
Mortality in patients with COVID-19 requiring extracorporeal membrane oxygenation:A meta-analysis
2022-06-30 03:28YeZhangLeiWangZhiXianFangJingChenJiaLianZhengMingYaoWenYuChen
World Journal of Clinical Cases 2022年8期
INTRODUCTION
Coronavirus disease 2019(COVID-19),caused by the novel severe acute respiratory syndrome coronavirus 2(SARS-CoV-2)infection,has become a global pandemic.As of October 25,2021,there have been over 243 million infections and approximately 4.9 million deaths[1].It was characterized by rapid disease progression and a high risk of acute respiratory distress syndrome(ARDS)due to severe or fatal pneumonia[2].Although the majority of COVID-19 patients have very moderate disease,current studies suggest that approximately 18% of them have serious disease[3]with a mortality rate of up to 53%-67%[4,5].
Extracorporeal membrane oxygenation(ECMO),which can support gas exchange in patients failing conventional mechanical ventilation[6],has been proven to be effective in the treatment of severe respiratory failure and cardiovascular compromise caused by ARDS,based on the experience of previous viral outbreaks,such as Middle East Respiratory Syndrome and H1N1 influenza[7-9].There are two primary ECMO therapy methods: Veno-venous ECMO(VV-ECMO)and veno-arterial ECMO(VA-ECMO).For the vast majority of COVID-19 patients who need ECMO treatment,we adopted VVECMO.The World Health Organization(WHO)and Chinese experts have recommended that ECMO can be used as a salvage therapy for severe COVID-19 patients who are not responding to conventional ARDS treatments[10-14].Although there are still numerous complications,research has revealed that 63% of patients recovered from ARDS and were weaned from ECMO.
Despite such optimism for a possible role for ECMO in COVID-19,concerns have been raised due to the high mortality rate observed in studies[15].Venerable age,late ECMO initiation time,and multiple complications(diabetes,heart disease,obesity,)are all independent risk factors that increase the 90-d mortality rate.The role of ECMO in the treatment of diseases caused by this new virus is still uncertain and controversial.Currently,there is insufficient worldwide evidence to assess the effectiveness of ECMO.The majority of prior studies were based on retrospective cohort studies and case reports in a specific population,making it difficult to analyze the impact of ECMO on COVID-19 patients in a systematic manner[6].Therefore,we conducted a meta-analysis focusing on the mortality of COVID-19 patients requiring ECMO in order to guide current clinical practice and future research efforts.
MATERIALS AND METHODS
Search strategy
To identify articles concerning ECMO and COVID-19,a comprehensive literature search was undertaken utilizing the PubMed,EMBASE,Web of Science,Cochrane Library,and Clinical Trials databases.On December 9,2020,all searches were updated,and the search strategy was divided into two categories:(1)COVID-19;and(2)ECMO.The following keywords were used: “COVID-19”,“2019 novel coronavirus disease”,“2019-nCoV”,and “Extracorporeal membrane oxygenation.” The articles were limited to English literature.To prevent missing relevant records,reference lists from the selected studies and systematic reviews were thoroughly searched.Furthermore,this systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)and Metaanalysis of Observational Studies in Epidemiology(MOOSE)guidelines,and it was registered at the International Prospective Register of Systematic Reviews(number CRD42020227414)prior to submission.
Inclusion and exclusion criteria
Original studies that matched the following criteria were included in the meta-analysis:(1)Studies with tenor more patients;(2)Patients with laboratory-confirmed COVID-19 receiving ECMO;(3)Studies with primary data;and(4)Studies with more than 5 points on the Newcastle-Ottawa scale(NOS).The exclusion criteria were:(1)Duplicate publication or dataset;and(2)Animal andexperiments,case reports,letters,editorials,comments,conference summaries,meta-analyses,and reviews were excluded.
Data extraction
Data from the included articles were extracted,including authors' names,publication year,study location,study design,sample size,patient baseline characteristics,clinical parameters,management,primary outcome,and complications.The article search,selection,data extractions,and quality assessment were all conducted independently by two reviewers(ZY and CWY),and any disagreements were resolved after consensus.
As you can imagine, I could hardly wait to have the day for our reunion. After several months waiting, 25 of my former high school classmates and 3 of our teachers were crowded in a small restaurant near our high school. We were more than happy to meet with each other again. Our former Chinese teacher was so excited that he even choked() to say some words. With gratitude4, we thanked our teachers for their hard work; with great joy, we exchanged the happy things happening in each of our present colleges; We talked and talked before someone shouted. Oh, it was 11:30 now. But no one would be the first to say good bye to others.
