
Exosomal glypican-1 is elevated in pancreatic cancer precursors and can signal genetic predisposition in the absence of endoscopic ultrasound abnormalities
2022-08-18 03:16PedroMoutinhoRibeiroInesBatistaSofiaQuintasBarbaraAdemMarcoSivaRuiMoraisArmandoPeixotoRosaCoelhoPedroCostaMoreiraRenatoMedasSusanaLopesFilipeVilasBoasManuelaBaptistaDiogoDiasSilvaAnaEstevesFilipaMartinsJoanneLopesHelena
World Journal of Gastroenterology 2022年31期
Pedro Moutinho-Ribeiro, Ines A Batista, Sofia T Quintas,Barbara Adem, Marco Siva,Rui Morais,ArmandoPeixoto, Rosa Coelho, Pedro Costa-Moreira, Renato Medas, Susana Lopes, Filipe Vilas-Boas,ManuelaBaptista, Diogo Dias-Silva,Ana L Esteves, Filipa Martins,Joanne Lopes, Helena Barroca, Fatima Carneiro,Guilherme Macedo, Sonia A Melo
Abstract
Key Words: Glypican-1; Circulating exosomes; Endoscopic ultrasound; Pancreatic cancer risk groups;Pancreatic cancer precursor lesions; Genetic predisposition
lNTRODUCTlON
Pancreatic ductal adenocarcinoma (PDAC) is considered one of the deadliest malignant diseases around the world, and is estimated to become the second leading cause of cancer-related deaths in the United States in 2030[1]. Most patients present with advanced disease at diagnosis, with only 20% being candidates for surgical treatment, the only chance for cure[2,3].
In its early stages, PDAC usually develops with few or no symptoms, and current sectional imaging modalities are inadequate to detect early small lesions[3]. Endoscopic ultrasound (EUS) is a highly accurate diagnostic technique for pancreatic lesions, with its role majored by the possibility of performing EUS-guided tissue acquisition[4-6].
Among PDAC precursor lesions are pancreatic intraepithelial neoplasias (PanINs) and mucinous cystic lesions (MCLs)[7,8]. While the former are very difficult to identify by available imaging modalities, the latter can be more clearly detected and characterized, specially by magnetic resonance imaging (MRI)/magnetic resonance cholangiopancreatography (MRCP) and EUS[5,9].
Along with the improvement of imaging diagnostic accuracy, the search for a biomarker that could adequately identify PDAC at early stages or its high-risk precursor lesions is a top research priority. The only biomarker approved for clinical use is carbohydrate antigen 19-9 (CA 19-9), but it lacks sensitivity and specificity for PDAC early detection, being mostly reserved for monitoring response to therapy and disease progression[10]. In recent years, several molecules have been tested to serve this purpose[11,12].Among these, membrane-anchored proteoglycan glypican-1 (GPC1) has been shown to be a good candidate. We previously studied GPC1 in circulating exosomes (crExos) and found that it could identify PDAC patients among healthy individuals with perfect accuracy[13]. In addition, GPC1+crExos correlated with tumor burden and patients’ survival. Moreover, in a genetically engineered mouse model of PDAC, GPC1 was overexpressed in crExos even before the tumor could be detected by MRI[13]. Finally, we also showed higher levels of GPC1+crExos in MCL compared to controls, although the number of patients was very limited[13]. Several studies have demonstrated the role of GPC1 in PDAC[14-18]. Considering the distinct methodologies that some of the studies adopted to study GPC1 in circulation, some support the potential of GPC1+crExos as a biomarker for early detection of PDAC[14,15,19], while others only demonstrate their correlation with disease burden[16-18].
At present, while 90% of PDAC cases are sporadic, only individuals harboring increased hereditary risk (HR), either kindreds of familial pancreatic cancer (FPC) (7%) or belonging to other cancer syndromes with increased risk of PDAC (3%), are candidates for screening[20-22]. Nevertheless, there are other well-defined PDAC-associated risk groups that deserve special attention and can constitute a refined population to be surveilled in order to increase the rate of early detection and improve overall survival. One of these groups is composed by individuals older than 50 years with a recent (< 36 mo)diagnosis of type II diabetes mellitus (DM). Increasing epidemiological, clinical, and experimental evidence shows that new-onset DM can be a clinical manifestation of asymptomatic PDAC or harbinger the disease and offers the promise for early detection in these individuals[3,23-26]. In fact, although the complex and multidirectional relationship between the two entities is not fully understood, new-late onset DM (NLOD) has been recognized as an entity signaling a 6- to 8-fold increased risk of developing PDAC in 3 years[27].
We previously showed that levels of GPC1+crExos discriminate PDAC from chronic pancreatitis (CP)with high accuracy[28]. In this work, we aimed to determine the capacity of GPC1+crExos to identify individuals at higher risk of developing PDAC, comparing its levels with EUS pancreatic abnormalities(PA) within specific risk groups: MCL, HR, and NLOD.
MATERlALS AND METHODS
Design of the study and population
This cross-sectional study with a prospective unicentric cohort included 88 subjects: 40 patients with MCLs, 20 individuals with HR, 20 patients with NLOD, and 8 individuals in the control group (CG).The inclusion period was between October 2016 and January 2019, and the study was approved by the Ethics Committee of Centro Hospitalar Universitário de São João (CHUSJ) (ID No. CES 327-15), Porto,Portugal. All patients provided written informed consent and underwent blood sample collection at the time of EUS.
In the MCL group, we considered for inclusion both intraductal papillary mucinous neoplasms(IPMNs) and mucinous cystic neoplasms (MCNs). For its diagnosis, we used both imagiological and cyst fluid analysis criteria. We have assumed IPMN etiology when EUS and/or MRCP clearly showed communication of the cyst(s) with the pancreatic ductal system. In this situation, branch-duct type (BDIPMN) were presumed if multiple and no dominant main pancreatic duct (MPD) dilation was seen.Main-duct IPMN (MD-IPMN) was considered if a segmental or diffuse dilatation of the main duct > 5 mm was observed without any other cause of obstruction. Mixed-type IPMN (MT-IPMN) was defined when features of MD-IPMN and BD-IPMN coexisted[29]. MCN was assumed when a mucin-producing cyst forming epithelial neoplasia of the pancreas with a distinctive ovarian-type stroma was present,typically with no communication with the ductal system[30].
