
Pediatric case of colonic perivascular epithelioid cell tumor complicated with intussusception and anal incarceration:A case report
2022-07-16 05:51LuanKouWenWenZhengLiJiaXiaoLiWangJiHaiZhouJiaoRongHaoZhuLiuFengYuGao
INTRODUCTION
Colonic perivascular epithelioid cell tumor (PEComa) is rare in clinical practice, especially in children.Intussusception caused by PEComa is even rarer. This report describes a pediatric case of colonic PEComa with intussusception and anal incarceration treated with endoscopic intussusception reduction. This is the first report of such a case. Furthermore, we review the studies on colorectal PEComa indexed in the PubMed database and accessed with the keywords “Colonic PEComa” and“Rectal PEComa”. A total of 30 cases were retrieved, and we provide a detailed analysis and summarization of these cases here.
When my inventory was completed I proudly showed it to a wise elder who had been the mentor4 and spiritual model of my youth. Perhaps I was trying to impress him with my precocious5 wisdom. Anyway, I handed him the list. This , I told him confidently, is the sum of mortal(,) goods. Could a man possess them all, he would be as a god.
CASE PRESENTATION
Chief complaints
A 12-year-old girl presented with abdominal pain as the first manifestation.
History of present illness
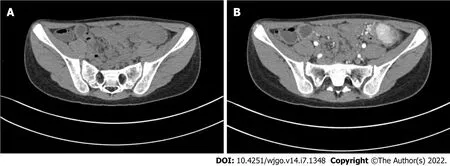
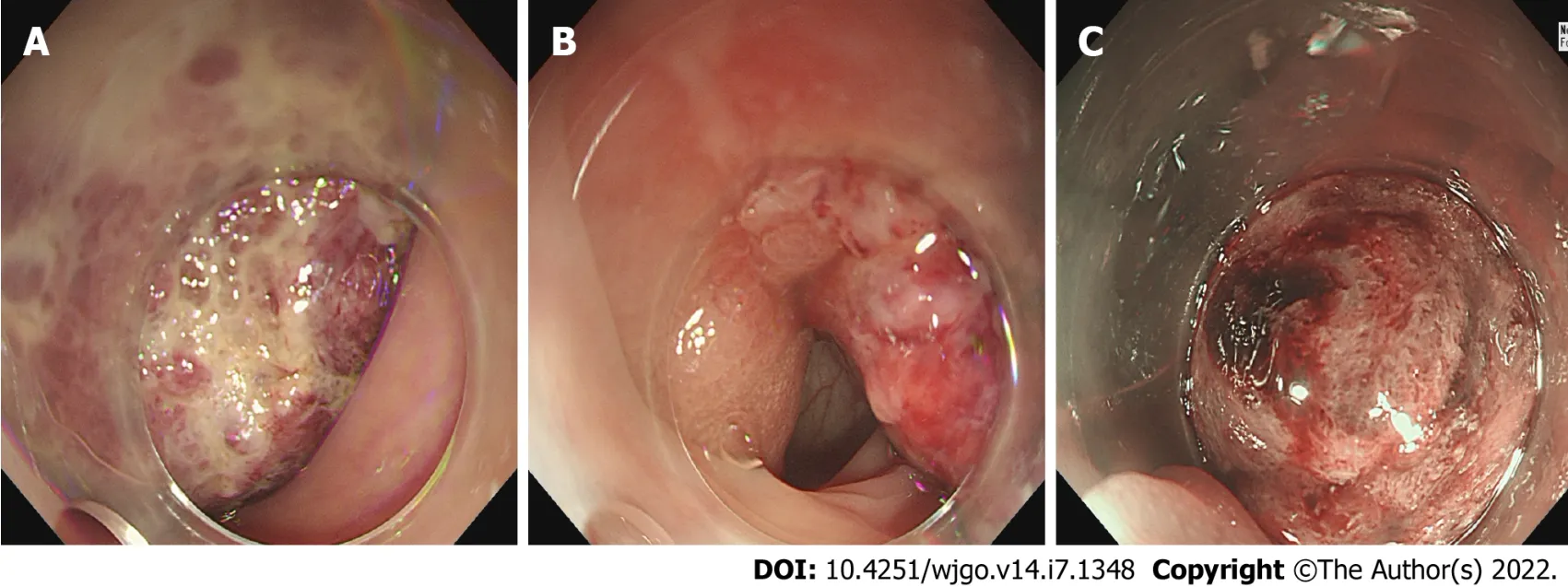
The patient had developed paroxysmal angina pectoris around the umbilicus and lower abdomen 17 d prior, accompanied by nausea and vomiting. Intussusception was diagnosed in a local hospital by ultrasound, and was reduced by air enema. Contrast-enhanced computed tomography (CT) scan showed abnormal enhancement on the left side of the transverse colon with intussusception, which was considered as polyps (Figure 1). Supplementary colonoscopy showed a spherical protuberance of 5 cm in diameter in the transverse colon (Figure 2). The patient was transferred to our hospital for further diagnosis and treatment.
