
Delayed immune-related sclerosing cholangitis after discontinuation of pembrolizumab: A case report
2022-08-12 08:47TakeshiTanakaArataSakaiMasahiroTsujimaeYasutakaYamadaTakashiKobayashiAtsuhiroMasudaYuzoKodama
World Journal of Gastroenterology 2022年28期
Takeshi Tanaka, Arata Sakai,Masahiro Tsujimae, Yasutaka Yamada,Takashi Kobayashi, Atsuhiro Masuda,Yuzo Kodama
Abstract
Key Words: Immune-related adverse events; Sclerosing cholangitis; Delayed immunerelated events; Case report
INTRODUCTION
Secondary sclerosing cholangitis (SC) is a chronic disease characterized by biliary obstruction and can be caused by a variety of specific etiologies such as infections, immune-related factors, toxicity,obstruction, ischemic injury, or drugs, including immune checkpoint inhibitors (ICIs)[1]. ICIs have transformed the treatment landscape for patients with many advanced malignancies but have often been reported to induce adverse events, called immune-related adverse events (irAEs)[2]. The irAEs differ from toxicities caused by cytotoxic or molecularly targeted agents, and the time to toxicity may be delayed and not follow a cyclical pattern, as observed with conventional cytotoxic agents[3]. Biliary system complications, such as irAEs, remain rare, and the management strategy remains unclear. There are a few reports of SC induced by ICIs; however, no cases developed immune-related SC after discontinuation of ICIs. Herein, we report a case of delayed immune-related SC caused by pembrolizumab.
CASE PRESENTATION
Chief complaints
A 68-year-old male patient was admitted to our hospital with abdominal pain and fever.
Imaging examinations
Contrast-enhanced computed tomography and endoscopic ultrasonography revealed swelling and wall thickening of the gallbladder and dilatation of the common bile duct without obstruction (Figure 1A-D).Endoscopic retrograde cholangiopancreatography revealed a dilated common bile duct and irregularly narrowed right intrahepatic bile duct (Figure 1E). Intraductal ultrasonography demonstrated diffuse wall thickening from the right bile duct to the common bile duct (Figure 1F).
Laboratory examinations
Laboratory tests revealed increased levels of white blood cells [10100/μL (3300-8600/μL)], C-reactive protein [4.88 mg/dL (0.00-0.18 mg/dL)], aspartate transaminase [31 U/L (13–30 U/L)], alanine transaminase (ALT) [50 U/L (7–23 U/L)], gamma-glutamyl transpeptidase [205 U/L (13-64 U/L)], and alkaline phosphatase (ALP) [996 U/L (38-113 U/L)]. Total bilirubin was within the normal range [0.7 mg/dL (0.4-1.5 mg/dL)], and blood cultures showed no bacterial infection. The serum immunological markers, including antinuclear antibody, antimitochondrial antibody, and anti-smooth muscle antibody were negative, and the immunoglobulin G4 Level (59 mg/dL) was within the normal range.
Physical examination
The patient's body temperature was 38.9 °C, but the other vital signs were stable. Regarding the pulmonary and cardiac examination, no obvious abnormality was observed. Physical examination revealed epigastric tenderness without rebound tenderness or Murphy’s sign. No jaundice or palpable masses were observed.
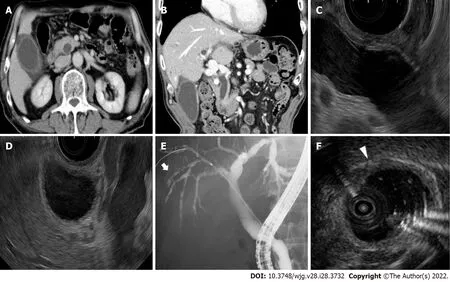
Figure 1 Imaging examinations of the gallbladder and common bile duct. A, B: Contrast-enhanced computed tomography shows swelling and wall thickness of the gallbladder and common bile duct; C, D: Endoscopic ultrasonography shows dilatation of the common bile duct without obstruction and wall thickness of the gallbladder; E: Endoscopic retrograde cholangiopancreatography shows a dilated common bile duct and irregularly narrowed right intrahepatic bile duct (white arrow); F: Intraductal ultrasonography shows the wall thickness from the right bile duct to the common bile duct (white arrowhead).
