
Incidence and clinical characteristics of hypertriglyceridemic acute pancreatitis: A retrospective singlecenter study
2022-08-12 08:10XueYanLinYiZengZhengChaoZhangZhiHuiLinLuChuanChenZaiShengYe
World Journal of Gastroenterology 2022年29期
Xue-Yan Lin, YiZeng, Zheng-Chao Zhang, Zhi-Hui Lin, Lu-Chuan Chen, Zai-Sheng Ye
Abstract
Key Words: Hypertriglyceridemic acute pancreatitis; Triglyceride; Improved Marshall score; Severity of acute pancreatitis; Intravenous insulin; Hemoperfusion
lNTRODUCTlON
Acute pancreatitis (AP) is an inflammatory condition of the pancreas that originates within the pancreatic acinar cells and causes pancreatic necrosis, systemic inflammatory response syndrome, and multiple organ failure[1], with a mortality rate for severe cases as high as 20%-25%[2]. The great majority of AP is driven by gallstones (40%-70%) and alcohol (25%-35%)[3]. With the change of people’s diet structure and lifestyle, the incidence and mortality of hypertriglyceridemic (HTG)-AP are increasing year by year and has surpassed alcohol as the second leading cause of AP in China[4]. The standardized incidence rate of HTG-AP increased from 0.7 to 1.7 per 100000 person-years from 2008 to 2019 in Denmark[5], and the incidence has increased by 2.4 times in 10 years. However, the increasing number of HTG-AP incidence remains unclear in China.
The mechanism by which severe HTG precipitates to AP remains unknown. Studies have shown that pancreatic lipase hydrolyses excess triglyceride (TG) with accumulation of free fatty acids, thereby inducing the production of acinar cell and pancreatic capillary injury; chylomicrons lead to increased blood viscosity and local tissue ischemia[6,7]. Therefore, early detection of serum TG and active treatment measures to reduce serum TG are crucial for the prognosis of AP. Some scholars believe that rapid reduction of serum triglyceride levels within 48 h before the onset of HTG-AP is the key to treatment[8]. Effective treatments of reducing serum TG levels include anti-lipidemic agents, insulin,heparin, low-molecular weight heparin, and blood purification, such as hemoperfusion (HP),plasmapheresis (PE), and continuous renal replacement therapy[6,9]; however, no HTG-AP treatment guideline has been established. At present, selecting routine treatment or blood purification for patients with HTG-AP after admission remains controversial.
In view of the increasing incidence of HTG-AP in recent years and its short and long-term harmful effects on patients, families, and society, scholars have focused on preventing and effectively blocking HTG-AP as well as on its diagnosis and treatment. However, the causes remain unknown[10-12]; the low elevation of amylase (AMY) levels[13] and other characteristics[14] lead to the early misdiagnosis of HTG-AP. In addition, HTG-AP is prone to young age of onset[10], many complications[15], higher chance of systemic inflammatory response syndrome and cardiopulmonary and renal insufficiency[16],severe tendency[17], and lack of unified clinical treatment standards, which bring some difficulties to clinical treatment.
This study aims to improve the clinical diagnosis rate of HTG-AP by summarizing the clinical characteristics of HTG-AP and developing appropriate and cost-effective treatments for patients with HTGAP.
MATERlALS AND METHODS
Patients
From April 2012 to March 2021, AP was diagnosed in 2206 patients in the Fujian Provincial Hospital. A total of 371 hospitalized patients who met the diagnostic criteria of HTG-AP were retrospectively studied, and 219 patients met the inclusion and exclusion criteria that were used to explore risk factors for severe HTG-AP. Fifty-two patients were included after propensity score matching (PSM) was adjusted by sex, age, grades of severity, and baseline TG. Clinical outcomes were compared between the 52 patients treated with intravenous insulin (INS) and HP (Figure 1). The Ethics Committee of Fujian Provincial Hospital approved the study (K2021-02-007).
The inclusion criteria were as follows: (1) Diagnosis of HTG-AP; (2) Admission within 72 h after onset; (3) Age older than 18 years; (4) Assessment of the first episode (for patients with multiple episodes of AP); and (5) Serum TG detected within 24 h after admission.
The exclusion criteria were as follows: (1) Did not undergo serum lipid detection within 48 h after treatment upon hospitalization; (2) AP due to other etiologies (including gallstones, alcohol,autoimmune, drug-induced, hypercalcemia, hyperparathyroidism, pancreatic tumor-related etiology of AP); (3) Treatment in another hospital; and (4) Incomplete information.
