animals underwent computed tomography angiography (CTA)before surgery. CTA was performed using a 256-row CT scanner (Brilliance iCT,Philips,USA)in the craniocaudal direction to cover the entire body. A nonionic iodinated contrast agent (Optiray; Tyco Healthcare,Montreal,Quebec,Canada)was injected at a rate of 4 mL/s using a dualsyringe power injector (Ulrich Medizintechnik, Germany) for a total of 40–60 mL each time, followed by 40 mL of 0.9% sodium chloride solution at the same rate.The ascending aortic arch was defined as the region of interest(ROI).The trigger threshold inside the ROI was set at 100 HU.The maximal diameter of the aortic arch was measured using a commercial software(ADW 4.4;General Electric Company,USA).

Abbreviations:CTA Computed tomography angiography HE Hematoxylin and eosin ANOVA Analysis of variance TEVAR Thoracic endovascular aortic repair ROI Region of interest VR Volume rendering CPR Curved planar reformation RIA Right innominate artery LIA Left innominate artery AA Aortic arch
After fasting for 12 h, the animals were anesthetized with an intramuscular injection of Sumianxin II at 0.1 mL/kg (Jilin Research and Development Center of Veterinary Drug, Jilin, China) and 3% pentobarbital sodium at 0.5 mL/kg (Kefeng Chemical Reagent Co., LTD,Shanghai, China). Anesthesia was maintained with propofol 20 mL/h(Xian Nippon Pharmaceutical Co., LTD, Xian, China) under mechanical ventilation (AM100B; Yishiheng Co., Beijing, China). The dogs were fixed on the operating table in the supine position.The chest was shaved.Venous access was established via the superficial vein of the left hind leg.A median sternotomy was performed. A piece of pericardium was resected and fashioned into a 4×4 cm patch(Fig.1).The aortic arch,left innominate artery, right innominate artery, and proximal descending thoracic aorta were isolated and lifted using a blocking band.The anterior wall of the aortic arch was clamped using a Satinsky clamp as much as possible without stopping the flow of the distal aorta and two innominate arteries(Fig.2).A 3-cm transverse incision was made in the clamped anterior wall of the aortic arch. The pericardial patch was oversized compared to the aortotomy patch to facilitate the formation of an aneurysmal sac. The pericardial patch was sewn onto the aortotomy using a 5-0 prolene suture in a continuous over-and-over running suture,and spacers were used to reinforce the suture margin (Fig. 3). The Satinsky clamp was then removed from the aorta. After hemostasis was achieved,the blocking bands were removed.Finally,the thoracic cavity was closed. An enhanced computed tomography (CT) scan was performed (Fig. 4). The dogs were administered penicillin sodium (1.6 MU/d via intramuscular injection) for three days following the operation. The operative time from the skin incision to the closure of the thoracic cavity was recorded. The duration of the aortic arch clamping was also recorded.

Fig.1. An autologous pericardium patch(4×4 cm)was resected and fashioned during the operation.

Fig. 2. Clamping the anterior wall of the aortic arch. Right innominate artery(RIA), left innominate artery (LIA), aortic arch (AA).

