
Exercise training improves participation in persons with multiple sclerosis:A systematic review and meta-analysis
2022-06-09 09:24ThomsEdwrdsAnneSophieMihelsenAfolsdeFkoldeUlrikDlgsLrPilutti
Thoms Edwrds,Anne Sophie Mihelsen,Afolsde O.Fkolde,Ulrik Dlgs,Lr A.Pilutti*
a School of Human Kinetics,University of Ottawa,Ottawa,ON K1N6N5,Canada
b Department of Public Health-Exercise Biology,Aarhus University,Aarhus C 8000,Denmark
c School of Rehabilitation Therapy,Queens University,Kingston,ON K7L3N6,Canada
d Interdisciplinary School of Health Sciences,Brain and Mind Research Institute,University of Ottawa,Ottawa,ON K1N6N5,Canada
Received 5 March 2021;revised 29 May 2021;accepted 22 June 2021
Available online 27 July 2021
2095-2546/© 2022 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.
(http://creativecommons.org/licenses/by-nc-nd/4.0/)
Abstract Background:Although previous studies have examined the effects of exercise training on other International Classification of Functioning,Disability and Health (ICF) component levels in persons with multiple sclerosis (MS), the effects of exercise training on participation remain unclear.The objectives of this review were to:(1)characterize systematically the use of outcome measures that capture participation in exercise training studies;(2)quantify the effect of exercise training on participation in persons with MS. Methods:A search of 6 electronic databases(CINAHL,SPORTDiscuss,Embase,MEDLINE,Cochrane Central,and Scopus)was conducted to identify controlled and noncontrolled trials involving exercise training and participation in persons with MS.Search strings were built from Medical Subject Headings and CINAHL headings.ICF linking rules were used to identify participation chapters and categories captured.Meta-analysis was used to quantify the effect of exercise training on participation in randomized controlled trials comparing exercise effects to no intervention/usual care. Results:We included 49 articles involving controlled and noncontrolled exercise trials in the systematic review of outcome measures.We captured 16 different outcome measures that captured all 9 participation chapters and identified 89 unique participation categories.Across these 16 outcome measures, mobility was the most commonly represented participation chapter, with 108 items.A subsample of 23 randomized controlled trials was included in the meta-analysis.An overall effect of 0.60(standard error=0.12,95%confidence interval:0.36-0.84,z=4.9,p <0.001)was calculated,indicating a moderate,positive effect of exercise training on participation. Conclusion:The current review provides information that can be used to guide the selection of outcome measures that capture participation in studies of exercise training in persons with MS.Exercise training has a positive effect on outcomes that capture participation,providing further evidence for the role of exercise training in promoting and maintaining engagement in everyday life.
Keywords: Exercise training;ICF framework;Multiple sclerosis;Participation
1.Introduction
The pathology of multiple sclerosis (MS) involves chronic neuroinflammation and neurodegeneration within the central nervous system,1,2often resulting in symptoms and physical limitations that impact an individual’s ability to participate in society.3,4According to the International Classification of Functioning, Disability and Health (ICF),5participation and associated restrictions have been described as the involvement in and problems experienced with life situations.Given the broad nature of participation, efforts have been made to identify participation categories that may be particularly relevant for persons living with MS.6The brief ICF core set for MS identifies involvement in situations related to “solving problems”, “carrying out daily routines”, “walking”, “family relationships”,and“remunerative employment”as key categories of relevance for understanding and describing disability in persons with MS.6Additionally, “recreation and leisure”,“socializing”, and “community life” are aspects ofparticipation that have been reported to be of relevance to persons with MS.3Outcomes that capture participation provide insights into the impact of MS on everyday living and have been identified as outcomes of high importance to people living with MS.6,7Importantly,persons with MS demonstrate significant impairment in multiple participation categories; and greater impairment is experienced as disability increases.8Despite this, there has been an underuse of study end-points that capture participation in clinical trials involving persons with MS.9Consequently, understanding the potential of interventions to improve participation is of the utmost importance.
Exercise training has emerged as a safe,effective,low-cost,nonpharmacological intervention for managing disability experienced by persons with MS.10Previous systematic reviews and meta-analyses have reported that exercise training promotes improvements in aerobic capacity, muscular strength, balance, walking performance, and gait kinematics,while also reducing fatigue and depression.10-13Within the context of the ICF, these effects reflect primarily improvements in “body structures”, “body functions”, and “activities”component levels.Previous studies of exercise training have used a variety of measures that capture different aspects of participation in everyday life,such as carrying out daily tasks and self-care, walking and movement, interpersonal relationships,and recreation and leisure.Such measures are rarely the primary outcome of intervention studies,9and are often not included with the intention of capturing changes in everyday life that may occur in response to exercise training.
Previous reviews have examined the effects of exercise and physical activity interventions on some aspects of participation,such as quality of life and physical activity levels.One metaanalysis conducted in 2008 reported that exercise training was associated with small,significant improvements in quality of life among persons with MS;14however, a systematic review conducted in 2013 reported inconclusive findings.15Another meta-analysis supported the efficacy of behavioral interventions,including those involving exercise and physical activity, for increasing self-reported physical activity behavior in persons with MS.16Although previous research provides insight into the effects of exercise training on some aspects of participation,they do not represent the entire scope of outcome measures that capture different elements of participation.As a result, the effect of exercise training on different categories of participation has not been described.The extent to which outcomes that capture participation have been included in studies of exercise training, and which aspects of participation are captured by these tools, also remain unclear.