Grouping methods
According to the grades of severity standard in the Revised Atlanta Classification, patients were classified into the mild acute pancreatitis (MAP) group, moderately severe acute pancreatitis (MSAP)group, and severe acute pancreatitis (SAP) groups.
Patients were divided into the INS group and HP group according to treatment method. All patients were given basic support treatment including abrosia, gastrointestinal decompression, enema, fluid resuscitation, water maintenance, electrolyte and acid-base balance, lactulose to improve intestinal function, low molecular weight heparin, proton pump inhibitors for gastric acid secretion, and somatostatin/octreotide inhibitor pancreatic secretion. The INS group was given INS. The HP group was treated with HP. Blood access was established by puncture of the femoral vein or internal jugular vein. HP was performed with a resin irrigator (HA330, Zhuhai Lizhu Group, Biological Material Co,Ltd., China) for 2 h every 24 h with a blood flow of 150-250 mL/min. During the procedure, heparin was used to flush the infusion tube. After the procedure, coagulation markers were monitored. For those with prolonged coagulation times, 10-15 mg protamine was given to neutralize the effect of heparin. For patients with bleeding tendency, low molecular weight heparin was chosen, or the dose of heparin was appropriately reduced.
Definition
The diagnosis of AP was in accordance with the Revised Atlanta Definitions[18]. AP was diagnosed when two of the following three characteristics were met: (1) Abdominal pain consistent with AP (acute onset of a persistent, severe, epigastric pain often radiating to the back); (2) At least three times higher levels of AMY and/or lipase above the upper limit of the normal value; and (3) Abdominal imaging(including computed tomography, magnetic resonance imaging, or transabdominal ultrasonography)consistent with changes in AP.
HTG-AP was considered in patients with AP when the level of serum TG was: (1) Over 1000 mg/dL;and (2) Between 500 and 1000 mg/dL with lactescent serum at admission[19].

Figure 1 Research sample screening and grouping process. HTG-AP: Hypertriglyceridemic acute pancreatitis; MAP: Mild acute pancreatitis; MSAP:Moderately severe acute pancreatitis; SAP: Severe acute pancreatitis; TG: Triglyceride; INS: Insulin; HP: Hemoperfusion; AP: Acute pancreatitis.
The severity of AP was graded according to the Revised Atlanta Definitions[18]: MAP, MSAP, and SAP. MAP was defined by the absence of organ failure and the absence of local or systemic complications. MSAP was defined by the presence of transient (< 48 h) organ failure or local or systemic complications in the absence of persistent organ failure. SAP was defined by persistent (> 48 h) organ failure.
Organ failure was determined according to the improved Marshall score standard in the Revised Atlanta classification[18]. Three organ systems were assessed to define organ failure: respiratory,cardiovascular, and renal. For respiratory (PaO2/FiO2), 301 mmHg ≤ PaO2/FiO2≤ 400 mmHg was scored as 1 point, 201 mmHg ≤ PaO2/FiO2≤ 300 mmHg was scored as 2 points, 101 mmHg ≤ PaO2/FiO2≤ 200 mmHg was scored as 3 points, and PaO2/FiO2≤ 101 mmHg was scored as 4 points. For renal serum creatinine (SCR), 134 μmol/L ≤ SCR ≤ 169 μmol/L was scored as 1 point, 170 μmol/L ≤ SCR ≤310 μmol/L was scored as 2 points, 311 μmol/L ≤ SCR ≤ 439 μmol/L was scored as 3 points, and SCR >439 μmol/L was scored as 4 points. For cardiovascular systolic blood pressure (BP), BP < 90 mmHg and fluid responsive was scored as 1 point, BP < 90 mmHg without fluid responsive was scored as 2 points,BP < 90 mmHg and pH < 7.3 was scored as 3 points, and BP < 90 mmHg and pH < 7.2 was scored as 4 points. A score of 2 or more in any system defined the presence of organ failure.
Data collection
Data were obtained from the patients’ medical records and hospital electronic database records. Sex,age, and comorbidities were collected. Clinical manifestations, improved Marshall score[18], modified computed tomography severity index (MCTSI) score[20], organ failure[18], laboratory and imaging data, treatments, intensive care unit admission, length of stay, and prognosis during hospitalization were recorded. All laboratory data were measured within 24 h after admission. Baseline TG and serum AMY were measured using the first tested values since onset. Serum lipids were reviewed within 48 h after administering lipid-lowering treatment.