We performed EUS-guided fine needle aspiration (FNA) in almost all cystic lesions included.Mucinous nature was supported by a fluid carcinoembryonic antigen (CEA) > 192 ng/mL and/or fluid glucose < 50 mg/dL[31]. In relation to amylase content, if > 250 U/L, a diagnosis of IPMN was likely,whereas levels < 250 U/L suggested MCN. If the aspirated content was sufficient, a sample was also evaluated by experienced cytopathologists.
In the HR group, we considered for inclusion FPC (family history of PDAC in at least two firstdegree, or in three or more first- and second-degree relatives) and PDAC susceptibility gene mutation carriers[20,22,32,33]. All of these individuals had a clinically and genetically established diagnosis and have been followed in a dedicated consultation for hereditary digestive cancers in our institution. They underwent detailed evaluation of family history, and verification of cancer diagnoses by review of medical records and genetic testing.
In the NLOD group, we included patients aged ≥ 50 years who had been diagnosed with type II DM within a period of 36 mo[23,24]. Diagnosis of type II DM was made according to the American Diabetes Association and consisted of: Fasting plasma glucose level ≥ 126 mg/dL, a 2-h plasma glucose level of ≥200 mg/dL during a 75-g oral glucose tolerance test, a random plasma glucose level of ≥ 200 mg/dL in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, or a hemoglobin A1c level of ≥6.5%[34].
In the CG, individuals who underwent EUS for other reasons than pancreatic pathology were included with a normal pancreas and absence of hereditary/familial risk factors. The exclusion criteria were patients unable or unwilling to give informed consent, individuals younger than 18 years of age,pregnancy or breast feeding, contraindications to endoscopic procedures or contrast administration,contraindications to computed tomography (CT) or MRI, coagulopathy (prothrombin time > 50% of control, activated partial thromboplastin time > 50 s, or international normalized ratio > 1.5), patients on chronic anticoagulation, platelet count < 50000/μL, and inability to tolerate sedated upper endoscopy due to cardiopulmonary instability or other contraindication to endoscopic procedures.
At the time of inclusion, immediately before EUS examination, a blood sample was collected for complete blood count as well as renal, liver, and pancreatic chemistry at the CHUSJ laboratory. A separate blood sample collected at the same time was used to quantify CA 19-9 serum levels (ab108642,CA 19-9 Human ELISA Kit; Abcam, Cambridge, MA, United States) and GPC1 expression in crExos by fluorescence-activated cell sorting (FACS) (Figure 1). For CA 19-9, the standard clinical cut-off of 37 U/mL was used. A complete personal and family clinical history was registered, and demographic data was recorded [age, body mass index (BMI)], previous history of pancreatic disease, smoking and drinking habits, history of diabetes and duration since diagnosis, digestive and systemic symptoms.Laboratory values and previous results of cross-sectional imaging (CT, MRI, or magnetic resonance cholangiopancreatography) were registered. The results of the EUS evaluation at the time of inclusion in the study as well as transechoendoscopic or surgically collected specimens were also recorded.
All subjects were observed, examined, and followed-up at the Department of Gastroenterology of CHUSJ (Porto, Portugal) until death or July 2021.
EUS, tissue acquisition techniques, and fluid/specimen analyses
All EUS evaluations were performed by three experienced endoscopists under deep sedation (propofol or pethidine plus midazolam as assisted by an anesthesiologist). Linear scopes from Olympus®(GTUCT140, GT-UCT180; Tokyo, Japan) and Pentax®(EG-3670UTK, EG-3870UTK; Tokyo, Japan) along with Olympus®EU-ME2 and Hitachi Avius®(Tokyo, Japan) image processors were used.
PA were classified into major and minor changes. Major changes comprised cystic lesions, CP-like parenchymal changes, and solid lesions. Minor ones constituted changes in pancreatic echogenicity compatible with lipomatous transformation[35,36]. EUS high-risk stigmata (HRS) and worrisome features (WF) were categorized according to the International consensus of Fukuoka guidelines for the management of IPMN of the pancreas[29]. A main duct dilatation ≥ 10 mm or an enhancing mural nodule > 5 mm were classified as HRS, whereas a main duct dilatation between 5 and 9 mm, an enhancing mural nodule < 5 mm, a cyst diameter > 3 cm, the presence of thickened/enhancing cyst walls, an abrupt change in pancreatic duct caliber with distal pancreatic atrophy, and lymphadenopathy were considered WF.

Figure 1 Schematic representation of the workflow for the analysis of circulating exosomes from control group, mucinous cystic lesions,hereditary risk and new-late onset diabetes mellitus patients for the expression of glypican-1. Scheme illustrating the workflow of our study of the expression of glypican-1 (GPC1) on exosomes retrieved from patients’ blood samples, from blood collection to the analysis by flow cytometry of GPC1+ circulating exosomes (crExos). A representative histogram of the percentage of beads bound to GPC1-positive crExos (GPC1+ crExos) that were isolated from the serum of a control group, composed by individuals submitted to endoscopic ultrasound for other reasons than pancreatic pathology, as well as the following pancreatic ductal adenocarcinoma risk groups: Mucinous cystic lesions, hereditary risk, and new-late onset diabetes mellitus. Red dashed lines in each histogram depict the start of the fluorescein isothiocyanate (FITC)-positive gate (anti-immunoglobulin G) Alexa Fluor 488), which was determined for each patient separately by considering FITC+approximately 1% on control-secondary-but maintained between control and GPC1 samples. GPC1: Glypican-1; FITC: Fluorescein isothiocyanate; crExos:Circulating exosomes.
Doppler, elastography, and contrast-enhanced EUS image acquisition (sulphur hexafluoride microbubbles; SonoVue®, Bracco, Italy) were used for assistance in the characterization of mural nodules and thickened cyst walls.
EUS-FNA was performed in almost all cystic lesions, preferably with a 22 G needle (Wilson-Cook Medical, Winston, NC, United States and Boston Scientific, Natick MA, United States) in a single pass,and along with antibiotic prophylaxis (single intravenous infusion of 200 mg ciprofloxacin). The fluid collected was sent for amylase, glucose, and CEA quantification, and also, if in enough volume, for cytological examination. Solid or indeterminate lesions, mural nodules, or suspicious thickenings of the cyst wall or septa were punctured in a distinct pass, preferably with a 22 G fine needle biopsy. Adverse events related to EUS procedures were registered and monitored.
Microscopic examinations of specimens resulting from EUS-FNA/B and/or surgical resection were analyzed by experienced pathologists in pancreatic diseases and contextualized to patients’ clinical history and imaging findings. Cytological evaluation was performed according to the Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology[37].
