
Association between HLA alleles and sub-phenotype of childhood steroid-sensitive nephrotic syndrome
2022-07-09 02:09HaoLeeLiWangFenFenNiXueYingYangShiPinFengXiaoJieGaoHuanChiYeTaoLuoXueLanChenBaoHuiYangJunLiWanJiaJiaoDaoQiWuGaoFuZhangMoWangHaiPingYangHanChanQiuLi
World Journal of Pediatrics 2022年2期
Hao Lee · Li Wang · Fen-Fen Ni · Xue-Ying Yang · Shi-Pin Feng · Xiao-Jie Gao · Huan Chi · Ye-Tao Luo ·Xue-Lan Chen · Bao-Hui Yang · Jun-Li Wan · Jia Jiao · Dao-Qi Wu · Gao-Fu Zhang · Mo Wang · Hai-Ping Yang ·Han Chan · Qiu Li
Abstract
Keywords Human leukocyte antigen · Immunoregulation · Mediating effect · Steroid-sensitive nephrotic syndrome · Subphenotypes
lntroduction
Idiopathic renal syndrome (INS) is the most common cause of chronic glomerular disease in children. The occurrence and development of INS could be affected by infection, abnormal lipid metabolism, immune disorders, circulating factors and the use of nonsteroidal antiinflammatory drugs. Childhood INS is with a prevalence of approximately 16 cases per 100,000 children. Nevertheless, existing theories cannot fully account for the pathogenesis and clinical characteristics of this syndrome [ 1– 4].Indeed, steroid therapy is the most common treatment for INS and approximately 80–90% of childhood INS patients achieve remission with such therapy. However, 20–30%of the cases progress to infrequent relapses and without recurrence (SSNSWR), who can be managed by steroids alone. Noteworthily, approximately 50% of children with initial SSNS exhibit decreased hormone sensitivity and increased likelihood of relapse during infection, steroid tapering or soon after discontinuation. These patients require second-line steroid-sparing therapy and can progress to a frequently relapse (i.e., frequently relapse nephrotic syndrome, FRNS) or steroid-dependent course(i.e., steroid-dependent nephrotic syndrome, SDNS) [ 5,6]. Moreover, a small proportion of children with FRNS or SDNS still undergo relapses or exhibit active disease in adulthood, accompanied by long-term adverse effects including renal interstitial damage, hypertension, diabetes, dyslipidemia, cataracts, osteoporosis, fracture, obesity,growth disorders, infertility and tumors.
In recent years, some researches have attached great importance to genetic mechanisms and revealed genetic mutations existing in 20–30% of patients with SRNS. To date, the causative mutations in more than 70 different genes have been identified to participate in renal dysfunction, including slit diaphragms, actin cytoskeletons,mitochondrial proteins involved in the biosynthesis of coenzyme Q10, and basement membranes in glomeruli[ 7– 9]. However, the etiology of most SSNS cases remains unclear, of which immune disorders are considered to be a key factor affecting the occurrence and development[ 10– 12]. It is worth emphasizing that human leukocyte antigen (HLA) allele polymorphisms are associated with a variety of kidney diseases [ 13– 16]. Strong associations among HLA alleles, especially HLA-II alleles, and their susceptibility to SSNS have been reported to be correlated with HLA-DQA1 and HLA-DQB1.
Highly variable HLA, the expression products of human major histocompatibility complex (MHC) molecules, present antigen peptides to T cells, thus triggering activation of immune complexes and regulating immune homeostasis. Intense investigations have identified HLA genes as inherited risk factors for conditions linked with autoimmunity. Previous findings have confirmed that the polymorphisms of HLA alleles could affect constant region peptide-binding grooves, which determines the antigen peptide repertoire [ 17 ]. During the immune response, HLA allele polymorphisms could affect the generation of peptides, antigen binding and antigen presentation, thereby affecting disease progression in SSNS patients. Previous studies on the association between HLA alleles and characteristics of SSNS have mostly focused on the identification of disease-related loci, and the populations included were small and mostly included patients with a single phenotype. Furthermore, a simple comparison of HLA type differences between SSNS patients and healthy controls may exclude the effects of indicators related to disease development and prognosis.Previous studies have highlighted the strong association between HLA and its susceptibility to SSNS [ 18– 23].However, ethnic and regional differences in HLA allele polymorphisms may lead to genetic heterogeneity [ 24].Analysis of the correlation between HLA allele polymorphisms and characteristics of SSNS requires detailed differentiation. Our clinical diagnosis and treatment of SSNS showed significant difference regarding the clinical characteristics between SSNSWR and SDNS/FRNS children, suggesting various genetic characteristics in two groups. Previous studies mostly used polymerase chain reaction (PCR) to type the target alleles, from the earliest PCR-restriction fragment length polymorphism to PCR-sequence specific oligonucleotides and then to the most commonly used PCR-sequence specific primer.These methods have the advantages of simplicity, sensitivity, low sample demand and low cost. However, the typing process has low throughput, is not easy to automate, is prone to errors, and cannot detect new genes and loci. Therefore, limitations remain in the study of diseases and HLA alleles. Compared with traditional HLA analysis methods, next generation sequencing (NGS) has higher resolution and larger sample throughput. Moreover, genetic heterogeneity exists in children with SSNS of different races, regions and clinical phenotypes [ 25– 27].Therefore, the associations among HLA alleles and different clinical phenotypes of SSNS (SSNSWR or SDNS/FRNS) still remain to be further studied. In this study, we used NGS to analyze the association between HLA alleles and SSNSWR and SDNS/FRNS characteristics in Chinese Han children, to explore the differences of HLA allele distribution and carrier frequency among groups, and to explore the potential impact of HLA allele polymorphism on clinical characteristics. Treatment response and prognosis are helpful to drug screening, clinical classification,and individualized treatment.
