
Prevalence and clinical characteristics of autoimmune liver disease in hospitalized patients with cirrhosis and acute decompensation in China
2022-08-18 03:15ZiXuanShenDanDanWuJieXiaXianBoWangXinZhengYanHuangBeiLingLiZhongJiMengYanHangGaoZhiPingQianFengLiuXiaoBoLuJiaShangHuaDongYanYuBaoZhengWenYiGuYanZhangJianYiWeiWenTingTanYiXinHouQunZhangYanXiongCongC
World Journal of Gastroenterology 2022年31期
Zi-Xuan Shen, Dan-Dan Wu, Jie Xia, Xian-Bo Wang, Xin Zheng, Yan Huang, Bei-Ling Li, Zhong-Ji Meng, Yan-Hang Gao, Zhi-Ping Qian, Feng Liu, Xiao-Bo Lu, Jia Shang, Hua-Dong Yan, Yu-Bao Zheng, Wen-Yi Gu,YanZhang, Jian-Yi Wei, Wen-Ting Tan, Yi-Xin Hou,Qun Zhang, Yan Xiong, Cong-Cong Zou, Jun Chen, Ze-BingHuang, Xiu-Hua Jiang, Sen Luo, Yuan-Yuan Chen, Na Gao, Chun-Yan Liu, Wei Yuan, Xue Mei, Jing Li, Tao Li,Xin-Yi Zhou, Guo-Hong Deng, Jin-Jun Chen, Xiong Ma,Hai Li
Abstract
Key Words: Prevalence; Autoimmune liver disease; Cirrhosis and acute decompensation; Mortality; Acuteon-chronic liver failure
lNTRODUCTlON
Autoimmune liver disease (AILD) includes primary biliary cirrhosis (PBC), autoimmune hepatitis(AIH), primary sclerosing cholangitis (PSC) and immunoglobulin G 4-related diseases (IgG4-RD)[1-3].Some patients display clinical manifestations of two different entities based on clinical and histological features, which is described as “overlap syndrome”, among which PBC-AIH overlap syndrome(PBC/AIH) is the most common[4]. AILD has been considered to be a relatively rare etiology of chronic liver disease (CLD) in China where viral hepatitis has a high prevalence. However, recent findings indicated that the prevalence of AILD is increasing in the Asia-Pacific region. In Japan, AIH prevalence increased from 8.7 to 23.9 per 100000 population from 2004 to 2016[5]. In a city in northern China, PBC prevalence rose from 0.5 to 8.0 per 100000 population in the past 10 years[6]. Several studies have illustrated the prevalence and clinical characteristics of AILD in general population[7-9]. Few studies have been conducted to investigate the nature history of AILD, especially in the late stage of CLDcirrhosis and acute decompensation (AD).
The Chinese Acute on Chronic Liver Failure (CATCH-LIFE) study consisted of two prospective,multicenter cohorts that enrolled hospitalized patients with CLD of various etiologies, most of whom had cirrhosis and complicated with AD. It is nationally representative of hospitalized CLD patients in China. In this study, we used the data from the CATCH-LIFE study to investigate the following: (1) The prevalence and short-term outcome of AILD in patients with cirrhosis and AD; (2) The impact of AILD etiology on mortality; and (3) Risk factors for 90-d mortality in AILD patients with cirrhosis and AD.
MATERlALS AND METHODS
Patients
Data were collected from 2 prospective, observational cohorts of the CATCH-LIFE study which enrolled hospitalized patients with CLD and acute events, from January 2015 to December 2016 and July 2018 to January 2019, respectively. The rationale and design of the cohorts have been described elsewhere[10,11]. The medical ethics boards of the Shanghai Renji Hospital, approved the study. Written informed consent were obtained from every participant or his or her legal surrogates before enrollment.
Cirrhosis was diagnosed according to a computed tomography/magnetic resonance imaging scan,clinical symptoms, laboratory tests and medical history[12]. AD was defined as ascites, variceal hemorrhage, hepatic encephalopathy (HE), infection and jaundice within 1 mo[13]. The diagnosis of AILD was exclusionary. The following patients were excluded: Coinfections with other viruses[hepatitis A virus, hepatitis B virus (HBV), hepatitis C virus and hepatitis E virus], alcoholic liver disease, nonalcoholic fatty liver disease, schistosomiasis, metabolic liver diseases, chronic drug-induced liver disease, and cryptogenic liver disease.
PBC was defined according to the American Association for the Study of Liver Diseases clinical guidance in 2008[14], with at least 2 of the following: (1) Elevated serum alkaline phosphatase (ALP) [>1.5 folds the upper limit of normal (ULN)] or gamma glutamyl transpeptidase (GGT) (> 3 ULN); (2)Positive test for antimitochondrial antibodies (AMA) (titer > 1:40); and (3) Compatible liver biopsy suggestive of suppurative destructive cholangitis (ductopenia, cholestasis, fibrosis and portal inflammation). AIH was defined based on simplified criteria (score > 6) proposed by the International Autoimmune Hepatitis Group in 2008[15]. PBC/AIH overlap syndrome was strictly diagnosed according to the Paris Criteria proposed by Chazouillèreset al[16] in 1998, which associated PBC and AIH either synchronously or consecutively. Presence of at least 2 of the 3 criteria was required. PBC criteria were the following: (1) ALP > 2 ULN or GGT > 5 ULN; (2) A positive serology for AMA; and (3)A liver biopsy specimen indicating florid bile duct lesions. AIH criteria were the following: (1) Serum alanine transaminase (ALT) > 5 ULN; (2) IgG > 2 ULN or a positive serology for anti-smooth muscle antibodies; and (3) A liver biopsy indicating moderate to severe periportal or periseptal lymphocytic piecemeal interface hepatitis.