History of past illness
The patient had no previous medical history.
Personal and family history
Results of routine blood, liver function, and coagulation and tumor marker tests were within the normal ranges.
Physical examination
The patient’s vital signs were stable, the abdomen was flat and soft, the left lower abdomen was tender,and there was mild rebound pain.
Laboratory examinations
There was no relevant personal or family history of colon tumor.
Imaging examinations
We performed surgery on the patient, a tumor was found in the transverse colon near the spleen, of about 6 cm × 4 cm × 3 cm in size, with a wide pedicle connected to the bowel. It had good mobility, a hard texture, and a rich blood supply. Edema of the surrounding bowel wall and mesentery was found,separating the mesentery in turn and being ligated to the affected mesenteric vessels. We completely removed the tumor, in addition to about 3 cm of the affected bowel (Figure 3).
MULTIDISCIPLINARY EXPERT CONSULTATION
Combined with the microscopy findings and considering the high risk associated with endoscopy, after discussion with the pediatric surgeons, pediatricians, pathologists, and ultrasonographers, we decided to remove the tumor
general surgery.
FINAL DIAGNOSIS
PEComa was diagnosed by immunohistochemistry.
Informed written consent was obtained from the patients for the publication of this report and any accompanying images.
TREATMENT
Contrast-enhanced CT scan showed abnormal enhancement on the left side of the transverse colon with intussusception, which was considered as polyps (Figure 1). Supplementary colonoscopy showed a spherical protuberance of 5 cm in diameter in the transverse colon (Figure 2).
21.Offered meat and drink:If the king is fasting as a form of penance to take the offered food would be a break of that fast. Because he refused, he shows his piety like his wife does when she prays.Return to place in story.
4.The forest: The forest in fairy tales functions as a place of change. It has all of . . . the symbols of all the dangers with which young people must deal if they are to survive their rite12 of passage and become more responsible adults (Biedermann 141).Return to place in story.
Postoperative pathology showed that the tumor volume was 5.0 cm × 4.5 cm × 3.0 cm and the tumor tissue was located in the submucosa of colon, arranged in an acinar shape with mild cell morphology,no tumor necrosis, and rare instances of mitosis. The immunohistochemical staining results were as follows:Human melanoma black 45 (HMB-45) (+), cluster of differentiation 31 (CD31) (+), cytokeratin (-), melanoma-associated antigen recognized by T cells (-), smooth muscle actin (-), molleya (-), desmin (-),S-100 (-), CD117 (-), and Ki67 (hot spot positive rate < 5%) (Figure 4).


OUTCOME AND FOLLOW-UP
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
DISCUSSION
PEComa represents a group of mesenchymal tumors characterized by perivascular epithelioid cells[1].The etiology is still unclear, and some scholars consider it to be related to the gene mutation of the tuberous sclerosis complex[2]. Histologically, it is mainly composed of blood vessels, spindle cells or epithelioid cells, and fat. The proportion of the three components varies, which leads to large differences in imaging manifestations; it can manifest as poorly differentiated soft tissue tumors or as sclerosing tumors. Its density or signal performance is also closely related to the tumor cell components, but most of these tumors are characterized by a soft tissue mass with a regular shape, clear boundary, high density, and low signal intensity[3].