Methods
Study participants
All samples in this study were collected from children diagnosed with SSNS from Children's Hospital of Chongqing Medical University in China from January 1, 2010 to December 30, 2016. All children in the study met the inclusion and exclusion criteria, and the clinical groups were confirmed by specialized physicians (Supplementary Table 1)[ 28], SSNSWR means the urine protein turned negative after 2 mg/kg/day or 60 mg/m 2 /day of steroids for less than 4 weeks, and no recurrence was found in outpatient followup for more than 3 years. SDNS/FRNS means steroid sensitive, but relapse within 2 weeks after two successive dose reduction or withdrawal. At the same time, it means that the recurrence is more than 2 times in half a year or more than 4 times in 1 year.
This study was registered with the China Clinical Trial Registration Center (registration number:ChiCTR1900023187) and approved by the Ethics Committee of Children's Hospital of Chongqing Medical University.All participants and their guardians understood the content and significance of the study and signed informed consent forms before participating.
Clinical data
Clinical information, including general information, initial examination/test results, drug response, clinical types, and clinical sub-phenotypes (SSNSWR or SDNS/FRNS) were collected by clinicians. Urinary protein levels, clinical manifestations, and treatment response of patients were monitored during follow-up and evaluated, and disease progression was evaluated over time.
Genotyping and correlation analysis
Standard procedures were conducted for DNA isolation,genotyping and quality control. Genotyping was carried out at China National Clinical Research Center (Child Health and Disease) using GenCap-WES Capture Kit (MyGenomics, Beijing). HLA alleles were analyzed by four-digit resolution genotyping using xHLA software, which provides fast and accurate HLA typing from short-read next-generation sequencing (NGS) data. Data for 1835 healthy controls were obtained from the database of Beijing Mygenomics Co., Ltd.(the MyGenostics database). We compared the distributions and carrying frequencies of HLA-I/II alleles in children with different clinical sub-phenotypes of SSNS, studied the association of allele carrier status with the clinical characteristics and prognosis of SSNSWR and SDNS/FRNS, and performed univariant/multivariate logistic regression analyses of disease-related indicators to search for risk factors associated with SDNS/FRNS in association with sex and age. We also investigated the relationship between alleles with a frequency > 1% and risk factors for SDNS/FRNS and analyzed underlying interfactor relationships using SDNS/FRNS riskrelated HLA alleles to reveal possible mechanisms by which HLA alleles affect the prognosis of children with SSNS.
Mediating effect analysis
Mediating effect means that the influence relationship between variables is not a direct causal relationship, but is indirectly affected by one or more variables. At this time,indirect variables are called mediating variables, and this effect mechanism is called mediating effect. In our study,mediating effect analysis was used to study the relationship between HLA alleles, C4 and SDNS/FRNS, the predictor variables were HLA allele (HLA
-B
*15:11, B
*44:03& C
*07:06
), the mediator variables were C4 level, and the outcome variables were SDNS/FRNS patients.Four steps of the mediation analysis were involved in the calculation of the mediating effect as follows: Step 1:shows that the predictor variable determines the outcome(Model Y = βTotX) (βTot = total effect); Step 2: shows that the predictor variable affects the mediator (Model M = β1X)(β1 = indirect effect 1); Step 3 shows that the mediator determines the outcome controlling for the predictor (Model Y = β2M + βDirX) (β2 = indirect effect 2, βDir = direct effect); Step 4: in mediation analyses, testing the significance of the mediation effect is equivalent to testing the null hypothesis H0: β2 = 0 versus the alternative hypothesis Ha: β2 ≠ 0.Statistical analysis
