
Claudin 18.2 is a potential therapeutic target for zolbetuximab in pancreatic ductal adenocarcinoma
2022-07-16 05:51XiWangChengShengZhangXuYuanDongYuanHuBaoJunDuanJunBaiYinYingWuLinFanXinHuaLiaoYeKangPengZhangMengYangLiJiaoXuZhiJunMaoHuiTongLiuXiaoLongZhangLiFeiTianEnXiaoLi
INTRODUCTION
Pancreatic cancer is the eleventh most frequently diagnosed cancer and the sixth most common cause of cancer-related deaths in China, being only slightly lower than the rates reported from the United States and United Kingdom[1]. However, the overall incidence and mortality rates of pancreatic cancer are expected to increase further[2]. Pancreatic ductal adenocarcinoma (PDAC) accounts for more than 90%of all pancreatic neoplasms. Yet, there is no effective screening tool for early detection of PDAC, and patients lack specific clinical symptoms at early stages. Thus, most patients are usually diagnosed at the advanced stage with distant metastases and are not suitable for curable surgery, aggravating its poor prognosis[3]. It is therefore urgent to develop nonsurgical therapeutic approaches for effective treatment of PDAC.
For systemic palliative treatment of unresectable PDAC patients, chemotherapy is the first-line approach. The majority of patients are treated with FOLFIRINOX (5-fluorouracil/irinotecan/oxaliplatin)[4] and gemcitabine-based chemotherapy, including combinations of gemcitabine and nanoparticle albumin-bound paclitaxel (nab-paclitaxel)[5], gemcitabine, and erlotinib[6]. These combination therapies exhibit an improvement in median and 1-year survival rates as compared with gemcitabine alone. However, the chemosensitivity of PDAC is moderate, and as the benefits of adding erlotinib are marginal but the toxicity of the combination is higher, erlotinib has not been widely adopted[6].
Immunotherapy has great success in treating many types of cancers, whereas it has not been very successful against PDAC. Most clinical outcomes of immunotherapy with immune checkpoint inhibitors, chimeric antigen receptor T cells, immunomodulators, and vaccines were not satisfactory[7].Therefore, immunotherapy is not recommended as a conventional treatment by the guidelines for PDAC. However, we cannot totally deny the immunotherapeutic potential. With a deeper level understanding of the PDAC immunology and mechanisms of immunotherapeutic resistance, immunotherapy may achieve great success in treating PDAC. A clinical trial showed that BL-8040, a CXCR4 antagonist, in combination with pembrolizumab and chemotherapy for pancreatic cancer enhanced the objective response rate, disease control rate, and median duration in PDAC[8]. Another study revealed that combination treatment of a vaccine p53MVA and pembrolizumab (an immune checkpoint inhibitor of programmed death protein 1) had higher cure rate or longer survival time than the control group, but there were still many patients who suffered grade 1-2 adverse events, despite the small sample size[9].Therefore, combination immunotherapy with or without chemoradiotherapy may be one of the future directions of immunotherapy application for treating PDAC. Novel treatments and early detection tools are still urgently needed for this highly aggressive and lethal disease.
Claudin 18 (CLDN18) is a highly specific tight junction protein, encoded by the
gene,regulating paracellular barrier functions. Its two isoforms are known as isoform 1 (CLDN18.1) and isoform 2 (CLDN18.2). Expression of CLDN18.2 has been revealed to be confined to short lived differentiated gastric epithelial cells of the primary gastric carcinoma and normal gastric mucosa, which suggesting its potential as a candidate therapeutic target in cancer treatment[10,11]. CLDN18.2 expression has also been reported in PDAC[12,13].
Zolbetuximab is a highly potent and tumor cell-selective therapeutic antibody that directly targets the tight junction molecule CLDN18.2, a proliferation-promoting transmembrane protein[14]. Zolbetuximab is currently in clinical testing. The phase II clinical trial (FAST:NCT01630083) revealed that zolbetuximab combined with first-line chemotherapy significantly improved the overall survival,progression-free survival and the objective response rate with acceptable safety and tolerability in patients with CLDN18.2-positive advanced/recurrent gastric cancers and gastroesophageal junction cancers[15]. Furthermore, health-related quality of life was sustained for a longer duration in patients who received zolbetuximab plus chemotherapy compared with those who received chemotherapy alone[16]. This prompted us to consider clinical testing of zolbetuximab in PDAC. Since few data are available regarding the clinicopathological characteristics of CLDN18.2 expression for PDAC, this study was designed and carried out as a part of the prefeasibility program for such clinical trials.
MATERIALS AND METHODS
Data extraction from multiple databases
Expression of the
gene in normal pancreatic tissue and pancreaticcancer was analyzed using TNMplot.com (https://tnmplot.com/analysis/)[17] and Xena (http://xena.ucsc.edu/compare-tissue/)[18], which allow for online analysis of The Cancer Genome Atlas (TCGA), Genotype-Tissue Expression,and Gene Expression Omnibus (GEO) data. In this study, TCGA and GEO offered the pancreatic tumor samples and solid tissue normal samples from individuals with cancer, while the Genotype-Tissue Expression offered normal tissue from individuals who did not have cancer. In addition, we used KM plotter to assess the effect of CLDN18 on survival in pancreatic cancer (https://kmplot.com/analysis/),which is based on the databases of TCGA, GEO, and European Genome-phenome Archive.
Sample collection
The primary tumor samples and para-cancer tissues as well as normal pancreatic tissues were collected between 2018 and 2020 at the Institute of Pathology of the First Affiliated Hospital of Xi’an Jiaotong University (Xi’an, Shaanxi Province, China). We included patients with pathologically confirmed PDAC.Patients with a tumor type different from PDAC were excluded. Each tissue had gone through gross sectioning and histological detection by qualified pathologists. The date of patients’ deaths was collected from the hospital records. Follow-up data of the patients who were still alive were obtained from the telephone follow-up and hospital records. The histopathological diagnosis and grading followed the recommendations of the World Health Organization, and the tumor stage was confirmed in accordance with the 8
edition of American Joint Committee on Cancer staging system. Sampling of tissues and clinical data for scientific purposes was approved by the ethics committee of The First Affiliated Hospital of Xi’an Jiaotong University. Additionally, tissue microarrays spotted with samples of primary PDAC and para-cancer tissues were bought from Shanghai Zhuo hao Pharmaceutical Technology Co., LTD (Shanghai, China) (Cat. No. PAC1602).