Collection of human blood samples
At the same time of EUS performance, blood samples were collected at the Department of Gastroenterology of CHUSJ. Serum samples were obtained by centrifugation of the whole blood sample at 2000 g for 10 min at 4 °C and collection of the supernatant. The resultant serum samples were then aliquoted and stored at -80 °C prior to analysis.
Isolation of exosomes by ultracentrifugation of serum samples and nanoparticle tracking analysis
Human serum samples were allowed to thaw on ice with periodic agitation to avoid degradation. A volume of 200 μL serum was retrieved into a new tube and centrifuged at 10000 rpm for 2 min at 4 °C.The recovered supernatant was diluted in 200 μL NaCl prior to filtration into 14 mL Open-Top Thinwall Ultra-Clear Tubes (Beckman Coulter, Inc., Brea, CA, United States) using a 0.2 μm pore filter (Whatman International Ltd., England, United Kingdom). The tubes were filled with NaCl, and the samples were ultracentrifuged at 100000 g overnight at 4 °C. The next day, the supernatant was carefully and thoroughly discarded and the exosomes’ pellet was resuspended in 300 μL of 1 × phosphate-buffered saline (PBS). To determine particle concentration and size distribution, nanoparticle tracking (NTA)(NanoSight NS300) was performed using 10 μL of the exosomes sample dissolved in 1 × PBS at a 1:100 dilution. The remaining exosomes sample was saved at -20 °C for downstream analysis.
GPC1 analysis by FACS of exosomes coupled to beads
Using the exosomes concentration previously obtained by NTA analysis as a reference, an equal number of exosomes was used for downstream FACS analysis. A total of 3.0 × 109exosomes were coupled to 4 μm aldehyde/sulfate latex beads (A37304; Thermo Fisher Scientific, Waltham, MA, United States) that had been previously equilibrated at room temperature (through resuspension of 5 μL beads in 100 μL of 1 × PBS and rotation at room temperature for 15 min). The sample volume was adjusted to 300 μL with 1 × PBS. Upon incubation in a rotator at room temperature for 15 min and then at 4 °C for 30 min to allow the formation of exosomes-bead complexes, 300 μL glycine 1 M in 1 × PBS was added to the sample, followed by incubation at room temperature for 1 h with continuous rotation. Samples were centrifuged at 12000 rpm for 2 min and the supernatant was discarded. The pellet containing the exosomes-bead complexes was subjected to a blocking step with 100 μL of 10% bovine serum albumin(BSA) in 1 × PBS and then incubated with continuous rotation at room temperature for 45 min. The samples were centrifuged at 12000 rpm for 2 min and divided into two tubes: Control and GPC1-incubated samples. Control samples were incubated with a solution of 2% BSA in 1 × PBS, whereas experimental samples were incubated with anti-GPC1 (1:240 dilution in a solution of 2% BSA in 1 × PBS,MAB8351; Abnova, Taipei, Taiwan) overnight in a rotator at 4 °C. The next morning, the samples were spun at 12000 rpm for 2 min and the pellet was washed twice with 2% BSA in 1 × PBS, with centrifugation at 12000 rpm for 2 min between washes. Following incubation with an Alexa-488-tagged secondary antibody (anti-mouse A-21202; Thermo Fisher Scientific) for 30 min with continuous rotation at room temperature of both control and experimental samples, samples were washed again twice with 2% BSA in 1 × PBS. Finally, samples were resuspended in 300 μL of 2% BSA in 1 × PBS for BD Accuri C6 or BD FACS Canto II analysis (BD Biosciences, Haryana, IN, United States). Using the control samples of each patient (i.e.exosomes-bead complexes from each patient only incubated with secondary antibody)as a reference, the fluorescein isothiocyanate (FITC) voltage was adjusted until the percentage of FITC+beads was 1%. Then, using the same gate and FITC voltage, the percentage of beads bound with GPC1+crExos in the experimental sample was determined for each patient separately. Data were analyzed using FlowJo software.
Statistical analyses
Categorical variables are described as absolute and relative frequencies and continuous variables as mean and standard deviation, median, percentiles, minimum, and maximum. Hypotheses were tested regarding the distribution of continuous variablesviathe independent samplest-test/one-way analysis of variance (ANOVA) or nonparametric Mann-Whitney and Kruskal-Wallis test depending on normal or non-normal distribution, respectively, and considering the nature of the hypothesis. The chi-squared and ANOVA tests were used for categorical variables analysis. Pearson's correlation coefficient was used to assess the statistical relationship/association between two continuous variables. The diagnostic accuracy of GPC1+crExos was assessed by receiver operating characteristic curve (ROC) considering 95% confidence intervals. Area under the ROC curve (AUROC) was calculated. SPSS®27.0 (IBM Corp.,Armonk, NY, United States) version was used. All graphs were created using GraphPad Prism 7.00(GraphPad Software, San Diego, CA, United States). The statistical review of the study was performed by a biomedical statistician.
RESULTS
Population demographic characteristics
The baseline demographic characteristics of the 88 individuals included in the study (40 MCL, 20 HR, 20 NLOD, and 8 CG) are summarized in Table 1. The overall female:male ratio was 1.6:1 and did not differ statistically among groups. The mean age of the population was 60.3 ± 12.6 years. The older individuals belonged to the MCL group, with a median age of 67.2 ± 8.9 years, whereas the younger individuals were in the HR group, with a median age of 48.7 ± 10.8 years (P< 0.001). Patients in the NLOD group presented with a significantly higher BMI (29.9 ± 4.5 kg/m2;P< 0.001).