Personal and family history
No information was available regarding his family history.
History of past illness
The patient has laparoscopic inguinal hernia repair twenty years ago.
History of present illness
The patient was diagnosed with stage IV lung adenocarcinoma (wild-type epidermal growth factor receptor and anaplastic lymphoma kinase, programmed death ligand 1 positive expression) and received first-line treatment with cisplatin and pemetrexed sodium hydrate. Four months after the initiation of first-line chemotherapy, the patient received second-line treatment with pembrolizumab because of disease progression. Three months later (three cycles of pembrolizumab), carboplatin and nab-paclitaxel were administered as third-line treatments. Four months after discontinuation of pembrolizumab (3 mo after initiation of third-line chemotherapy), the patient was admitted to our hospital with abdominal pain and fever.
FINAL DIAGNOSIS
The common bile duct biopsy showed intraepithelial infiltration of lymphocytes, and CD8+T cells were more predominant in the biliary epithelium than CD4+T cells (Figure 2A-C). Percutaneous ultrasonography-guided liver biopsy was also performed for differential diagnosis of other liver diseases. The liver biopsy showed infiltration of predominantly CD8+T cells in the portal area, but the periductal"onion-skin" fibrosis characteristic of primary sclerosing cholangiopathies, and panlobular hepatitis or isolated central zonal necrosis characteristic of acute hepatitis were not detected (Figure 2D-G).According to these imaging and pathological findings, the patient was diagnosed with immune-related SC induced by pembrolizumab.

Figure 2 Pathological findings of the common bile duct and liver. A: Hematoxylin–eosin staining (× 40): Intraepithelial infiltrations of lymphocytes are observed; B and C: CD8 (B) and CD4 (C) staining (× 40): Infiltration of CD8+ T cells are predominant in the biliary epithelium compared to CD4+ T cells; D and E:Hematoxylin–eosin staining: On liver biopsy, inflammation of the hepatic parenchyma is not observed. The periductal "onion-skin" fibrosis is not observed in the portal area (black arrow); F and G: CD8 (F) and CD4 (G) staining (× 200): In a zoomed-in view of the portal area, predominant infiltration of CD8+ T cells, compared with CD4+ T cells, is observed.
TREATMENT
Endoscopic nasobiliary drainage was performed and administration of 25 mg (0.5 mg/kg) of methylprednisolone was initiated. However, grade 3 elevation of ALP and grade 1 elevation of ALT were still present, and the cholangiography findings did not improve.
OUTCOME AND FOLLOW-UP
Because of disease progression, no further treatment was administered, and the patient was referred for palliative care.
DISCUSSION
ICIs enhance antitumor immunity by blocking negative regulators of T cell function that exist on both immune and tumor cells. Although these agents can lead to remarkable responses, their use may also be associated with irAEs. A previous study showed that most irAEs occur in the first few months of treatment, but late-onset toxicity even after ICI discontinuation is also possible[4]. To the best of our knowledge, no case of immune-related SC after pembrolizumab discontinuation has been reported.
Kawakamiet al[5] revealed that immune-related cholangitis was characterized by: (1) Localized extrahepatic bile duct dilation without obstruction; (2) Diffuse hypertrophy of the extrahepatic bile duct wall; (3) A dominant increase in the biliary tract enzymes ALP and gamma-glutamyl transpeptidase relative to the hepatic enzymes aspartate and alanine aminotransferase; (4) Normal or reduced levels of the serum immunological markers antinuclear antibody, antimitochondrial antibody, smooth muscle antibody, and immunoglobulin G4; (5) Pathological findings of biliary tract cluster of differentiation CD8+T cell infiltration from liver biopsy; and (6) A moderate to poor response to steroid therapy. The present case met all these characteristics of immune-related cholangitis.