Quality assessment
The NOS was applied for a quality assessment on all of the included papers.All included papers were classified as poor(scores 0–3),moderate(scores 4–6),or high(scores 7–9)quality studies,with papers with more than 5 points being considered for further analysis.
He drew the veil from her face, and when he saw her immeasurable ugliness, he sprang back terrified, and said, How comest thou here? Who art thou? I am thy betrothed bride, but because I feared lest the people should mock me when they saw me out of doors, I commanded the scullery-maid to dress herself in my clothes, and to go to church instead of me
Statistical analysis
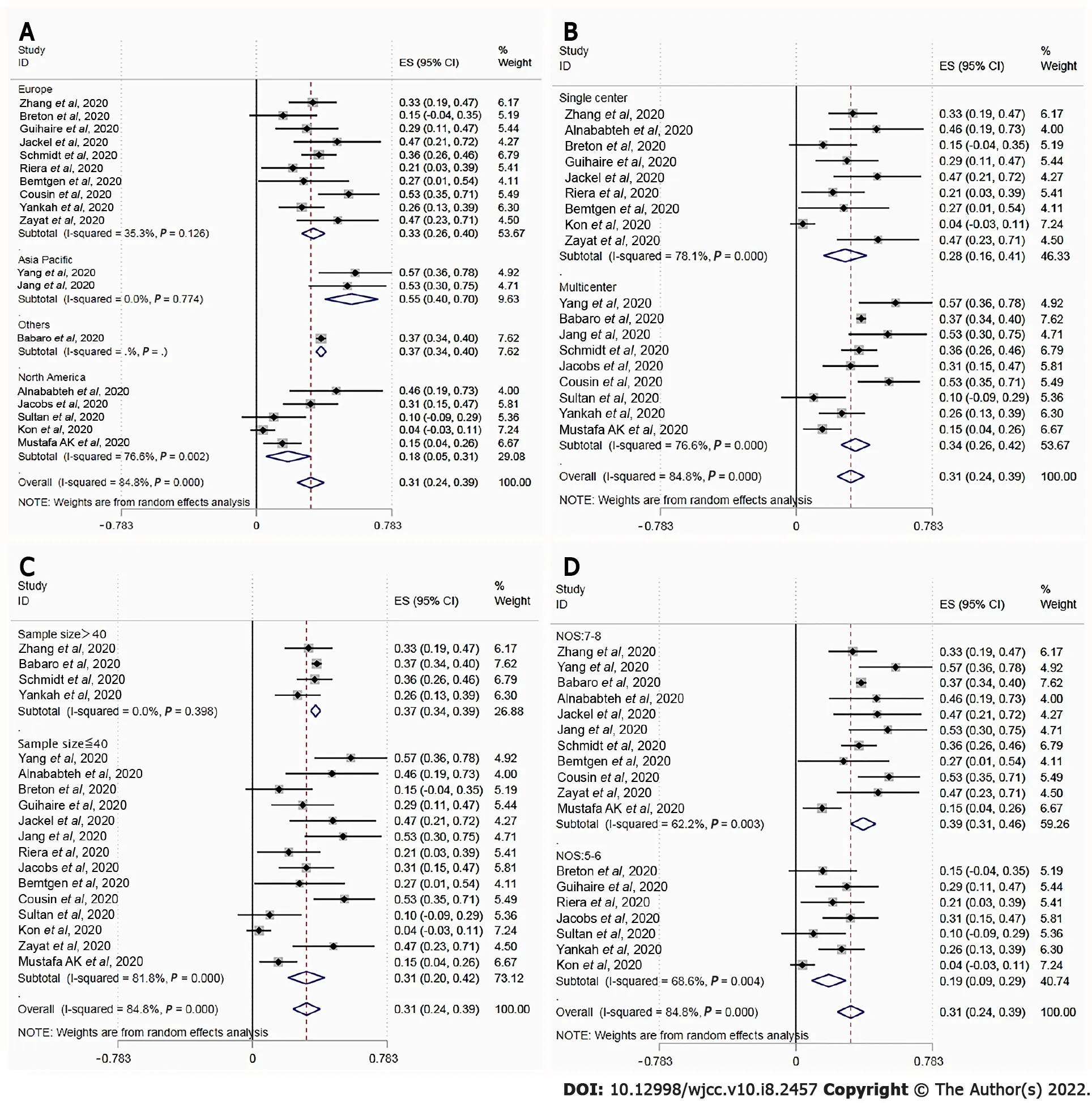
Figure 3 depicts the outcomes of the random effects model and subgroup analysis.There were significant differences in mortality between location groups(Figure 3A;33.0%55.0%37.0%18.0%,<0.001),setting groups(Figure 3B;28.0%34.0%,<0.001),sample size group(Figure 3C;37.0%31.0%,<0.001),and NOS groups(Figure 3D;39.0%19.0%,<0.001).There was no source of heterogeneity in any of the subgroups.