SAS 9.4 and IBM SPSS 25.0 were employed for statistical analysis. All variables were tested for normality. Measurement data with a normal distribution are expressed as the mean ± standard deviation, and comparisons between groups were conducted with Student’st
tests. Measurement data with skewed distributions are described as the median and interquartile range; comparisons between groups were carried out with the Mann–WhitneyU
test. Count data were analyzed by the Chi-square test or Fisher’s exact test, and the results described by case number and rate. Frequencies of HLA alleles were compared between children with different clinical sub-phenotypes of SSNS and healthy controls. A univariate logistic regression model was applied to explore the relationship between HLA alleles and outcomes,and multivariate logistic regression was utilized to explore risk factors for SDNS/FRNS. The results are expressed as odds ratios (OR) or risk ratios plus 95% confidence intervals(95% CIs). Statistical analysis was performed by doubletailed analysis, and the significance level was set as 0.05.A Sobel test was performed to assess the significance of a mediation effect. The false discovery rate (FDR) method was employed to correct theP
value. All statistical analyses were performed using SAS 9.4 software (Copyright ©2016 SAS Institute Inc. Cary, NC, USA).Results
Differences in clinical characteristics between SSNSWR and SDNS/FRNS
The clinical details of the patients screened are presented in Table 1. A total of 241 patients were enrolled in our study, including 125 SSNSWR and 116 SDNS/FRNS, with a median age of 42 months (range 26–71 months) and a sex ratio (male:female) of 2.8:1, which consistent with published studies [ 29]. To investigate the differences in clinical characteristics between SSNSWR and SDNS/FRNS, we compared the clinical indicators closely related to the disease.Compared with SSNSWR, SDNS/FRNS exhibited decreased levels of complement 3 (C3) and complement 4 (C4) at onset (1.19 ± 0.23 vs. 1.08 ± 0.25,P
< 0.001; 0.27 ± 0.12 vs.0.24 ± 0.11,P
= 0.018, respectively). Although proteinuria in both groups received initial sufficient steroid treatment was relieved within 4 weeks, the time to first remission after initial steroid treatment in SDNS/FRNS was significantly longer than that in SSNSWR (9.72 ± 4.59 vs. 13.91 ± 9.59,P
< 0.001).We further conducted related indicators and univariate logistic regression to analyze factors affecting therapy response and prognosis in SSNS (variables withP
< 0.05 in the univariate logistic regression analysis were included in multivariate analysis) (Table 2). After correcting for sex,age at onset and other confounding factors, this study suggested that the significant decreased C4 level in children with SDNS/FRNS, which indicate that it may be an independent risk factor for these patients (P
= 0.008, OR = 0.174,95% CI 0.048–0.630).HLA-A*11:01 is SSNSWR and SDNS/FRNS-associated alleles specific to Chinese Han children
To investigate whether HLA alleles influence susceptibility to SSNSWR and SDNS/FRNS, the total patients of the two groups were matched controls, respectively. Interestingly, our study successfully genotyped 178 HLA alleles including 101 class I (HLA
-A
, 27 alleles;HLA
-B
, 48 alleles andHLA
-C
, 27) and 77 class II (HLA
-DPB1
, 27 alleles;HLA
-DQB1
, 16 alleles andHLA
-DRB1
, 34 alleles) alleles.The distributions of the 6 HLA loci among the healthy control, SSNSWR and SDNS/FRNS are provided in Fig. 1.Among these alleles, 27 were expressed only in SSNSWR,the top 5 alleles with the highest frequency at 6 HLA loci wereHLA
-DPB1
*05:01
(66.40%),HLA
-A
*11:01
(52.00%),HLA
-DQB1
*03:01
(36.00%),HLA
-DQB1
*03:03
(30.40%)andB
*46:01
(28.00%); 24 were only expressed in SDNS/FRNS and the top 5 alleles with the highest frequency wereHLA
-DPB1
*05:01
(56.03%),HLA
-A
*11:01
(52.59%),HLADQB1
*03:01
(31.90%),HLA
-DQB1
*03:03
(31.90%) andHLA
-DRB1
*09:01
(30.07%). Compared with the control,the frequency of theHLA
-A
*11:01
allele was significantly higher in the SSNSWR and SDNS/FRNS (Supplementary Table 2, Fig. 2).Table 1 Compared with SSNSWR, SDNS/FRNS exhibited lower levels of C3 and C4 at onset and longer time to first remission