PEComa diagnosis depends on the pathology and immunohistochemistry findings. According to the World Health Organization classification of digestive system tumors published in 2019, the basic and ideal diagnostic criteria of PEComa are:epithelioid cells and (or) spindle cells in tissues, eosinophilic granular or transparent cytoplasm; nestlike, trabecular or lamellar structure; and co-expression of melanocytes and smooth muscle markers[4]. At present, there is no definitive standard for the diagnosis of benign and malignant PEComa. Folpe
[5] divided the tumors into benign, malignant, and undetermined malignant potential. The malignant features included:tumor size > 5 cm, marginal infiltration, atypical nuclear, mitotic image ≥ 1/50 high-power field, tumor necrosis, and vascular invasion.Benign tumors are considered malignant when they have more than two of the aforementioned features;cases where the diagnosis of malignant potential is uncertain and there is tumor necrosis, including obvious nuclear atypia and high proliferation index, need close follow-up[4]. Considering the pathological results of this case, we considered the tumor to be benign; however, due to the patient’s young age and large tumor volume, close follow-up is still needed.
PEComa is rarely reported. Cecal PEComa was first reported by Birkhaeuser
[6] in 2004. Since then, a total of 30 cases (Table 1)[6-32] of colorectal PEComa have been reported (as determined upon performance of a detailed PubMed search), including 18 females and 12 males, of ages ranging from 5.5-years-old to 69-years-old; most of these patients were adults, and only 7 (23%) were younger than 15-years-old. There was a significant sex difference among the adults but no significant sex difference among the children, consistent with the findings reported by Fadare[33], who proposed that PEComa may be a hormone-dependent tumor. PEComa can occur in all parts of the colon, although they occur more often in the left colon (9 cases in the sigmoid colon[11,12,15,16,18,21,22,26,31], 5 in the rectum[6,7,13,28,29], 3 in the descending colon[9,16,27], 4 in the ascending colon[16,19,30], 7 in the cecum[8,14,20,23-25,32], 1 in the transverse colon[10], and 1 in the right colon[17]).

The diameter of the reported tumors have ranged from 0.8 cm to 8.0 cm. There are no specific symptoms. The tumor can manifest abdominal pain, diarrhea, abdominal distension, hematochezia, or other symptoms of gastrointestinal tumors[19]. The most common clinical manifestation is abdominal pain (44%). Two intussusception cases have been reported. Among the 30 cases, 23 patients underwent surgery and 4 of them given postoperative adjuvant chemotherapy[14,19,26,31]. In total, 5 underwent endoscopic mucosal resection[10,20,24,25,30], and 1 patient underwent endoscopic mucosal dissection after pathological diagnosis. No recurrence was found during follow-up. There have been 10 malignant PEComa cases reported[8,9,11,14,15,19,23,26,28,31]; among them, 2 patients died[9,23] and 2 were lost to follow-up but involving the pancreas and liver metastasis respectively[28,31]. Combined with limited case analysis, the prognosis of malignant PEComa is poor.
With the last poignant34 note still reverberating35 in the air, she lowered her harmonica, placed it in her matronly-styled black purse, and snapped the purse shut
Ileocolic intussusception is one of the most common abdominal emergencies involving children who are less than 3-years-old[34]. The pathophysiology underlying the majority of pediatric intussusception cases is thought to be secondary to a transient viral illness[35]. In adults, 70%-90% of intussusception can be found to have a clear cause, and about 40% are caused by a primary or secondary malignant tumor[36]. Here, we have reported the first pediatric case of benign PEComa in the transverse colon with intussusception, tumor prolapse, and incarceration outside the anus.
At present, benign PEComa has no adjuvant drug treatment. The main treatment for colon PEComa is radical resection, with a good prognosis. Long-term clinical and CT follow-up is recommended.Scheppach
[23] administered sirolimus, doxorubicin, ifosfamide, citabine and docetaxel successively after surgery, which had no obvious effect. Park
[19] reported on a 7-year-old boy with poorly differentiated PEComa in the ascending colon, who received adjuvant interferon-alpha for 1 year after surgery. There was no recurrence after 26 mo of follow-up. That was the first report of interferon-alpha for the treatment of PEComa in the colon. In recent years, an increasing number of targeted drugs have been used in PEComa. Studies have shown that mechanistic target of rapamycin inhibitors are the most effective drugs for the treatment of advanced/metastatic PEComa[37].
CONCLUSION
PEComa is a special type of mesenchymal tissue tumor, which is rarely encountered in the clinic and lacks specific clinical manifestations. The diagnosis depends on pathology and immunohistochemistry findings. Radical resection is the preferred treatment method, and there is no standardized treatment for postoperative adjuvant therapy. Targeted drug application is gradually increasing and has achieved certain results but still needs further research.