Immunohistochemistry
Immunohistochemistry (IHC) was performed on slides of 4% buffered formalin-fixed paraffinembedded samples. Deparaffinized tissue slice were stained with hematoxylin and eosin. Immunohistochemical CLDN18.2 staining used the anti-CLDN18.2 antibody (Rabbit monoclonal EPR19202, Cat No.ab222512; Abcam, Cambridge, United Kingdom) in 1:500 dilution on a BOND-MAX automated staining system with Leica Bond Polymer Refine Detection Kit (Leica Biosystems, Wetzlar, Germany).
Scoring of CLDN18.2 staining
Scoring of 93 primary PDACs, 86 para-cancer tissues, and 13 normal pancreatic tissues was assessed by using a semi-quantitative pathology histoscore (H-score), defined as a method combined both percentages of positive-expression cells in the tissue slice and immunostaining intensities (hereinafter referred to as IHC-score). The IHC-score was on account of the membranous staining intensity level of CLDN18.2 from 0 to 1+ (weak), 2+ (intermediate), or 3+ (strong). Only membranous staining was retained for scoring. Nuclear and/or cytoplasmic CLDN18.2 expression was just noted but not scored.Tissue was assessed as IHC-score 0 (no staining was detectable), 1+ (faint membranous staining was partially showed), 2+ (moderate membranous staining was observed), or 3+ (strong membranous staining was present in the tissue section). In brief, the H-score was calculated according to the formula:(0 × percentage of immunonegative cells) + (1 × percentage of weakly stained cells) + (2 × percentage of intermediately stained cells) + (3 × percentage of strongly stained cells). Thus, the H-scoring ranged from 0 (a tissue sample that is completely negative) to a maximum of 300 (a tissue sample in which all the cells show a 3+ staining), which can separate samples with a predominantly high staining intensity from samples with a predominantly low staining intensity more distinctively. All samples of this study were assessed by two pathologists working independently. In case of discrepancies in the assessments,the sections were discussed to reach a final agreement.
For the purpose of finding correlations between CLDN18.2 expression and clinicopathological characteristics of PDAC patients, the tissues were divided into two groups according to the median H-score:negative/low (≤ median) and positive/high (> median).
For a moment, Alfred s respect for Kaela s mamma underwent asudden shock, and lessened20 considerably21; but, dazzled by the lightwhich surrounded Kaela, he soon found it quite natural that the oldlady should have no eye for color. After all, it was of very littleconsequence; for Kaela s mamma had the best of all possessions;namely, Kaela herself.
Assessment of heterogeneous expression
During the process of reviewing both IHC-score and H-score, we found the obvious intratumoral heterogeneity in PDAC. Due to lack of accredited guideline to evaluate the heterogeneity between PDAC patients, some literature materials were referenced and we classified the heterogeneity according to the IHC-score, if 3+ and 0 were present meanwhile in one tumor tissue and accounted for more than 50% combined, we thought the strong heterogeneous expression was showed[14]. Additionally, we assessed the immunostaining patterns of these heterogeneous tumors. Some tumor cells of PDAC showed diffusely distribution with low or no IHC staining, which we referred to as “scattered”. Another heterogeneity pattern of tumors with a “downward gradient” pattern displayed an obvious decline in intensity of the immunostaining towards the deep of the tissue.
Statistical analysis
SPSS version 24.0 (IBM Corp., Armonk, NY, United States) was used for statistical analyses. For assessing the correlation between non-ordinal variables, we applied the
test and Fisher’s exact test. To make up for the false discovery rate in the correlations, we used the Simes’ procedure, also known as Benjamini-Hochberg procedure. Multivariate analysis was performed to evaluate if a significant factor correlated to CLDN18.2 expression was an independent factor. The Kaplan-Meier method was used to determine median survival with 95%CIs and Log-rank test was applied to assess the differences between median survivals. Furthermore, Cox’s regression model was performed for the Multivariate survival analysis.
< 0.05 was accepted as demonstration of significant differences.
My first Thanksgiving in prison, I refused to eat. My first birthday I spent alternating between rage and feeling more sorry for myself than ever before. On Christmas, I wouldn t even get out of bed. I stayed under the covers to hide the tears I cried all day.