Some uncommon etiologies of AILD in this study, such as PSC, PBC-PSC overlap syndrome, AIHPSC overlap syndrome and IgG4-RD were categorized into a “others” group, as the number of cases of“others” was quite small to allow robust statistical analysis. Acute-on-chronic liver failure (ACLF) was diagnosed based on the European Association for the Study of the Liver (EASL) criteria[17]. Just as follows: (1) ACLF grade 1: Single kidney failure or single cerebral failure with renal dysfunction (1.5 mg/dL < creatinine < 1.9 mg/dL) or other single organ failure [serum bilirubin ≥ 12 mg/dL for liver;(international normalized ratio) INR = 2.5 for coagulation; vasopressors to maintain arterial pressure for circulation; PaO2/FiO2≤ 200 or SpO2/FiO2≤ 214 for respiration] with renal dysfunction and/or mild HE;(2) ACLF grade 2: The presence of 2 organ failures; and (3) ACLF grade 3: The failure no less than 3 organs.
Data collection
Demographics, medical history, imagological examination and laboratory parameters were obtained from every participant on admission. Participants were regularly followed up for 28 d, 90 d and 365 d until death or liver transplantation (LT). Development of ACLF was assessed on admission and during hospitalization within 28 d, respectively. The primary outcome of this study was 90-d LT-free mortality.The secondary outcome was ACLF development during 28-d hospitalization.
Statistical analysis
Continuous variables were summarized as mean (SD) or median (interquartile range) according to their distribution, while categorical variables were summarized as frequency (proportion). Comparisons between four groups were performed using Kruskal-Wallis test for continuous variables, Chi-square test or Fisher’s exact test for categorical variables. The impact of the etiology of AILD on short-term mortality were analyzed using a multivariable logistic regression model, adjusting for potential confounders, including demographics (age, sex) and AD events (HE, gastrointestinal bleeding, infection and ascites). Logistic regression was also used to determine the risk factors for 90-d mortality and ACLF development during hospitalization. Variables withPvalues less than 0.1 were included in the multivariate logistic regression model[18,19]. All continuous variables were log2 transformed before entering the model. Two-tailedPvalues of 0.05 were considered statistically significant. Statistical analysis was conducted using R 3.6.2 and SPSS 19.0.
RESULTS
Prevalence of AILD and ACLF in patients with cirrhosis and AD
A total of 3970 patients from CATCH-LIFE study were screened, 2597 of whom had cirrhosis and AD.Eventually, 242 patients conforming the diagnostic criteria of AILD were finally enrolled (Figure 1). In patients with cirrhosis and AD, the overall prevalence of AILD was 9.3% (242/2597). Prevalence of ACLF was significantly lower in AILD cases (14%) than those with all etiology groups with cirrhosis and AD (22.8%) (P< 0.001). Distribution of participating centers in this study and number of AILD patients enrolled from each center were displayed in Figures 2A and 2B, respectively. Among the 242 enrolled AILD patients, 234 (96.6%) are from eastern China, where 94% of Chinese population resides; 8(3.4%) are from western China, where 6% of Chinese population resides. Due to Renji Hospital accounted for 60.3% (146/242) of the total enrolled patients, we further analyzed district distribution of patients enrolled from Renji Hospital. Actually, these patients were from 20 different district all over the country (Figure 2C), the number of patients from each district was shown in Figure 2D. Distribution of patients enrolled from Renji Hospital were also consistent with population density distribution (divided by Hu Line) in China.
Baseline characteristics and outcomes among different etiologies in AILD patients
Baseline characteristics of 242 AILD patients with cirrhosis and AD categorized by etiology are depicted in Table 1. 123 (50.8%) patients showed PBC, 69 (28.5%) displayed AIH, 29 (12.0%) had AIH-PBC overlap syndrome (AIH/PBC) and 21 (8.7%) patients manifested other uncommon etiologies of AILD.Most patients were female (81.0%) and their mean age was 56.04 years. Patients with PBC/AIH had higher white blood cell (P< 0.001) and neutrophil-lymphocyte (NL) ratio (P< 0.001) levels than patients with PBC, AIH or others. ALT (P< 0.001) and AST (P= 0.04) levels were higher in the AIH/PBC group.In addition, the PBC group tended to have lower hemoglobin (P= 0.003) and higher ALP (P< 0.001)levels than other AILD etiologies.
