
Evaluating the best treatment for multifocal hepatocellular carcinoma: A propensity score-matched analysis
2022-08-12 08:10MatteoRisalitiIleniaBartoliniClaudiaCampaniUmbertoArenaCarlottaXodoValentinaAdottiMartinaRosiAntonioTaddeiPaoloMuiesanAmedeoAmedeiGiacomoBatignaniFabioMarra
World Journal of Gastroenterology 2022年29期
Matteo Risaliti, Ilenia Bartolini, Claudia Campani, Umberto Arena, Carlotta Xodo, Valentina Adotti, MartinaRosi,Antonio Taddei, Paolo Muiesan,Amedeo Amedei, Giacomo Batignani, Fabio Marra
Abstract
Key Words: Hepatocellular carcinoma; Multifocal hepatocellular carcinoma; Liver resection; Trans-arterial chemoembolization; Guidelines; Liver tumour management
lNTRODUCTlON
Hepatocellular carcinoma (HCC) is the most frequent primary liver cancer worldwide, accounting for approximately 90% of cases[1]. HCC incidence has grown over the last two decades, with more than 900.000 new casesperyear. Moreover, it is expected to further increase in the next few years due to the exponential growth in nonalcoholic fatty liver disease[2]. Despite the improvements in diagnosis and management, HCC is detected in a multinodular form in 35%-40% of cases[3,4] with a reported 5-year survival rate of 19.5%[5].
Over the years, various staging systems have been proposed to overcome the limitations of the tumour-node-metastasis system, which only considers tumour burden[6]. Currently, the Barcelona Clinic Liver Classification (BCLC) is one of the most widely used staging systems for HCC, and includes variables related to tumour status, liver function, and performance status (PS), and recommends one or more specific treatment modalities for each disease stage[7].
Several additional efforts have been made to deal with the heterogeneity of the BCLC-B or intermediate stage of this classification. The Italian Liver Cancer (ITA.LI.CA) group recently proposed a new staging system and prognostic score, based on the BCLC staging system, which includes tumour burden, liver function, and other patient-related variables, and provides a subclassification of this stage[8].
Surgical treatments, including liver resection (LR) and liver transplantation, are considered the best choice for survival and quality of life whenever feasible, while Trans-Arterial ChemoEmbolization(TACE) is not a curative treatment and should be used for patients with well-defined, multifocal HCC, a preserved portal flow, and adequate liver function and PS. TACE outcomes are poor, and several lines of information about the safety and effectiveness of surgery in selected patients for whom TACE is usually recommended have been reported[9-12]. Finally, liver transplantation could also have a central role for these patients, especially after successful downstaging[7], but organ shortage and increased demand for organ transplantation could lead to high drop-out rates.
The debate concerning whether selected patients with multinodular HCC may benefit from surgery rather than TACE remains unsolved.
In this study, a propensity-score matching analysis was used to compare procedure-related morbidity and oncological outcomes in multifocal HCC patients classified as BCLC-B who underwent LR or TACE to determine if one treatment should be given priority over the other.
MATERlALS AND METHODS
Study design and patients
A retrospective analysis was conducted on patients with multifocal HCC who had undergone surgical resection or TACE as first-line treatment between May 2011 and March 2021. The following exclusion criteria were considered: Age < 18 years, Child-Pugh score > 7, vascular invasion or extrahepatic spread,and hepatic venous pressure gradient > 15 mmHg. HCC was diagnosed histologically or by imaging techniques [magnetic resonance imaging and/or triphasic computed tomography (CT)] according to the available EASL guidelines version. Before LR or TACE, an evaluation of age, comorbidities, blood chemistry, tumour number and size (major radiological diameter of the largest lesion from the last available imaging test), ITA.LI.CA. stage and Eastern Cooperative Oncology Group PS.
The decision to perform surgery or TACE was taken by the local multidisciplinary team who considered patients and tumour features, including lesion location and relation with the pedicles, and the volume of the future liver remnant. During surgery, intraoperative ultrasound sonography (IOUS)was routinely performed to confirm preoperative planning. Whenever feasible, anatomic resections were preferred. Both conventional, lipiodol-based TACE and TACE with drug-eluting beads were included. The patients’ response was evaluated one month after the procedure with a CT scan. For patients who did not achieve a complete response, data and the effectiveness of each subsequent TACE were also recorded.
Post-treatment morbidity was evaluated according to the Clavien-Dindo (CD) classification[13].
All patients underwent a standardised follow-up programme that included blood tests with alphafetoprotein (AFP), and a triple phase-contrast enhanced CT scan every three months for the first year and then biannually for 5 years after surgery (starting 3 mo after surgery or 1 mo after TACE).Recurrence was diagnosed in the case of radiological evidence of HCC.
