
Correlation study between dendritic cell and eosinophil in refractory rhinosinusitis
2022-08-12 02:31:24YinPingZengZhongLinMuShunDingZhiFeiLuo
Journal of Hainan Medical College 2022年11期
Yin-Ping Zeng, Zhong-Lin Mu✉, Shun Ding Zhi-Fei Luo
First Affiliated Hospital of Hainan Medical University
1. Department of Otorhinolaryngology Head and Neck Surgery
2. Department of Pathology,Haikou 570102,China
Keywords:Refractory rhinosinusitis Eosinophil Dendritic cell
ABSTRACT Objective: To investigate the correlation of refractory rhinosinusitis by detecting the expression of dendritic cells and eosinophils infiltration in nasal mucosa. Methods: Histological staining was performed to detect eosinophils infiltration respectively in 30 normal nasal mucosa, 30 chronic rhinosinusitis tissues and 30 refractory rhinosinusitis tissues,Immunohistochemistry and immunofluorescence double labeling were performed to detect the expression of CD83 and CD11c in each group, and univariate anova was used to analyze the differences among groups.The correlation between the co-expression of CD83 and CD11c and the infiltration of eosinophilic cells was measured by Pearson correlation analysis. Results: The positive expression of dendritic cells immune markers CD83 and CD11c and eosinophils infiltration of refractory rhinosinusitis was significantly increased compared with the other two groups(P <0.05). Through Pearson correlation analysisthe, correlation coefficient r between CD83 and CD11c co-expression and eosinophils infiltration in each group was positive and P <0.05,both were positively correlated. Conclusion: The number of dendritic cells in refractory rhinosinusitis increased significantly and was positively correlated with the infiltration of eosinophils, which was involved in the development of refractory rhinosinusitis.
1. Introduction
The clinical treatment effect of refractory sinusitis (refractory rhinosinusitis,RRS) is difficult to be satisfactory, and the fundamental reason is that the pathogenesis is not clear and the treatment cannot be made.Most scholars believe that immunodeficiency is one of the potential reasons for poor surgical efficacy and refractory in patients with refractory sinusitis[1], Dendritic cells (Dendritic cell,DC)are the most functional antigen-presenting cells known, and are the initiator of the body's immune response, especially the role in nasal polyposogenesis and development mechanism has become a research hotspot in recent years.Dendritic cells can lead to increased infiltration of eosinophils through a range of cellular and humoral immune mechanisms[2], While eosinophils (Eosinophil,EOS) can also induce the maturation of dendritic cells[3], Currently, CD83、CD11c、S100 is considered together with CD1a as a membrane marker molecule with mature DC[4-6], is also the main marker of DC.One of the characteristics of refractory sinusitis is the increased infiltration of the eosinophil[7]. We applied immunohistochemistry and immunofluorescence to explore the pathogenesis of mature dendritic cells by detecting CD83 and CD11c expression in the sinus mucosa of refractory sinusitis and analyzing the correlation with increased eosinophil infiltration.
2. Data and Methods
2.1 Object
Patients with chronic sinusitis who were hospitalized in nasal endoscopic surgery in otolaryngology-head and neck surgery from January 2018 to December 20 19 were selected, A total of 90 cases, All patients improved endoscopic and three-dimensional CT examination of sinus before surgery, The severe intrasurgical or malignant tumor diseases such as asthma、tuberculosis、hepatitis、hypertension and diabetes were excluded, No antihistamines,glucocorticoids and immunosuppressor drugs were used within 1 month before surgery, The operation was completed by a senior professional title doctor with rich technical experience in nasal endoscopy in our department.Patients who met this experimental criteria were screened by the following criteria and enrolled in groups.Treatment group: RRS patients required reasonable drug treatment without ideal efficacy and received one or more nasal endoscopic surgery; standardized perioperative and nasal care before and after surgery; 3 months or more; follow-up and above showed these signs and symptoms, 12 men, 18 women, 34-57 years, average age 42.17±5.75.Primary treatment group: chronic sinusitis (chronic rhinosinusitis, CRS) Significant improvement or recovery of their clinical symptoms after comprehensive treatment with drugs and surgery; Patients after ② should not score more than 3 after review;The Lund-Kennedey score of unilateral nasal nasal endoscopy should not be more than 3 points after ③; ④nasal unobstructed,The sinus is well open, Nasal mucosa showed no oedema, The nasal cavity has no or only small amounts of abnormal secretions, A total of 30 cases, 17 Men, There were 13 women, Age is 18-63 years old, The mean age was 40.03±9.81 years old.Control group: there were no obvious symptoms of nasal inflammation, no simple nasal septal patients with nasal polyps or inflammatory lesions detected by nasal endoscopy or CT examination, a total of 30 patients, 21 men,9 female, aged 16-54 years, and a mean age of 39.50±7.18 years.There were no significant differences in gender proportion and age between the tested groups (P>0.05).