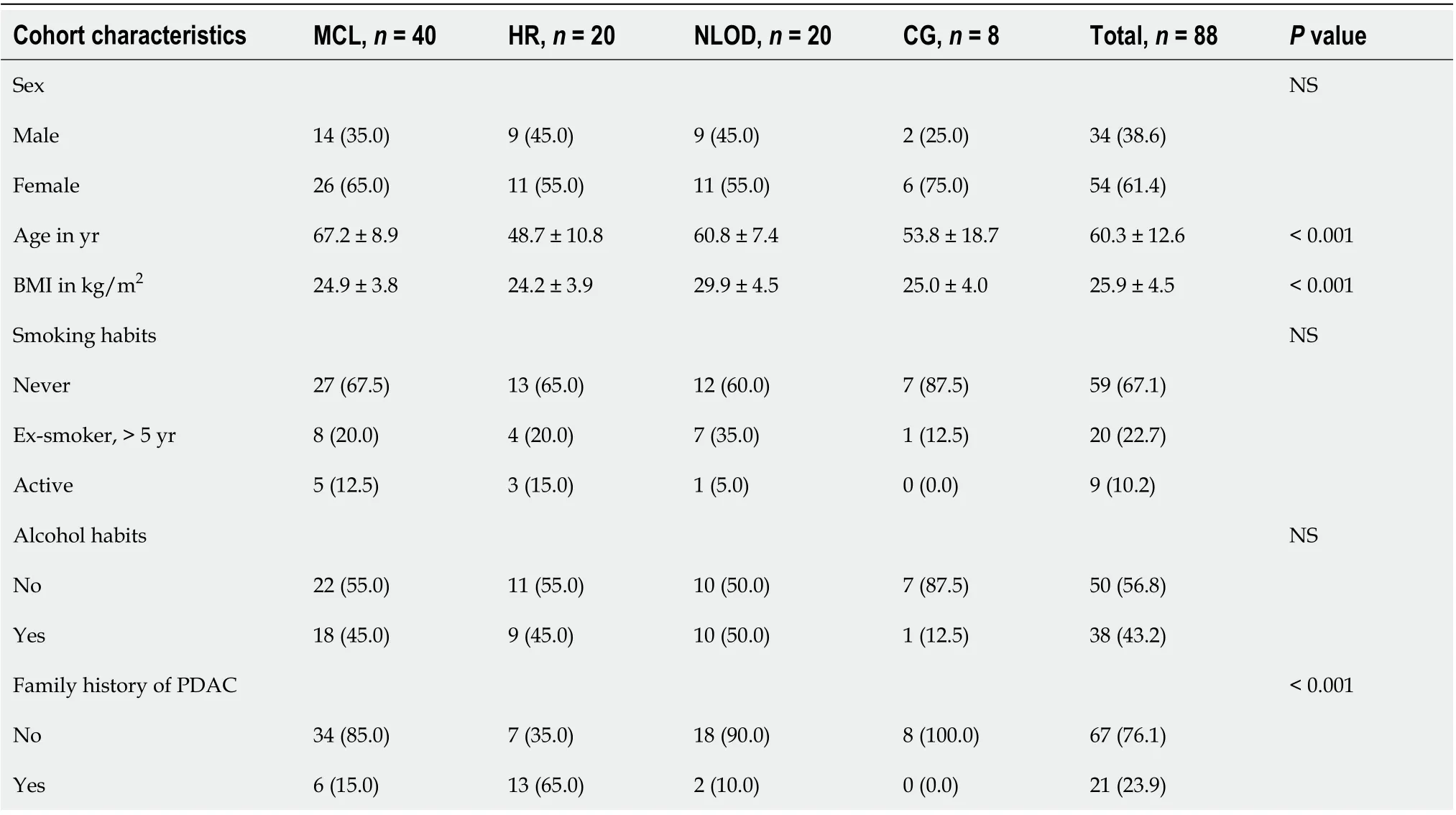
Table 1 Baseline demographic characteristics of the study population, n = 88
No statistically significant differences were observed in relation to smoking or drinking habits among the studied groups. Overall, 10.2% of the population were active smokers and 22.7% ex-smokers (more than 5 years of abstinence). In relation to alcohol consumption, 43.2% were considered active drinkers(average ingesting amounts of > 30 g or > 40 g alcoholperday, in case of female or male individuals,respectively).
Family history of PDAC was present in 23.9% of the entire population, with the highest proportion observed in the HR group (65.0%;P< 0.001). In the HR group, 17 (85.0%) individuals were diagnosed with Lynch Syndrome, 1 (5.0%) with Peutz-Jeghers syndrome, and the remaining 2 (10%) with FPC. Six individuals with Lynch Syndrome had a previous personal history of cancer, mostly colorectal (n= 5),but all were disease-free at the time of inclusion. Detailed information about this group, including the type of harbored mutation(s), can be found in Table 2. In the NLOD group, the mean time between inclusion in the study and establishment of DM diagnosis was 20.9 ± 8.6 mo.
EUS findings and other clinicopathological features
Main PA detected by EUS is illustrated in Figure 2A-F and constituted cystic lesions (with or without WF/HRS), CP-like parenchymal changes, and lipomatous transformation of pancreatic parenchyma.The EUS features of cystic lesions in the MCL group are described in Table 3. Of the 40 cases included,39 (97.5%) were IPMNs, and most (89.8%) were classified as BD-IPMNs. Sixty percent of patients presented with multiple cysts, with a mean size of the dominant lesion of 28.1 ± 14.1 mm. In respect to WF and/or HRS, mural nodules, wall thickening, and a dilated MPD were identified in 10%, 7.5%, and 15% of the lesions, respectively. Nineteen of the forty MCL patients (47.5%) underwent additional study with MRCP.
The clinicopathological characteristics of the study population, particularly the type of PA found in EUS among the different groups, the results of EUS-guided tissue acquisition, surgical treatment and specimen analysis, as well as information on cancer detection during follow-up and mortality rate, are summarized in Table 4. Besides the MCL group, where PA in the form of cyst(s) were present in all patients by definition, PA were also detected during the EUS exam in 10.0% and 35.0% of the subjects belonging to HR and NLOD groups, respectively. Half of the lesions in the MCL group were considered to harbor WF or HRS, in contrast to the PA found in the other groups that were all “harmless” in terms of ultrasonographic appearance (CP-like parenchymal changes, lipomatous transformation and infracentimetric simple cystic lesions). EUS-FNA/B was performed only in the MCL group in 35 of the 40 patients (87.5%), either to confirm the diagnosis or in the presence of WF or HRS (Figure 2G and H).Malignancy was detected in 3 patients; in 1, the malignancy was detected in a subsequent EUS exam performed during follow-up (this case was previously reported by our team[38]). The result of cytological exam was considered inconclusive in 37.1% of the procedures. Of the 88 patients of thecohort, 15 (17.0%) were submitted to surgical resection, and all belonged to the MCL group. These 15 patients either harbored MD or MT-IPMNs or presented a cyst with WF/HRS with suspicious or positive cytology. Malignancy was confirmed in the surgical specimen in all 3 patients with a previous positive cytological exam, and the remaining 12 had a definitive histopathological diagnosis of a low grade dysplastic MCL.