Statistical analysis
Quantitative data were expressed as mean ± SD or median and range, as appropriate. Qualitative data are reported as absolute and relative frequencies. Satterthwait’s test or the Mann-Whitney test was used according to the Shapiro-Wilk test and F-Test, respectively, for normality distribution and homoscedasticity to assess the difference in quantitative variables between treatment groups t-test. The chisquare test or Fisher’s test were used as appropriate to verify the association between qualitative variables and treatment groups. The propensity score matching (PSM) method was used to compare similar treatment groups for known prognostic factors (AFP levels as a dichotomous variable with a cutoff set at 400 ng/dL, presence or not of cirrhosis, Child-Pugh and Model for End-Stage Liver Disease(MELD) score, number, and diameter of lesions). An AFP level > 400 ng/mL was considered a prognostic factor of poor outcome, as suggested by recent guidelines[14]. A diagnosis of cirrhosis was established based on the presence of one or more of the following: Compatible histology, imaging showing compatible hepatic morphology, liver stiffness > 15 kPa by vibration-controlled transient elastography, clinical or endoscopic or imaging signs of portal hypertension. The propensity score was calculated by a multiple logistic regression model with a backward selection method. The nearest neighbour method was used to match the two groups with a 1:1 ratio.
Overall survival (OS) was calculated from the date of the first treatment to death of any cause or the last follow-up. As TACE patients could need more than one treatment to achieve a complete response,disease-free survival (DFS) was calculated from the date of the effective treatment to the date of first radiological recurrence. Survival was expressed as the median and 95% confidence interval.
The Kaplan-Meier curve method and the log-rank test were used to evaluate the difference in OS and DFS between the groups.
Subgroup survival analyses were performed comparing the results of the different treatment modalities and stratifying patients by the different grades of the ITA.LI.CA classification, the AFP levels(using 400 ng/mL as cut-off), and by the different number and size of HCC (dividing them into two groups using the median value as a cut-off). APvalue < 0.05 was considered statistically significant.
All the analyses were conducted using SAS, version 9.2 (SAS Corporation, Cary, NC, United States),and revised by a biomedical statistician.
RESULTS
Patient clinical characteristics
A total of 50 patients with multifocal HCC were included in the study, 25 underwent LR while 25 underwent TACE. The distribution of the factors used for the PSM in the general population is reported in Table 1. All patients belonging to the TACE group had cirrhosis, whereas, among those who underwent LR, cirrhosis was absent in 36% of cases (P= 0.002). The number of lesions was higher among patients who underwent TACE, whereas resected patients usually had more extensive tumours.No significant differences were found between the two groups regarding Child-Pugh score and AFP levels. In contrast, the MELD score tended to be higher in patients who underwent TACE compared with the resected patients. After the PSM, only 30 patients were eligible for the final analysis, 15 from each subgroup.
The general baseline clinical characteristics are shown in Table 2, while data regarding liver function aspects, tumour characteristics, and patient distribution according to the Up-to-7 criteria[15] and ITA.LI.CA classification are reported in Table 3. No statistical differences were found in baseline characteristics. The median age was 69 years, and more than two/thirds of patients were male. The most common cause of liver disease was viral hepatitis, followed by NASH and alcohol use disorder. Lower platelet counts and higher bilirubin levels were present in the TACE group. There was also a trend towards a higher presence of varices in the TACE group. No significant differences across the Up-to-7 criteria in or out and ITA.LI.CA. staging distribution were found.
Postoperative short-term outcomes and survival analysis
Patients in the TACE group received a significantly higher number of treatments (Table 4,P= 0.001).Post-procedure complications were not significantly different between patients who underwent LR and TACE (Table 4). In the surgery group, complications classified as grade 1 and 2 of CD included fever,pneumonia, or the need for blood transfusion. Only one patient developed bile leakage classified as grade 3 according to CD and was treated with percutaneous drainage.
In the TACE group, complications classified as grade 1 and 2 of CD included mostly transient alterations in liver biochemistry and/or fever. Only one patient developed temporary liver failure and required percutaneous drainage due to an abdominal effusion.
The median follow-up was 19 mo (range 3-62). The estimated global median OS and DFS were 31 and 5 mo, respectively (Figure 1). There were no significant differences in OS and DFS for the global population stratified by the ITA.LI.CA classification. Median OS for B1, B2, and B3 groups were 31, 31,and 14 mo, respectively (P= 0.803), while median DFS for B1, B2, and B3 groups were 5, 14.5, and 1.5 mo, respectively (P= 0.516).
No differences in OS were observed when the two treatment groups were compared. A significantly longer DFS was found in resected patients compared with those undergoing TACE (19 movs0 mo,respectively,P= 0.0001) (Figure 2).