Statistical analysis
SPSS 25.0 (IBM Corp., Armonk, NY, United States) was used for data analysis, and GraphPad Prism7.0 was used for mapping. Measurement data in normal distribution were expressed as mean ± SD and analyzed with Student’st-test or analysis of variance. Otherwise, variables were described as medians and interquartile ranges and analyzed by Mann-WhitneyUtest or Kruskal-Wallis test. Categorical variables were presented as absolute numbers and proportions and tested byχ2or Fisher’s exact test.Pairedttest was used for continuous variables before and after treatment. Multivariate logistic regression analysis was used to identify independent risk factors with odds ratios (ORs) and 95%CIs. In addition, 1-1 PSM was performed, followed by univariate analysis.P< 0.05 was considered statistically significant.
RESULTS
Trends in incidence of HTG-AP
For nearly a decade, 371 patients were diagnosed with HTG-AP in Fujian Provincial Hospital. The total number of patients with HTG-AP in our hospital increased, and the incidence of HTG-AP was increased by approximately 2.6 times over the past 10 years and ranged from 8.4% to 22.3% (Figure 2).
Clinical characteristics of HTG-AP
A total of 371 patients were diagnosed with HTG-AP, the mean age of the patients with HTG-AP was 39.86 ± 10.20 years, and most of the patients (approximately 93.8%) were young and middle-aged individuals, with a male/female ratio of 2.0 (247/124). The highest incidence rate of AP was observed for men in the age group of 30-39 years (Figure 3).
The mean serum baseline TG values in HTG-AP were significantly high (2544.59 ± 2305.37 mg/dL).The serum AMY elevated levels were higher than normal in 80.1% of the patients with HTG-AP but only three times greater than normal in 46.9% of patients (Table 1).
About 90.6% of patients with HTG-AP had comorbidity with fatty liver disease, and 11 women (3.0%)had an HTG-AP attack during pregnancy. About 54.7% of the cases were related to diet (high fatty acid)and/or drinking (beer). Patients with HTG-AP had a high frequency of SAP (100, 26.9%), organ failure(117, 31.5%), recurrence (122, 32.9%), and high MCTSI score (5.00 ± 1.83). Eleven patients (3.0%) died during hospitalization (Table 1).
Comparisons of different grades of severity of HTG-AP
A total of 219 patients met the inclusion and exclusion criteria divided into the MAP group (n= 29),MSAP group (n= 114), and SAP group (n= 76).
Table 2 shows that the more severe HTG-AP was, the more frequent blood purification was used.Improved Marshall score (P< 0.000), MCTSI score (P< 0.000), baseline TG (P= 0.035), baseline AMY (P< 0.000), CRP (P< 0.000), albumin (P< 0.000), aspartate aminotransferase (P< 0.000), low-density lipoprotein-cholesterol (P= 0.003), urea nitrogen (P< 0.000), creatinine (P< 0.000), calcium (P< 0.000),hemoglobin (P= 0.010), free triiodothyronine (P= 0.018), admission to the intensive care unit (P< 0.000),and mortality (P< 0.000) were significantly different between patients with different grades of severity.
Multivariate logistic regression analysis confirmed that high CRP (P= 0.005, OR = 1.011, 95%CI:1.003-1.019), low calcium (P= 0.003, OR = 0.016, 95%CI: 0.001-0.239), and low albumin (P= 0.023, OR =0.821, 95%CI: 0.693-0.973) were risk factors of severe HTG-AP (Table 3).
Comparisons between INS and HP treatments
Of the 219 patients, 84 patients were treated with INS in the INS group and 32 patients were treated with HP in the HP group. The entire cohort showed that the grades of severity of HTG-AP (P= 0.002)and baseline TG (P= 0.037) were significantly different between patients treated with INS and HP(Table 4).
Given the large severity and baseline TG gap between the two groups, patients were selected for further analysis using PSM, adjusted by sex, age, grades of severity, and baseline TG. After matching, 26 patients were in the INS group and 26 patients were in the HP group (1:1, match tolerance = 0.02). No significant differences in sex (P= 0.184), age (P= 0.895), grades of severity (P= 0.755), improved Marshall score (P= 0.186), MCTSI score (P= 0.127), and baseline TG (P= 0.734) were found between the two groups (Table 4).