Table 2 Characterization of hereditary risk group: Germline mutations and personal history of cancer, n = 20

Table 3 Endoscopic ultrasound features of cystic lesions among the mucinous cystic lesions group, n = 40
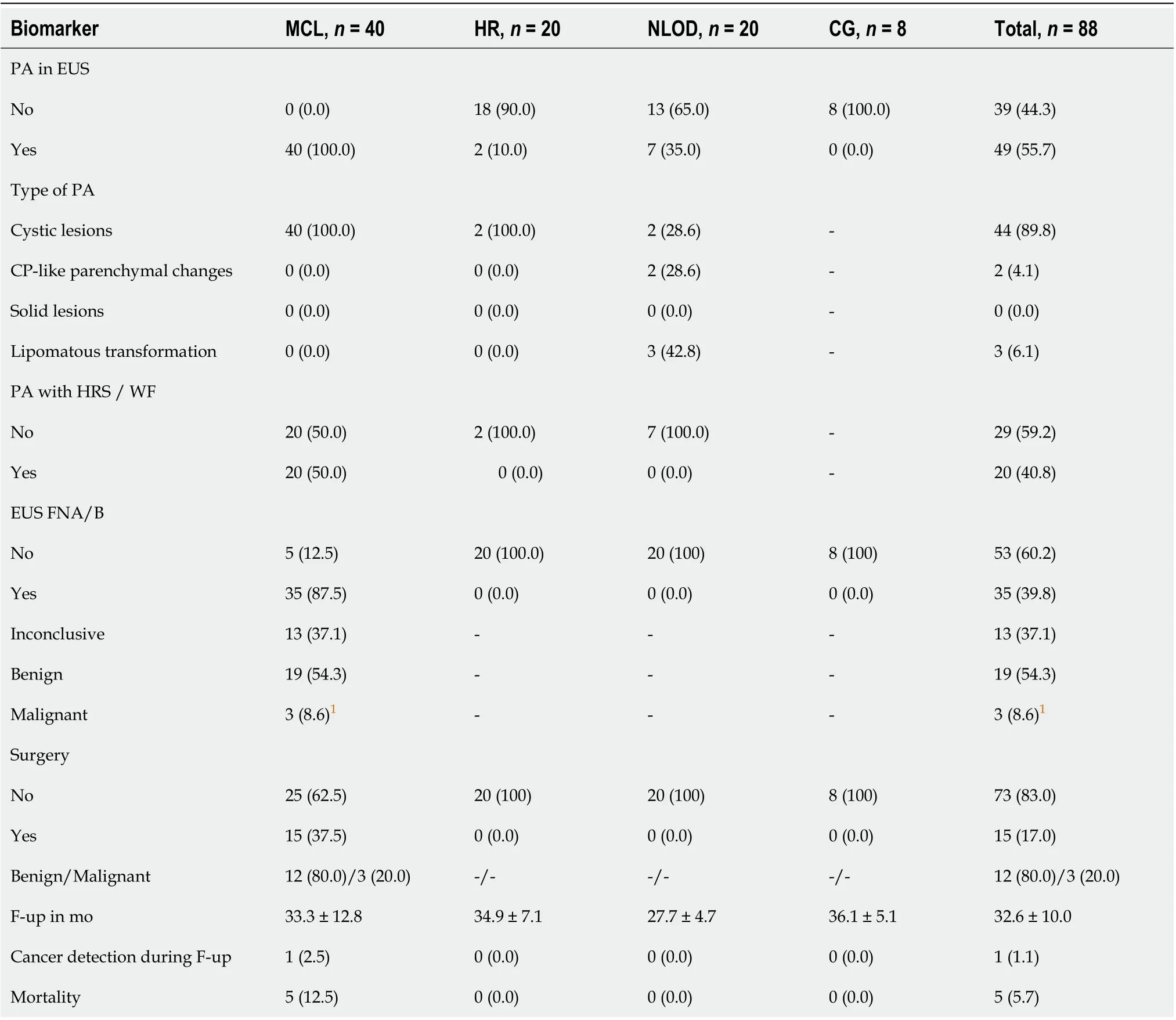
Table 4 Clinical-pathological findings, treatment and follow-up of the study population, n = 88
The mean follow-up period of the entire cohort was 32 ± 8.6 mo and did not differ statistically among groups (P= NS). Five of the 88 individuals (5.7%) died during follow-up, but only one of these due to cancer progression. Two of the other deaths were related to post-operative complications in a 74-yearold and 75-year-old patients, one was related to a pulmonary carcinoma that developed 1 year after inclusion in a 72-year-old patient, and the remaining one corresponded to an 85-year-old patient that did not survive to an infectious respiratory insufficiency. The 2 other patients submitted to surgical resection of malignant cysts were alive and disease-free after 45 mo of follow-up.
Exosomal GPC1 levels are elevated in MCL lesions with WF/HRS and HR groups
The overall median levels of GPC1+crExos coupled to beads were statistically different among the studied groups: MCL [99.4%, interquartile range (IQR): 94.9%-99.8%], HR (82.0%, IQR: 28.9%-98.2%),and NLOD and CG groups (12.6%, IQR: 5.2%-63.4% and 16.2%, IQR: 6.6%-20.1%, respectively) (P<0.0001) (Figure 3A and Table 5).
The crExos concentration and their median size were significantly higher in NLOD patients(6.05E+10/mL; IQR: 4.83-7.22 and 100.7 nm; IQR: 89.2-110.1, respectively) compared to all other groups (P< 0.001 andP= 0.012, respectively) (Figure 3B and C and Table 6).
In turn, overall median levels of CA 19-9 were 18.4 U/mL (IQR: 8.3-206) and did not differ statistically between groups: MCL: 20.4 U/mL (IQR: 14.0-35.8), HR: 16.9 U/mL (IQR: 11.7-18.1), NLOD: 18.8U/mL (IQR: 12.8-48.7) and CG: 30.6 U/mL (IQR: 13.7-69.6)(P=NS) (Figure 3D and Table 5). All CA 19-9 median levels were considered in the normal range considering the clinical standard cut-off (37 U/mL).