Subgroup analyses were also performed to evaluate the possible differences in OS or DFS according to AFP levels, size, lesion number, Up-to-7 criteria, and ITA.LI.CA staging between each treatment group.
A significant difference was found in both OS and DFS (P< 0.0001 andP= 0.0001, respectively,Figure 3A), with patients presenting with lower levels of AFP showing the best prognosis, in both treatment groups. Furthermore, patients with AFP levels higher than 400 ng/mL and receiving surgery showed a poor OS compared to the TACE group.
No difference in OS was found when comparing treatment modalities in patients stratified according to the Up-to-7 criteria. On the contrary, DFS was higher in the LR group (P= 0.002) (Figure 3B).
The results of different treatment modalities for patients stratified by the ITA.LI.CA classification are reported in Figure 3C. Similar to the previous analysis, a significant difference was found in both OS and DFS (P= 0.047 andP= 0.001, respectively), with patients classified as B2 and receiving resection,showing the best prognosis, while those classified as B3 and receiving resection had the worst prognosis.
Although no significant differences were found in OS, the 4 patients with more than 3 lesions receiving TACE showed a 1, 3, and 5-year OS of 75%, 25%, and 25%, respectively. Among the surgery group, patients with less than 3 lesions had a significantly higher DFS compared with those with 3 or more lesions (P= 0.001). Conversely, no differences in terms of OS and DFS were found in the TACE group stratified by the number of lesions (Figure 3D). Similar results were obtained when the treatment groups were stratified according to the size of the more extensive lesion (Figure 3E). Patients with smaller lesions in the surgery group had a better DFS.
DlSCUSSlON
HCC is the most common primary liver tumour. Despite recent advantages in terms of follow-up, early diagnosis, and treatment, a considerable percentage of patients are still diagnosed in multiple or advanced forms and global mortality remains high with poor long-term prognosis[16]. The term multifocal HCC comprises patients presenting with a broad disease spectrum, ranging from small,oligonodular tumours to diffuse disease. The accompanying liver cirrhosis, portal hypertension, and liver function impairment should be considered, as they are related to high post-procedure morbidityand mortality. Therefore, a tailored approach is mandatory for each patient, and the decisional role of a specialised multidisciplinary team has been highlighted and encouraged in the last version of the BCLC classification[7].

Table 1 Distribution of the factors used in the propensity score matching in the general population (n = 50), n (%)

Figure 1 Kaplan–Meier curves of global overall survival and disease-free survival. The median overall survival (OS) and disease-free survival (DFS)were 31 mo [95% confidence interval (CI): 14-53] and 5 mo (95%CI: 1-8), respectively. 1, 3 and 5-yr OS rates were 71.4%, 43.6%, and 7.6%, respectively. 1-, and 3-yr DFS rates were 32.6%, and 16.3%, respectively. A: OS; B: DFS. OS: Overall survival; DFS: Disease-free survival.
The BCLC algorithm recommends TACE as the primary treatment modality for multinodular HCC,but whether a subset of patients may benefit from a surgical approach remains unestablished. We conducted a retrospective analysis using the PSM, a method that may provide high-quality evidence in conditions when randomised clinical trials are unethical or unfeasible. For the PSM analysis, both indicators of liver function and tumour burden and aggressiveness were used. Although the Child-Pugh and MELD scores could be considered outdated after the last published version of the BCLC staging system[7], these data are still commonly used in clinical practice. Wanget al[5] showed that patients with gradual deterioration in CP score had shorter survival times and worse prognosis (5-year OS rates of 31.1%, 2.4%, and 0.9% for CP A, B, and C, respectively). AFP is a well-established independent risk factor for survival in HCC patients and levels greater than 400 ng/mL are generally considered diagnostic for HCC, in the presence of appropriate radiologic findings[5,17]. Finally, the number and dimension of the nodules are two of the major prognostic factors, and the most used guidelines underscore their importance in treatment allocation[7,8,14,18].