Fig. 3. Aortic arch aneurysm model. Aortic arch (AA).
The animals were followed up for 3 months. CTA was performed at the end of each month. The aneurysm models were visualized using volume rendering (VR) and their maximal diameters were measured using curved planar reformation(CPR).
At 3 months, all the dogs were euthanized with 10% potassium chloride solution intravenously under general anesthesia.The aortic arch was then resected. The specimens were fixed in a 10% formaldehyde solution and embedded in paraffin for histological examination using light microscopy after HE staining.
Statistical analysis was performed using the statistical software SPSS 22.0 (SPSS Inc., Chicago, IL, USA). Numerical data are expressed as the mean ± standard deviation. Changes in aneurysm diameter over time were analyzed using ANOVA.
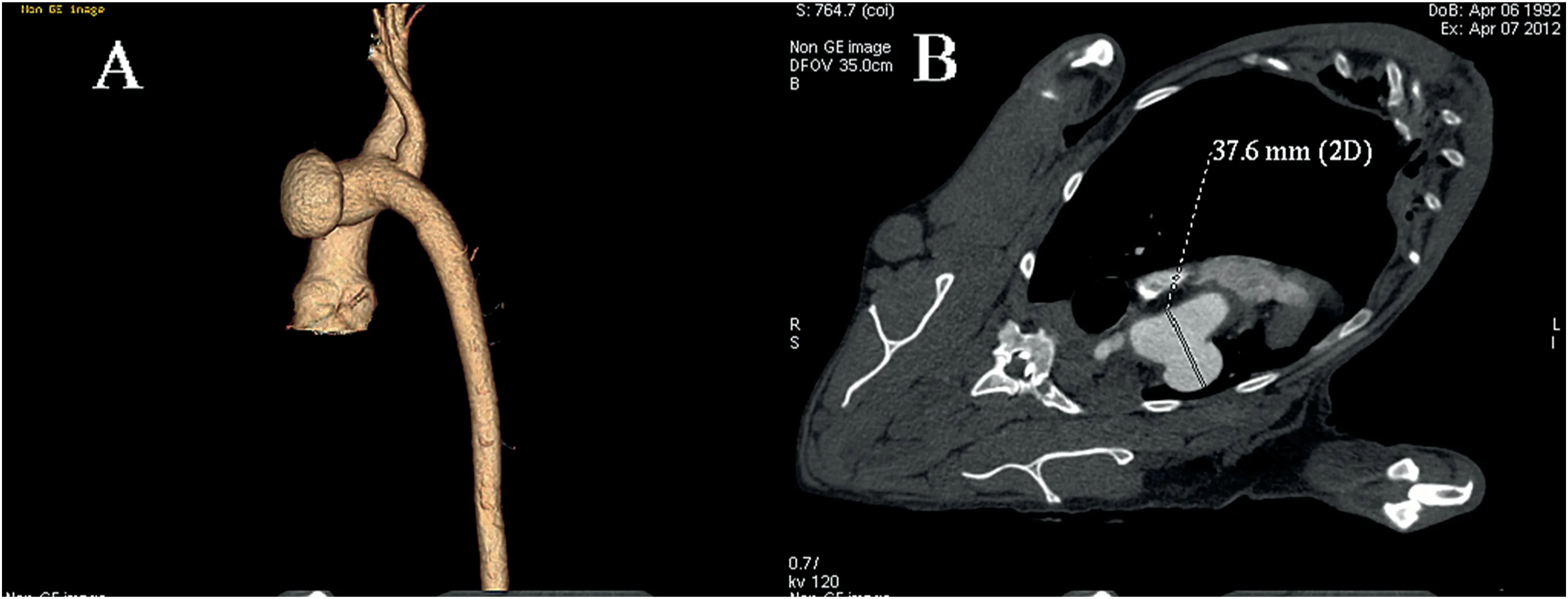
Fig. 4. (A) The volume reconstruction imaging of the aneurysm model; (B) The maximal diameter of the aneurysm model was measured using the curve planar reconstruction.
3. Results
One animal died of hemorrhage caused by slippage of the Satinsky clamp during the operation. Fourteen animals survived the surgical procedures. However, two animals died on the first day after surgery.Autopsies showed that the two dogs died from ruptures at the suturing margin. There were no complications such as infarction at distal sites,paraplegia, or serious infection in the remaining animals during the follow-up period.The average operation time was 195.0±25.8 min.The clamping time of the anterior wall of the aortic arch was 43.7±5.8 min.
The aneurysm model created using an autologous pericardial patch was a saccular aneurysm. According to the Criado classification,22the aneurysm model was located in Zone 1(Fig.4).Before the operation,the maximal diameter of the aortic arch was 17.11±1.40 mm.The maximal diameter of the aneurysm model was 35.26 ± 4.30 mm on the first day after the operation.The diameter of the aneurysm model was twice that of the aortic arch. The diameters of the aneurysm model at month 1,month 2, and month 3 were 34.85 ± 4.64 mm, 34.75 ± 4.47 mm, and 34.79 ± 4.51 mm, respectively. There was no significant change in the maximum diameter of the aneurysm model during the follow-up period(p =0.990).
Macroscopic examination revealed that the pericardial patch was well-incorporated into the aortic wall(Fig.5).Microscopic examination revealed that the outer surface of the pericardial patch was covered with mechanocytes and collagenous fibers, and the inner surface of the aneurysm was covered with endotheliocytes(Fig.6).
4. Discussion
Endovascular repair has been the most popular treatment for thoracic aortic aneurysms because of the lower incidence of procedure-related mortality and morbidity.3–5However, the aortic arch remains a challenge for endovascular repair because the supra-aortic vessels cannot be covered by stent grafts.4Total endovascular techniques in the aortic arch include the fenestrated stent graft, branched stent graft, and chimney technique.6–11Fenestrated stent grafts and branched stent grafts are complex and not widely available.12With regard to the chimney technique, the risk of a type Ia endoleak from the gutters between the main aortic graft and the chimney graft is much higher than that of other techniques.13Therefore, new endovascular devices and techniques must be developed to overcome these challenges.Before these new techniques can be applied clinically,their efficiency and safety must be tested in vivo.Various aortic aneurysm models have been previously reported.14–21However,the majority of these aneurysm models involved the abdominal or thoracic aorta. Thus far, there has been no animal model suitable for research on new techniques applied to the aortic arch. In this study, we established a novel canine model of aortic arch aneurysm.According to the Criado classification,22the aneurysm model was located in zone 1.