RESULTS
Identification of gene expression data of CLDN18 in pancreatic cancer from databases
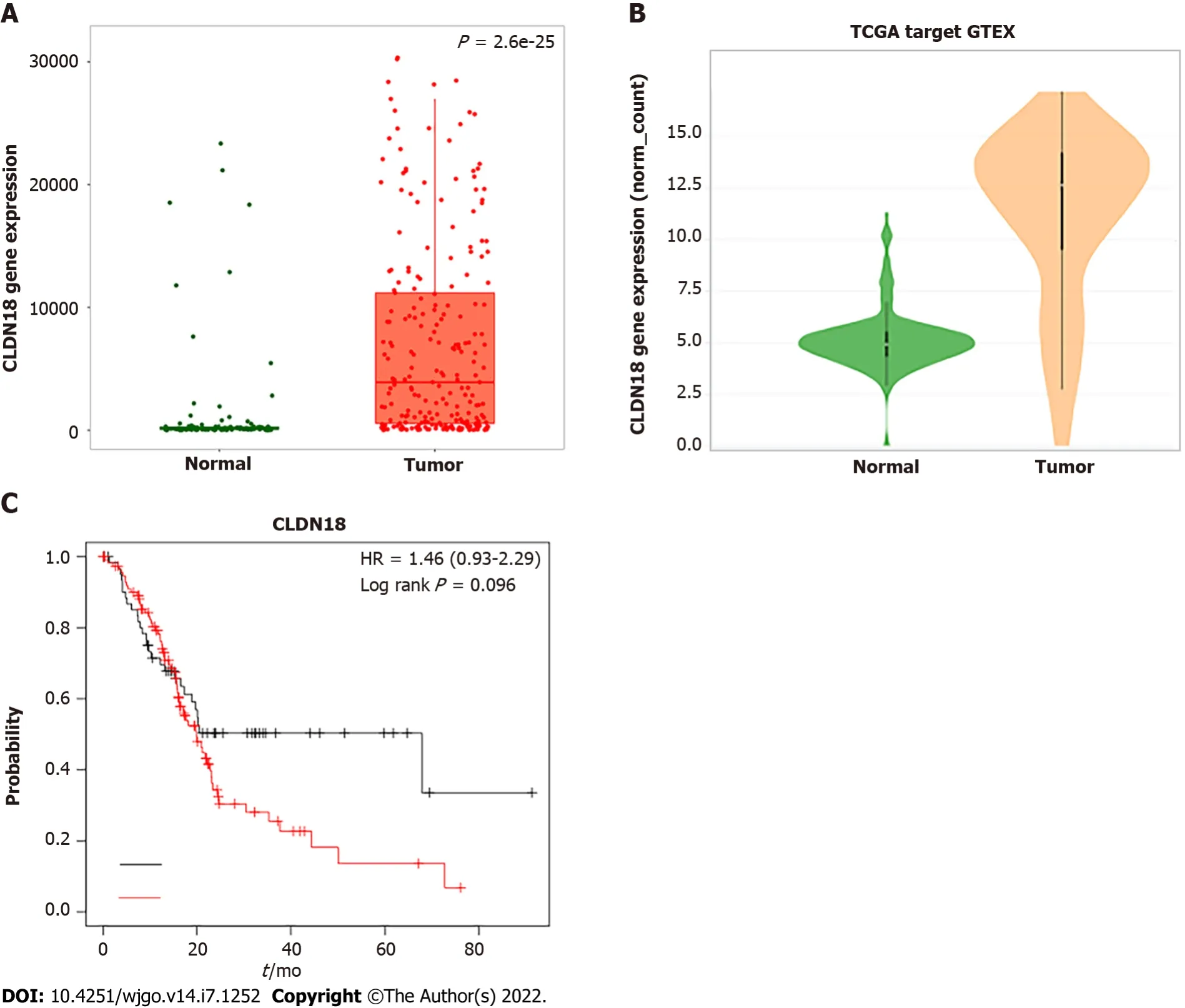
The TNMplot.comanalysis involved 108 normal tissues and 248 pancreatic tumors. We found that the gene expression of
in pancreatic tumors was much higher than that in normal tissues, and the difference was statistically significant (
< 0.01) (Figure 1A). Xena analysis of the gene expression of
in 167 normal tissues and 183 pancreatic tumors yielded results that were consistent with those from TNMplot.com (Figure 1B). KM plotter assessment of the effect of
expression on survival in 177 pancreatic cancer patients revealed no significant correlation between
expression and survival (Figure 1C).
CLDN18.2 expression in non-neoplastic pancreatic tissue
We observed a set of non-neoplastic pancreatic tissue samples (
= 13) for CLDN18.2 expression. All histological cell types and distinct structures of normal pancreatic tissue, such as duct cells, acinar cells,and endocrine cells, were observed. CLDN18.2-specific staining was not detectable in any of the normal pancreatic tissue cells. Representative images are displayed in Supplementary Figure 1.
CLDN18.2 expression in para-cancer tissue
Eighty-six para-cancer tissues of PDAC were analyzed for CLDN18.2 expression. We found that 81(94.2%) cases showed the positive fraction ≥ 1%, in which 32 (39.5%) cases were characterized as strong staining intensities (Table 1).
In our study, almost all tumors showed compositive IHC-intensity with IHC 3+ and IHC 0 were present meanwhile in one tumor tissue, revealing the expression of CLDN18.2 had a high tendency to heterogeneous expression. In order to elaborate the degree of tumor heterogeneity, it was considered that if both strong and negative expressions were existed simultaneously and accounted for more than 50%combined, the tumor showed strong heterogeneity. Nine (9.7%) tumors met these criteria. We assessed the different immunostaining distribution patterns of these heterogeneous tumors. Six (66.7%) PDACs showed a “scattered” pattern, which had diffusely distribution with low or no IHC staining in tumor cells. Three (33.3%) PDACs displayed a “downward gradient”, with weaker staining intensity towards the depth of the tumor. Representative images are displayed in Supplementary Figure 2.
CLDN18.2 expression in primary PDAC
In total, 93 cases of primary PDAC were analyzed for CLDN18.2 expression. The average age was 63.48(51.6%). PDAC samples were poorly differentiated (
grade 3). Twenty-seven (29.0%) cases were classified as pT3/4. Thirty-six (38.7%) cases had already-confirmed lymph node invasion (pN1/2),twenty-three (24.7%) cases were confirmed as nerve invasion, and fourteen (15.1%) cases presented distant metastasis at the time of first diagnosis (Table 2).
As sometimes happened in those days, long before shared custody1(,) and divorce mediation2, we didn t maintain much contact with our natural father. It was hoped that our new stepfather would grow to be the apple of our eyes.