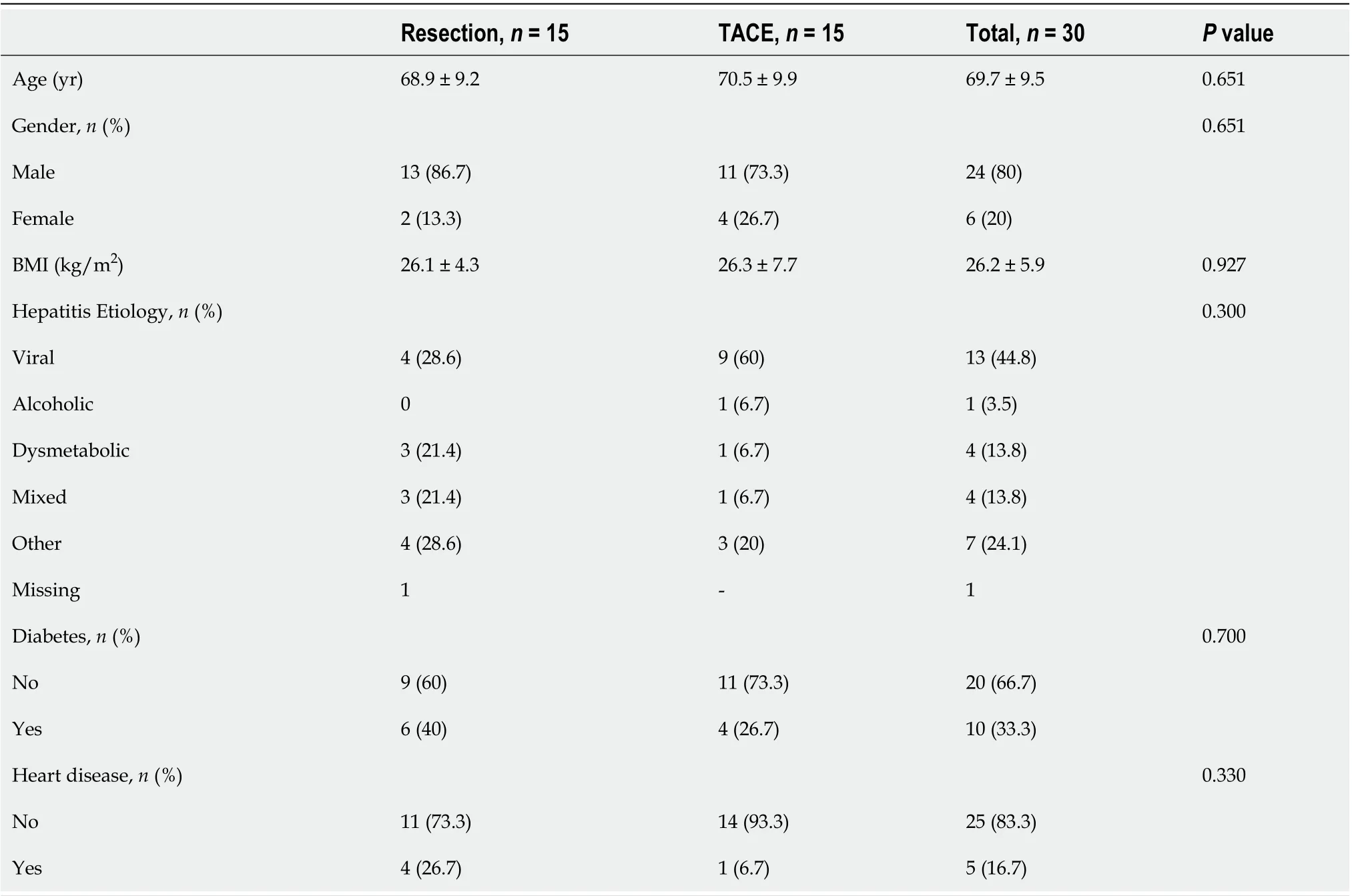
Table 2 General baseline characteristics after propensity score matching (n = 30)

Figure 2 Kaplan–Meier curves of overall and disease-free survival comparing the results of the different treatment modalities (P = 0.312 and P = 0.0001, respectively). Median overall survival (OS) and disease-free survival (DFS) for the resection group were 53 [95% confidence interval (CI): 31-53] and 19 mo (95%CI: 3-Not Evaluable), respectively. Median OS and DFS for the Trans-Arterial ChemoEmbolization group were 18 (95%CI: 8-31) and 0 (95%CI: 0-2) months, respectively. A: OS; B: DFS. OS: Overall survival; DFS: Disease-free survival; TACE: Trans-Arterial ChemoEmbolization.
TACE is considered the standard treatment for BCLC-B patients, as evidence from randomised clinical trials and meta-analyses indicates that TACE provides better survival outcomes compared to the best supportive care with a 1-year mortality rate of 34.1%[19-21]. On the other hand, guidelines do not recommend LR for BCLC-B patients, due to the unfavourable prognostic impact of multinodular presentation and high postoperative morbidity[18]. Moreover, LR for multifocal HCC is a challengingsurgery as wide and/or multiple resections are needed, possibly leading to bile leaks and/or postoperative liver failure.

Table 3 Liver function test and disease burden after propensity score matching (n = 30)
Advances in surgical techniques, including extensive use of IOUS, better coagulation devices, and wider application of minimally invasive surgery, together with better perioperative management, have contributed to improving the results of LR in this difficult-to-treat population. Remarkably, the comparison between different studies is limited by variations in the modalities of detection and reporting of post-procedural complications.