The eGFR was calculated by the Schwartz formula: GFR (mL/min × 1.73 m 2 ) = 0.413 × Ht/Scr [Scr: 1 mg/dL = 88.4 μmol/L; Ht: height (cm);Scr: serum creatinine (mg/dL)]. Continuous variables with a normal distribution are presented as the mean ± standard deviation; categorical variables or continuous variables with a nonnormal distribution are presented as the median (interquartile range). values lower than 0.01 are shown in bold (SSNSWR vs. SDNS/FRNS). steroid-sensitive nephrotic syndrome without recurrence, steroid-dependent nephrotic syndrome, frequently relapse nephrotic syndrome, estimated glomerular filtration rate, creatinine, uric acid, total cholesterol, triglyceride, immunoglobulin, complement 3, complement 4
Clinical items Overall SSNS P SSNSWR SDNS/FRNS Number 241 125 116 Male, n (%) 182 (75.5) 104 (83.2) 78 (67.2)Age (mon) 42 (26, 71) 42 (27, 69) 41 (25, 72) 0.931 eGFR at onset (mL/min × 1.73 m 2 ) 144.76 ± 51.03 144.86 ± 51.02 144.64 ± 51.25 0.973 Cr (μmol/L) 28.9 (22.0, 37.0) 28 (22, 36) 30.25 (23.50, 38.75) 0.150 UA (μmol/L) 310 (245, 365) 304 (242, 361) 318 (251, 391) 0.200 TC (mmol/mL) 9.82 (8.08, 11.67) 10.00 (8.39, 11.76) 9.47 (7.63, 11.47) 0.221 TG (mmol/mL) 2.79 (1.87, 4.09) 2.91 (1.89, 4.03) 2.72 (1.87, 4.11) 0.762 IgG (g/L) 2.67 (1.77, 3.92) 2.54 (1.87, 3.53) 2.85 (1.61, 4.38) 0.601 IgA (g/L) 1.04 (0.72, 1.37) 1.00 (0.68, 1.30) 1.07 (0.76, 1.42) 0.339 IgM (g/L) 1.75 (1.35, 2.38) 1.77 (1.38, 2.22) 1.74 (1.34, 2.47) 0.741 IgE (IU/mL) 313.32 (80.60, 743.15) 311.86 (79.40, 681.41) 324.69 (83.55, 818.65) 0.743 C3 at onset (g/L) 1.14 ± 0.24 1.19 ± 0.23 1.08 ± 0.25 < 0.001 C4 at onset (g/L) 0.26 ± 0.11 0.27 ± 0.12 0.24 ± 0.11 0.018 Time to first remission (d) 11.74 ± 7.7 9.72 ± 4.59 13.91 ± 9.59 < 0.001
Table 2 Complement 4 at onset level indicating that it may be an independent risk factor for SDNS/FRNS
Single-factor logistic regression analysis of factors relevant to clinical practice was carried out. Factors with < 0.05 or that were influential in the univariate analysis were included in the multivariate logistic regression analysis to identify independent risk factors for SDNS/FRNS in SSNS. values lower than 0.05 are shown in bold. steroid-dependent nephrotic syndrome, frequently relapse nephrotic syndrome, estimated glomerular filtration rate, blood urea nitrogen, creatinine, uric acid, total cholesterol,triglyceride, immunoglobulin, high density lipoprotein,low density lipoprotein, complement 3, complement 4,odds ratio, confidence interval
Predictors P OR 95% CI Single factor logistic regression Age (mon) 0.750 1.001 0.994, 1.009 eGFR at onset (mL/min × 1.73 m 2 ) 0.973 1.000 0.995, 1.005 BUN (mmol/mL) 0.089 1.069 0.990, 1.154 Cr (μmol/L) 0.095 1.011 0.998, 1.024 UA (mol/L) 0.064 1.002 1.000, 1.004 TC (mmol/mL) 0.365 0.962 0.885, 1.046 TG (mmol/mL) 0.882 0.991 0.876, 1.120 HDL (mmol/mL) 0.068 1.379 0.977, 1.947 LDL (mmol/mL) 0.020 0.893 0.811, 0.982 IgG (g/L) 0.602 1.035 0.910, 1.176 IgA (g/L) 0.503 1.144 0.772, 1.694 IgM (g/L) 0.628 1.085 0.780, 1.511 IgE (IU/mL) 0.325 1.000 1.000, 1.001 C3 at onset (g/L) 0.001 0.138 0.045, 0.427 C4 at onset (g/L) 0.023 0.048 0.004, 0.659 Multiariable logistic regression Age (mon) 0.994 1.000 0.992, 1.008 eGFR at onset (mL/min × 1.73 m 2 ) 0.713 0.999 0.992, 1.005 LDL (mmol/mL) 0.016 0.883 0.797, 0.977 C4 at onset (g/L) 0.008 0.174 0.048, 0.630
Risk- and protection-HLA alleles for SSNSWR and SDNS/FRNS
In order to confirm the region-specific susceptibility HLA alleles that associated with steroid dependent and frequent relapse, we further indirectly compared patients’group (SSNSWR and SDNS/FRNS) with the control.After FDR correction, 6 loci showed statistical significance (DQB1
*06:02
,A
*11:01
,B
*15:02
,DPB1
*107:01
,A
*02:01
,A
*02:03
;P
-FDR < 0.01). Taken together, these results indicated thatHLA
-A
*11:01
,HLA
-B
*15:02
andHLA
-DPB1
*107:01
are risk alleles for SSNSWR but thatHLA
-DQB1
*06:02
is a protective allele. In SDNS/FRNS,HLA
-A
*02:03
andHLA
-A
*11:01
are risk alleles, butHLAA
*02:01
andHLA