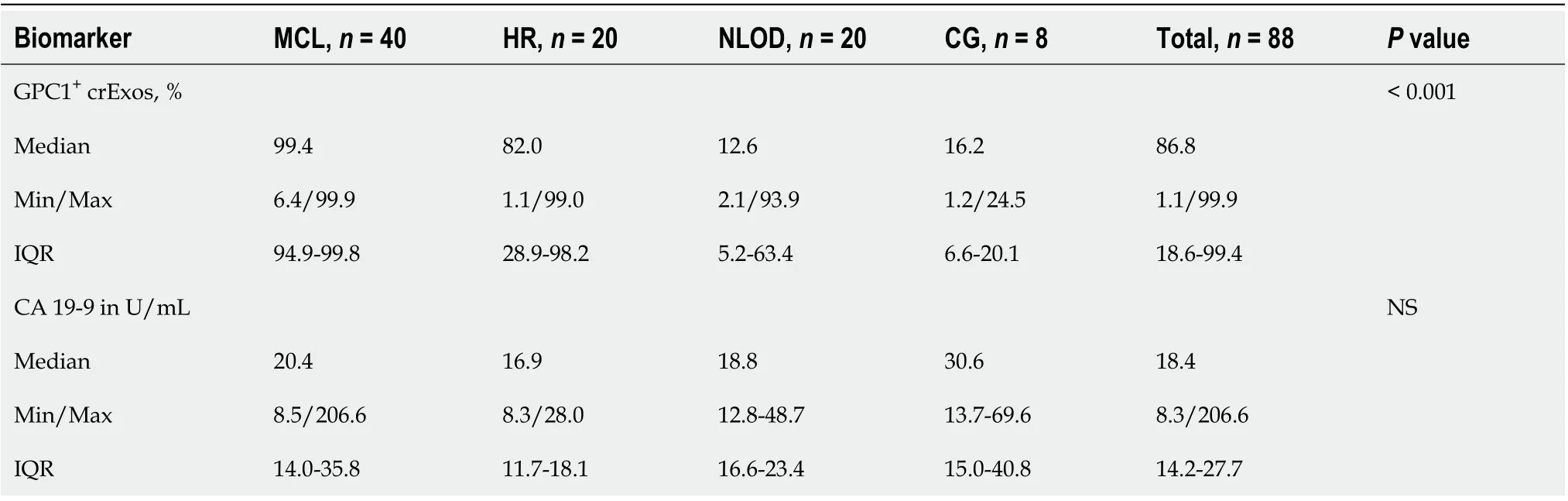
Table 5 Biomarkers (glypican-1-positive circulating exosomes and carbohydrate antigen 19-9) profiles in the study groups, n = 88

Table 6 Size and concentration of exosomes according to the study groups, n = 88
We further investigated the profile of both biomarkers in a sub-analysis in two distinct settings. First,among the HR group, we evaluated GPC1+crExos and CA 19-9 levels according to the presence or absence of personal cancer history (Figure 4A and B). In the individuals with a positive history of cancer(5 colorectal and 1 cancer of the endometrium), although not statistically significant, we observed higher median levels of GPC1+crExos (97.9%; IQR: 61.7%-99.5%) compared to those with a negative history (n= 14) (59.7%; IQR: 26.3%-96.4%) (P= 0.21). In relation to CA 19-9 median levels, they did not differ among these two subgroups (17.5 U/mL; IQR: 10.7%-20.1% and 16.3 U/mL; IQR: 12.2%-19.5%,respectively) (P= NS).
Second, in the total number of patients harboring pancreatic cystic lesions (40 in the MCL group, 2 diagnosed in the HR group, and 2 in the NLOD group), we studied the levels of GPC1+crExos and CA 19-9 according to the presence or absence of WF/HRS in the EUS examination (Figure 4C and D). When WF or HRS were present (n= 20), patients presented with statistically significant higher median levels of GPC1+crExos (99.6%; IQR: 97.6%-99.8%) compared to those with endosonographic “harmless”lesions (n= 24) (96.5%; IQR: 81.3%-99.5%) (P= 0.011) (Figure 4C). The levels of GPC1+crExos presented an AUROC value of 0.723 in differentiating the group of cystic lesions with WF/HRS from those without (sensitivity 75.0% and specificity 67.7% for a cut-off of 98.5% (P= 0.012) (Figure 4E). CA 19-9 median levels did not statistically differ between these two subgroups (22.9 U/mL; IQR: 14.1-35.8 and 17.4 U/mL; IQR: 13.7-29.8, respectively)(P=NS) (Figure 4D).
DlSCUSSlON

Figure 2 Pancreatic abnormalities in endoscopy ultrasound examination and pathological exams of endoscopic ultrasound-guided fine needle aspiration/biopsy specimens from intraductal papillary mucinous neoplasms.A: Main-duct intraductal papillary mucinous neoplasm (MDIPMN) with a large mural nodule, visualized in B-mode (right panel) and characterized with qualitative elastography (left panel) that revealed areas of hard consistency (blue color); B: Endoscopic ultrasound-guided fine needle biopsy with a 22 G needle targeting the harder lesions in the described mural nodule(pathological exam showed malignant degeneration); C: Complex septate cyst with areas of wall focal thickenings and a mural nodule (green arrow); D: Simple bilobulated cyst without worrisome features or high-risk stigmata; E: Chronic pancreatitis-like parenchymal changes (lobulation, hyperechoic foci, and strands); F:Homogenous hyperechogenic appearance of pancreatic parenchyma suggestive of lipomatous transformation; G: Branch-duct IPMN with low-grade dysplasia[hematoxylin and eosin (H&E)-stained cellblock]. These images show the wall of a cystic lesion, partly lined by a cylindrical mucosecretory epithelium with low-grade atypia (left: 100 ×; right: 200 ×); H: Well-differentiated adenocarcinoma originated in a MD-IPMN (H&E-stained cellblock: 400 ×). These images show an epithelial neoplasm with marked architectural disorganization and severe cytological atypia. The cells have a high nucleus-cytoplasmic ratio, with anisokaryosis, irregular nuclei with coarse chromatin and some with an exuberant nucleolus.