RESULTS
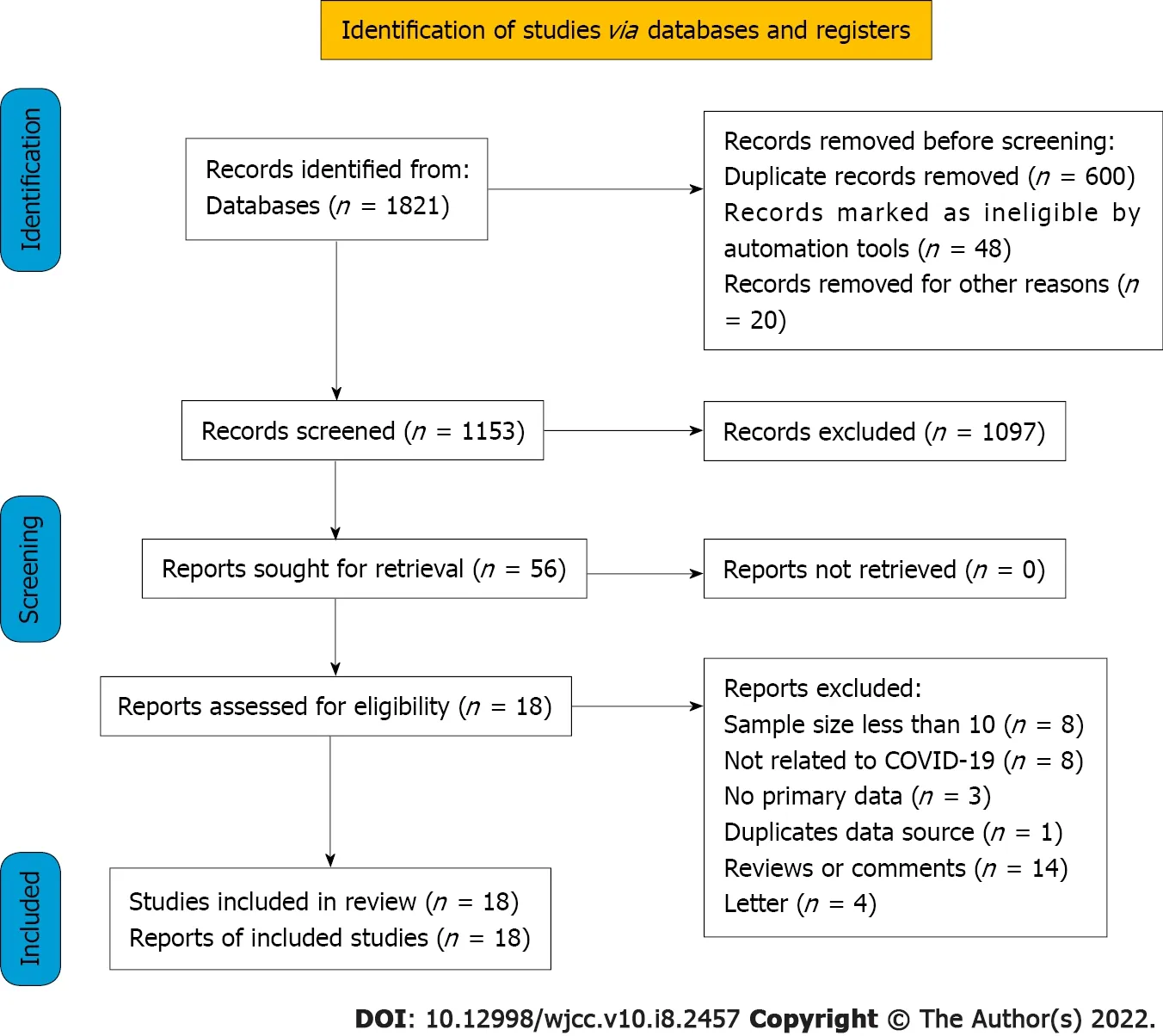
In the initial search,1821 potentially relevant articles were identified.After eliminating duplicates,1153 studies were assessed based on title and abstract.Following a full-text review of the remaining 56 studies,38 studies were excluded.Finally,the meta-analysis comprised 18 articles representing 1494 verified COVID-19 patients treated with ECMO(Figure 1).Since EuroELSO was a subset of centers participating in the international ELSO registry,we eliminated the previous study on EuroELSO to avoid data duplication[16,17].