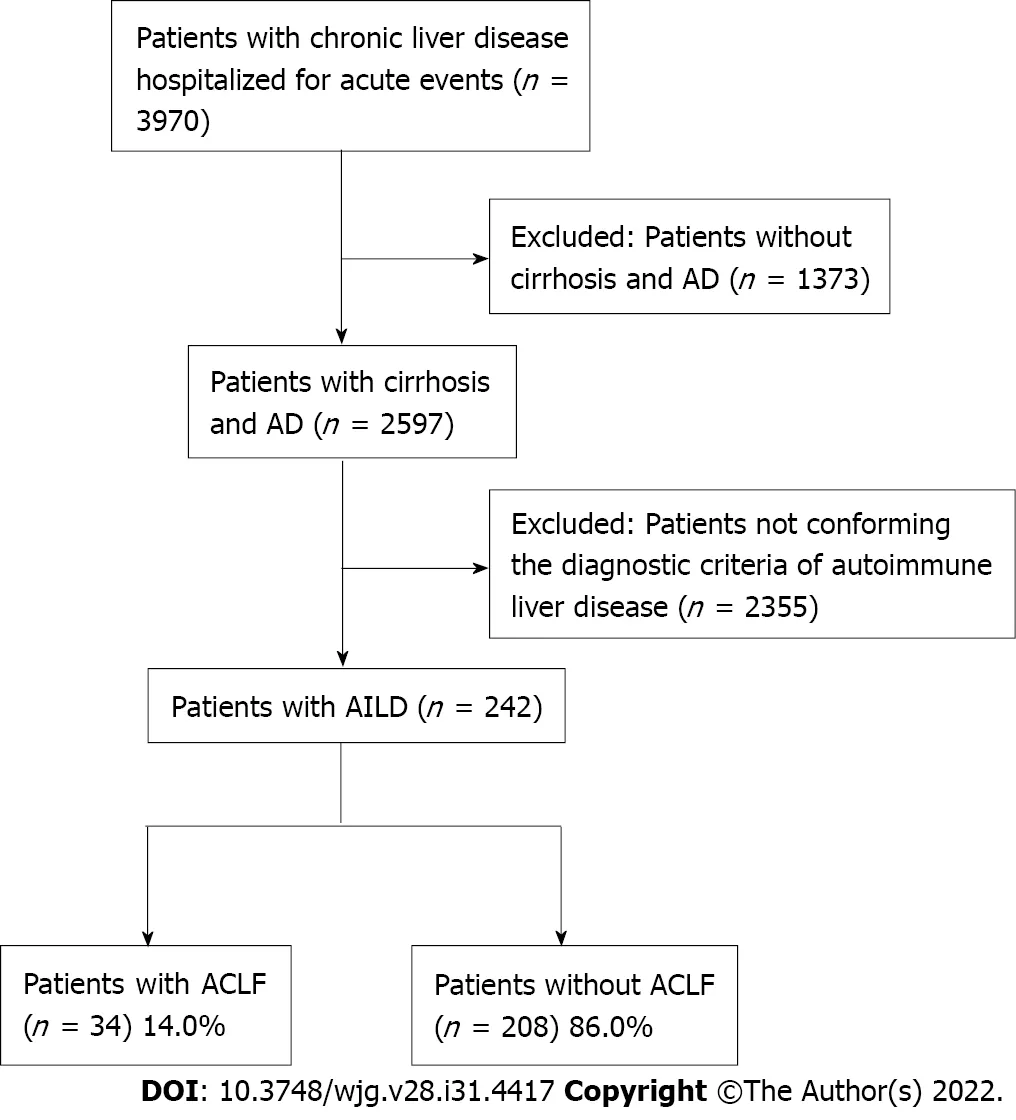
Figure 1 Flow chart of the study. AD: Acute decompensation; AILD: Autoimmune liver disease; ACLF: Acute-on-chronic liver failure.
Baseline characteristics of 34 ACLF patients categorized by etiology are shown in Table 2. PBC(41.2%) was still the most common etiology among ACLF patients with AILD, followed by AIH (29.4%),AIH/PBC overlap syndrome (20.6%) and others (8.8%). However, as the number of patients in some subgroups was small, the results may not be robust and require further validation in a larger population. At the end of 28-d and 90-d, no patients were lost to follow up. At the end of 365-d, 3 (1.2%)patients were lost to follow-up. Short-term (28-d, 90-d and 365-d) LT-free mortality of AILD patients with cirrhosis and AD are presented in Figure 3. Generally, among AILD patients with cirrhosis and AD, 90-d LT-free mortality were 17%. AIH/PBC had higher 28-d, 90-d and 365-d mortality, although the results were not statistically significant. Among patients with AILD-related ACLF, 28-d and 90-d mortality were 43.8% and 80.0%, respectively.
The impact of etiology on mortality
To investigate the effect of etiology on short-term (28-d, 90-d and 365-d) LT-free mortality in AILD patients with cirrhosis and AD, we constructed 3 models to gradually control other potential confounding factors (Table 3). Both univariate (unadjusted) and multivariate (adjusted I and adjusted II)analyses showed that compared to PBC, AIH patients were at lower risk for death at 90-d and 365-d,whereas PBC/AIH patients were at higher risk for death at all time periods. However, none of the associations were statistically significant. Subgroup analysis was conducted according to Child Turcotte Pugh and model for end-stage liver disease (MELD) score, there was no heterogeneity in the impact of etiology types on 90-d LT-free mortality in different AILD subgroups, as was shown in Supplementary Figure 1.
Risk factors of short-term mortality in AILD patients with cirrhosis and AD
Logistic regression model was conducted to assess the risk factors for 90-d LT-free mortality.Univariable analysis identified 10 variables on admission correlated with 90-d prognosis: Bacterial infection, HE, total bilirubin (TB), INR, blood urea nitrogen (BUN), albumin, ALT, white blood cell, NLratio and sodium (Supplementary Table 1). Variables withP< 0.1 were selected into multivariable model for further analysis. Only HE, TB and BUN were found to be independently associated with 90-d mortality in AILD patients with cirrhosis and AD (Figure 4). We also investigated risk factors for ACLF development during hospitalization (Table 4). 21 ACLF patients diagnosed on admission were excluded from analysis. Multivariable analysis revealed that only TB (P= 0.046) and INR (P= 0.048)independently correlated with ACLF development.