Figure 3 Glypican-1-positive circulating exosomes levels are different among the studied groups, whereas the levels of carbohydrate antigen 19-9 do not differ and are within the normal range in the entire population. A: Scatter dot plot representing the percentage of beads bound to glypican-1-positive exosomes (GPC1+ crExos) in the control group (CG) (n = 8), mucinous cystic lesions (MCLs) (n = 40), hereditary risk (HR) (n = 20) and new-late onset diabetes mellitus (NLOD) (n = 20), (Mann-Whitney U Test, aP < 0.02, bP = 0.005, cP < 0.001); B: Scatter dot plot representing exosomes concentration measured by nanoparticle tracking analysis depicting the number of exosomes/0.666 mL serum derived from CG (n = 8), MCL (n = 40), HR (n = 20), and NLOD (n =20) donors (Mann-Whitney U Test, bP = 0.005, cP < 0.001); C: Scatter dot plot representing exosomes mode size distribution determined by nanoparticle tracking analysis from CG (n = 8), MCL (n = 40), HR (n = 20), and NLOD (n = 20) donors (Mann-Whitney U Test, dP = 0.018, eP = 0.04); D: Scatter dot plot representing the serum carbohydrate antigen 19-9 concentration (U/mL) as determined by enzyme-linked immunoassay in CG (n = 8), MCL (n = 40), HR (n = 20), and NLOD (n = 20),(Kruskal-Wallis Test, P = NS). Data are shown as the median ± interquartile range. NS: Non-significant; GPC1: Glypican-1; CA 19-9: Carbohydrate antigen 19-9;crExos: Circulating exosomes.
MCLs are established as PDAC precursor lesions, with different risks considering morphologic appearance as well as cytological findings resulting from guided tissue acquisition. While the diagnostic and management of pancreatic cysts differs between international guidelines[29,39-42], they all agree that the risk of malignancy should be based, essentially, in the assessment of the classical WF/HRS,which was initially defined in the Fukuoka consensus[43].
Our cohort mainly constituted IPMNs, most of which were BD-IPMN type and half of the lesions presented with WF and/or HRS[29]. Malignancy was suspected by EUS in two advanced lesions with main duct involvement, which were confirmed by cytology. Interestingly, the third confirmed malignant cyst corresponded to a case we have previously reported[38], and was diagnosed during a follow-up examination of an apparently “inoffensive” cystic lesion in the index EUS. Our results have confirmed the limited utility of the use of cytology alone for cyst etiological characterization[44,45], as 37% of the results of EUS-FNA of the cyst fluid were considered inconclusive by pathologists. This limitation of cyst fluid cytological analysis tends to be overwhelmed by the referral for surgical resection of indeterminate suspicious lesions. In fact, 15 of the 40 patients with MCL proposed for surgical treatment, after evaluation by a multidisciplinary team, corresponded to 3 cases with a positive cytology for malignancy and 12 patients with indeterminate/inconclusive results of EUS-FNA. The surgical specimen confirmed malignancy in all 3 cases with previous diagnosis and in the remaining 12 revealed benign IPMNs with low grade dysplasia. The overtreatment of some of these patients is an important issue, as the morbidity and mortality of pancreatic surgery is not negligible[46,47]. In the present cohort,2 of the 5 deaths recorded were precisely due to complications after surgery, both in patients harboring benign lesions. This observation supports the drive of research, justifying the need to evaluate the role of upcoming biomarkers, like exosomal GPC1, in complement with EUS evaluation, for the stratification of MCL, ultimately contributing to refine the criteria for surgical treatment or continued surveillance. In this setting, our preliminary results initially reported were promising, as the levels of GPC1+crExos were equally elevated in patients with PDAC and with MCLs[48,49]. The findings in the present study confirm these observations, as the median levels of GPC1+crExos observed in the MCL group(significantly higher than in the other studied groups) were in the same magnitude as the ones registered for PDAC patients, that we have recently reported using the same methodology[28].Moreover, when we analyzed the levels GPC1+crExos among all pancreatic cystic lesions (MCL group plus those detected in the screening EUS in HR and NLOD groups), we found that they were statistically more elevated when WF/HRS were present, suggesting that this biomarker can, in fact, have a role in the risk stratification of these PDAC precursor lesions.

Figure 4 Glypican-1-positive circulating exosomes are higher in individuals with personal history of cancer within the hereditary risk group, and among patients harboring pancreatic cystic lesions when worrisome features/high-risk stigmata are present. A: Scatter dot plot representing the percentage of beads bound to glypican-1 (GPC1)-positive circulating exosomes (GPC1+ crExos) in subjects in the hereditary risk (HR) group, without(n = 14) and with (n = 6) a personal history of cancer (HxCancer) [Mann-Whitney U Test, P = non-significant (NS)]; B: Scatter dot plot representing the serum carbohydrate antigen 19-9 (CA 19-9) concentration (U/mL) as determined by enzyme-linked immunoassay (ELISA) in subjects in the HR group, without (n = 14) and with (n = 6) HxCancer (Mann-Whitney U Test, P = 0.21); C: Scatter dot plot representing the percentage of GPC1+ crExos coupled to beads in subjects harboring pancreatic cystic lesions, without (n = 24) and with (n = 20) worrisome features (WF) or high-risk stigmata (HRS) (Mann-Whitney U Test, fP = 0.011); D: Scatter dot plot representing the serum CA 19-9 concentration (U/mL) as determined by ELISA in subjects harboring pancreatic cystic lesions, without (n = 24) and with (n = 20)WF/HRS (Mann-Whitney U Test, P = NS); E: Receiver operating characteristic curve of the cohort of pancreatic cystic lesions without (n = 24) or with (n = 20)WF/HRS, regarding the GPC1+ crExos levels (% beads with GPC1+ crExos). 1Under nonparametric assumption; 2Null hypothesis: True area = 0.5. Data are shown as the median ± interquartile range. NS: Non-significant; GPC1: Glypican-1; crExos: Circulating exosomes; WF: Worrisome features; HRS: High-risk stigmata.
This is the first study to access the profile of GPC1+crExos in HR and NLOD individuals, and our results showed that the median levels of this biomarker were statistically more elevated among the HR group when compared to NLOD patients and controls. Considering our previous published observations[28], these levels of GPC1+crExos in HR individuals were also higher than those registered among patients with CP (28.4%), but not as elevated as in those with PDAC (99.7%). Interestingly, our results also showed a tendency of the individuals with a history of previous cancer (mainly colorectal)to present higher levels of GPC1+crExos when compared to those without. While PA were detected in only 10% among HR individuals, all representing simple cystic lesions, these observations may suggest a potential role of GPC1+crExos as a marker of genetically determined predisposition for cancer development, even in the absence of “harmful” pancreatic lesions.
Important studies have recently been published[24-26] and prospective investigational projects are ongoing[50] demonstrating the importance to access the magnitude of the risk to develop PDAC among NLOD patients and to define PDAC incidence during long-term follow-up. This justified the inclusion of NLOD patients in our investigation cohort. We found PA in EUS in 35% of the NLOD patients,comprising simple cystic lesions, CP-like changes and lipomatous parenchymal transformations, all of them considered “harmless”, not requiring further investigation. Despite the highest median values of exosomes’ size and particle concentration being registered in this group, the percentage of crExos positive for GPC1 was low and not statistically different from the CG. This finding is in accordance with the lack of sufficient evidence, at the present, to include these patients in regular screening programs for PDAC early detection.