She had no sooner done so but her godmother turned them into six37 footmen, who skipped up immediately behind the coach, with their liveries38 all bedaubed with gold and silver, and clung as close behind each other as if they had done nothing else their whole lives. The Fairy then said to Cinderella:
Kou L analyzed the data and wrote the paper; Zheng WW, Jia L, and Gao FY revised the paper;Wang XL, Zhou JH, Hao JR, and Liu Z collected the patient’s clinical data; Gao FY designed the report.
Deep silence reigned21 everywhere, and at last, tired of roaming through empty rooms and galleries, he stopped in a room smaller than the rest, where a clear fire was burning and a couch was drawn22 up closely to it
The authors declare that they have no conflict of interest.
The patient recovered well after the operation, and no abnormalities were found at the 6 mo follow-up.
But she soon thought again of the world above her, for she could not forget the charming prince, nor her sorrow that she had not an immortal soul like his; therefore she crept away silently out of her father’s palace, and while everything within was gladness and song, she sat in her own little garden sorrowful and alone
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
China
Luan Kou 0000-0001-6728-7956; Wen-Wen Zheng 0000-0003-0524-3549; Li Jia 0000-0002-2541-4723;Xiao-Li Wang 0000-0002-8947-4645; Ji-Hai Zhou 0000-0002-4760-6494; Jiao-Rong Hao 0000-0003-0260-8805; Zhu Liu 0000-0002-6785-3820; Feng-Yu Gao 0000-0002-7226-7842.
Chen YL
28.Said the Marquis: Note the son s ability to follow-up on the cat s schemes. He knows the right words and behavior to convince the king and princess of his nobility. It also makes him the accessory as well as benefactor of the cat s schemes.Return to place in story.
A
Chen YL
1 Hornick JL, Fletcher CD. PEComa:what do we know so far?
2006; 48:75-82 [PMID:16359539 DOI:10.1111/j.1365-2559.2005.02316.x]
2 Thway K, Fisher C. PEComa:morphology and genetics of a complex tumor family.
2015; 19:359-368[PMID:26144278 DOI:10.1016/j.anndiagpath.2015.06.003]
3 Tan Y, Zhang H, Xiao EH. Perivascular epithelioid cell tumour:dynamic CT, MRI and clinicopathological characteristics--analysis of 32 cases and review of the literature.
2013; 68:555-561 [PMID:23245276 DOI:10.1016/j.crad.2012.10.021]
4 WHO Classification of tumours Editorial Board. WHO Classification of tumours of the digestive system. 5th ed. Lyon:IARC Press, 2019:485-488
5 Folpe AL, Mentzel T, Lehr HA, Fisher C, Balzer BL, Weiss SW. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin:a clinicopathologic study of 26 cases and review of the literature.
2005; 29:1558-1575 [PMID:16327428 DOI:10.1097/01.pas.0000173232.22117.37]
6 Birkhaeuser F, Ackermann C, Flueckiger T, Guenin MO, Kern B, Tondelli P, Peterli R. First description of a PEComa(perivascular epithelioid cell tumor) of the colon:report of a case and review of the literature.
2004; 47:1734-1737 [PMID:15540307 DOI:10.1007/s10350-004-0637-5]
7 Genevay M, Mc Kee T, Zimmer G, Cathomas G, Guillou L. Digestive PEComas:a solution when the diagnosis fails to"fit".
2004; 8:367-372 [PMID:15614743 DOI:10.1053/j.anndiagpath.2004.08.008]
8 Evert M, Wardelmann E, Nestler G, Schulz HU, Roessner A, Röcken C. Abdominopelvic perivascular epithelioid cell sarcoma (malignant PEComa) mimicking gastrointestinal stromal tumour of the rectum.
2005; 46:115-117[PMID:15656899 DOI:10.1111/j.1365-2559.2005.01991.x]
9 Yamamoto H, Oda Y, Yao T, Oiwa T, Kobayashi C, Tamiya S, Kawaguchi K, Hino O, Tsuneyoshi M. Malignant perivascular epithelioid cell tumor of the colon:report of a case with molecular analysis.
2006; 56:46-50[PMID:16398680 DOI:10.1111/j.1440-1827.2006.01917.x]
10 Baek JH, Chung MG, Jung DH, Oh JH. Perivascular epithelioid cell tumor (PEComa) in the transverse colon of an adolescent:a case report.
2007; 93:106-108 [PMID:17455882]
11 Pisharody U, Craver RD, Brown RF, Gardner R, Schmidt-Sommerfeld E. Metastatic perivascular epithelioid cell tumor of the colon in a child.