2.2 Methods
2.2.1 Specimen collectionThe diseased sinus mucosal tissue was taken from the refractory and primary treated groups, and the nasal septum mucosal tissue from the control group.Each tissue specimen was fixed in 10% paraformaldehyde solution and then stored in paraffin embedding for further hematoxylin-eosin (Hematoxylin-eosin,H-E)staining, immunohistochemistry (Immunohistochemistry,IHC),immunofluorescence double labeling experiments.
2.2.2 The CD83 and CD11c expression steps were detected by epidemic histochemistry
Two consecutive sections were taken in the same specimen,Monitoring separately; Sections were routinely dewaxed in each group, Thermal repair antigens, Dritered with 5%BSA blocking solution,Appropriate diluted primary antibodies were added,respectively, CD83(1:200) and CD11c(1:250), respectively They were incubated at 4℃ overnight, Add biogoat dilution concentration of anti-rabbit IgG (: 1:100) and SABC reagent (dilution concentration: 1:100), Line DAB color display,Then hematoxylin underwent mild reoxylin,Alcohol was then dehydrated step by step gradient, Transparency was performed using xylene, Quickly drip with a neutral gum seal, This observation was observed under a microscope.Immunohistochemical results of CD83 and CD11c were localized and quantitatively visualized using the LEICA imaging system to compare the expression of the mature DC cell markers CD83 and CD11c in the sinus or nasal mucosa tissue of each group of patients.
2.2.3 The EOS infiltration steps in each group were detected by H-E staining
The fixed groups of sections were stained with conventional H-E,first xylene dewaxed, fixed using gradient ethanol, hematoxylin for about 5-10 min, dilute ammonia water (1%) returned blue,eosin for 1-5 min, each gradient ethanol dehydration, xylene transparent,quickly dripping with neutral gum,glass sealing,observed and photographed under the microscope.The H-E staining results of EOS were used to locate and quantitatively using the LEICA imaging system to compare the infiltration of EOS in the sinus or nasal mucosa tissue in each group.
2.2.4 Detection step of fluorescent double labeling of epidemic
Paraffin sections were dewaxed to water, They was fixed using
gradient ethanol, Secsections were then placed into a repair box filled with EDTA antigen repair buffer (PH 8), Antigen repair in the microwave oven, Painting circle spontaneous fluorescence quenching, The circles were incubated with BSA for 30min, Serum was then blocked, Add a primary antibody, Sections were incubated flat in a wet castridate overnight with 4℃, The slides were shaken in PBS (PH7.4) in a decolrocaker three times, 5min, each time The secondary antibody cover tissue with the corresponding primary antibody species, They were incubated at room temperature for 50min. at room temperatureAfter the slides were washed again with PBS, the nuclei were restained with DAPI dye solution in the circle,incubated for 10min, at room temperature and washed again, sealed with anti-fluorescence quenched agent, sections were then repeatedly observed under a fluorescence microscope, and finally images were collected.
2.3 Results determination
2.3.1 Immunohistochemical
Expression of CD83 and CD11c determination, tissue sections determined five regions with more positive cells before low magnification (×100), the unified standard for positive cells is brownish yellow or yellow cells, blue nucleus as total cells, then photographed at high magnification(×400), analyzed using Imageproplus 6.0 software to yield a positive cell rate (%).
2.3.2 EOS
Eells were counted before determining five regions expressing positive cells under low magnification field ( 100) and then under high magnification field(×400).
2.3.3 According to the co-expression determination of epidemic
Five CD11c and CD83 co-labeled high expression sites were determined in low magnification visual field (×100). Then images were collected with high magnification visual field(×400)and analyzed by image analysis software Image-proplus6.0,the percentage of positive cells was positive rate (%), with the mean of multiple visual fields as the final value of the section.