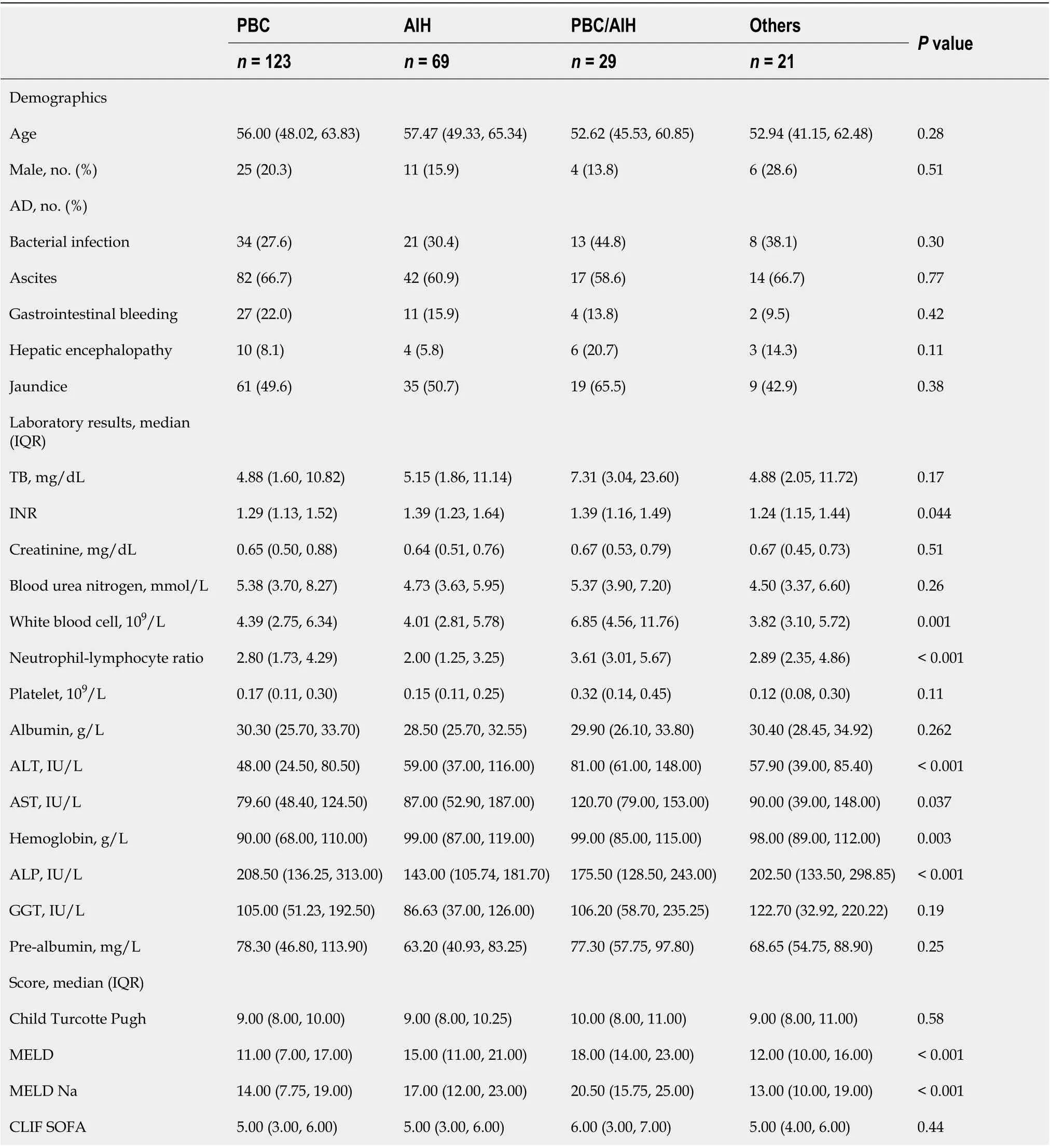
Table 1 Characteristics of autoimmune liver disease patients with cirrhosis and acute decompensation among different etiologies
DlSCUSSlON
The current study is the first nationwide investigation of the prevalence and short-term outcome of endstage AILD in China, which is a traditional HBV high endemic area. Our study showed that the overall prevalence of AILD was 9.3% in tertiary hospitalized patients with cirrhosis and AD. PBC was responsible for half of AILD cases. The prevalence of ACLF was significantly lower in AILD patients than those with all etiology groups with cirrhosis and AD. Short-term mortality were extremely high in AILD-related ACLF.
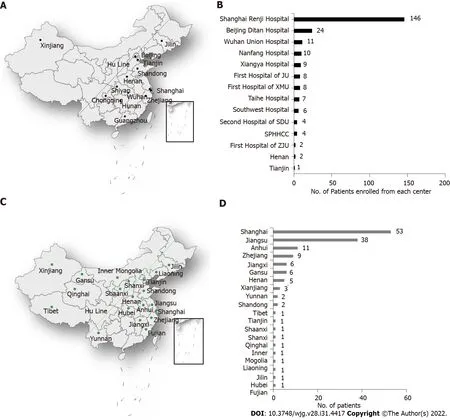
Figure 2 Distribution and the number of autoimmune liver disease patients enrolled from each of center and from Renji Hospital. A: District distribution of each enrolled center; B: The number of patients enrolled from center; C: Population distribution of patients from Renji Hospital; D: The number of patients enrolled from each of the 20 districts. Approximately 94% of the total Chinse population resides east of the dividing line (Hu Line) in the figure, and 6%resides west of the line; 13 centers lie in eastern China, and 1 lies in western China.
EASL-CLIF study reported that the prevalence of ACLF was 30.9% in alcohol-related cirrhosis and AD, whereas COSSH study showed that the prevalence of ACLF reached up to 26.2% in patients with HBV-related cirrhosis and AD[17,20]. However, in this study, among 242 AILD patients with cirrhosis and AD, only 34 (14%) had ACLF, the prevalence was significantly lower than that of patients with other etiology types. One plausible explanation may be that AILD patients have distinct clinical characteristics (higher severity, higher prevalence of infection and lower prevalence of organ failures) that differ distinctly from those of patients with other etiologies, which led to lower prevalence of ACLF but higher short-term mortality.