The old clock was going “tick, tick,” and the hands pointed19 to the time of day, but as they passed through the door into the room they perceived that they were both grown up, and become a man and woman

CLDN18.2 correlates with lymph node metastasis, distant metastasis, nerve invasion, and stage
Group comparison analysis revealed that CLDN18.2 correlated with lymph node metastasis, distant metastasis, nerve invasion, and stage (Table 2). In our study, the N category was assessed in 93 cases,including N0 (
= 57), N1 (
= 27), and N2 (
= 9). CLDN18.2 positivity showed the following distribution of N categories:N0 in 23 (40.4%) cases; N1 in 15 (55.6%) cases; and N2 in 8 (88.9%) cases. There was a statistically significant difference between them (
= 0.019). When we stratified the lymph node metastasis, we found the difference also existed (
= 0.034). CLDN18.2 expression was predominantly increased in the cases of lymph node invasion (pN1/2). A similar observation was also made for distant metastasis. Compared to patients with M0, the expression of CLDN18.2 significantly increased in PDAC patients with distant metastases (78.6%
44.3%,
= 0.022). Moreover, we found that 17 cases with nerve invasion showed positive CLDN18.2 expression, while the patients without nerve invasion showed much lower expression (73.9%
38.5%,
= 0.006), the difference between two group was statistically significant.
Furthermore, it is interesting to note that the relative proportion of positive CLDN18.2 expression was not different between the four stage groups (I, II, III and IV). But when we stratified it, the correlation was observed. CLDN18.2 expression was significantly increased in III + IV stages than that in I + II stages (70.4%
40.9%,
= 0.012). The cases with stage IV showed significantly higher CLDN18.2 expression than I + II + III stages (78.6%
44.3%,
= 0.022).
To evaluate if any of the significant factors correlated to CLDN18.2 expression was an independent factor, we performed multivariate analysis. We found that the significant factors of stage, lymph node metastasis, distant metastasis, and nerve invasion related to the expression of CLDN18.2 as independent factors. Corresponding
values were all less than 0.05.
We demonstrated that the expression of CLDN18.2 had no relevance with T category and grading(Table 2). No other clinicopathological characteristic of PDAC patient, for example, age, sex, tumor site,CA199, local infiltration, vascular invasion, or vessel carcinoma embolus, correlated with CLDN18.2 expression.
This he did, but afterwards wished to kiss the Princess s hand as a reward for having been so obliging; but the Fairy Melinette was not going to allow anything of that kind


CLDN18.2 is frequently heterogeneously expressed in PDAC
” Very soon it was said that the prince must marry, and that the beautiful daughter of a neighboring king would be his wife, for a fine ship was being fitted out
CLDN18.2 and survival
CLDN18.2 expression is frequently increased in PDAC patients. Thus, it may act as a potential therapeutic target for zolbetuximab in pancreatic ductal adenocarcinoma.
DISCUSSION
PDAC is still difficult to diagnose and has a poor prognosis. The main aim of this study was to investigate CLDN18.2 expression in a large PDAC patient population using IHC and then find its correlation with diverse clinicopathological characteristics, including survival in order to detect possible distinctive features of CLDN18-positive PDACs and assess whether it is a suitable indication for clinical development of zolbetuximab, the therapeutic antibody directed against CLDN18.2.
Previous studies reported CLDN18 expression in 50%-90% of pancreatic cancer[12,13,19]. These studies involved patients with different cancer types and different stages, and they used different grade staining protocols and various anti-CLDN18 antibodies or sera, which is a drawback because of crossreactivity to CLDN18.1. Furthermore, different approaches to analyze and score CLDN18 positivity status were implemented. Therefore, it was not suitable to completely rely on these data for a clinical development program. To further add to the validity and reliability of the obtained data, we used Hscore to assess the CLDN18.2 expression, which combined both the fraction of stained tumor cells and intensity of cell surface staining. It can separate the sample’s staining intensity more distinctively. Based on this, our study has the following major key findings, which are novel and support indications for clinical testing of zolbetuximab in PDAC patients.
From that day forth2, the girl began a new habit. Her cell phone never shuts down at night. Because she was afraid that she might not be able to hear the phone ring in her sleep, she tried to stay very alert3. As days passed, she became thinner and thinner. Slowly, a gap4 began to form between them.
The ideal therapeutic target should show high and specific expression in the tumor and show a very low or no expression in normal tissues. The majority of PDACs in our study showed a high rate of CLDN18.2 positivity, but all normal pancreatic tissue showed CLDN18.2 negativity. Thus, CLDN18.2 may act as an ideal therapeutic target, and a considerable number of PDAC patients would be eligible for a CLDN18.2-targeting therapeutic approach. However, we need to realize that the expression of a target does not necessarily mean that a patient will definitely benefit from the respective targeting drug.The clinical curative effect may depend on the intensity of expression[20], the fraction of positive tumor cells, or may not be associated at all to the target expression state[21]. Well-controlled clinical trials should be designed to investigate the therapeutic agent of our CLDN18.2-targeting approach. It is noteworthy that almost 86 (92.5%) tumors assessed in this study presented at least 2+ cell surface expression of CLDN18.2, and the majority of tumor tissue displayed a relatively high fraction of positive cells (median was 50%). This indicates that even if the clinical benefit requires high expression of CLDN18.2, a considerable number of PDAC patients will still be eligible.
In addition, the correlation analysis revealed that the fractions of positive cells and the intensities of membrane staining of CLDN18.2 were significantly higher in lymph node-positive tumors, distant metastatic tumors, nerve invasion tumors, and stage III/IV PDAC patients. Lymph node positivity and distant metastasis were independent factors for poor prognosis in PDAC[22]. Moreover, CLDN18.2 expression correlated to cancer survival of PDAC patients with stage III, stage IV, and distant metastasis meaningfully, which was not in accordance with the result from the database (Figure 1C and Figure 3).The reason for this inconsistency may be that the database analyzed the relevance between gene expression and cancer survival, whereas our research explored the relationship between protein expression and cancer survival. The survival data from the database was analyzed but not stratified.This result also needs to be verified in more substantial pancreatic cancer patients. Besides, CLDN18.2 expression was not associated with tumor size, differentiation, localization, CA199, local infiltration,vascular invasion, nor vessel carcinoma embolus. These data revealed that CLDN18.2 might play a role as an oncogene in the development and progression of pancreatic cancer, and the expression of this gene could promote the aggressiveness of tumor cells. Therefore, CLDN18.2 has the potential to act as a risk assessment and as a prognostic indicator for PDAC.