2.4 Statistical method
Using SPSS 19.0 statistical software, mean numerical variables were expres sed by ± standard deviation (±s), measurement data were tested for normality, multi-group difference statistics by oneway analysis of ANOVA, and the correlation between CD83 and CD11c co-expression and EOS cell infiltration by correlation analysis, which were statistically significant as P <0.05.
3. Results
3.1 Statistical analysis of CD83 and CD11c expression and differences between groups
After immunohistochemical treatment, the cells with positive CD83 and CD11c markers were mostly yellow, brown or brown, round or oval. Only a small number of CD 83 and CD11c positive cells were visible in the nasal septal tissue of the control group, and positive cells for C D83 and CD11c were mainly located in the upper cortex and propria, and scattered, significantly more than the primary and control groups, see Figure 1.1, Figure 1.2 and Table 1 below.Figure 1.1 shows the immunohistochemical expression of CD83, Figure 1.2 shows the immunohistochemical expression of CD11c; Table 1 shows the specific statistical data of the immunohistochemical expression of CD83 and CD11c, One-way ANOVA compared the positive expression of immunohistochemical markers CD83 and CD 11c in the refractory, naive and control groups in Table 1, According to the statistical results, both the refractory and primary treatment groups were significantly different compared with the control groups(P <0.05); There were also statistically significant differences in the proportion of CD83 and CD11c expression positive rates between the refractory and naive groups (P <0.05), This indicates that the number of dendritic cells in the nasal mucosa varies in patients with refractory sinusitis.

Figure 1.1 Immunohistochemical images of CD83 in each group A refractory group,B initial treatment group,C control group.(The scale is 50μm)

Figure1.2 Immunohistochemical images of CD11c in each group A refractory group,B initial treatment group,C control group.(The scale is 50μm)
Table1 Expression of CD83 and CD11c in each group (±s)

Table1 Expression of CD83 and CD11c in each group (±s)
Group Example number The CD83 positive rate was% The CD11c positive rate was%① refractory group 30 10.9683±1.4343 13.0508±2.5576② initial treatment group 30 7.5627±0.5383 6.9791±1.6477③ control group 30 3.8367±0.8191 3.2110±0.5791 F value 189.711 115.631
3.2 Co-expression of CD83 and CD11c in all groups on mature DC under immunofluorescence and differential analysis between all groups
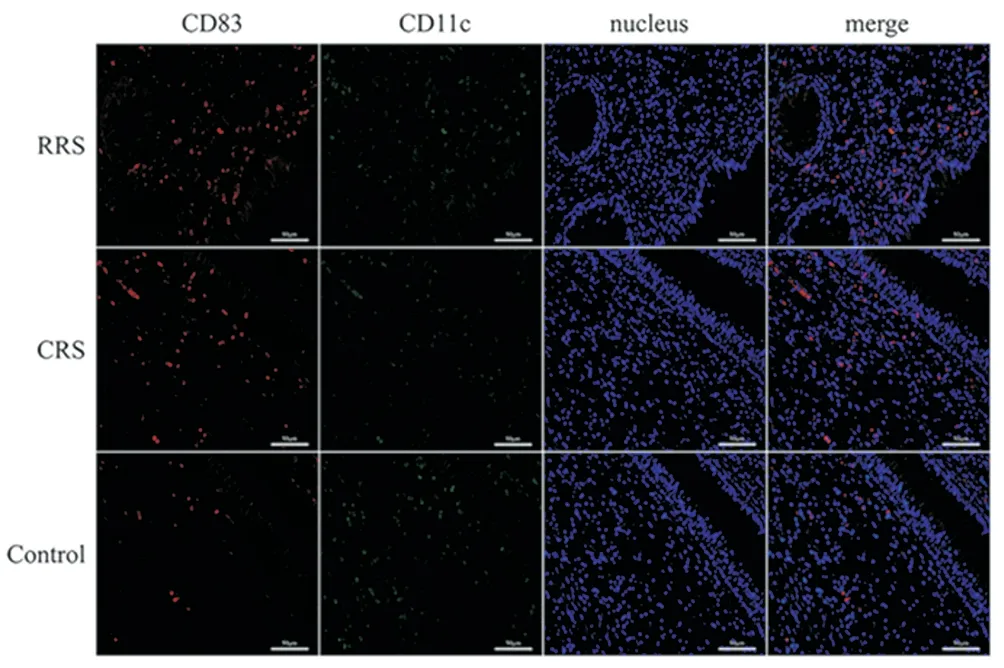
Figure 2 Immunofluorescence images in each group (The scale is 50μm)
Both CD83 and CD11c act as surface marker molecules and colocalization of both more indicates the high expression of mature DC in RRS.Therefore, this study co-labeled CD83 and CD11c to explore the expression of CD83-colocalized DC with CD11c in RRS.Red represents CD83, green represents CD11c, nuclear staining in blue and superimposed in orange when co-labeled DC.DC found that colocalization of CD83 and CD11c was significantly different in refractory group compared to naive group and control group (P<0.05) is shown in Table 2, immunofluorescence for each group,RRS in refractory group, CRS for primary treatment group and control for control group.