In the present series, we did not find any differences in post-procedure morbidity when comparing resection and TACE. According to the CD classification, only three patients undergoing LR and one patient in the TACE group had a clinically relevant event. However, it should be documented that TACE patients often required more than one treatment to achieve the best response, thus partially explaining the lower morbidity rate of the procedure. Conflicting results on morbidity were previously reported. Zhonget al[22] showed a complication rate of 35% and 21% for resection and TACE,respectively[22]. On the contrary, a meta-analysis did not find any difference in post-procedure morbidity between these two treatment modalities[23].
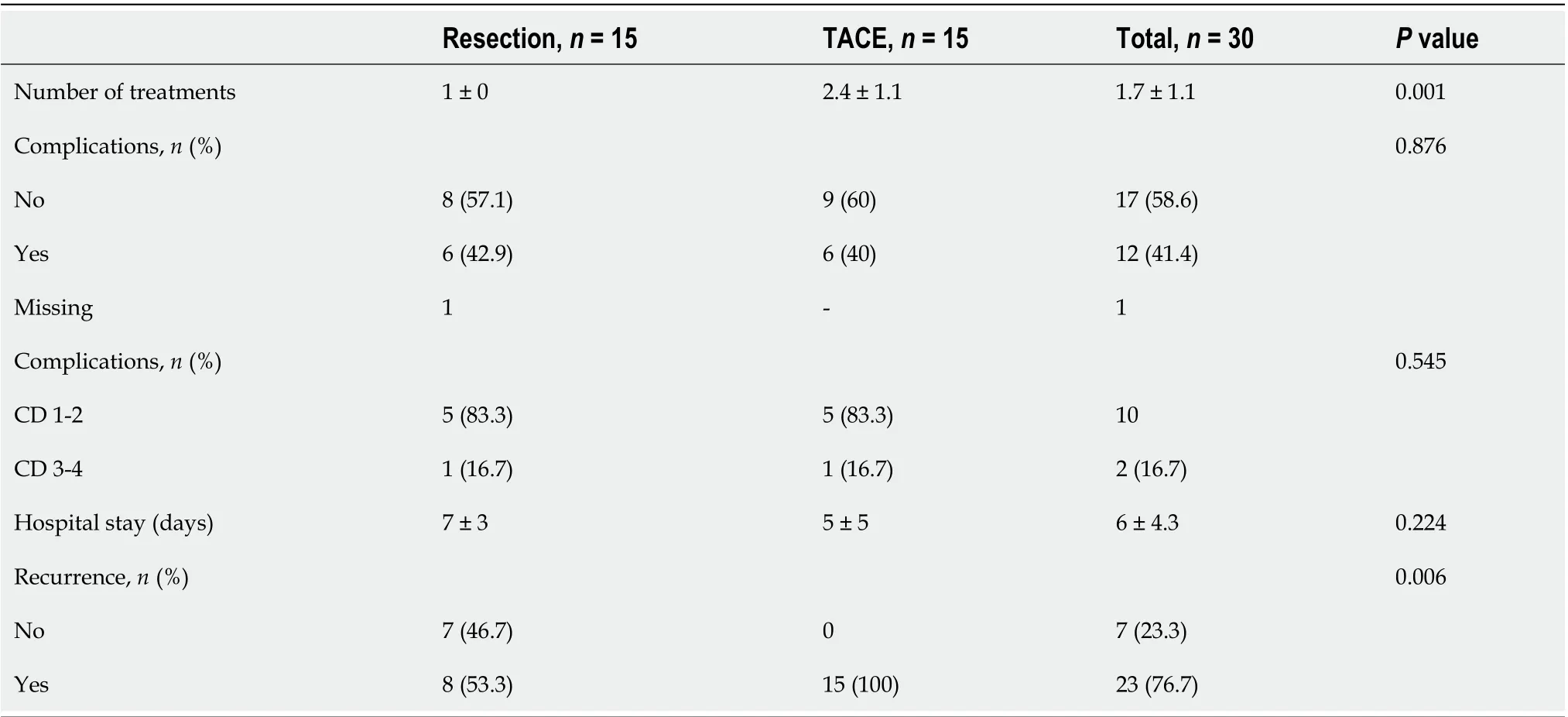
Table 4 Postoperative morbidity and recurrence status (n = 30)
While only a nonsignificant trend towards better OS was observed with surgery, we found that DFS was significantly longer in resected patients. These results confirm and extend previous studies conducted on patients with multinodular HCC. Favourable results with surgery were originally reported by non-controlled studies[10,24]. In a multicentric study including 736 BCLC-B patients,Torzilliet al[24] reported a 5-year survival rate of 57% and a DFS of 27%. The survival benefit of LR compared with TACE in BCLC-B patients has been previously reported in the meta-analysis by Liuet al[23], and similar conclusions were reached in a randomised controlled trial enrolling 173 patients[25].