2008; 46:598-601 [PMID:18493218 DOI:10.1097/MPG.0b013e318148b65c]
12 Righi A, Dimosthenous K, Rosai J. PEComa:another member of the MiT tumor family?
2008; 16:16-20[PMID:18203778 DOI:10.1177/1066896907309733]
13 Qu GM, Hu JC, Cai L, Lang ZQ. Perivascular epithelioid cell tumor of the cecum:a case report and review of literatures.
2009; 122:1713-1715 [PMID:19719977]
14 Ryan P, Nguyen VH, Gholoum S, Carpineta L, Abish S, Ahmed NN, Laberge JM, Riddell RH. Polypoid PEComa in the rectum of a 15-year-old girl:case report and review of PEComa in the gastrointestinal tract.
2009; 33:475-482 [PMID:19092636 DOI:10.1097/PAS.0b013e31819003d1]
15 Tanaka M, Kato K, Gomi K, Matsumoto M, Kudo H, Shinkai M, Ohama Y, Kigasawa H, Tanaka Y. Perivascular epithelioid cell tumor with SFPQ/PSF-TFE3 gene fusion in a patient with advanced neuroblastoma.
2009; 33:1416-1420 [PMID:19606011 DOI:10.1097/PAS.0b013e3181a9cd6c]
16 Shi HY, Wei LX, Sun L, Guo AT. Clinicopathologic analysis of 4 perivascular epithelioid cell tumors (PEComas) of the gastrointestinal tract.
2010; 18:243-247 [PMID:19124450 DOI:10.1177/1066896908330481]
17 Gross E, Vernea F, Weintraub M, Koplewitz BZ. Perivascular epithelioid cell tumor of the ascending colon mesentery in a child:case report and review of the literature.
2010; 45:830-833 [PMID:20385296 DOI:10.1016/j.jpedsurg.2010.01.015]
18 Freeman HJ, Webber DL. Perivascular epithelioid cell neoplasm of the colon.
2010; 2:205-208 [PMID:21160599 DOI:10.4251/wjgo.v2.i4.205]
19 Park SJ, Han DK, Baek HJ, Chung SY, Nam JH, Kook H, Hwang TJ. Perivascular epithelioid cell tumor (PEComa) of the ascending colon:the implication of IFN-α2b treatment.
2010; 53:975-978 [PMID:21218021 DOI:10.3345/kjp.2010.53.11.975]
20 Maran-Gonzalez A, Baldet P, Costes V. [Polypoid PEComa:case report and literature review].
2011; 31:102-107 [PMID:21601115 DOI:10.1016/j.annpat.2010.07.005]
21 Lee M, Cho KJ, Yu C, Park Y, Kim JC, Kim J, Yu E, Kim MJ. Perivascular epithelioid cell tumor of the sigmoid colon with transcription factor E3 expression.
2012; 16:306-311 [PMID:21546294 DOI:10.1016/j.anndiagpath.2011.01.007]
22 Cho YW, Kim KJ, Ye BD, Byeon JS, Myung SJ, Yang SK, Kim JH. [A case of a perivascular epithelioid cell tumor mimicking colon cancer].
2012; 60:377-381 [PMID:23242022 DOI:10.4166/kjg.2012.60.6.377]
23 Scheppach W, Reissmann N, Sprinz T, Schippers E, Schoettker B, Mueller JG. PEComa of the colon resistant to sirolimus but responsive to doxorubicin/ifosfamide.
2013; 19:1657-1660 [PMID:23539498 DOI:10.3748/wjg.v19.i10.1657]
24 Im S, Yoo C, Jung JH, Choi HJ, Yoo J, Kang CS. Primary perivascular epithelioid cell tumor in the rectum:a case report and review of the literature.
2013; 209:244-248 [PMID:23484779 DOI:10.1016/j.prp.2013.01.001]
25 Kanazawa A, Fujii S, Godai TI, Ishibe A, Oshima T, Fukushima T, Ota M, Yukawa N, Rino Y, Imada T, Ito J, Nozawa A,Masuda M, Kunisaki C. Perivascular epithelioid cell tumor of the rectum:report of a case and review of the literature.
2014; 12:12 [PMID:24410788 DOI:10.1186/1477-7819-12-12]
26 Cheng J, Deng M, Gao J, Tao K. A recurrent perivascular epithelioid cell tumor of sigmoid colon with pancreatic metastasis:an extremely rare case report and review of the literature.