Despite having higher levels of inflammation and liver injury, PBC/AIH had similar short-term mortality rates compared to PBC individually after adjusting for confounding factors. Neuhauseret al[21] and Yanget al[22] showed that a more aggressive clinical course and worse clinical consequences were observed in patients with PBC/AIH than patients with pure PBC. Based on these results, some experts suggested that PBC/AIH should be identified and aggressively treated. Notably, these studies only evaluate the univariate prognostic value of etiology and did not take confounders into consideration. It is, therefore, likely that they fail to objectively reveal the independent impact of etiology on the prognosis of AILD. PBC, AIH and PBC/AIH are all complex disorders but result in significant morbidity and mortality. Once progressed to liver failure, no effective treatment is clinically available.Herein, our results clearly showed that presence of HE, higher TB and BUN levels, rather than liver disease etiologies, were independently associated with short-term mortality in AILD patients withcirrhosis and AD. Therefore, in clinical management of AILD, physicians are supposed to pay more attention to the presence of HE and closely monitor the changes of liver and renal function.

Table 2 Characteristics of autoimmune liver disease patients with acute-on-chronic liver failure according to etiology
This study had several strengths. With national samples, our multicenter data provided an overview of epidemiological features of end-stage AILD in China, where it is considered uncommon. Thus, we presented a national view of the disease. Indeed, most of the studies in this field originated from single center or other geographic areas[7,23-25]. We focused on the role of the etiology on short-term mortality.Moreover, we clarified that HE, TB and BUN were significant risk factors of short-term mortality in AILD patients with cirrhosis and AD. These data will be an important complement to the public epidemiological data of AILDs in Asian-Pacific regions.
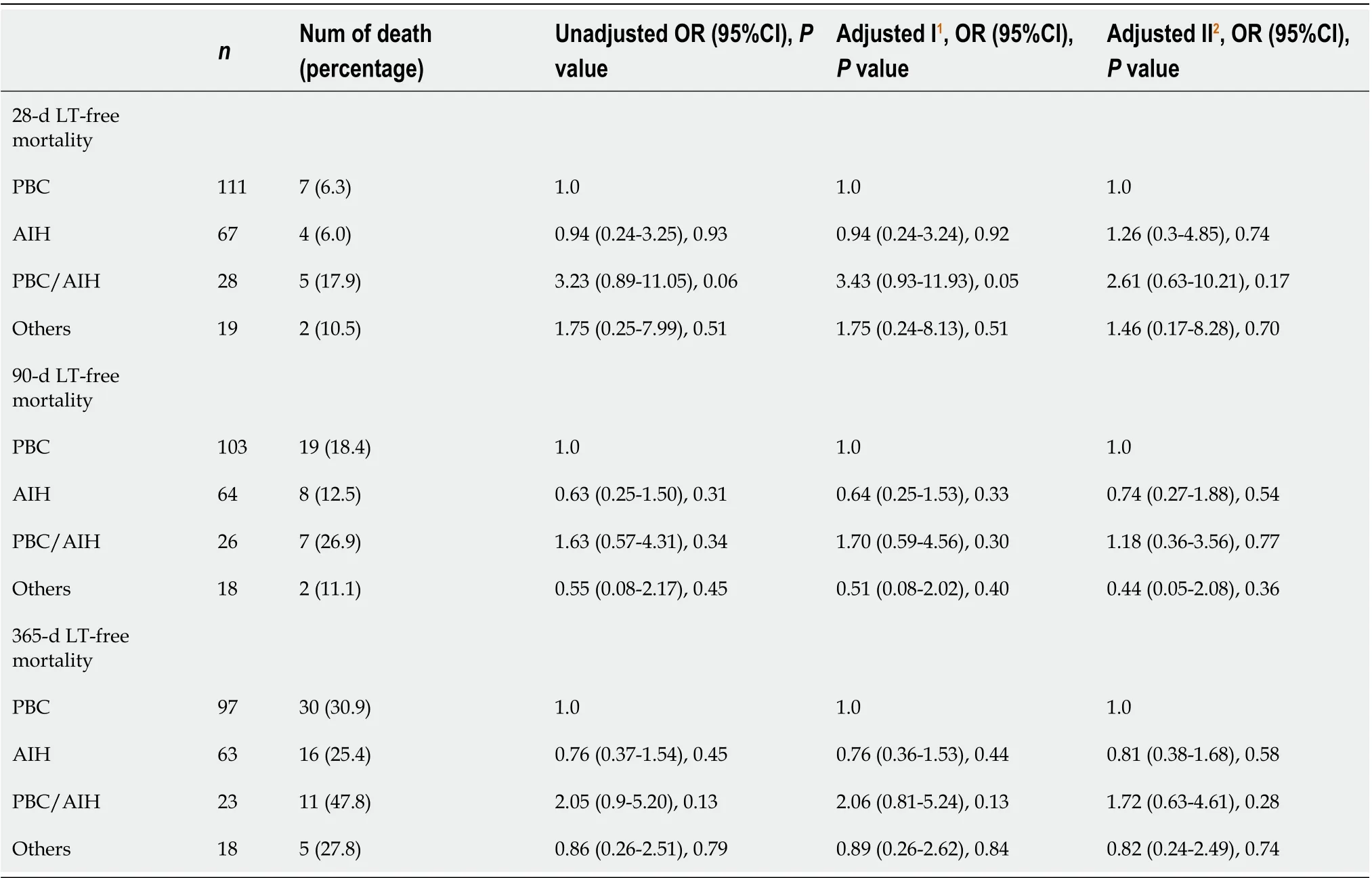
Table 3 The impact of etiology on liver transplantation-free mortality in acute-on-chronic liver failure patients with cirrhosis and acute decompensation (primary biliary cirrhosis as a reference)

Figure 3 Outcomes of autoimmune liver disease patients with acute decompensated cirrhosis and acute-on-chronic liver failure. A: Liver transplantation (LT)-free mortality in patients with cirrhosis and acute decompensation; B: LT-free mortality in patients with acute-on-chronic liver failure. LT: Liver transplantation; PBC: Primary biliary cirrhosis; AIH: Autoimmune hepatitis; PBC/AIH: Primary biliary cirrhosis-autoimmune hepatitis overlap syndrome; AD: Acute decompensation; ACLF: Acute-on-chronic liver failure.