Considering the marked population heterogeneity of patients with multinodular HCC, subgroup analyses may provide additional clues for better selection of the treatment modality. Not surprisingly,patients with lower AFP levels had the best prognosis. An exciting result was the observation that patients with high AFP levels benefit more from TACE in terms of OS, and further studies are needed to confirm these data and investigate the possible mechanisms thereof. Another aspect which deserves further investigation is to what extent some of these patients with multinodular HCC could benefit from new systemic combination treatments which include the use of immunotherapy with excellent results[26].
Interesting results were also provided by patient stratification according to the ITA.LI.CA classification. Patients in the B2 subgroup, characterised by nodules of smaller size or lower number, showed the best prognosis when receiving LR. In contrast, those classified as B3,i.e., with larger nodules and higher numbers, had the worst prognosis when resected. Patients with two HCC nodules had a more significant benefit from LR compared with TACE in terms of DFS. These data emphasise the relevance of the number of nodules, which is considered a poor prognostic factor and a predictor of early recurrence.
Nonetheless, a clear cut-off value for the number of nodules beyond which resection is contraindicated has not been determined[10,12,25,27]. Furthermore, although using the same parameters of the Up-to-7 criteria (number of lesions and a maximum diameter of the bigger lesions), the ITA.LI.CA.classification showed better ability in patient stratification.
We also evaluated the impact of nodule size on survival in our series. Interestingly, patients with lesions larger than 41 mm had an even more significant benefit from LR in terms of DFS. Previously published studies reported that patients with large solitary HCC had better survival rates when treated with resection than TACE[28,29]. Furthermore, conflicting results have been reported regarding the potential role of tumour diameter as a prognostic factor. While some studies indicated that tumour size alone was not a predictor of poor prognosis[24,30], other reports mentioned tumour dimension as a predictor of survival[31-33]. In particular, in the analysis of 2887 HCC patients, tumour size was an independent prognostic factor of poor survival at multivariate analysis[5], and Wadaet al[12] concluded that while size alone was not a contraindication for resection, a diameter lower than 5 cm was a favourable factor[12].