Studies characteristics and quality assessment
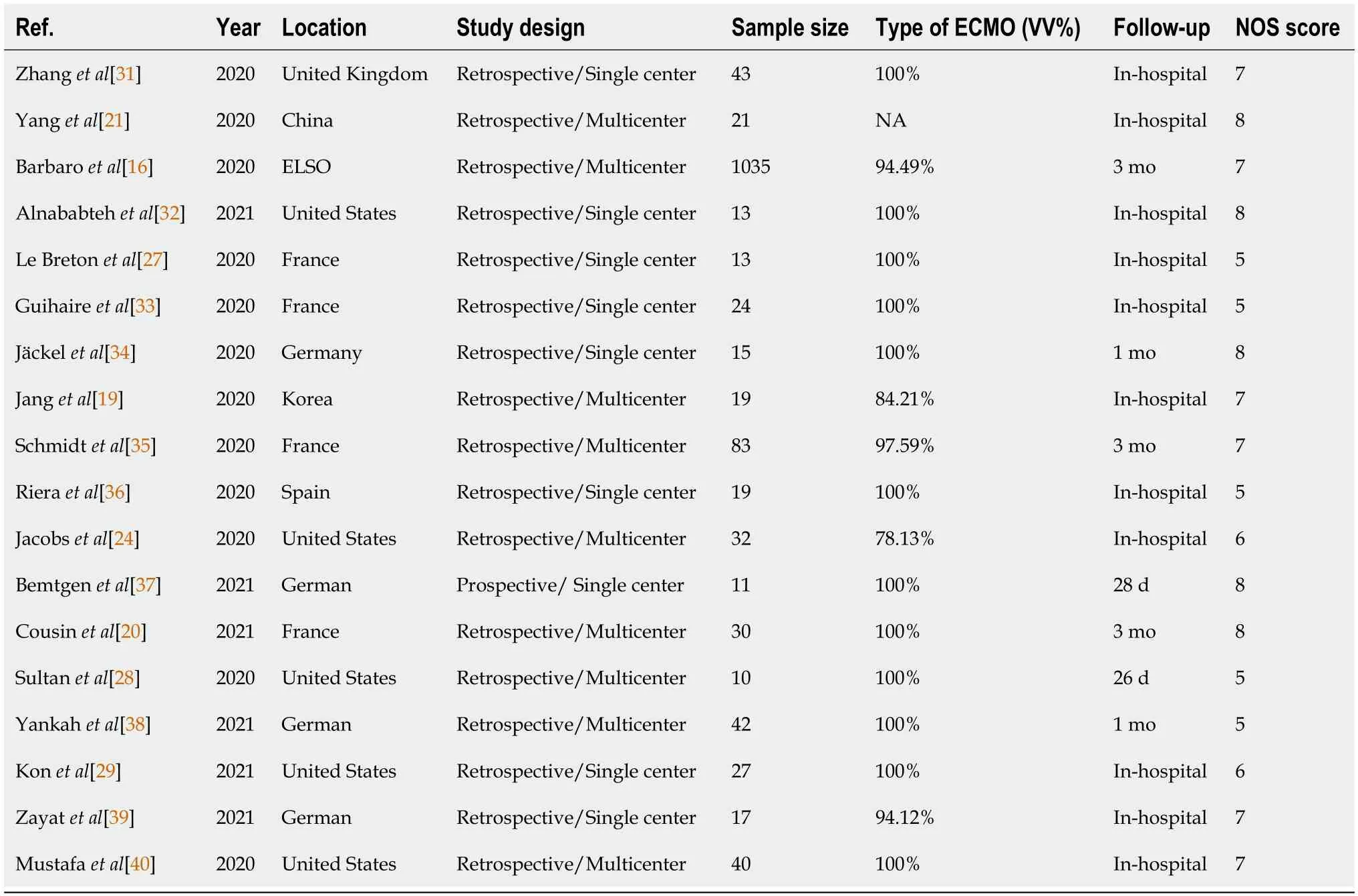
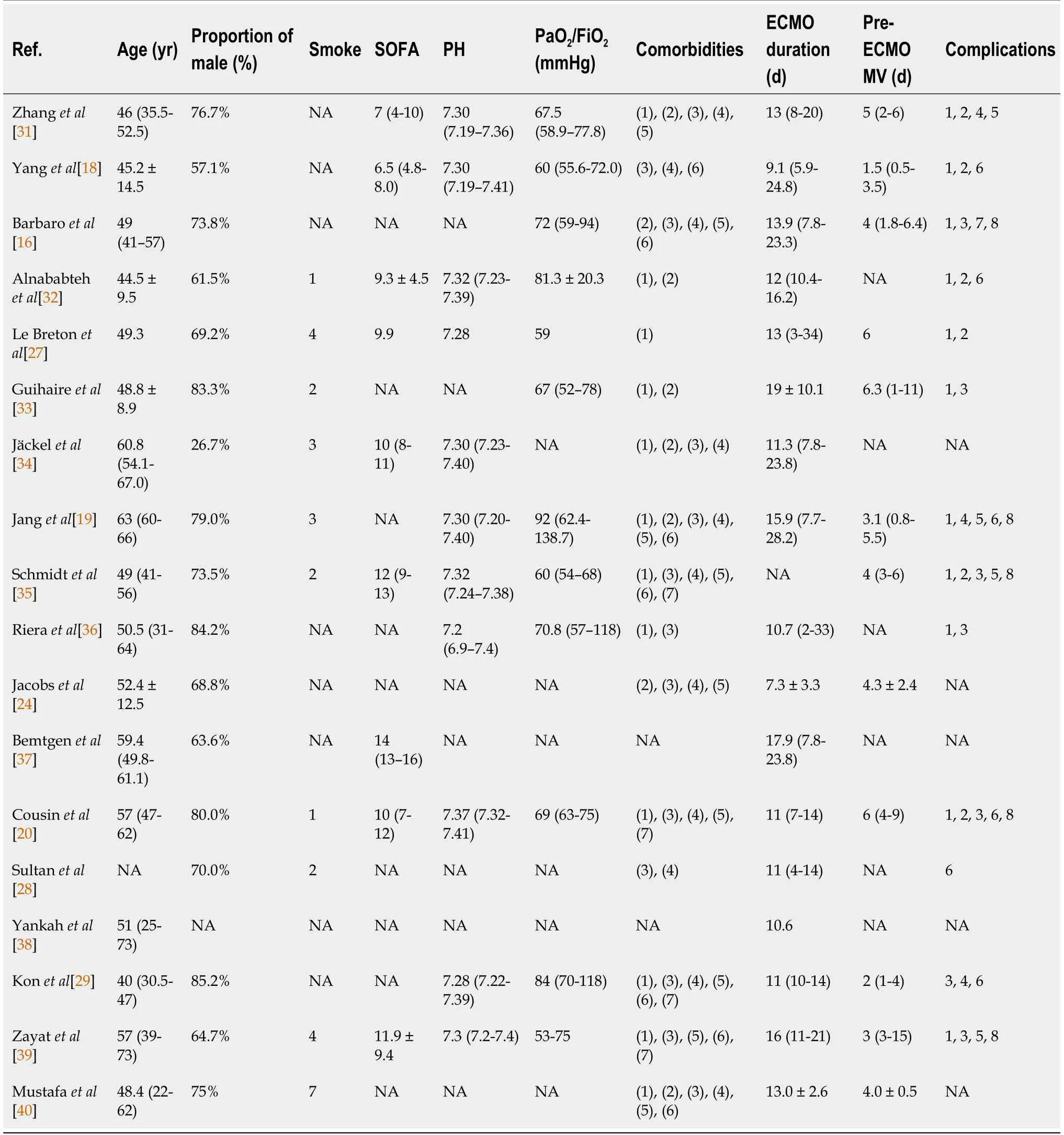
The characteristics of these studies are summarized in Table 1.All of the studies were observational in design,with the majority of them being retrospective(94.2%).The score of the quality assessment ranged from 5 to 8 on the NOS.All studies were rated as “moderate to high quality.” In the majority of cases,VV-ECMO was utilized(93.8%).Table 2 summarizes the sample characteristics of the included studies.
We would like to thank all authors of the included primary studies.