There were still several limitations in our study. First, since AILD is a relatively rare disease, the number of patients recruited in our study was not quite large, especially ACLF patients. The limited sample size could also slightly reduce the accuracy of the results of risk factor analysis. Second, one of our centers, Renji hospital, is a nationwide center of AILD. Thus, some degree of selection bias could be present in the prevalence rates of AILD due to the participation of this center. However, our furtheranalysis showed that patients recruited from Renji Hospital were from 20 different districts all over the country, the population distribution of these patients were also consistent with that of Chinese population density.
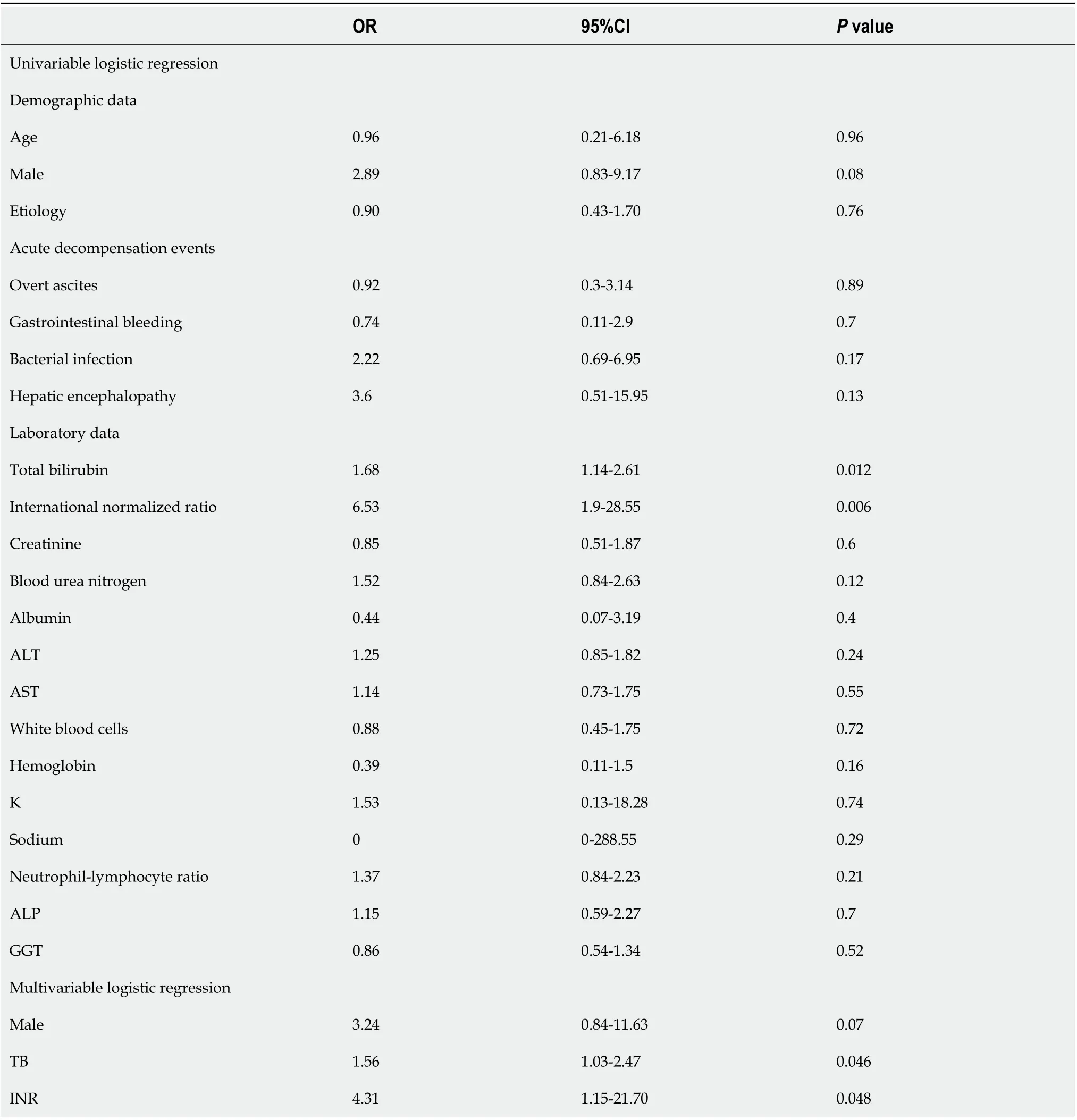
Table 4 Association of risk factors with acute-on-chronic liver failure development during hospitalization using logistic regression in univariate and multivariate analysis
CONCLUSlON
In conclusion, our study showed that AILD was not rare in China. The etiology of AILD had no significant impact on short-term mortality in AILD patients with cirrhosis and AD. HE, elevated levels of TB and BUN were significantly associated with high 90-d mortality in these patients. Strategies are needed to the presence of HE and closely monitor the changes of liver and renal function in clinical practice. These data will be a crucial complement to the public epidemiology of AILD in Asian-Pacific regions.