Several limitations of this study must be acknowledged, including its retrospective nature with the inherent selection bias. Moreover, the fact that a limited number of patients from a single centre were enrolled should lead to caution in the general applicability of the results. In addition, the relatively long period of enrollment could have been associated with differences due to modifications in the HCC management. On the other hand, we performed a rigorous matching using a powerful statistical tool such as the propensity score, although some additional variables not included in the score could have influenced the outcomes.
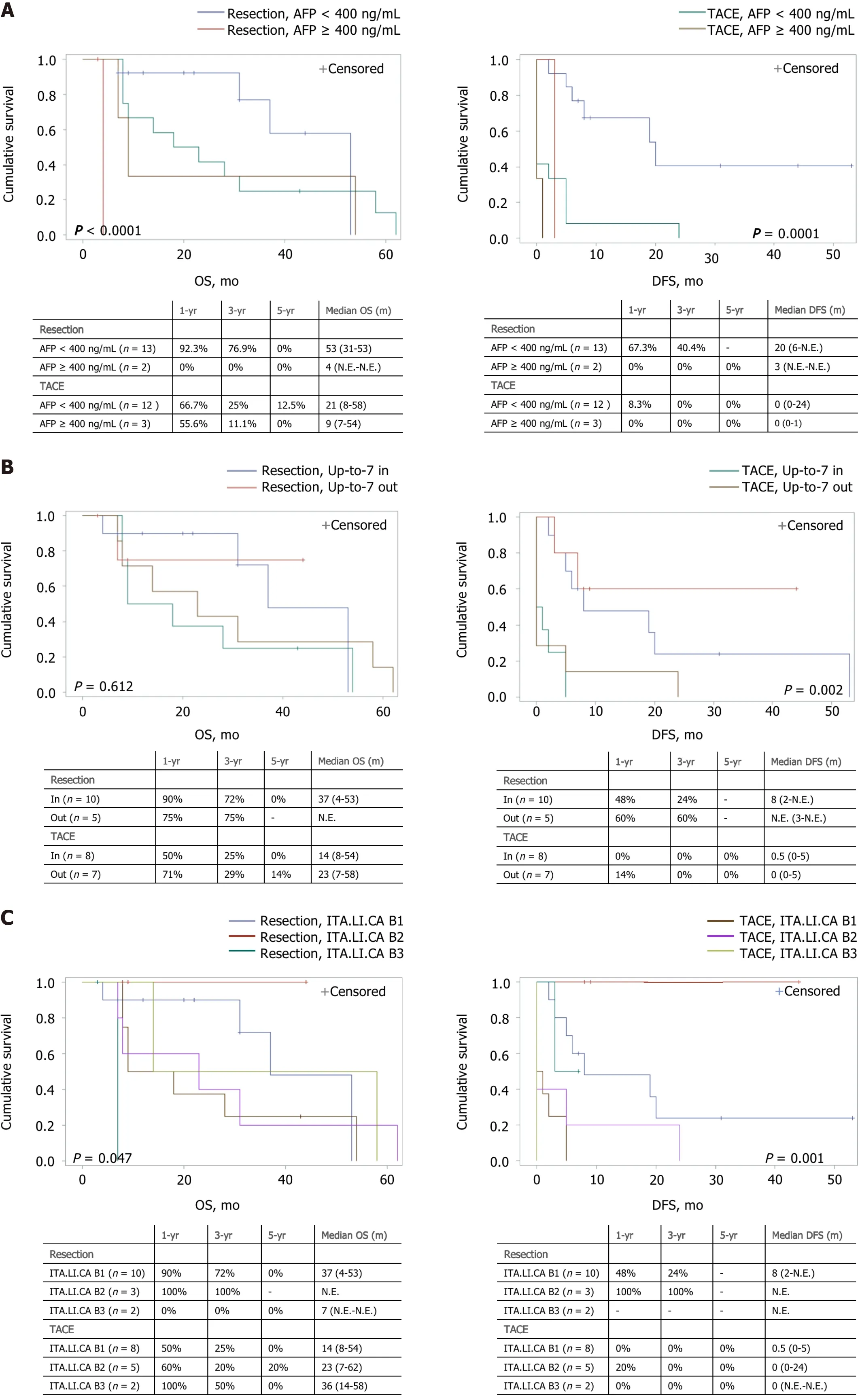
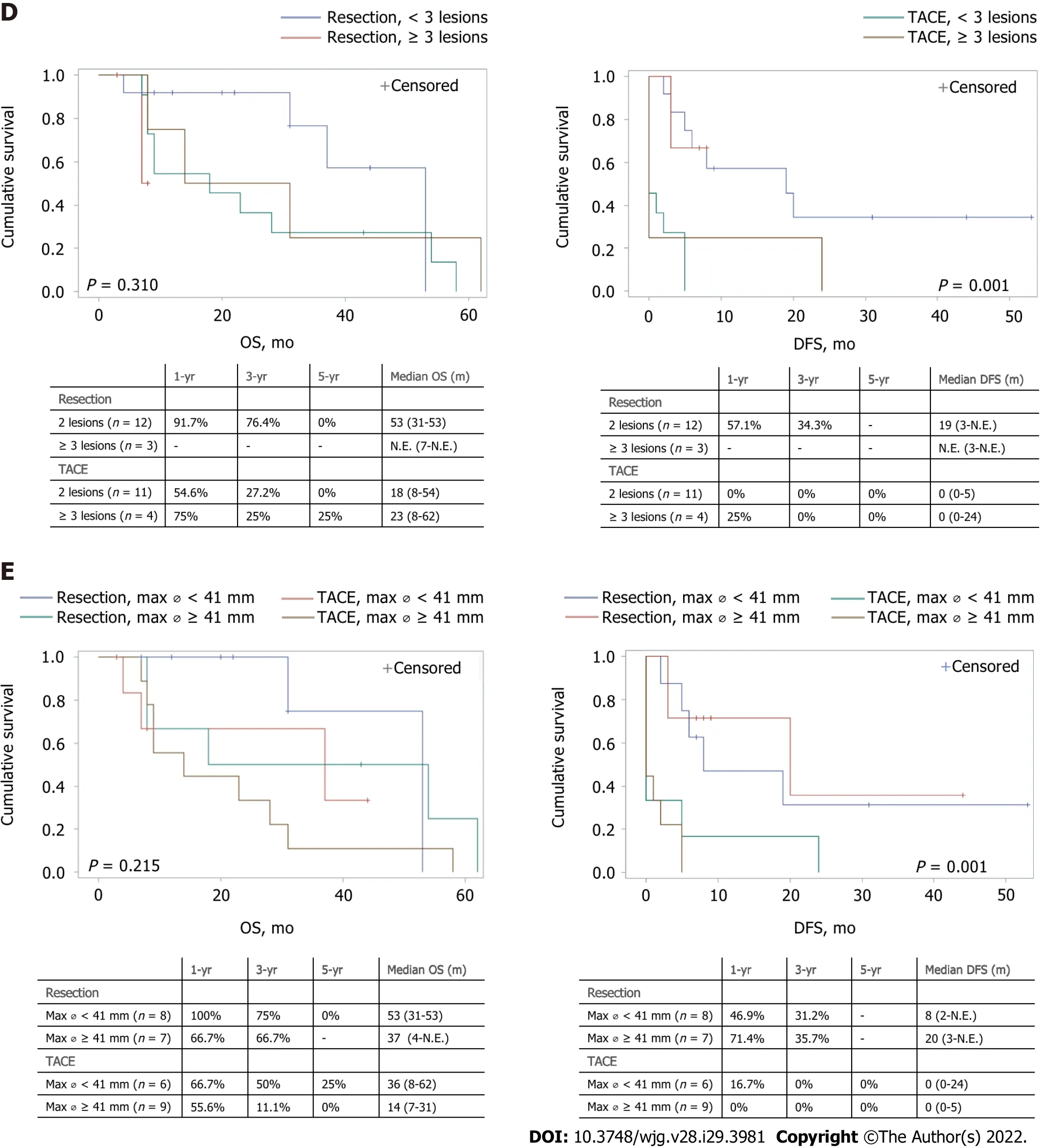
Figure 3 Kaplan–Meier curves of overall and disease-free survival comparing the results of the different treatment modalities for patients stratified by different parameters (n = 30). A: Stratification by alpha-fetoprotein levels, lower or higher than 400 ng/mL [overall survival (OS): P < 0.0001 and disease-free survival (DFS): P = 0.0001]; B: Stratification by the Up-to-7 criteria, in or out (OS: P = 0.612 and DFS: P =0.002); C: Stratification by the ITA.LI.CA classification (OS: P = 0.047 and DFS: P = 0.001); D: Stratification by the number of lesions, 2 lesions or more than 3 lesions (OS: P = 0.310 and DFS: P = 0.001); E:Stratification by the maximum diameter of the lesion, smaller or bigger than 41 mm (OS: P = 0.215 and DFS: P = 0.001). Median survival is expressed as months and 95% confidence interval. OS: Overall survival; DFS: Disease-free survival; AFP: Alpha-fetoprotein; N.E.: Not Evaluable; TACE: Trans-Arterial ChemoEmbolization.
CONCLUSlON
Although the small sample analysed should lead to careful interpretation of the results, after a propensity score matching analysis, patients with multinodular HCC appear to significantly benefit from a surgical approach over TACE in terms of DFS. These results are more evident in the subpopulation belonging to the less advanced B2 subgroup according to the ITA.LI.CA. classification, with AFP levels lower than 400 ng/mL, 2 lesions, and with lesions bigger than 41 mm. Patients classified as ITA.LI.CA B3, with AFP levels higher than 400 ng/mL, and more than 3 lesions had higher benefits from TACE in terms of OS. Future studies are needed to confirm these results in a larger population and to identify other HCC subgroups of patients who would benefit from personalised treatment.