In contrast, SC developed while carboplatin and nab-paclitaxel were administered. Previous studies reported that chemotherapy-induced SC and drug-induced SC appeared to be one or more strictures of the large bile ducts, mainly the common hepatic duct and the right and left hepatic ducts, usually sparing the common bile duct and smaller intrahepatic ducts[6,7]. Histologically, Weberet al[8] showed that a shift in the CD4+/CD8+cell ratio in favor of CD8+cytotoxic T lymphocytes is useful in discriminating irAEs from other conditions (e.g., autoimmune diseases and drug-induced injury). In our case,an irregularly narrowed right intrahepatic bile duct and infiltration of predominantly CD8+T cells were observed. Therefore, we diagnosed the patient with SC induced by pembrolizumab on the basis of the imaging and pathological findings of previous reports.
Recently, new reports of irAEs emerging after discontinuation of immunotherapy, a clinical diagnostic complex termed delayed immune-related events (DIRE), have surfaced[9]. The first case of DIRE after discontinuation of pembrolizumab was reported in 2013[10], and various late-onset irAEs have also been reported in the literature[11]. Anti-PD-1 antibodies continue to bind to lymphocytes several weeks after the last infusion of PD-1 inhibitors, which explains the development of irAEs after discontinuation of ICI therapy[12]. Although there have been some reports of DIRE after discontinuation of pembrolizumab, no cases of delayed immune-related SC induced by pembrolizumab have been reported.
Previous studies showed that steroid therapy was recommended for the treatment of irAEs, but was not useful for the treatment of immune-related SC[4,13]. Ursodeoxycholic acid (UDCA) and other antiinflammatory agents, including immunomodulators and infliximab, have been considered for the treatment of irAEs, but their efficacy and response have been reported to be insufficient for the treatment of immune-related SC[14,15], and more cases may be needed to evaluate the usefulness of these drugs for immune-related SC. Biliary drainage has been reported to be ineffective for immunerelated SCs[5,16,17]. It remains uncertain why there is a poor response to steroid therapy and biliary drainage for immune-related SC, and further studies are necessary to establish the treatment for immune-related SC.
This indicates that immune-related SC can occur later, similar to other hepatic irAEs. The imaging features and pathological findings of immune-related SC have become almost clear, but the mechanism and onset time of immune-related SC have not been elucidated. Further studies and accumulation of cases are necessary to establish appropriate diagnostic criteria and management strategies, and caution should be exercised for late-onset irAEs after discontinuation of ICIs.
CONCLUSION
Immune-related sclerosing cholangitis may have a late onset, and such cases occurring after discontinuation of immune checkpoint inhibitors should be carefully managed.
FOOTNOTES
Author contributions:All authors contributed to the study conception and design; Tanaka T, Tsujimae M, Yamada Y,and Kobayashi T performed the material preparation, data collection and analysis; Tanaka T wrote the first draft of the manuscript; Sakai A designed the study concept; Masuda A and Kodama Y were involved in study supervision and revised the manuscript; All authors commented on previous versions of the manuscript, read and approved the final manuscript.
Supported byJSPS KAKENHI, No. JP19K07938.
Informed consent statement:Informed consent was obtained from the patient presented in this article.
Conflict-of-interest statement:The authors declare that they have no conflicts of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Japan
ORCID number:Takeshi Tanaka 0000-0003-0490-3453; Arata Sakai 0000-0003-1072-5243; Takashi Kobayashi 0000-0002-9202-7643; Atsuhiro Masuda 0000-0002-2138-1207; Yuzo Kodama 0000-0003-1223-7147.
S-Editor:Ma YJ
L-Editor:A
P-Editor:Ma YJ
 World Journal of Gastroenterology2022年28期
World Journal of Gastroenterology2022年28期
- World Journal of Gastroenterology的其它文章
- Peroxisome proliferator-activated receptor gamma as a therapeutic target for hepatocellular carcinoma:Experimental and clinical scenarios
- Gut microbiota alteration and modulation in hepatitis B virus-related fibrosis and complications:Molecular mechanisms and therapeutic inventions
- Combination approaches in hepatocellular carcinoma: How systemic treatment can benefit candidates to locoregional modalities
- Update on endoscopic ultrasound-guided liver biopsy
- Non-alcoholic fatty liver disease-related hepatocellular carcinoma: Is there a role for immunotherapy?
- Potassium-competitive acid blockers and gastroesophageal reflux disease