-DQB1
*06:02
are protective. The details of the difference in HLA allele frequency are listed in Table 3.Furthermore, we also found that compared with the control,both SSNSWR and SDNS/FRNS exhibited differential frequency of the allelesHLA
-A
*11:01
andHLA
-DQB1
*06:02
,with high-frequency ofHLA
-A
*11:01
and low-frequency ofHLA
-DQB1
*06:02
in SSNSWR and SDNS/FRNS (Fig. 3).These findings suggest thatHLA
-A
*11:01
andHLADQB1
*06:02
are potential risk/protective alleles. Nevertheless, no FDR-adjusted significance was observed between SSNSWR and SDNS/FRNS.HLA alleles influence the clinical features of SSNSWR and SDNS/FRNS
To explain the relationship between HLA system and patients’group (SSNSWR and SDNS/FRNS), we have further analyzed the effect of different alleles on clinical characteristics in these two groups. The results showed that the carrier status of HLA-I and HLA-II alleles affects the onset age, immune status, complement levels and the time to first remission in each group and the HLA-I (HLA
-A
,HLA
-B
, andHLA
-C
) alleles were the most common among the two groups (Table 4).HLA-B*15:11, HLA-B*44:03 and HLA-C*07:06 act an intermediary role in SDNS/FRNS
Although several HLA alleles were differentially observed in patient’s group (SSNSWR and SDNS/FRNS) compared with healthy control, there was no FDR-adjusted significance was detected between SSNSWR and SDNS/FRNS. These results suggested an indirect regulation/modification mechanism by which HLA alleles affect the development of SSNS in children with different clinical sub-phenotypes. In order to explore this possible mechanism, we conducted a mediating effect analysis.Based on logistic regression analysis model,HLA
-B
*15:11
,HLA
-B
*44:03
andHLA
-C
*07:06
correlated significantly with the C4 level in SDNS/FRNS (Table 5). Interestingly, this result is consistent with above result that C4 is an independent risk factor for SDNS/FRNS.
Fig. 1 The distribution of HLA-I/II alleles and their six loci were average among the healthy control, SSNSWR and SDNS/FRNS. HLA human leukocyte antigen, SSNSWR steroid-sensitive nephrotic syndrome without recurrence,SDNS steroid-dependent nephrotic syndrome, FRNS frequently relapse nephrotic syndrome

Fig. 2 The distributions of the top five HLA alleles with the highest frequencies across healthy control, SSNSWR and SDNS/FRNS and the HLA-A*11:01 allele is highly expressed in SSNSWR and SDNS/FRNS. HLA human leukocyte antigen, SSNSWR steroid-sensitive nephrotic syndrome without recurrence, SDNS steroid-dependent nephrotic syndrome, FRNS frequently relapse nephrotic syndrome.† P < 0.01, ‡ P < 0.001
Discussion
Previous studies have shown that HLA allele polymorphism is closely related to the susceptibility, development and prognosis of SSNS. At present, the research on the correlation between HLA and SSNS at home and abroad mainly focuses on the prediction of high-risk genes. SinceHLA
-DR7
was first reported as the risk locus of SSNS in the 1980s, the correlation betweenHLA
-DQA1, DQB1, DR
/DQ,DRB1
and SSNS have been found and verified, indicating that HLA alleles play an important role in the occurrence and development of SSNS (Supplementary Tables 3, 4).However, previous studies also showed that children with SSNS of different races and regions have genetic heterogeneity in disease susceptibility, treatment effect and prognosis:there is an association betweenHLA
-DR7
antigen and SSNS in Caucasian, Chinese and Arab patients, and the frequency ofHLA
-DQB1:0302
in Japanese population is increased;Bouissou et al. found that the presence ofHLA
-DR7, DR3
/7
orDQ2
suggests that patients with SSNS are very likely to have frequent recurrence/hormone dependence in the course of the disease. In German children with frequent recurrence,carryingHLA
-DR7
suggests that the treatment response to cyclophosphamide or amphetamine is worse, while Indian children with SSNS have higher expression frequency ofHLA
-BW44
, which may affect the efficacy of cyclophosphamide [ 15, 18– 22, 30]. Taken together, it suggests an importance of distinguishing race and region in HLA allele research.Table 3 Differences of HLA allele carrier frequencies