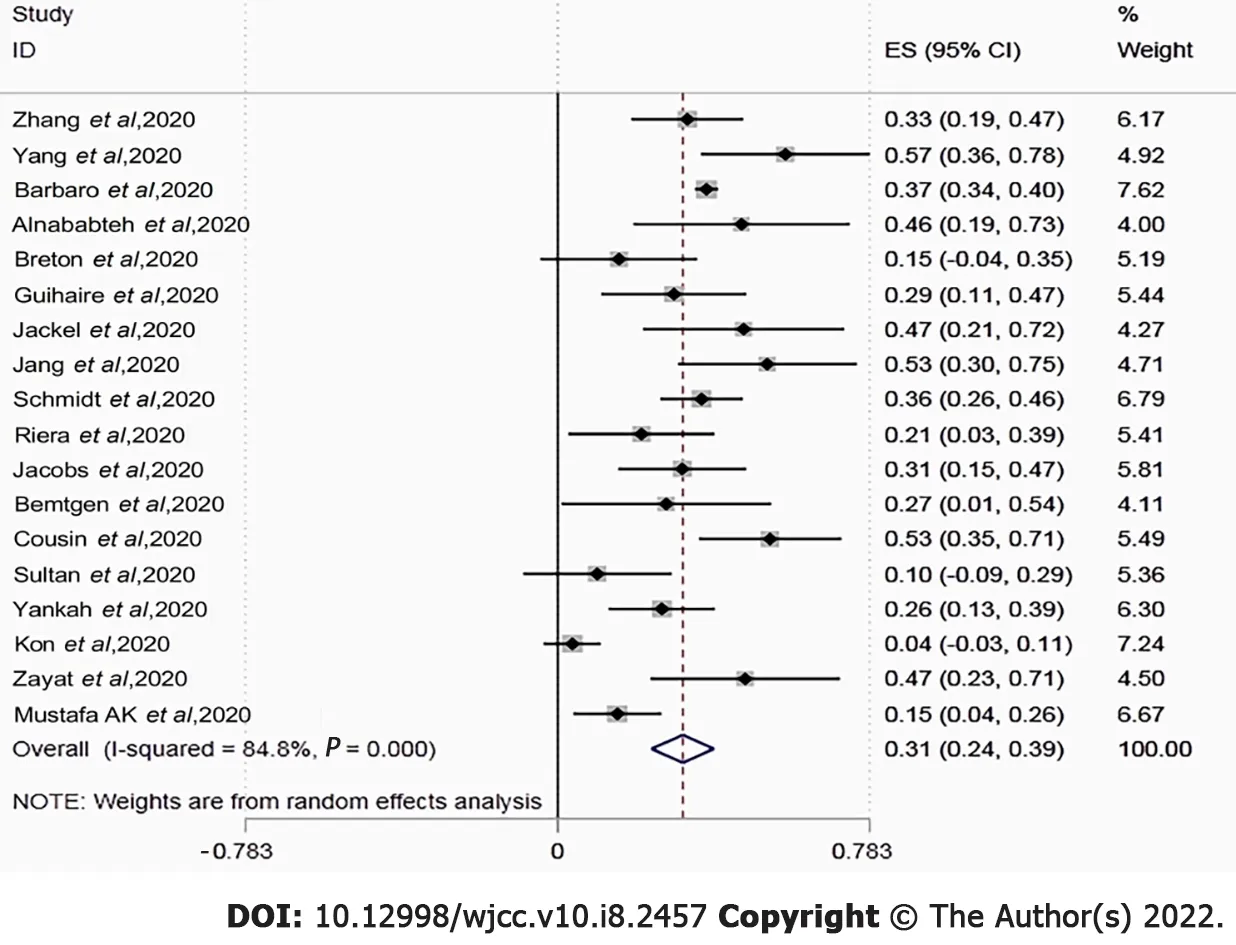
The in-hospital or short-term mortality ranged between 0.04 and 0.57.Overall pooled mortality was estimated to be 0.31[95% confidence interval(CI): 0.24-0.39;= 84.8%]using random-effect pooled estimates(Figure 2).Two studies found that the mortality rate in the ECMO group was lower than that in the mechanical ventilator group(57.1%63.2% and 46.2%47.8%).
Subgroup analysis
The pooled estimates of the event rate were obtained using the random-effects model.Each study had its own underlying effect size.The random-effects model assumes that there is a mean population effect size that varies depending on the study.We used the inconsistency statistic()to evaluate the extent of heterogeneity.Anvalue greater than 50% was considered to indicate substantial heterogeneity.The Egger's and Begg's tests were used to assess publication bias and a visual funnel plot for asymmetry was presented.Sensitivity analysis and subgroup analysis were also utilized to investigate the source of heterogeneity and a two-sided test at the 5% level was considered statistically significant.Moreover,Stata 15.1(Stata Corporation,College Station,TX,United States)was utilized to conduct the metaanalysis.
Publication bias and sensitivity analysis
Funnel plots showed no obvious asymmetry.The Egger’s(= 0.95)and Begg’s tests(= 0.14)further revealed no significant publication bias.The recalculated pooled results did not change significantly after removing each study sequentially,showing that there was no outlier study that influenced the overall result.