Table2 Co-expression of CD83 and CD11c in each group (±s)
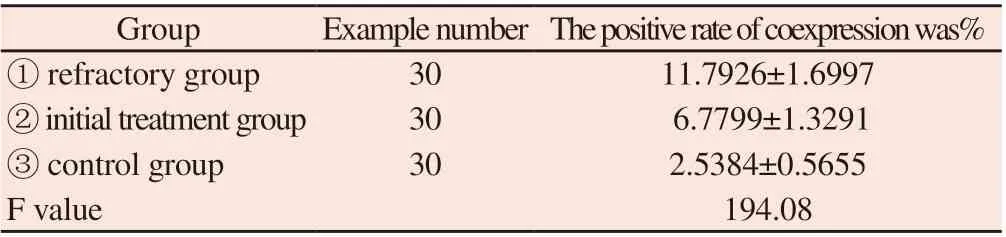
Table2 Co-expression of CD83 and CD11c in each group (±s)
Group Example number The positive rate of coexpression was%① refractory group 30 11.7926±1.6997② initial treatment group 30 6.7799±1.3291③ control group 30 2.5384±0.5655 F value 194.08
3.3 Statistical analysis of EOS infiltration and differences between groups
Eosinophils were mainly separated by the nucleus 2-3,characterized by the cytoplasm as bright red particles.It was mainly found in the upper cortex and the stromal layer, and the number of eosinophil infiltrations in the tissue sections of both the refractory and primary groups increased significantly compared with the control group.The normal epithelium of nasal septal mucosa were neat, no obvious basement thickening, no stromal edema, less eosinophil infiltration; in the first treatment group, loose connective tissue with edema, gland hyperplasia, infiltrating inflammatory cells in the stroma, disordered arrangement, shedding, fracture, gland hyperplasia, and significantly increased eosinophil infiltration,as shown in Figure 3 below. The results of each group in Table 3 were analyzed by one-way ANOVA, with the higher number of eosinophils infiltration than the control group (P <0.05), the higher eosinophil counts in the refractory group than in the primary group,and the specific statistical significance (P <0.05).
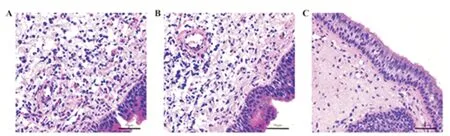
Figure 3 EOS infiltrating images in each group A refractory group,B initial treatment group,C control group.(The scale is 50μm)
Table3 EOS infiltration in each group (±s)
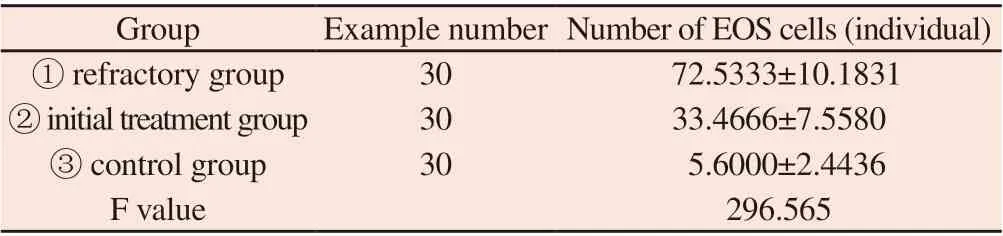
Table3 EOS infiltration in each group (±s)
Group Example number Number of EOS cells (individual)① refractory group 30 72.5333±10.1831② initial treatment group 30 33.4666±7.5580③ control group 30 5.6000±2.4436 F value 296.565
3.4 Correlation analysis of CD83 and CD11c coexpression and EOS infiltration in each group
After immunofluorescence detection of CD83 and CD11c in the nasal mucosa tissue, the r values of each group. The correlation coefficient are shown in Table 4. According to statistical results,a positive correlation between CD83 and CD11c and EOS infilt r ation.