ARTlCLE HlGHLlGHTS

FOOTNOTES
Author contributions:All authors contributed to the conceptualization and design of the study; Risaliti M, Bartolini I and Campani C wrote the original draft; all authors contributed to critical revision of the article and final approval of the version to be published; Amedei A, Batignani G and Marra F supervised the work.
lnstitutional review board statement:The study was approved by the Ethical Committee Area Vasta Centro(Florence), No. 12254/22.
lnformed consent statement:All study participants or their legal guardian provided informed written consent for personal and medical data collection prior to study enrolment.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
STROBE statement:The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Italy
ORClD number:Matteo Risaliti 0000-0001-8476-2536; Ilenia Bartolini 0000-0003-0387-2042; Claudia Campani 0000-0003-3842-782X; Umberto Arena 0000-0002-8839-1506; Carlotta Xodo 0000-0002-7975-5865; Ⅴalentina Adotti 0000-0003-3639-0509; Martina Rosi 0000-0001-6601-4737; Antonio Taddei 0000-0003-2963-4085; Paolo Muiesan 0000-0002-7389-6691;Amedeo Amedei 0000-0002-6797-9343; Giacomo Batignani 0000-0001-8369-6418; Fabio Marra 0000-0001-8629-0878.
S-Editor:Fan JR
L-Editor:Webster JR
P-Editor:Chen YX
 World Journal of Gastroenterology2022年29期
World Journal of Gastroenterology2022年29期
- World Journal of Gastroenterology的其它文章
- Mechanistic and functional extrapolation of SET and MYND domain-containing protein 2 to pancreatic cancer
- Clinical challenge for gastroenterologists-Gastrointestinal manifestations of systemic mastocytosis: A comprehensive review
- Structural changes of proteins in liver cirrhosis and consequential changes in their function
- Epidemiologic and socioeconomic factors impacting hepatitis B virus and related hepatocellular carcinoma
- Enhanced endoscopic ultrasound imaging for pancreatic lesions: The road to artificial intelligence
- Qingyi decoction attenuates intestinal epithelial cell injury via the calcineurin/nuclear factor of activated T-cells pathway