2016; 31:1237-1240 [PMID:26567117 DOI:10.1007/s00384-015-2443-z]
27 Iwamoto R, Kataoka TR, Furuhata A, Ono K, Hirota S, Kawada K, Sakai Y, Haga H. Perivascular epithelioid cell tumor of the descending colon mimicking a gastrointestinal stromal tumor:a case report.
2016; 14:285 [PMID:27842558 DOI:10.1186/s12957-016-1046-7]
28 Lin KH, Chang NJ, Liou LR, Su MS, Tsao MJ, Huang ML. Successful management of perivascular epithelioid cell tumor of the rectum with recurrent liver metastases:A case report.
2018; 97:e11679 [PMID:30075560 DOI:10.1097/MD.0000000000011679]
29 Iwa N, Yutani C, Kobayashi TK. Presence of eosinophilic intracytoplasmic inclusions diagnosed by fine needle aspiration cytology in perivascular epithelioid cell tumor (PEComa) arising from the cecum.
2019; 47:359-361[PMID:30499191 DOI:10.1002/dc.24086]
30 Bennett J, Laury R, Dai H, Walde C, Kasi A. A Curious Case of Colonic Perivascular Epithelioid Cell Tumor:A Unique Diagnosis With Variable Presentations.
2020; 12:e11164 [PMID:33251071 DOI:10.7759/cureus.11164]
31 Cheng HC, Kuo CY, Huang CW, Shih HH, Lin CH, Wang JY. Unusual paediatric sigmoid perivascular epithelioid cell tumour with regional lymph node metastasis treated using gemcitabine and docetaxel:a case report and literature review.
2021; 49:3000605211041509 [PMID:34510959 DOI:10.1177/03000605211041509]
32 Yeon HJ, Sung NS, Roh SJ, Choi WJ, Park YW. PEComa in the rectum:A case report and review of the literature on epithelioid angiomyolipoma.
2021; 86:106301 [PMID:34392019 DOI:10.1016/j.ijscr.2021.106301]
33 Fadare O. Perivascular epithelioid cell tumor (PEComa) of the uterus:an outcome-based clinicopathologic analysis of 41 reported cases.
2008; 15:63-75 [PMID:18418088 DOI:10.1097/PAP.0b013e31816613b0]
34 Applegate KE. Intussusception in children:evidence-based diagnosis and treatment.
2009; 39 Suppl 2:S140-S143 [PMID:19308373 DOI:10.1007/s00247-009-1178-9]
35 Burnett E, Kabir F, Van Trang N, Rayamajhi A, Satter SM, Liu J, Yousafzai MT, Anh DD, Basnet AT, Flora MS, Houpt E, Qazi SH, Canh TM, Rayamajhi AK, Saha BK, Saddal NS, Muneer S, Hung PH, Islam T, Ali SA, Tate JE, Yen C,Parashar UD. Infectious Etiologies of Intussusception Among Children <2 Years Old in 4 Asian Countries.
2020; 221:1499-1505 [PMID:31754717 DOI:10.1093/infdis/jiz621]
36 Akbulut S. Unusual cause of adult intussusception:diffuse large B-cell non-Hodgkin's lymphoma:a case report and review.
2012; 16:1938-1946 [PMID:23242720]
37 Unluoglu S, Bayol U, Korkmaz N, Ozenen B, Ipekci F, Pala EE. Perivascular epithelioid cell tumor of the ileum presenting as diverticulitis.
2012; 2012:476941 [PMID:22953133 DOI:10.1155/2012/476941]
 World Journal of Gastrointestinal Oncology2022年7期
World Journal of Gastrointestinal Oncology2022年7期
- World Journal of Gastrointestinal Oncology的其它文章
- Gut microbiome and pancreatic cancer cachexia:An evolving relationship
- Prospects and applications of enucleation in solid pseudopapillary neoplasms of the pancreas
- Claudin 18.2 is a potential therapeutic target for zolbetuximab in pancreatic ductal adenocarcinoma
- KIFC3 promotes proliferation, migration and invasion of esophageal squamous cell carcinoma cells by activating EMT and β-catenin signaling
- Differences of core genes in liver fibrosis and hepatocellular carcinoma:Evidence from integrated bioinformatics and immunohistochemical analysis
- Efficacy of neoadjuvant chemotherapy for initially resectable colorectal liver metastases:A retrospective cohort study