Table 4 Correlation between CD83 and CD11c co-expression and EOS expression
4. Discussion
With the progress and development of medicine, the vast majority of patients with chronic sinusitis (chronic rhinosinusitis,CRS), can get better treatment after systematic drug and surgical treatment.However, there are data indicating that more than 15% of CRS patients will still have persistent clinical symptoms and postoperative recurrence after comprehensive treatment, known as refractory sinusitis[8]. As early as 2001, Wreesmann et al first proposed that refractory sinusitis (refractory rhinosinusitis,RRS) was secondary to drug and surgical treatment, and inflammation remained prolonged for persistent sinusitis, and elaborated the possible pathogenesis[9],It was elaborated by Desrosiers from a pathophysiological perspective in 2004[10], 2012 The European Guidelines for the Diagnosis and Treatment of nasal-sinusitis polyps also formally defined RRS as Difficult-to-treat rhinosinusitis, simply as DTRS[11].In 2013, combining with the previous treatment experience, Han Demin first expounded the relevant content of RRS in China, and systematically discussed its definition, possible pathogenesis,diagnosis and treatment concepts[12]. The 2018 Chinese Guidelines for the Diagnosis and Treatment of Chronic sinusitis affirmed the two descriptions of RRS and DTRS, but also noted that its clinical definition and diagnostic criteria have not been reached.However,because the etiology and pathogenesis of RRS are still not fully elucidated, clinical treatment has been lack of pertinence, and the therapeutic effect is still difficult to be satisfactory.
RRS is a complex, multifactorial inflammatory disease, and current studies have shown that eosinophil infiltration is involved in the pathogenesis of refractory sinusitis, an important link of the multifactorial combination[13]. Eosinophils (Eosnophil,EOS), which have inflammatory and cytotoxic effects, are an important clinical indicator of allergic rhinitis and is often seen in allergic diseases[14],and plays an important role in the formation and growth of nasal polyps[15, 16]. In sinusitis patients, local activation and degranulation of EOS release alkaline proteins such as methyl diphosphol and acidophilic cation protein, causing local damage to the epithelium,inflammatory mediators such as platelet activation factors act on the blood vessels and cause mucosal edema; and it can enable cytokines activation, stimulate epithelial hyperplasia and metaplasia,and neascularization leading to the occurrence and development of polyps.In patients with refractory sinusitis, mucosal edema,mucous purulent secretions, vesicles, polyps and prolonged chronic inflammatory persistence are seen in the postoperative sinus, which is closely related to the increase of EOS infiltration[17-19]. The results of this study increased the number of eosinophils in the mucosa compared with the primary group and control groups. The same as the previous results, we again verified that eosinophils infiltration is involved in the occurrence and development of refractory sinusitis.
Japanese scholar Yoshimi found a small number of Langerhan cells in the normal nasal mucosa, most of which were dendritic cells(Dendritic cell,DC), which found a significantly increased number of Langerhan cells in the nasal mucosa of rhinitis patients[20].This finding is sufficient to demonstrate the involvement of DC dominated Langerhan cells in the development and development of nasal inflammatory disease.DC is characterized by the ability to stimulate initial T cell (Naive T cell) proliferation, and is the initiator of the body's immune response, playing a major role in regulating the direction of T cell differentiation for the most functional antigenpresenting cells currently found.DC-induced immune tolerance is strongly associated with its immature or semi-mature state, mature D C mainly induces immune activation, normally most DC in vivo in an immature state, when mature DC deficiency can lead to T cell negative selection, thus inducing antigen-specific tolerance[21].Therefore, the different D C maturation state is closely related to the type and degree of immune response, which can induce both immune activation response and immune tolerance, and plays an important role in the immunomodulatory process of inflammatory diseases.Mature DC surface can highly express recognition markers such as CD83, CD11c, S100 and CD1a[4-6], Mature DC maturity was investigated by the expression of CD83 molecules with high expression of CD83, when cultured in vitro[22, 23]. An additional characteristic marker of DC is that CD11c, plays an important role in cellular endocytosis, capturing the antigen by CD11c and presenting it to CD4+ and CD8+T cells for an immune response[24]. It can also simultaneously carry an antigen-directed migration to the CD11c cell region at the lymph node edge for targeted presentation to CD4+ and CD8+T cells[25]. Thus, CD11c is also a positive regulator of cellular immunity[26]. Therefore, this study first used immunohistochemistry to separately label the CD83, CD11c molecules indicated by DC,and detect their expression levels to determine DC maturation.The positive expression rate of DC coexpressed by CD83 and CD11c was determined by immunofluorescence colocalization, and it was found that the positive coexpression rate of CD83 and CD11c was significantly higher in RRS than in two other groups (P <0.05).This all suggests that the involvement of mature DC in the pathogenesis of R RS provides new insight into the mechanism of action of mature DC in R RS.