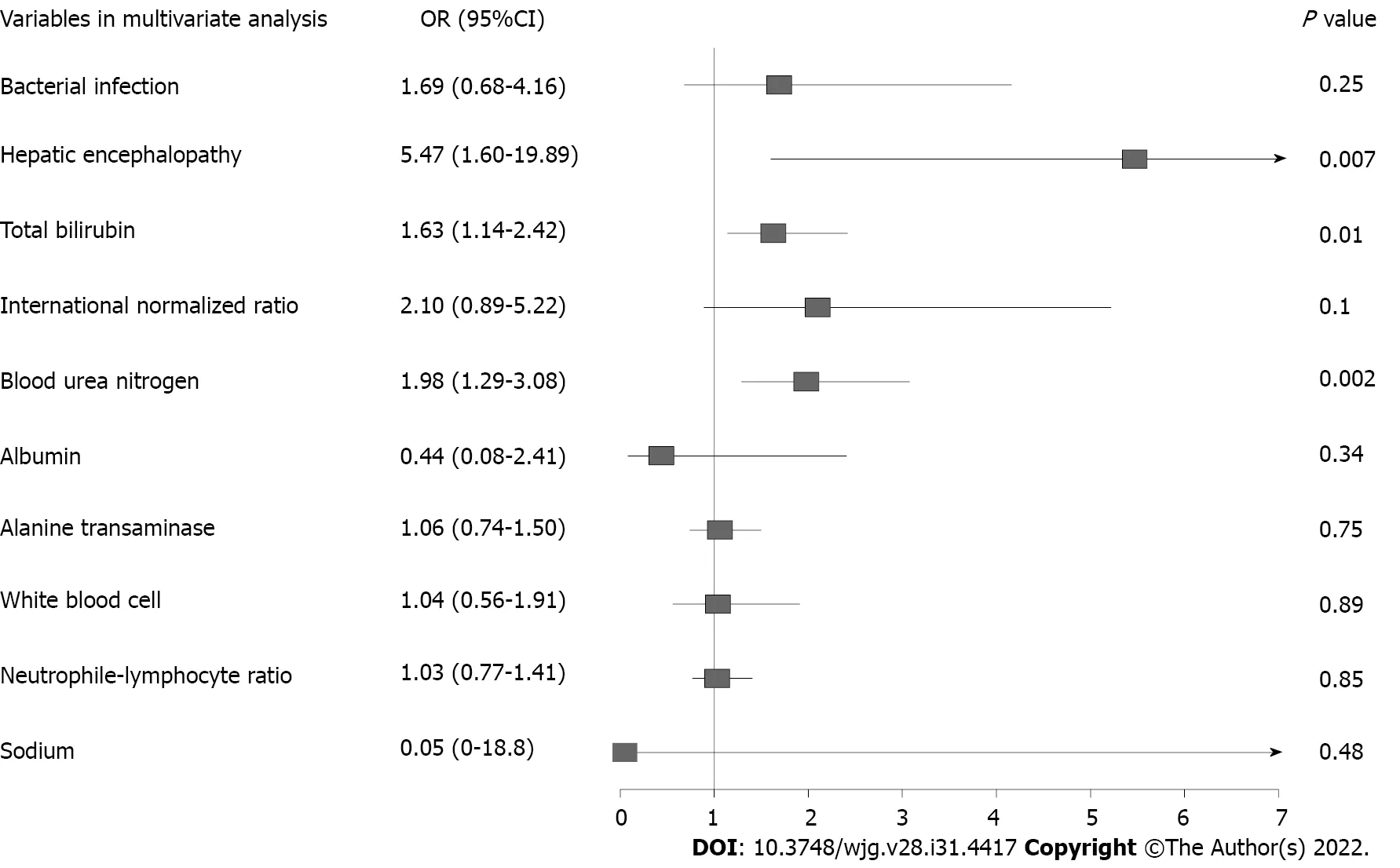
Figure 4 Multivariate analysis of 90-d liver transplantation free mortality in autoimmune liver disease patients with cirrhosis and acute decompensation. OR: Odds ratio; CI: Confidence interval.
ARTlCLE HlGHLlGHTS

Research perspectives
In clinical management of AILD, strategies are needed to prevent presence of HE and closely monitor the changes of liver and renal function.
ACKNOWLEDGEMENTS
We acknowledge the following Chinese (Acute on) Chronic Liver Failure Consortium members and participants for their hard work. Department of Gastroenterology, Renji Hospital, School of Medicine,Shanghai Jiao Tong University - Shi-Jin Wang, Wen-Yi Gu, Liang Qiao, Yan Zhang; Clinical Research Institute, Shanghai Jiao Tong University School of Medicine, Shanghai, China, Zhang Wei-Tuo; Centre of Integrative Medicine, Beijing Ditan Hospital, Capital Medical University - Qun Zhang, Yi-Xin Hou,Yu-Xin Li, Yun-Yi Huang; Department of Infectious Diseases, Southwest Hospital, Third Military Medical University (Army Medical University) - Jie Xia; Yi Zhou; Bao-Yan Xu; Shu-Ning Sun, Yun-Jie Dan, Wen-Ting Tan; Department of Infectious Disease, Hunan Key Laboratory of Viral Hepatitis,Xiangya Hospital, Central South University - Jun Chen, Ruo-Chan Chen, Xiao-Xiao Liu; Department of Infectious Diseases, Institute of Infection and Immunology, Union Hospital, Tongji Medical College,Huazhong University of Science and Technology - Jing Liu, Ling Xu, Shue Xiong; Hepatology Unit,Department of Infectious Diseases, Nan-fang Hospital, Southern Medical University - Xiu-Hua Jiang,Bei-Ling Li, Cong-Yan Zhu; Department of Hepatology, First Hospital of Jilin University - Chang Jiang,Xiao-Yu Wen, Na Gao, Chun-Yan Liu; Department of Infectious Disease, Taihe Hospital, Hubei University of Medicine - Yuan-Yuan Chen, Sen Luo, Qing Lei; Department of Liver Intensive Care Unit,Shanghai Public Health Clinical Centre, Fudan University - Xue Mei, Liu-Juan Ji, Jie-Fei Wang;Department of Infectious Diseases and Hepatology, Second Hospital of Shandong University - Tao Li,Xuan-Qiong Fang, Zi-Yu Wang; Liver Disease Centre, First Affiliated Hospital of Xinjiang Medical University - Rong-Jiu Zheng, Nan Li; Department of Infectious Disease, Henan Provincial People’s Hospital - Hui-Ming Jin; Affiliated Hospital of Logistics University of People’s Armed Police Force - Hai Li, Qing Zhang, Xue-Qun Zheng; Department of Infectious Diseases, Affiliated Hospital of Logistics University of People’s Armed Police Force - Shao-Yang Wang. We thank all the patients participated in the study.