While some researchers have reported weak expression of CLDN18 in normal pancreatic tissue[19],others have denied it. Our study confirmed that CLDN18.2 was not expressed in normal pancreatic tissue including all different cell types prevalent in the pancreas. More interestingly, we found that CLDN18.2 expression was increased in para-cancer tissues and higher in PDAC tissues. This gradual upward trend of CLDN18.2 expression has not been reported before, which suggests that CLDN18.2 is silenced in normal pancreatic tissue but strongly activated during the course of malignant occurrence and development. However, there is little research reporting the molecular mechanism of CLDN18.2.Combined with the previous correlation analysis results, we thus hypothesize that CLDN18.2 may be
This, however, he also got used to, when he saw that they could never hit him, and in this way he flew about all that year, until the troll called him home again, said some strange words to him, and gave him his human shape again
CLDN18.2 presented quite high expression rate in PDAC patients, with 88 (94.6%) PDACs showed positive expression (Table 1), in which most patients showed compositive IHC-intensity. Fifty (56.8%)cases were scored up to IHC 3+, eighty-six (97.7%) cases were scored equivalent to but no more than IHC 2+, seventy-seven (87.5%) cases were no higher than IHC 1+ (representative images are displayed in Figure 2A). The supreme expression of CLDN18.2 IHC 3+ was discovered with 94.0% of tumor cells,observable in 1 case. The IHC-score distribution of CLDN18.2 in this study is exhibited in Figure 2B.Figure 2C summed up the distribution and frequency of the H-scores.
involved in the tumor migration process, but further experiments are needed to test this hypothesis and explore the exact molecular mechanism of CLDN18.2.
Moreover, the differential expression of CLDN18.2 in normal pancreatic tissue and pancreatic neoplasm suggests that CLDN18.2 can be used as a diagnostic marker for PDAC. This has been reported in other studies. Li
[23] reported the sensitivity of CLDN18 for identifying the gastric and pancreatobiliary tract as primary tumor sites was 79% and the specificity was 93%. The positive and negative predictive values were 76% and 94%, respectively, which indicated that CLDN18 represented a sensitive and specific marker for stomach and pancreatobiliary adenocarcinoma that might be a useful diagnostic tool in routine surgical pathology. However, CLDN18.2 heterogeneity poses a challenge to diagnostic evaluations. In the light of distributions of IHC-score and H-score, this research demonstrated a universal phenomenon of CLDN18.2 expression heterogeneity in PDAC (Supplementary Figure 2), and then we describe heterogeneity types, which likely bring huge challenges to scientific explore and clinical practice. For example, one small tumor specimen with a scattered pattern may lead a serious misjudgment of total expression rate. In addition, the occurrence of the “downward gradient” staining pattern that shows obvious decline in intensity of the immunostaining towards the depth of the tissue may have some impact on biopsy within the deep of PDAC tissue specimen, which mainly allow evaluation of the superficial malignant tumor tissues. Therefore, we should obtain as much tissue as possible when taking a biopsy so that the accuracy of diagnosis can be further improved.
Harry met every train for the next three or four days. Of course, the railroad5 lines made a routine6 checkup and the police looked into the case. But nobody was any real help. I could see that they all figured that May had simply played a trick on him. But I never believed that, somehow.
This study suffered from a few limitations that deserve to be underlined. First, our study was limited by the types of samples. We described and illustrated CLDN18.2 expression in PDAC but not in other types of pancreatic tumors, such as adenosquamous carcinoma and pancreatic endocrine neoplasms.Second, we were limited by the numbers of samples. More large-scale studies need to be conducted to further analyze CLDN18.2 expression in PDAC in the future.
CONCLUSION
In general, this research describes a specified illustration for the expression of CLDN18.2 and its relationship with different clinicopathological elements in PDAC. We conclude CLDN18.2 is a potential therapeutic target for the treatment of PDAC.
ARTICLE HIGHLIGHTS
Research background
This study is part of the prefeasibility program for some clinical trials that applied zolbetuximab in PDAC patients.
Research motivation
Zolbetuximab is a highly potent and tumor cell-selective therapeutic antibody that directly targets the tight junction molecule CLDN18.2. Zolbetuximab is currently in clinical testing and has shown good therapeutic effect. This prompted us to consider clinical testing of zolbetuximab in PDAC. Since few data are available for clinicopathological characteristics of the expression of CLDN18.2 in PDAC, this study is part of the prefeasibility program for such clinical trials.
Research objectives
The present study designed to investigate the CLDN18.2 expression in PDAC patients, and subsequently analyze its relevance with diverse clinicopathological characteristics of PDAC, and then propose a novel target for the cancer treatment of PDAC.
Research methods
The databases, including The Cancer Genome Atlas, Genotype-Tissue Expression, Gene Expression Omnibus, and European Genome-phenome Archive, were used to analyze the expression of the CLDN18 gene in normal pancreatic tissue and pancreatic cancer. Immunohistochemistry was used to analyze the expression of CLDN18.2 in 93 primary PDACs, 86 para-cancer tissues, and 13 normal pancreatic tissues. Immunostained tissues were assessed applying the histoscore and subsequently fell into two groups according to detection of any or no CLDN18.2 expression. Furthermore, the correlations between CLDN18.2 expression and diverse clinicopathological characteristics, including survival, were investigated.