DISCUSSION
Now the Princess happened to walk that way; and when she heard the tune13, shestood quite still, and seemed pleased; for she could play Lieber Augustine ;it was the only piece she knew; and she played it with one finger.
We acknowledge that our study has several limitations.To begin with,the power of the study is limited by the small sample size.Biases in patient selection and indication may have existed due to the small sample size.Additionally,the majority of the included studies were observational with retrospective designs,and more than half of the studies were single-center ones,which may lead to selection and reporting bias.Finally,the survival analyses for mortality were based on a short-term follow-up and varied death observation time,which might have underestimated the reported prevalence of mortality and complications.
According to the studies with a low mortality rate among patients who received ECMO treatment,we recommend that ECMO should be combined with the use of other therapies,such as antiviral,immunosuppressive,anticoagulant,and supportive therapies,as well as the collaboration of professional multidisciplinary teams and professional nursing[27-29].Additionally,the timing of ECMO intervention may also be a critical factor affecting the prognosis.Previous studies have confirmed that early ECMO intervention after mechanical ventilation can enhance the survival rate of patients with HINI pneumonia and ARDS[26].The majority of patients with severe ARDS and severe SARS-CoV-2 pneumonia received delayed treatment and rapidly worsened.Yang[21]showed that among COVID-19 patients treated with ECMO,the average time from mechanical ventilation to ECMO in the survival group was shorter than that in the death group.The use of early ECMO may be associated with a better prognosis[18].Despite the fact that the PaO/FiOratio is less than 80 mm Hg and the MV treatment has been administered,we believe that ECMO should be initiated as soon as possible.Moreover,research has shown that prolonged ECMO treatment may be associated with an increased risk of death and multiple organ failure[30].Therefore,both the timing and duration of ECMO treatment are critical to consider when treating critically ill patients with COVID-19.
Although some studies reported that the mortality rate of COVID-19 patients treated with ECMO is as high as 53%-83.3%[18-22],which is substantially higher than the results of this study,we believe such high mortality may be due to other reasons rather than the ECMO treatment being ineffective.For example,many previous studies conducted in the early stage of the COVID-19 outbreak used a small sample size with a high proportion of patients having pre-existing comorbidities,which may be an important factor contributing to the high mortality[23].Additionally,due to a lack of experience in treating COIVD-19 at the beginning of the outbreak,ECMO treatment may have been initiated too late.The secondary infection and other complications may also lead to high mortality.These possible reasons of increased mortality are consistent with prior results obtained by certain researchers who discovered that variables such as advanced age(>65 years old),gender(male),pre-existing diseases,and acute or chronic organ failure may contribute to a poor prognosis[24-26].Considering these factors,our findings may provide evidence for the future application of ECOM in treating severe COVID-19 patients.
The heap of feathers that you see here, said she, you must get finished before I come home in the evening, otherwise you shall be set to harder work
CONCLUSION
Despite the fact that ECMO is approved as a rescue treatment for severe COVID-19,its application during the COVID-19 pandemic is currently restricted due to high treatment costs and an unclear usage procedure.Our findings suggested that ECMO might be a feasible and effective treatment for COVID-19 patients with more resource evaluation and risk-benefit analysis.Further research with a large sample size and multi-center designs is needed to examine the effectiveness of ECMO in the treatment of COVID-19 patients.
Later that day the junior executive went in to see his boss, who had been noted5, by the way, as being kind of a grouchy6 fellow. He sat his boss down and he told him that he deeply admired him for being a creative genius. The boss seemed very surprised. The junior executive asked him if he would accept the gift of the blue ribbon and would he give him permission to put it on him. His surprised boss said, Well, sure.
When I m 18 , When I buy a new 450SL Mercedes Benz , When I put my last kid through collage5 , When I have paid off the mortgage , When I get a promotion6 , When I reach the age of the retirement7, I shall live happily ever after
ARTICLE HIGHLIGHTS
Research background
Patients with moderate to severe coronavirus disease 2019(COVID-19)infection often have severe acute respiratory distress syndrome,with a poor prognosis,limited treatment options,and high mortality.Extracorporeal membrane oxygenation(ECMO)has been proven to have the advantages of improving symptoms and reducing mortality in previous studies.However,existing studies lack strong evidence and disagreement whether ECMO can reduce the mortality of patients with moderate to severe COVID-19 infection.This article intends to summarize the mortality of COVID-19 patients treated with ECMO in order to evaluate the efficacy of ECMO in COVID-19 patients.