Differences of HLA allele carrier frequencies between control and SSNSWR; differences of HLA allele carrier frequencies between control and SDNS/FRNS. There was no significant difference in the frequency of HLA alleles between SSNSWR and SDNS/FRNS. The allele carrier frequency is expressed as a percentage. values lower than 0.01 are shown in bold ( control vs. SSNSWR, control vs. SDNS/FRNS).human leukocyte antigen, steroid-sensitive nephrotic syndrome without recurrence, steroid-dependent nephrotic syndrome,frequently relapse nephrotic syndrome, false discovery rate, confidence interval, odds ratio
HLA allele Frequency P1 P1_FDR OR1 (95% CI) P2 P2_FDR OR2 (95% CI)Control SSNSWR SDNS/FRNS Protection alleles A*01:01 7.68 1.60 0.00 0.0114 0.0835 0.242 (0.068, 0.862) 0.0019 0.0131 0.051 (0.003, 0.839) A*02:01 25.78 16.80 8.62 0.0253 0.0999 0.592 (0.368, 0.953) 0.0000 0.0006 0.284 (0.149, 0.540) A*30:01 11.39 5.60 3.45 0.0455 0.1365 0.491 (0.231, 1.044) 0.0078 0.0422 0.311 (0.119, 0.807) DQB1*06:02 16.84 4.00 1.72 0.0002 0.0024 0.225 (0.095, 0.534) 0.0000 0.0003 0.108 (0.031, 0.380)Susceptible alleles A*02:03 5.07 12.00 12.93 0.0010 0.0137 2.615 (1.474, 4.639) 0.0003 0.0030 2.846 (1.600, 5.062) A*11:01 33.95 52.00 52.59 0.0000 0.0012 2.105 (1.465, 3.026) 0.0000 0.0006 2.155 (1.480, 3.138) B*15:02 4.63 15.20 10.34 0.0000 1.62E−05 3.749 (2.203, 6.379) 0.0060 0.1451 2.450 (1.307, 4.592) DQB1*05:02 12.59 21.60 18.10 0.0039 0.0315 1.935 (1.240, 3.021) 0.0859 0.3435 1.560 (0.957, 2.543) DPB1*107:01 3.16 11.20 6.90 0.0001 0.0030 3.951 (2.147, 7.270) 0.0550 0.5351 2.380 (1.124, 5.041)
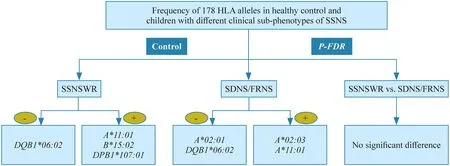
Fig. 3 Differences in HLA allele frequencies between children with different clinical sub-phenotypes of SSNS. HLA-A*11:01, HLAB*15:02 and HLA-DPB1*107:01 were risk alleles for SSNSWR,while HLA-DQB1*06:02 was a protective allele. For SDNS/FRNS,HLA-A*02:03 and HLA-A*11:01 were risk alleles, while HLAA*02:01 and HLA-DQB1*06:02 were protective alleles. HLA human leukocyte antigen, SSNSWR steroid-sensitive nephrotic syndrome without recurrence, SDNS steroid-dependent nephrotic syndrome,FRNS frequently relapse nephrotic syndrome. + risk alleles, − protective alleles
HLA gene complex, one of the most polymorphic regions of the genome, has been reported as the most polymorphic genetic system in humans. By analyzing the genetic and clinical characteristics in SSNSWR and SDNS/FRNS, we found that HLA alleles polymorphisms may affect susceptibilities to different clinical sub-phenotypes of SSNS.HLA
-A
*11:01
may confers susceptibilities to SSNSWR and SDNS/FRNS whileHLA
-DQB1
*06:02
plays a protective role. A lower level of C4 from logistic regression analysis indicated a higher likelihood of steroid dependence and/or recurrence in a long term. Additionally, HLA-I alleles (HLA
-B
*15:11
,HLA
-B
*44:03
, andHLA
-C
*07:06
) are positively correlated with C4 level. Further mediating effect analysis suggested thatHLA
-B
*15:11
,HLA
-B
*44:03
, andHLA
-C
*07:06
may participate in the regulation of immune recognition,response and homeostasis by affecting the C4 level, which indirectly affects the progression and long-term prognosis of children with SDNS/FRNS. Therefore, our study highlighted the association of the HLA alleles with SSNSWR and SDNS/FRNS, investigated the potential impact of HLA alleles polymorphisms on clinical characteristics, treatment response and prognosis, which aids in drug screening, clinical classification and individualization of treatment in Chinese Han children.Table 4 Correlation between HLA different alleles and clinical characteristics of SSNSWR and SDNS/FRNS
human leukocyte antigen, steroid-sensitive nephrotic syndrome without recurrence, steroid-dependent nephrotic syndrome,frequently relapse nephrotic syndrome, low density lipoprotein, complement 3, complement 4, total cholesterol-the time to first remission