Research results
Reports found in the searched databases showed that the gene expression of CLDN18 in pancreatic tumors was much higher than that in normal tissues. Moreover, the difference was statistically significant (P < 0.01), and there was no significant correlation between CLDN18 expression and survival in pancreatic cancer patients. CLDN18.2 was expressed in 88 (94.6%) PDACs. Of these tumors, 50(56.8%) cases showed strong immunostaining. The para-cancer tissues were positive in 81 (94.2%) cases,in which 32 (39.5%) cases were characterized as having strong staining intensities. Normal pancreatic tissue showed only weak immunostaining. CLDN18.2 expression significantly correlated with lymph node metastasis, distant metastasis, nerve invasion, stage, and survival of PDAC patients, while there was no correlation between CLDN18.2 expression and localization, tumor size, patient age and sex, nor any other clinicopathological characteristic.
Research conclusions
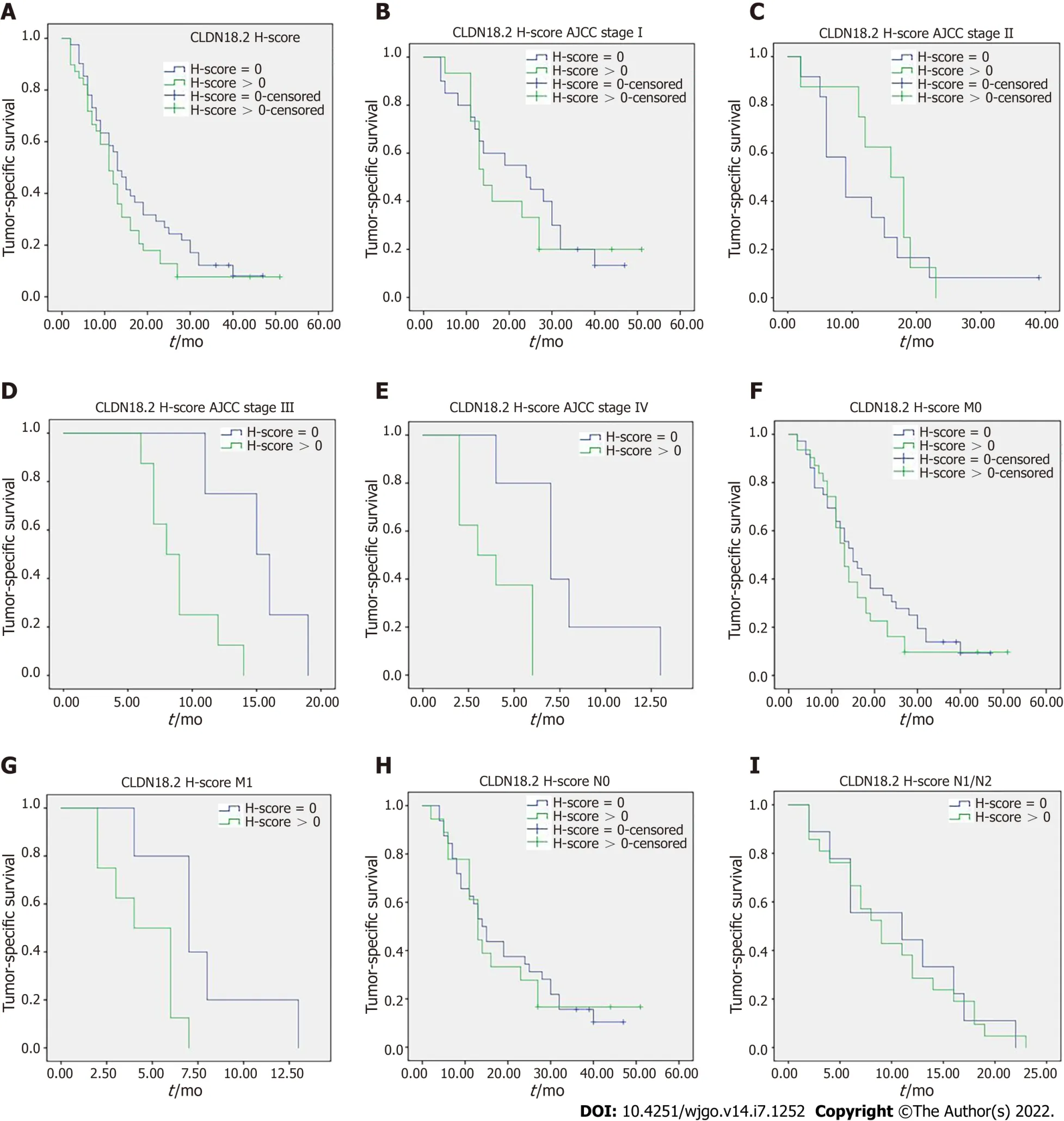
Tumor-specific survival data were available in 80 cases and no correlation was discovered between the cancer specific survival and expression of CLDN18.2 (Figure 3A). Nevertheless, when stratified analysis was applied to verify the influence of diverse CLDN18.2 expression on various tumor stages (American Joint Committee on Cancer) and different N category and M category, the correlation was discovered.The study revealed that the expression of CLDN18.2 correlated with cancer survival of PDAC patients with stage III, stage IV, and distant metastasis meaningfully (Figure 3B-I). This suggests the CLDN18.2-positive patients with late stage and distant metastasis may have a poorer prognosis.
Second, the heroine is accomplishing a difficult task, removing a settled stain from clothing. Psyche, in Cupid and Psyche, has to perform three impossible tasks to prove her devotion to Cupid.
Research perspectives
Pancreatic ductal adenocarcinoma (PDAC) is frequently diagnosed and treated in advanced tumor stages with a poor prognosis. More effective screening programs and novel therapeutic means are urgently needed. The tight junction protein claudin 18.2 (CLDN18.2) has been proved as a novel candidate drug target for cancer treatment, and zolbetuximab (formerly known as IMAB362) has been developed against CLDN18.2. Due to the few data available for clinicopathological characteristics of CLDN18.2 expression in PDAC, this study was performed to evaluate CLDN18.2 expression and to determine whether it can act as a potential therapeutic target for PDAC patients.
After nearly a year, a telegraph came with a plan to make his life complete. Mr. Henderson had agreed to send his daughter to Edward in America. Because she was a hardworking young woman with a good mind for business, she would work alongside Edward for a year to help the mining business grow. By then both families could afford to come to America for their wedding.