FOOTNOTES
Author contributions:Shen ZX, Wu DD, Xia J, Wang XB, Zheng X, Huang Y and Li BL contributed equally to this work; Ma X and Li H contributed equally to this work; Li H generated the concept and designed the research; all authors acquired the data; Shen ZX, Wu DD performed statistical analysis; Shen ZX, Wu DD, Xia J, Wang XB generated the results; Shen ZX, Wu DD, Zheng X, Huang Y and Li BL interpreted the results; Shen ZX and Wu DD drafted the manuscript which was revised by Ma X and Li H for important intellectual content; Ma X made important contribution patient recruitment; Li H was responsible for administrative, technical, or material support and study supervision; and all authors have access to the data, approved this final version of the manuscript and are accountable for all aspects.
Supported byShanghai Hospital Development Commission, No. SHDC2020CR1037B; the National Key R&D Program of China, No. 2017YFC0908100; the National Science and Technology Major Project, No. 2018ZX10302206,2018ZX10723203 and 2017ZX10202202; Shanghai Municipal Education Commission-Guofeng Clinical Medicine Grant, No. 20152213; the National Natural Science Foundation of China, No. 82170629, 81930061, 81900579, 81970550,82070613, 82070650, and 81972265; Chongqing Natural Science Foundation, No. CSTC2019jcyj-zdxmX0004; Beijing Municipal Science & Technology Commission, No. Z191100006619033; Local Innovative and Research Teams Project of Guangdong Pearl River Talents Program, No. 2017BT01S131; the Foundation for Innovative Research Groups of Hubei Provincial Natural Science Foundation, No. 2018CFA031; and Guangdong Basic and Applied Basic Research Foundation, No. 2020A1515010052.
lnstitutional review board statement:The study was conducted in accordance with the Declaration of Helsinki. The Medical Ethics Board of Shanghai Renji Hospital, Shanghai, China, approved the studies (ethics codes: [2014]148k and [2016]142k).
lnformed consent statement:Informed consent was obtained from all patients for being included in the study.
Conflict-of-interest statement:All authors declare that they have no conflict of interest in this manuscript.
Data sharing statement:Data are available within 1 year after publication upon reasonable requestviaemail:aclf_group@163.com.
STROBE statement:The authors have read the STROBE Statement-checklist of items, and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Zi-Xuan Shen 0000-0003-0122-3954; Dan-Dan Wu 0000-0002-0453-008X; Jie Xia 0000-0002-9580-7186;Xian-Bo Wang 0000-0002-3593-5741; Xin Zheng 0000-0001-6564-7807; Yan Huang 0000-0002-4747-3740; Bei-Ling Li 0000-0002-0633-5632; Zhong-Ji Meng 0000-0003-0401-535X; Yan-Hang Gao 0000-0002-6836-0614; Zhi-Ping Qian 0000-0003-4641-3348; Feng Liu 0000-0001-7060-3710; Xiao-Bo Lu 0000-0001-5532-7551; Jia Shang 0000-0001-9197-8773; Hua-Dong Yan 0000-0003-2792-7490; Yu-Bao Zheng 0000-0002-2630-2563; Wen-Yi Gu 0000-0002-1615-6064; Yan Zhang 0000-0003-0159-9062; Jian-Yi Wei 0000-0003-3897-6896; Wen-Ting Tan 0000-0002-2884-071X; Yi-Xin Hou 0000-0001-8233-7210; Qun Zhang 0000-0002-6365-0030; Yan Xiong 0000-0001-9356-4777; Cong-Cong Zou 0000-0002-9197-055X; Jun Chen 0000-0001-8320-636X; Ze-Bing Huang 0000-0003-0485-1294; Xiu-Hua Jiang 0000-0002-4646-6186; Sen Luo 0000-0001-5846-6717;Yuan-Yuan Chen 0000-0003-3587-7711; Na Gao 0000-0002-8622-9273; Jing Li 0000-0001-5878-6964; Tao Li 0000-0002-2548-5476; Guo-Hong Deng 0000-0003-1263-7220; Jin-Jun Chen 0000-0003-4275-9149; Xiong Ma 0000-0001-9616-4672; Hai Li 0000-0002-3645-6232.
L-Editor:A
P-Editor:Wang JJ
1Carbone M, Neuberger JM. Autoimmune liver disease, autoimmunity and liver transplantation.J Hepatol2014; 60: 210-223 [PMID: 24084655 DOI: 10.1016/j.jhep.2013.09.020]
 World Journal of Gastroenterology2022年31期
World Journal of Gastroenterology2022年31期
- World Journal of Gastroenterology的其它文章
- Duodenal-jejunal bypass reduces serum ceramides via inhibiting intestinal bile acid-farnesoid X receptor pathway
- Preoperative contrast-enhanced computed tomography-based radiomics model for overall survival prediction in hepatocellular carcinoma
- Application of computed tomography-based radiomics in differential diagnosis of adenocarcinoma and squamous cell carcinoma at the esophagogastric junction
- Radiomics and nomogram of magnetic resonance imaging for preoperative prediction of microvascular invasion in small hepatocellular carcinoma
- Insights into induction of the immune response by the hepatitis B vaccine
- Low-grade myofibroblastic sarcoma of the liver misdiagnosed as cystadenoma: A case report