Fig. 5. The specimen of the aortic arch aneurysm model. The pericardial patch was well incorporated into the aortic wall. Right innominate artery (RIA), left innominate artery (LIA).
The incidence of endoleak after thoracic endovascular aortic repair(TEVAR) for aortic arch aneurysms is much higher than that of other aneurysms because of the curve of the aortic arch and the supra-aortic vessels.23There are many reports about the animal model of thoracic aortic dissection.24–26However,the false lumens of these animal models are narrow, and the tears of the intima are small. The false lumen and tears of the intima can be easily sealed by common stent grafts. Therefore, they are unsuitable for research on endoleaks after TEVAR. In the aortic arch aneurysm model,the maximal diameter of the aneurysm was two times larger than that of the aortic arch.The ostium of the aneurysm model was much larger than that of the aortic dissection model.Although the aneurysm model is a saccular aneurysm, and fusiform dilatation of the aortic arch is not apparent,the aneurysm model,compared with the aortic dissection model,is much more suitable for research on endoleaks after TEVAR.

Fig. 6. The pericardium patch was covered by mechanocytes and collagenous fiber. The inner surface of the aneurysm wall was covered by endotheliocytes(HE staining, × 40).
Formichi et al.created animal models of thoracic aortic aneurysms in mongrel dogs using polyester patches,which cannot imitate the structure of natural aortic aneurysms.15Kajimoto et al.used jugular vein patches to create thoracic aortic aneurysms in beagles.17However, the use of jugular vein patches increased the risk of trauma and infection. An autologous pericardial patch was used to create the aneurysm. A medial sternotomy can fully expose the aortic arch and the pericardium.The use of autologous pericardium did not increase the trauma of the operation.
There are many reports on elastase, hypoxia inducible factor, and leptin-mediated Ang II-induced aneurysm models.19–21These aneurismal models could imitate the formation mechanism of human aneurysms.However, the diameter of the aneurysm model could not be controlled;thus, the diameter of the aneurysm model might continue to increase.Animals might die from aneurysm rupture before undergoing endovascular repair. Additionally, the diameters of the aortae of the animals in this study were small. They were not suitable for research on endovascular instruments. In this study, we could control the diameter of the aneurysm model by adjusting the diameter of the patch. To prevent the rupture at the suture margin,spacers were used to reinforce the margin.During the follow-up period,the diameter of the aneurysm model did not change significantly. Therefore, the aneurysm model created using autologous pericardium patch was more controllable and could be easily reproduced. Mongrel dogs were chosen as experimental animals. The diameter of the aortic arch in mongrel dogs (20.0–33.0 kg) is 17.11 ±1.40 mm.This diameter is sufficiently large for research on endovascular devices.10,27In addition, histological examination showed that the aneurysm wall was much thinner than that of the thoracic aorta, the outer surface of the pericardium patch was covered with mechanocyte and collagenous fiber, and the inner surface of the aneurysm wall was covered with endotheliocytes.These characteristics were similar to those observed in natural aneurysms.
A limitation of this study is that the aortic arches of all domestic animals are different from those of humans.28There are only two supra-aortic vessels on the canine aortic arch.
In conclusion, we established a controllable and stable aortic arch aneurysm model created with an autologous pericardium patch. The aneurysm model can be used to research endoleaks after TEVAR and new endovascular techniques applied to the aortic arch.
Funding
This study was supported by the Henan medical science and technology research projects (222102310014 and LGHJ20200058).
Declaration of competing interest
We declare that we do not have any commercial or associative interest that represents a conflict of interest in connection with the work submitted.
Acknowledgements
We thank Professor Ke Xu(First Affiliated Hospital of China medical University)for his valuable comments.
 Journal of Interventional Medicine2022年3期
Journal of Interventional Medicine2022年3期
- Journal of Interventional Medicine的其它文章
- A review of high-intensity focused ultrasound as a novel and non-invasive interventional radiology technique
- Ultrasound-guided microwave ablation for symptomatic adenomyosis: More areas of concern for more uniform and promising outcomes
- Balloon-occluded retrograde transvenous obliteration with lauromacrogol sclerosant foam for gastric varices
- Recent advances of multimoda ultrasound in image-guided prostate-targeted biopsy
- Diagnosis of hepatic inflammatory pseudotumor by fine-needle biopsy
- Efficacy of contrast-enhanced ultrasound-guided percutaneous core needle biopsy in anterior mediastinal masses