The authors would like to acknowledge all staff members of the department of Cancer Precision Medicine, Med-X Institute for skillful technical assistance.
Wang X, Zhang CS, Dong XY, Duan BJ, Bai J, Wu YY and Li EX designed and coordinated the study; Wang X, Hu Y, Kang Y, Li MY, Xu J and Zhang P performed the experiments and acquired and analyzed the data; Fan L and Liao XH supervised the study design and collected the clinical sample; Wang X and Zhang CS interpreted the data and wrote the manuscript; All authors contributed to the critical revisionfor important intellectual content and provided final approval of the manuscript.
Grannonia, who saw her hopes dashed to the ground in this cruel way, had recourse to flattery and cunning, weapons which have often stood the sex in good stead, and called out after the fox, Father Fox, you would be quite right to save your skin, if, in the first place, I didn t feel I owed so much to you, and if, in the second, there weren t other foxes in the world; but as you know how grateful I feel to you, and as there are heaps of other foxes about, you can trust yourself to me
the Basic Research Project of Natural Science of Shaanxi Province, No.2020JQ-943, 2021JQ-916 and 2021JQ-914; Research Project of Chinese Society of Clinical Oncology-Sai Sheng Fund, No. Y-2020Sciclone/qn-0181;Science and Technology Support Program of Shaanxi Provincial People’s Hospital, No. 2021JY-26, 2021JY-38, 2021JY-50 and 2021BJ-13; Research Fund Project of Shaanxi Provincial People’s Hospital, No. 2021YJY-18; and China Postdoctoral Science Foundation, No. 2021M702607.
The study was reviewed and approved by the First Affiliated Hospital of Xi’an Jiaotong University Institutional Review Board (No. XJTU1AF2019LSL-C001).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
No additional data are available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
China
Xi Wang 0000-0001-9516-0397; Cheng-Sheng Zhang 0000-0003-4792-7009; Xu-Yuan Dong 0000-0003-2037-7852; Yuan Hu 0000-0003-3267-1565; Bao-Jun Duan 0000-0002-8375-7951; Jun Bai 0000-0002-9063-3631; Yin-Ying Wu 0000-0002-4132-2714; Lin Fan 0000-0001-8260-1886; Xin-Hua Liao 0000-0003-2171-9287; Ye Kang 0000-0002-5735-8295; Peng Zhang 0000-0002-5673-4404; Meng-Yang Li 0000-0001-8270-2994; Jiao Xu 0000-0002-6702-8855; Zhi-Jun Mao 0000-0001-5689-5307; Hui-Tong Liu 0000-0003-4585-7932; Xiao-Long Zhang 0000-0003-3107-7046; Li-Fei Tian 0000-0001-8374-3683; En-Xiao Li 0000-0001-5225-0173.
Zhang H
A
Yu HG
1 Qiu H, Cao S, Xu R. Cancer incidence, mortality, and burden in China:a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020.
2021; 41:1037-1048 [PMID:34288593 DOI:10.1002/cac2.12197]
2 Ilic M, Ilic I. Epidemiology of pancreatic cancer.
2016; 22:9694-9705 [PMID:27956793 DOI:10.3748/wjg.v22.i44.9694]
3 Yu S, Zhang C, Xie KP. Therapeutic resistance of pancreatic cancer:Roadmap to its reversal.
2021; 1875:188461 [PMID:33157162 DOI:10.1016/j.bbcan.2020.188461]
4 Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de la Fouchardière C, Bennouna J, Bachet JB, Khemissa-Akouz F, Péré-Vergé D, Delbaldo C, Assenat E, Chauffert B, Michel P,Montoto-Grillot C, Ducreux M; Groupe Tumeurs Digestives of Unicancer; PRODIGE Intergroup. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer.
2011; 364:1817-1825 [PMID:21561347 DOI:10.1056/NEJMoa1011923]
5 Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, Harris M, Reni M, Dowden S, Laheru D, Bahary N, Ramanathan RK, Tabernero J, Hidalgo M, Goldstein D, Van Cutsem E, Wei X, Iglesias J, Renschler MF. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine.
2013; 369:1691-1703 [PMID:24131140 DOI:10.1056/NEJMoa1304369]
6 Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, Murawa P, Walde D, Wolff RA, Campos D,Lim R, Ding K, Clark G, Voskoglou-Nomikos T, Ptasynski M, Parulekar W; National Cancer Institute of Canada Clinical Trials Group. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer:a phase III trial of the National Cancer Institute of Canada Clinical Trials Group.
2007; 25:1960-1966 [PMID:17452677 DOI:10.1200/JCO.2006.07.9525]
7 Wu J, Cai J. Dilemma and Challenge of Immunotherapy for Pancreatic Cancer.
2021; 66:359-368 [PMID:32140943 DOI:10.1007/s10620-020-06183-9]
8 Bockorny B, Semenisty V, Macarulla T, Borazanci E, Wolpin BM, Stemmer SM, Golan T, Geva R, Borad MJ, Pedersen KS, Park JO, Ramirez RA, Abad DG, Feliu J, Muñoz A, Ponz-Sarvise M, Peled A, Lustig TM, Bohana-Kashtan O, Shaw SM, Sorani E, Chaney M, Kadosh S, Vainstein Haras A, Von Hoff DD, Hidalgo M. BL-8040, a CXCR4 antagonist, in combination with pembrolizumab and chemotherapy for pancreatic cancer:the COMBAT trial.
2020; 26:878-885 [PMID:32451495 DOI:10.1038/s41591-020-0880-x]
9 Chung V, Kos FJ, Hardwick N, Yuan Y, Chao J, Li D, Waisman J, Li M, Zurcher K, Frankel P, Diamond DJ. Evaluation of safety and efficacy of p53MVA vaccine combined with pembrolizumab in patients with advanced solid cancers.