There is a positive association between DC and EOS infiltration in the refractory group of this study, suggesting a possible interaction between eosinophils and dendritic cells in the occurrence and development of refractory sinusitis, and exactly how the correlation can be preliminarily understood in previous studies.Lotfi et al[3]Through experimental findings that non-methylated oligonucleotide DNA of pathogen-associated molecular patterns can stimulate EOS-induced DC maturation, the ratio of DC cells demonstrated that DC maturation is directly associated with EOS; Yang Jihong et al[2]Immunohistochemical staining and Meigge (May-Grunwald Giemsa,MGG) staining experiments for normal nasal mucosa and nasal polyp tissue, respectively, which significantly increased the expression of macrophages, antigen-presenting cells and eosinophils in nasal polyp tissue.As Th1 /Th2 proportional balance plays a key role in the regulation of immune response, some scholars believe that DC leads to its balance imbalance through a series of cellular and humoral immunity, inhibits T cell differentiation into Th1,promotes Th2 polarization, and predominates the cytokines secreted by Th2, mainly IL-4, IL-5, IL-6, IL-10[27]. IL-5 expression has been confirmed to be significantly elevated in nasal polyp tissue, involved in the development of nasal polyposis, and it inhibits the apoptosis of the EOS and extends EOS survival while also promoting EOS infiltration in the inflammatory response[28].
As mentioned above, most scholars believe that immunofunction defects are one of the potential reasons for poor surgical efficacy and refractory in RRS patients.DC acts as the strongest antigenpresenting cells, It is the central link of initiating, regulating, and maintaining the immune response, Through a systematic study of this project, Not only clarifies the trend of high expression of DC's markers CD83 and CD11c in the sinus mucosa of patients with refractory sinusitis, Moreover, it was positively associated with the degree of EOS infiltration, It is shown that DC and EOS play an promoting role in the occurrence and development of RRS, It was confirmed that DC is involved in the occurrence and development of refractory sinusitis,Provide new ideas for studying the pathogenesis of refractory sinusitis, Providing new targets for its treatment,There are still some limitations to this study, First, the sample size was small, Lack of multicenter, large sample, randomized control experiments, And whether DC leads to RRS, through the regulation of EOS,Specifically,how to interact,Can it be used as an important reference indicator to assess RRS severity and prognosis, Further research will be needed.
Author's contribution
Zeng Yinping: Experimental design and case data collection,experimental operation, data analysis and writing of the paper.
Mou Zhonglin: Guide the experimental design and help to modify the paper.
Ding Shun: Participated in the experimental case collection, data collation, etc.
Luo Zhifei: Participate in the pathological data collection, guide the experimental operation, etc.
 Journal of Hainan Medical College2022年11期
Journal of Hainan Medical College2022年11期
- Journal of Hainan Medical College的其它文章
- Study on the mechanism of “Salvia chinensis and Radix Ranunculi Ternati” drug pair in the treatment of lung cancer
- Potential targets and mechanism of Xingxiao Pill for the treatment of lung cancer were analyzed based on network pharmacology and molecular docking
- Effect of total glucosides of paeony on serum cytokines in patients with psoriasis and its clinical efficacy: A meta-analysis
- Effects of post-dilation on coronary blood flow and MACE events following primary percutaneous coronary intervention in patients with STEMI
- An exploration on the protective mechanism of Xuduan Zhongzi prescription against epididymis oxidative damage in oligoasthenospermia model rats based on Nrf2-NQO1/γ-GCS signaling pathway
- Effects of compatibility of Scutellaria baicalensis stems and Polygonum cuspidatum on TRPV1 expression and inflammatory cytokines in rats with acute lung injury