Research motivation
Prospective,large-sample,multi-center studies are needed to have a more comprehensive understanding of the effectiveness and safety of ECMO treatment.
ECMO is an essential instrument for treating severe respiratory and heart failure,and it was widely employed in the treatment of critically ill patients during the COVID-19 pandemic.However,previous research found that the impact of ECMO in critically ill COVID-19 patients was controversial due to the high mortality rate.Therefore,we conducted this meta-analysis that included 18 original independent studies to examine the effectiveness of ECMO in the treatment of COVID-19.The mortality rate of COVID-19 patients treated with ECMO in our investigation was 31%,which was lower than the mortality rate of severe COVID-19 patients in the prior study.These data imply that ECMO treatment may decrease the mortality rate of COVID-19 patients who are severely ill.
Research objectives
To evaluate the efficacy and adverse reactions of ECMO inCOVID-19 patients.
Research methods
This research was conducted through the method of meta-analysis.A random effects model was adopted to assess the mortality of COVID-19 patients treated with ECMO.
Research results
The mortality rate of COVID-19 patients treated with ECMO was 31%,which was lower than the mortality rates of severe COVID-19 patients in previous studies,suggesting that ECMO treatment can reduce the mortality rate of severe COVID-19 patients.Previous studies have not yet given clear answers to when ECMO should be used and the duration of ECMO treatment.
Then he would cry, but what nobody knows nobody cares for; so he would cry till he was tired, and then fall asleep; and while we are asleep we can feel neither hunger nor thirst
The Magician s servants hurried after the fresh tracks, but when they came to the bridge, they stood, not knowing which road to take, as the footprints stopped suddenly, and there were three paths for them to choose from
Research conclusions
ECMO may be a feasible and effective treatment for COVID-19 patients.
Research perspectives
To summarize the mortality and comorbidities of COVID-19 patients treated with ECMO,to evaluate the efficacy and adverse reactions of ECMO inCOVID-19 patients,and to clarify the effectiveness of ECMO treatment,in order to provide a basis for future treatment options for patients with moderate to severe COVID-19.
ACKNOWLEDGEMENTS
With the last poignant34 note still reverberating35 in the air, she lowered her harmonica, placed it in her matronly-styled black purse, and snapped the purse shut
FOOTNOTES
Zhang Y,Wang L,and Fang ZX conceptualised and designed the protocol,drafted the initial manuscript,and reviewed the manuscript;Chen J and Zheng JL defined the concepts and search items,data extraction process,as well as methodological appraisal of the studies;Yao M planned the data extraction and statistical analysis;Chen WY provided critical insights;all authors have approved and contributed to the final written manuscript.
The Jiaxing Fight Novel Coronavirus Pneumonia Emergency Technology Attack Special Project in 2020,No.2020GZ30001;the Key Discipline of Jiaxing Respiratory Medicine Construction Project,No.2019-zc-04;Scientific Technology Plan Program for Healthcare in Zhejiang Province,No.2021KY1100;and A Project Supported by Scientific Research Fund of Zhejiang Provincial Education Department,No.Y202043573 and No.Y202043729.
All the authors report no conflicts of interest for this article.
The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution Non Commercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Ye Zhang 0000-0001-9740-1502;Lei Wang 0000-0003-0434-5340;Zhi-Xian Fang 0000-0001-6164-6727;Jing Chen 0000-0001-8115-5896;Jia-Lian Zheng 0000-0002-7129-0696;Ming Yao 0000-0002-3014-0560;Wen-Yu Chen 0000-0003-0412-2913.
They flew nearer, and presently the young birds woke and cried, Mother, what have you brought for us? and they told the whole story of the fight, and of how they were alive only by the favour of the young man under the tree, and of his cutting up the dragon and of their eating it
Fan JR
Wang TQ
Fan JR
 World Journal of Clinical Cases2022年8期
World Journal of Clinical Cases2022年8期
- World Journal of Clinical Cases的其它文章
- Analysis of bacterial spectrum,activin A,and CD64 in chronic obstructive pulmonary disease patients complicated with pulmonary infections
- Developing natural marine products for treating liver diseases
- Computed tomography perfusion imaging evaluation of angiogenesis in patients with pancreatic adenocarcinoma
- Epidemiological features and dynamic changes in blood biochemical indices for COVID-19 patients in Hebi
- Identification and predictive analysis for participants at ultra-high risk of psychosis:A comparison of three psychometric diagnostic interviews
- Prognostic significance of peritoneal metastasis from colorectal cancer treated with first-line triplet chemotherapy