In patients with MAP and MSAP, the serum TG level significantly decreased in patients treated with INS (P< 0.000) and HP (P< 0.000) within 48 h (Figure 4). The clearance rates of TG were 57.24% ±33.70% and 56.38% ± 33.61%, respectively (P= 0.927). However, the clearance rate of TG (P= 0.927) and length of stay (13.04 ± 7.92 dvs12.35 ± 6.40 d,P= 0.730) did not differ between the two groups (Table 4).
DlSCUSSlON
Trends in incidence of HTG-AP
AP has many etiologies, and previous studies reported that HTG as an etiologic factor is between 1.3%and 6.9%[21,22]. However, HTG-AP increased at a fast rate in the Asian region during recent years.Taiwan reported that the frequency of HTG as an etiologic factor in patients with AP ranged from 6.3%to 12.3%[23]. A study reported that the incidence of HTG-AP reached 25.6% in 2013[14]. Zhenget al[24]retrospectively analyzed 2461 patients with AP in Beijing during a 5-year period and reported that the causes of AP included biliary (55.75%), alcoholism (10%), hypertriglyceridemia (10.36%), and others(23.89%); however, this work did not mention the rate of increase in HTG-AP.

Table 1 Clinical characteristics of hypertriglyceridemic acute pancreatitis
The standardized incidence rate of HTG-AP increased from 0.7 to 1.7 per 100000 person-years from 2008 to 2019 in Denmark, and the incidence has increased by 2.4 times over the past 10 years[5]. Another study from Guangdong showed that the incidence of HTG-AP in 2000 to 2005 was 2.6 times higher than that in 1990 to 1994 (8.9%vs3.4%,P< 0.05)[25]. Based on recent observations from China[26], theproportion of patients with HTG-AP increased from 14.0% to 34.0% during a 16-year period in a tertiary hospital setting. Our study found that the incidence of HTG-AP increased by approximately 2.6 times and ranged from 8.4% to 22.3% during nearly 10 years, with a significant increase detected after 2017.Our results are similar to previously reported data.

Figure 2 The total number of patients with hypertriglyceridemic acute pancreatitis and other acute pancreatitis in Fujian Provincial Hospital increased significantly during nearly 10 years. HTG-AP: Hypertriglyceridemic acute pancreatitis.
At present, updated population-based estimates on the incidence of HTG-AP are lacking. Some studies have shown that the incidence and mortality of HTG-AP were increasing year by year, which was related to the change of people’s diet structure and lifestyle[4]. At the same time, the availability of the detection of serum TG also improved the diagnosis of HTG-AP. For example, the emergency of our hospital began testing serum TG in 2017, and Figure 1 shows the incidence of HTG-AP has increased since 2017.Figure 1 showed the decrease in the incidence of HTG-AP from April 2016 to March 2017 and from April 2019 to March 2020, which coincided with the opening of the South Hospital of Fujian Provincial Hospital and the outbreak of coronavirus disease 2019 in China, leading to the diversion and reduction of the number of patients with AP and HTG-AP.
Clinical feature of HTG-AP
This study also found that the clinical manifestations of patients with HTG-AP included the most common abdominal pain and abdominal distension as well as nausea, vomiting, and anhelation withoutspecificity. However, patients with HTG-AP have some clinical characteristics, such as serum TG level(2544.59 ± 2305.37 mg/dL) that was significantly higher than normal values at the onset of disease.Hence, serum TG level ≥ 1000 mg/dL is the most important characteristic of HTG-AP[19]. Thus, we can improve the diagnosis rate of HTG-AP by improving the early detection rate of serum TG in clinical work.

Table 4 Comparisons of clinical characteristics and laboratory parameters with different treatment between intravenous insulin and hemoperfusion before and after propensity score matching

Figure 3 lncidence rates of hypertriglyceridemic acute pancreatitis stratified by age and sex.