2019; 21:363-372 [PMID:30094792 DOI:10.1007/s12094-018-1932-2]
10 Sahin U, Koslowski M, Dhaene K, Usener D, Brandenburg G, Seitz G, Huber C, Türeci O. Claudin-18 splice variant 2 is a pan-cancer target suitable for therapeutic antibody development.
2008; 14:7624-7634 [PMID:19047087 DOI:10.1158/1078-0432.CCR-08-1547]
11 Türeci O, Koslowski M, Helftenbein G, Castle J, Rohde C, Dhaene K, Seitz G, Sahin U. Claudin-18 gene structure,regulation, and expression is evolutionary conserved in mammals.
2011; 481:83-92 [PMID:21571049 DOI:10.1016/j.gene.2011.04.007]
12 Wöll S, Schlitter AM, Dhaene K, Roller M, Esposito I, Sahin U, Türeci Ö. Claudin 18.2 is a target for IMAB362 antibody in pancreatic neoplasms.
2014; 134:731-739 [PMID:23900716 DOI:10.1002/ijc.28400]
13 Türeci Ӧ, Mitnacht-Kraus R, Wöll S, Yamada T, Sahin U. Characterization of zolbetuximab in pancreatic cancer models.
2019; 8:e1523096 [PMID:30546962 DOI:10.1080/2162402X.2018.1523096]
14 Dottermusch M, Krüger S, Behrens HM, Halske C, Röcken C. Expression of the potential therapeutic target claudin-18.2 is frequently decreased in gastric cancer:results from a large Caucasian cohort study.
2019; 475:563-571[PMID:31332522 DOI:10.1007/s00428-019-02624-7]
15 Sahin U, Türeci Ö, Manikhas G, Lordick F, Rusyn A, Vynnychenko I, Dudov A, Bazin I, Bondarenko I, Melichar B,Dhaene K, Wiechen K, Huber C, Maurus D, Arozullah A, Park JW, Schuler M, Al-Batran SE. FAST:a randomised phase II study of zolbetuximab (IMAB362) plus EOX versus EOX alone for first-line treatment of advanced CLDN18.2-positive gastric and gastro-oesophageal adenocarcinoma.
2021; 32:609-619 [PMID:33610734 DOI:10.1016/j.annonc.2021.02.005]
16 Lordick F, Al-Batran SE, Ganguli A, Morlock R, Sahin U, Türeci Ö. Patient-reported outcomes from the phase II FAST trial of zolbetuximab plus EOX compared to EOX alone as first-line treatment of patients with metastatic CLDN18.2+gastroesophageal adenocarcinoma.
2021; 24:721-730 [PMID:33755863 DOI:10.1007/s10120-020-01153-6]
17 Bartha Á, Győrffy B. TNMplot.com:A Web Tool for the Comparison of Gene Expression in Normal, Tumor and Metastatic Tissues.
2021; 22 [PMID:33807717 DOI:10.3390/ijms22052622]
18 Goldman MJ, Craft B, Hastie M, Repečka K, McDade F, Kamath A, Banerjee A, Luo Y, Rogers D, Brooks AN, Zhu J,Haussler D. Visualizing and interpreting cancer genomics data
the Xena platform.
2020; 38:675-678[PMID:32444850 DOI:10.1038/s41587-020-0546-8]
19 Tanaka M, Shibahara J, Fukushima N, Shinozaki A, Umeda M, Ishikawa S, Kokudo N, Fukayama M. Claudin-18 is an early-stage marker of pancreatic carcinogenesis.
2011; 59:942-952 [PMID:21832145 DOI:10.1369/0022155411420569]
20 Van Cutsem E, Bang YJ, Feng-Yi F, Xu JM, Lee KW, Jiao SC, Chong JL, López-Sanchez RI, Price T, Gladkov O, Stoss O, Hill J, Ng V, Lehle M, Thomas M, Kiermaier A, Rüschoff J. HER2 screening data from ToGA:targeting HER2 in gastric and gastroesophageal junction cancer.
2015; 18:476-484 [PMID:25038874 DOI:10.1007/s10120-014-0402-y]
21 Eich ML, Athar M, Ferguson JE 3rd, Varambally S. EZH2-Targeted Therapies in Cancer:Hype or a Reality.
2020; 80:5449-5458 [PMID:32978169 DOI:10.1158/0008-5472.CAN-20-2147]
22 Silvestris N, Brunetti O, Bittoni A, Cataldo I, Corsi D, Crippa S, D'Onofrio M, Fiore M, Giommoni E, Milella M, Pezzilli R, Vasile E, Reni M. Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up of Exocrine Pancreatic Ductal Adenocarcinoma:Evidence Evaluation and Recommendations by the Italian Association of Medical Oncology (AIOM).
2020; 12 [PMID:32599886 DOI:10.3390/cancers12061681]
23 Li WT, Jeng YM, Yang CY. Claudin-18 as a Marker for Identifying the Stomach and Pancreatobiliary Tract as the Primary Sites of Metastatic Adenocarcinoma.
2020; 44:1643-1648 [PMID:32925194 DOI:10.1097/PAS.0000000000001583]
 World Journal of Gastrointestinal Oncology2022年7期
World Journal of Gastrointestinal Oncology2022年7期
- World Journal of Gastrointestinal Oncology的其它文章
- Gut microbiome and pancreatic cancer cachexia:An evolving relationship
- Prospects and applications of enucleation in solid pseudopapillary neoplasms of the pancreas
- KIFC3 promotes proliferation, migration and invasion of esophageal squamous cell carcinoma cells by activating EMT and β-catenin signaling
- Differences of core genes in liver fibrosis and hepatocellular carcinoma:Evidence from integrated bioinformatics and immunohistochemical analysis
- Efficacy of neoadjuvant chemotherapy for initially resectable colorectal liver metastases:A retrospective cohort study
- Increased 5-hydroxymethylcytosine is a favorable prognostic factor of Helicobacter pylori-negative gastric cancer patients