Some limitations of this study should be pointed out, namely the sample size, the possibility of a referral bias giving the nature of our tertiary center, the relatively short period of patients’ follow-up,and the cut-off found to stratify patients with cystic lesions and WF/HRS from those without. Also, the impossibility to include PanIN lesions in the study that would certainly power the analysis of GPC1 profile among PDAC pathological precursors. Lastly, the technique of exosomes isolation and analysis can still hamper its translation to clinical use. Despite these restraints, our results open the door for future studies to determine the value of this biomarker in the stratification of risk groups.
CONCLUSlON
In summary, we demonstrate that GPC1+crExos levels are elevated in MCL, in the same magnitude of PDAC patients. These levels were statistically higher in cysts harboring WF/HRS. High levels were also registered among individuals with HR for PDAC (predominantly in those with history of previous cancer). Longitudinal studies will clarify the potential of exosomal GPC1 as a biomarker for the diagnosis and stratification of PDAC precursor lesions, as well as in signaling individuals with genetic predisposition for this neoplasia, ultimately contributing to refine screening and surveillance strategies.
ARTlCLE HlGHLlGHTS

Research conclusions
Our study supports the role of GPC1+crExos in the diagnosis and stratification of PDAC precursor lesions, namely MCL, and its eventual capacity in signaling individuals with genetic predisposition for this neoplasia, even when no harmful PA are detected by EUS.
Research perspectives
Our data encourage longitudinal studies to confirm the potential of exosomal GPC1 as a biomarker to be used in the future in the management of individuals at risk for PDAC.
ACKNOWLEDGEMENTS
The authors acknowledge the support of the Translational Cytometry i3S Scientific Platform and the collaboration of Catarina Meireles MD, Elvira Sampaio MD, Liliana Silva MD and Mariana Santos MD in patient management.
FOOTNOTES
Author contributions:Moutinho-Ribeiro P was the main project investigator, was responsible for patient selection and sample collection, performed pancreatic endoscopic ultrasound, and wrote the initial manuscript; Batista IA participated in the sample processing, supervised and collected the data, performed the data analyses, and supported the manuscript writing; Quintas ST participated in the sample processing, data collection and analyses, assembled the figures, and supported the manuscript writing; Adem B participated in the sample processing and supported the data analyses; Silva M participated in the data collection and performed the statistical analyses; Morais R, Peixoto A,Coelho R, Costa-Moreira P, and Medas R participated in patient observation, data collection, and database management; Medas R performed the statistical analyses; Lopes S and Vilas-Boas F performed the pancreatic endoscopic ultrasound; Baptista M, Dias-Silva D, Esteves AL, and Martins F participated in patient observation and data collection; Lopes J, Barroca H, and Carneiro F performed the cytological and histological examination of the pancreatic specimens; Macedo G conceived and designed the study, interpreted the data analyses, and critically reviewed the manuscript; Melo SA conceived and designed the study, supervised the data analyses, and critically reviewed the manuscript; All authors approved the final version to be published.
Supported byGuilherme Macedo team was supported by the Portuguese Society of Digestive Endoscopy (SPED)2017 Research Grant, No. SG/CHSJ-A2017; Norte Portugal Regional Programme (NORTE 2020) under the PORTUGAL 2020 Partnership Agreement through the European Regional Development Fund (ERDF) to Sonia A Melo, No. NORTE-01-0145-FEDER-000029; National Funds through Foundation for Science and Technology (FCT) to Sonia A Melo, No. POCI-01-0145-FEDER-32189; and Foundation for Science and Technology (FCT) to Bárbara Adem and Ines A Batista, No. PD/BD/135546/2018 and No. SFRH/BD/144854/2019.
lnstitutional review board statement:This study was reviewed and approved by the Ethics Committee ofCentro Hospitalar Universitário de São João(CHUSJ), Porto, Portugal, No. CES 327-15.
lnformed consent statement:All study participants or their legal guardian provided informed written consent about personal and medical data collection prior to study enrolment.
Conflict-of-interest statement:Sónia A Melo holds patents in the field of exosomes biology and are licensed to Codiak Biosciences, Inc. All other authors have no conflicts of interest to declare.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Portugal
ORClD number:Pedro Moutinho-Ribeiro 0000-0002-4782-6489; Ines A Batista 0000-0003-0321-7902; Sofia T Quintas 0000-0002-4190-3527; Bárbara Adem 0000-0003-0398-1185; Marco Silva 0000-0001-8215-1213; Rui Morais 0000-0003-1293-3353;Armando Peixoto 0000-0003-3994-2882; Rosa Coelho 0000-0003-2706-2351; Pedro Costa-Moreira 0000-0003-0981-2497;Renato Medas 0000-0002-1892-2666; Susana Lopes 0000-0002-0407-6016; Filipe Vilas-Boas 0000-0001-7041-0863; Manuela Baptista 0000-0002-4306-769X; Diogo Dias-Silva 0000-0001-7367-6915; Ana L Esteves 0000-0001-8844-7939; Filipa Martins 0000-0002-5753-9811; Joanne Lopes 0000-0002-2339-2823; Helena Barroca 0000-0001-5684-3523; Fátima Carneiro 0000-0002-1964-1006; Guilherme Macedo 0000-0002-9387-9872; Sonia A Melo 0000-0002-2291-4263.
S-Editor:Fan JR
L-Editor:Filipodia
P-Editor:Fan JR
 World Journal of Gastroenterology2022年31期
World Journal of Gastroenterology2022年31期
- World Journal of Gastroenterology的其它文章
- Duodenal-jejunal bypass reduces serum ceramides via inhibiting intestinal bile acid-farnesoid X receptor pathway
- Preoperative contrast-enhanced computed tomography-based radiomics model for overall survival prediction in hepatocellular carcinoma
- Prevalence and clinical characteristics of autoimmune liver disease in hospitalized patients with cirrhosis and acute decompensation in China
- Application of computed tomography-based radiomics in differential diagnosis of adenocarcinoma and squamous cell carcinoma at the esophagogastric junction
- Radiomics and nomogram of magnetic resonance imaging for preoperative prediction of microvascular invasion in small hepatocellular carcinoma
- Insights into induction of the immune response by the hepatitis B vaccine