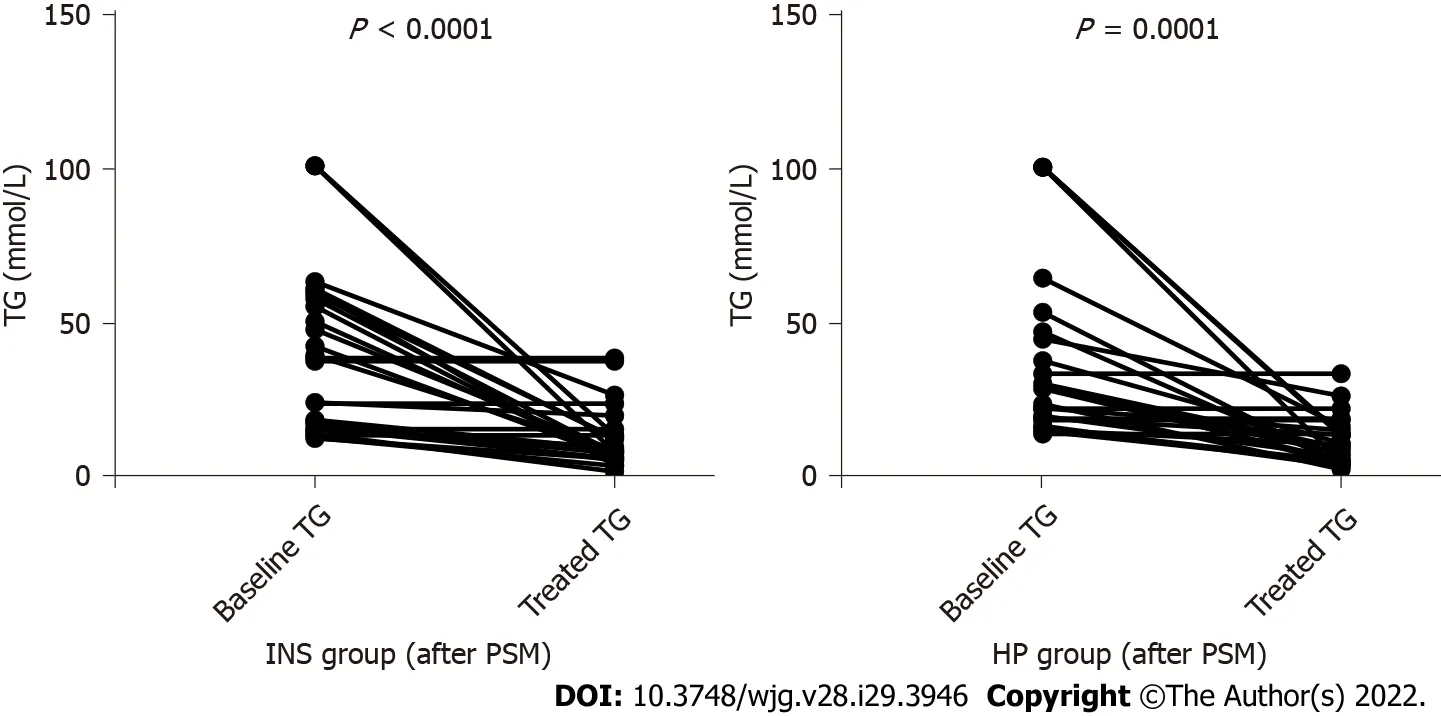
Figure 4 Changes of serum triglyceride levels in both groups before and after treatment. TG: Triglyceride; INS: Insulin; PSM: Propensity score matching; HP: Hemoperfusion.
We found that the mean age of patients with HTG-AP was 39.86 ± 10.20 years. The highest incidence rate of AP was observed for men in the age group of 30-39 years, and the male/female ratio was 2.0(247/124). Liet al[10] reported that patients with HTG-AP were younger (40vs51,P< 0.01) and were mostly males (214/91vs242/183,P< 0.01) compared with patients with biliary AP.
Sekimotoet al[27] stated that the average age for HTG-AP was lower than that for other causes.Zhenget al[24] reported a higher proportion of alcoholic and HTG-AP in men than in women and in patients younger than 50 years. Olesenet al[5] reported that the highest incidence rate of severe HTG was observed for men in the age group of 40-49 years, and severe HTG is a well-known risk factor for AP. Therefore, HTG-AP is becoming more prevalent among younger individuals.