HLA allele Clinical items Overall Positive Negative P HLA different alleles and clinical characteristics of SSNSWR B*15:02 Age (mon) 42 (27, 69) 29 (20, 48) 43 (29, 72) 0.042 C3 at onset 1.19 ± 0.23 1.29 ± 0.24 1.17 ± 0.22 0.046 C4 at onset 0.26 (0.20, 0.31) 0.29 (0.24, 0.34) 0.25 (0.19, 0.30) 0.036 DQB1*06:02 Age (mon) 42 (27, 69) 74 (72, 124) 42 (27, 61) 0.044 DPB1*107:01 LDL (mmol/mL) 6.37 (4.48, 8.10) 7.70 (6.56, 9.15) 6.06 (4.32, 7.93) 0.022 C3 at onset 1.19 ± 0.23 1.34 ± 0.21 1.17 ± 0.22 0.008 HLA different alleles and clinical characteristics of SSNSWR and SDNS/FRNS A*02:01 UP(-) (d) 13.91 ± 9.59 11.1 ± 3.07 14.17 ± 9.95 0.032 A*02:03 TC 9.47 (7.63, 11.47) 10.42 (9.48, 13.96) 9.42 (7.41, 11.06) 0.040 A*11:01 Age (mon) 41 (25, 72) 46 (31, 77) 33 (21, 62) 0.039
As one of the most common HLA-I alleles in Asian population,HLA
-A
*11:01
is a susceptible allele often carried in SRNS children in Singapore and end stage renal disease children in China with a high frequency. Studies on the structure of human alloantibodies bound toHLA
-A
*11:01
demonstrated its association with a variety of autoimmune diseases, including rheumatoid arthritis and skin diseases. A high frequency of this allele is also reported in cases of infection and parasitic diseases (for example, toxoplasma gondii infection) [ 31– 33]. Together,these results suggest an important role ofHLA
-A
*11
in the development of T cell-mediated abnormal immune responses [ 34– 36], thusHLA
-A
*11:01
might affect the immune response and participate in the occurrence and development of SSNSWR and SDNS/FRNS by regulating T cell antigen presentation.In this study, the frequency ofHLA
-A
*11:01
in SSNSWR and SDNS/FRNS was significantly higher than that in the healthy control, which suggested it to be a predicting factor for children who are predisposed toward SSNSWR and SDNS/FRNS. UnlikeHLA
-A
*11:01
,HLA
-DQB1
*06:02
was expressed at significantly lower levels in SSNSWR and SDNS/FRNS than that in the control group.HLADQB1
*06:02
allele and its high-frequency haplotypes have been previously reported to play different (risk/protection)roles in diseases of endocrine system, nervous system and immune system, thus indicating extensive and significant genetic effect [ 37– 42]. In our study, low frequencies ofHLADQB1
*06:02
in SSNSWR and SDNS/FRNS suggested it to be a protective role in regulating the immune response and affecting the occurrence and development of the disease.Table 5 Effects of HLA alleles on SDNS/FRNS risk in SSNS
-*, -* and -* were correlated with the C4 level at onset. Included these three alleles in the mediating effect analysis, and a correlation between the risk factors and SDNS/FRNS in SSNS patients was found. Indirect effect 1: β1,between HLA allele and C4; indirect effect 2: β2, between C4 and SDNS/FRNS; total indirect effect: βInd = β1 × β2. Logistic regression analysis was used to explore the relationship between alleles with frequencies > 1% (frequency = 3%) and risk factors for SDNS/FRNS,and the value was corrected by the FDR method. values lower than 0.05 are shown in bold. human leukocyte antigen, steroid-dependent nephrotic syndrome, frequently relapse nephrotic syndrome, steroid-sensitive nephrotic syndrome, complement 4, false discovery rate, odds ratio
HLA allele C4 Total indirect effect P P_FDR OR B*15:11 0.0006 0.0112 643.879 − 0.058 B*44:03 0.0010 0.0112 331.997 − 0.054 C*07:06 0.0007 0.0100 545.960 − 0.066
Complement plays an important role in regulating antigen-specific immunity, maintaining immune homeostasis,promoting tissue and vascular regeneration, and avoiding autoimmune-based injury [ 43– 45]. Abnormal activation/inhibition of the complement system has been reported in a variety of autoimmune diseases as well as kidney and vascular diseases [ 46– 49]. C4 is the second molecule activated in the classical complement pathway, and it participates in regulating complement activation, preventing immune complex deposition and neutralizing viruses. C4 (C4A and C4B)genes exist in the MHC genome region, between class I and class II HLA genes. Classical complement proteins help to eliminate fragments of dead and damaged cells, therefore attenuating the visibility of diverse intracellular proteins to the adaptive immune system.