AMY was elevated to levels higher than the normal value in 80.1% of patients but only three times higher than the normal in 46.9% of patients. About 50% of patients with HTG-AP showed no significant increase in serum and urine AMY levels[13], which may be due to the presence of AMY activity inhibitors in their plasma; these inhibitors can enter the urine through the kidneys and inhibit urinary AMY activity. In addition, increased TG levels directly affected the determination of AMY. Therefore,the early diagnosis of HTG-AP is more difficult. The diagnostic accuracy of lipase for HTG-AP was 91.83%, while that of AMY was only 40.38%[14]. Thus, we can improve the diagnosis rate of HTG-AP by combining serum AMY and lipase.
In this study, the frequency of SAP (26.9%), organ failure (31.5%), rate of recurrence (32.9%), and mortality (3.0%) of HTG-AP was high. A large multicenter study in China showed higher incidences of local complication (34.13%vs15.72%,P< 0.000) and MSAP (28.85%vs12.95%,P< 0.000) in patients with HTG-AP than in patients without HTG-AP[14]. HTG-AP varied in severity between mild (41%),moderate (26%), and severe (33%)[17]. A foreign study showed that patients with HTG-AP had significantly higher percentages of multiple organ dysfunction syndrome (24.1%vs12.1%,P= 0.009)and cardiovascular failure (17.6%vs4.6%,P< 0.001) compared with biliary AP[26].
Some reports showed a more severe course of AP induced by HTG compared with other causes,whereas other scholars seemed to favor no significant difference in disease severity[28]. Vipperlaet al[17] reported that the risk of recurrent AP attacks was 32%, often in patients with poorly controlled diabetes, alcoholism, and TG levels. Our study showed that the recurrence rate of MSAP was higher than that of SAP, which may be due to insufficient attention and medical care. Different studies reported that the mortality rate of HTG-AP ranged from 0.48% to 7.9%[10,14,26], but the mortality rate for severe cases reached as high as 20%-25%[2].
The high frequency rates of fatty liver disease, diabetes mellitus, and hypertension were found in patients with HTG-AP, with values of 90.6%, 31.0%, and 16.7%, respectively. Patients with HTG-AP were often complicated with metabolic diseases such as diabetes mellitus and obesity, and patients with type 2 diabetes mellitus had an elevated risk of AP compared with patients without diabetes[15].
Comparisons of different grades of severity of HTG-AP
A comparison was conducted among patients with MAP, MSAP, and SAP to investigate the association of the severity of HTG-AP with clinical data and laboratory indicators. Table 2 showed that age and sex had no difference among the three groups (allP> 0.050). Improved Marshall score, MCTSI score,baseline TG, baseline AMY, CRP, albumin, aspartate aminotransferase, low-density lipoproteincholesterol, urea nitrogen, creatinine, calcium, hemoglobin, and free triiodothyronine were significantly different among patients with different grades of severity of HTG-AP (allP< 0.050). Multivariate logistic regression analysis confirmed that high CRP (P= 0.005, OR = 1.011, 95%CI: 1.003-1.019), low calcium (P= 0.003, OR = 0.016, 95%CI: 0.001-0.239), and low albumin (P= 0.023, OR = 0.821, 95%CI:0.693-0.973) were risk factors of severe HTG-AP.
CRP, serum calcium, and serum albumin are well-known predictors of severe AP with non-HTG-AP and are widely used in its early detection. Experts suggested that CRP levels > 150 mg/L 48 h after the onset of symptoms have a high sensitivity for predicting the severity of AP[29]. Yuet al[30] reported that patients with HTG-AP had lower serum ionized calcium associated with a higher risk of developing SAP. Chenet al[31] confirmed that low serum albumin (P= 0.004, OR = 3.362, 95%CI:1.492-8.823) and high CRP (P= 0.005, OR = 3.061, 95%CI: 1.407-6.659) were risk factors of moderately severe to severe HTG-AP.
Our study showed that the predictors of SAP with HTG-AP were similar to those of AP with other etiologies including alcoholic and biliary AP.
Comparisons among different treatments
Reducing serum TG levels quickly is crucial in the early treatment of HTG-AP. This method mainly includes two categories of routine treatment, and blood purification had been implemented for the patients with HTG-AP. Currently, the TG levels should be reduced to below 500 mg/dL as soon as possible; when follow-up TG levels were < 500 mg/dL, an associated reduction in the risk of clinical events and decrease in health care resource use and costs were observed[32]. However, selecting routine treatment or blood purification for patients with HTG-AP after admission to obtain economic cost effectiveness remains controversial. Routine treatments, such as insulin, heparin, and anti-HTG drugs, are effective in reducing TG and have the advantages of non-invasiveness and low cost.
Blood purification includes HP, PE, and continuous renal replacement therapy, which have the disadvantages of invasiveness and expensive. Compared with HP and PE, continuous renal replacement therapy can not only reduce TG rapidly but also remove inflammatory mediators and is more accurate for systemic inflammatory response syndrome control[9]. However, selecting routine treatment or blood purification for patients with HTG-AP after admission in order to obtain economic cost effectiveness remains controversial. Therefore, this study mainly compared the effect of INS and HP on lowering serum TG.
Among patients with MAP and MSAP, a significant decrease in serum TG was found in patients treated with INS (P< 0.000) and HP (P< 0.000) within 48 h. The clearance rates of TG were 57.24% ±33.70% and 56.38% ± 33.61%, respectively (P= 0.927). This rate of decline was similar to a report[33]wherein 22 episodes of HTG-AP had a calculated fall in serum TG of 69.8% within 48 h by conservative management. This finding is also similar to that reported in an HP case series, which demonstrated 49%-80% reductions in serum TG after a single session[34,35]. These reports showed no difference in the rate of TG decline between patients managed with or without HP. This study also showed that length of stay (13.04 ± 7.92 dvs12.35 ± 6.40 d,P= 0.730) did not differ between the two treatments. A large multicenter retrospective study collected 1159 patients with SAP, which included 30 patients with HTGAP, and 10 patients treated with PE compared with 20 patients treated with routine therapy; no additional reduction in TG levels and no improvement in clinical outcomes were detected[36].
Study strengths and limitations
The strengths of this study are the high accuracy of data due to the strict inclusion and exclusion criteria and the use of PSM to avoid test errors. At present, few studies have reported on how to choose the treatment mode of HTG-AP, which is the innovation of this study.
Our study has some important limitations. This study adopted a single-center retrospective design.The incidence of HTG-AP is not universal and can only reflect the situation of our hospital. Data such as body mass index, urine AMY, blood lipase, and blood gas analysis were missing. The choice of treatment had selection bias.
CONCLUSlON
The incidence of HTG-AP exhibited a significant increase, remarkable severity, and recurrent trend. By understanding the characteristics of HTG-AP, we can improve the clinical diagnosis rate and identify patients who are likely to develop severe disease early. Patients with MAP and MSAP can be treated with INS safely and effectively without HP. This work provides a basis for doctors to choose an appropriate treatment plan for patients.
ARTlCLE HlGHLlGHTS

FOOTNOTES
Author contributions:Lin XY, Zeng Y, and Zhang ZC contributed equally to the work; Lin XY, Zeng Y, and Zhang ZC designed the study, collected and analyzed the data, and wrote the manuscript; Lin ZH, Chen LC, and Ye ZS made contributions to conception, design, and coordination of the study and gave final approval of the version to be published; All authors read and approved the final manuscript.
lnstitutional review board statement:The Ethics Committee of Fujian Provincial Hospital approved the study (K2021-02-007).
lnformed consent statement:Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement:The authors declare that they have no conflict of interest.
Data sharing statement:Participants gave informed consent for data sharing.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Xue-Yan Lin 0000-0002-3397-0498; Yi Zeng 0000-0001-9144-8414; Zheng-Chao Zhang 0000-0003-3291-2947; Zhi-Hui Lin 0000-0001-6595-7952; Lu-Chuan Chen 0000-0003-3362-447x; Zai-Sheng Ye 0000-0001-9881-6400.
S-Editor:Zhang H
L-Editor:Filipodia CL
P-Editor:Zhang H
 World Journal of Gastroenterology2022年29期
World Journal of Gastroenterology2022年29期
- World Journal of Gastroenterology的其它文章
- Mechanistic and functional extrapolation of SET and MYND domain-containing protein 2 to pancreatic cancer
- Clinical challenge for gastroenterologists-Gastrointestinal manifestations of systemic mastocytosis: A comprehensive review
- Structural changes of proteins in liver cirrhosis and consequential changes in their function
- Epidemiologic and socioeconomic factors impacting hepatitis B virus and related hepatocellular carcinoma
- Enhanced endoscopic ultrasound imaging for pancreatic lesions: The road to artificial intelligence
- Qingyi decoction attenuates intestinal epithelial cell injury via the calcineurin/nuclear factor of activated T-cells pathway