Our results of univariate/multivariate logistic regression analyses proved the C4 level to be an independent risk factor for SDNS/FRNS. Compared with SSNSWR, a lower level of C4 was detected in SDNS/FRNS. In the correlation analysis between HLA alleles and risk factors, the loci with carrying frequency less than 1% (n
is less than 2) were excluded due to statistical considerations to ensure a certain level of statistical efficiency. Using logistic regression analysis, we found thatHLA
-B
*15:11, B
*44:03 & C
*07:06
were positively correlated with C4 level, suggesting that there may be a correlation between complement and HLA alleles in SSNS.In the current study of SSNS, there is no report on the levels ofHLA
-B
*15:11, B
*44:03 & C
*07:06
and C4, but there are similar findings in other diseases, that is, the relationship between HLA and complement. Studies have shown that the total copy number of C4 gene is associated with the risk of autoimmune diseases such as systemic lupus erythematosus(SLE), and this association is considered to be caused by linkage disequilibrium (LD*) with nearby HLA gene alleles[ 50, 51]. In the European population,DRB1
*03:01
has a strong LD (R
2 = 0.71) with the common C4B-b (s) allele.Many MHC single nucleotide polymorphism associated with SLE and Stevens Johnson syndrome (SJS) have a proportional LD with C4 &DRB1
*03:01
[ 52].Up to now, there are few reports on these three HLA alleles:HLA
-B
*15:11
was first verified by Hildebrand in Korean patients, and the allele is most likely evolved fromB
*1501
point mutation/short fragment exchange/transformation, encoding fragment of B75 antigen [ 53]. In 2000,a strong correlation betweenB
*44032
-CW
*0706
(HLAC
*07:06
) was found in Bubi population [ 54].HLA
-B
*44:03
:serious allergic reaction of skin and mucosa with complex pathogenesis including SJS and toxic epidermal necrolysis(TEN) is considered to be a non-immediate hypersensitivity reaction mediated by T cells. Studies have shown thatHLAB
*44:03
is a common marker of SJS/TEN and severe cellular surface complications (SOC) in Eurasian populations such as Europe, India, Japan and Thailand. Haplotype analysis shows thatHLA
-B
*44:03
-HLA
-C
*07:01
is a potential risk factor for CM-SJS/TEN combined SOC in Thai population [ 55]; In 2020, the research results reported by Wang et al. clarified the expression profile and expression degree of several complement components in niDHRs, especially SJS and TEN, at the mRNA and protein levels for the first time. To a certain extent, it indicates that the abnormality of complement system may be a part of the pathogenesis of SJS and TEN [ 56]. Combined with the results showing the impact of HLA alleles on the complement system of other diseases, we speculate that there may be LD betweenHLAB
*15:11, B
*44:03 & C
*07:06
and C4 or C4-related complement genes. These three alleles may affect C4 gene expression or copy number via this potential association, and it in turn affects C4 levels, participating in immune recognition,response and homeostasis, and indirectly affecting treatment response and prognosis. In addition, our results suggested a higher likelihood of steroid dependence/relapse all over the course of the disease.In conclusion, theHLA
-A
*11:01
allele is associated with SSNSWR and SDNS/FRNS in Chinese Han children, which emphasizes the value of HLA alleles’ detection in precise typing of Chinese children with SSNS.HLA
-B
*15:11
,HLA
-B
*44:03
andHLA
-C
*07:06
may indirectly affect the prognosis of children with SDNS/FRNS by regulating C4 level. Our research aims to provide a new direction for pathogenesis, functional studies and individualized clinical diagnosis and treatment strategies for SSNS patients. Also, this research provided an important reference for HLA-I allele (includingHLA
-A
*11:01
,HLA
-B
*15:11
,HLA
-B
*44:03
andHLA
-C
*07:06
) in further genetic counseling and testing for inherited gene mutations in SSNSWR or SDNS/FRNS.Supplementary Information
The online version contains supplementary material available at https:// doi. org/ 10. 1007/ s12519- 021- 00489-y.Acknowledgements
We thank the children and their families in Children's Hospital of Chongqing Medical University (CHCMU) for their support and cooperation and Na Liu, Shao-Wei Zhang and Ya-Jun Qin(MyGenostics Inc, Beijing, China) for their assistance.Author contributions
All authors are responsible for the entire content of this manuscript and agree to submit it. The project is jointly designed and directed by LQ and CH, and has made equal contributions to this paper. LQ leads the laboratory of Chongqing international science and technology cooperation center for child development and disorders. YHP led the application of clinical and genetics in clinical practice, and led and discussed the design and implementation of the project. LH was responsible for the concepts of statistics,methodology, initial analysis of the data, collection and extraction of clinical data, and writing of the manuscript. WL, NFF, FSP, and GXJ provide professional clinical knowledge for the research. YXY and CH were responsible for the collection and extraction of clinical data.LYT was responsible for the rationality of statistical methods. CXL YBH, WJL, JJ, and WDQ participated in the patient recruitment. ZGF and WM led the molecular diagnoses of cases under clinical genetic guidelines. All authors revised and agreed to the final version of the manuscript.Funding
This work was funded by the China National Natural Science Foundation (No. 81770713) and China National Clinical Research Center Foundation (No. YBXM-2019-002).Data availability
The data used to support the findings of this study are available from the corresponding author upon request.Declarations
Ethical approval
This study has been approved by China Clinical Trial Registration Center (registration number: ChiCTR1900023187) and the Ethics Committee of Children's Hospital Affiliated to Chongqing Medical University. All participants and their guardians understood the content and significance of the study and signed informed consent forms before participating.Conflict of interest
No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. The authors have no conflict of interest to declare.Open Access
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source,provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/. World Journal of Pediatrics2022年2期
World Journal of Pediatrics2022年2期
- World Journal of Pediatrics的其它文章
- Jacobsen syndrome with bilateral periventricular white matter lesions
- Diagnostic performance of serum interleukin-6 in pediatric acute appendicitis: a systematic review
- Variations in length of stay among survived very preterm infants admitted to Chinese neonatal intensive care units
- Epidemiology and region-specific risk factors for low Apgar scores in China: a nationwide study
- Ursodeoxycholic acid prevention on cholestasis associated with total parenteral nutrition in preterm infants: a randomized trial