Given the importance of participation for describing the impact of MS on daily life and the significance of such outcomes to persons with MS, and in order to gain a preliminary understanding of the effects of exercise training on participation, a review of the current literature is warranted.Consequently, the objectives of this review were to: (1)systematically characterize the use of outcome measures that capture participation in studies of exercise training involving persons with MS;and(2)quantify the effect of exercise training on participation in persons with MS.Results from this review can be used by researchers and clinicians to guide the selection of relevant participation outcomes as endpoints of exercise and rehabilitation interventions.This review further provides evidence for the role of exercise training in improving involvement in everyday life for persons with MS.
2.Methods
The protocol for the current review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)17recommendations and was submitted, accepted,and published in the international database of prospectively registered systematic reviews in health and social care(PROSPERO;ID#CRD42020155721).18
2.1.Search strategy and screening
This review focused on published studies examining the effect of exercise training on participation in persons with MS.According to the ICF framework, participation outcome measures were defined as those that capture the “involvement of people in all areas of life”.5Exercise training was defined as a “form of leisure-time physical activity that was performed repeatedly over an extended period of time with a specific external objective”.19
A search of 6 electronic databases(CINAHL,SPORTDiscuss,Embase,MEDLINE,Cochrane Central,and Scopus)was initially conducted on August 16, 2019, and then updated on August 31,2020.The following Population/Patient, Intervention, Comparison, Outcome question18guided the search strategy: “Amongst persons with MS, to what extent does exercise training, in comparison to a non-exercise condition, effects participation?”Searches were conducted using database-specific terms based on Medical Subject Headings (MeSH) and CINAHL headings to identify keywords related to “multiple sclerosis” (Term 1),“exercise training” (Term 2), and “participation” (Term 3)(Supplementary Table 1).The database search was supplemented by hand searches of the authors’ personal databases, relevant reviews, meta-analyses, and reference lists of the included articles.Results from the literature search were exported to Covidence (Veritas Health Innovation, Melbourne, Australia),which was then used to de-duplicate the retrieved articles.
After removal of duplicates,an initial screening at the title/abstract level was conducted using the following inclusion criteria to identify studies involving: (1) adults (>18 years of age)with a diagnosis of MS;and(2)exercise training.Following the initial screening, full-text articles were evaluated and excluded using the following criteria: (1) not in English; (2)animal models; (3) nonprimary research; (4) non-MS population;(5)no exercise intervention(≥2 weeks in length);and(6)no participation outcome.At that stage of the screening process, all eligible articles (controlled and noncontrolled trials)were included in the systematic review for the purpose of characterizing the use of outcome measures that capture participation.Articles were further screened for inclusion in the metaanalysis using the following criteria: (1) randomized controlled trial(RCT)design;(2)control group involving no exercise intervention or usual care; and (3) sufficient data tocalculate effect sizes.TE and ASM individually reviewed each article during the title/abstract screening, full-text screening,and meta-analysis screening stages.Upon the completion of each stage of the screening process,discrepancies between the authors regarding article inclusion were discussed.If consensus could not be reached,a third author(LAP)served as a tiebreaker.
2.2.Data extraction
Following the screening process, relevant data from the included articles were extracted into Microsoft Excel 2019(Microsoft, Redmond, WA, USA) by 2 members of the research team(TE and ASM).Data were initially extracted by TE, with ASM ensuring the accuracy of the extracted data.Extracted data included study characteristics (study design,sample size, and country of origin), participant characteristics(age, body mass index, and sex distribution), clinical characteristics (disease duration, MS type, and disability status),exercise prescription (modality, setting, duration, frequency,and intensity), and participation outcome values (pre/post mean, significance of change).Any discrepancies or errors in data extraction were settled by consensus.
2.3.Quality assessment
The Tool for the Assessment of Study Quality and Reporting in Exercise (TESTEX) scale, was used to evaluate the quality of each article.20The TESTEX scale was selected to evaluate study quality as it has demonstrated reliability in scoring exercise training studies,has been used in other systematic reviews/meta-analysis involving exercise trials, and was designed specifically for the evaluation of exercise training studies.20The TESTEX overcomes some limitations of other quality evaluation tools by accounting for aspects of study design unique to exercise training studies, allowing a more nuanced evaluation of study quality.
The TESTEX scale has a maximum possible score of 15 points, with a higher score indicating better methodological quality.20Each article was independently evaluated by TE and ASM.Any scoring discrepancies between the raters were discussed and resolved when possible.A third author(LAP)acted as a tiebreaker when discrepancies could not be resolved.A breakdown of the TESTEX scores per item for each article is presented in Supplementary Table 2.
2.4.Characterization of participation outcomes
Outcome measures used to capture participation were identified and quantified per study.Established ICF linking rules and protocols were then used to identify the participation chapters and categories captured within each outcome measure.21,22Each individual item within the retrieved outcome measure was linked to the corresponding ICF participation chapter and category code.If an item could not be linked to a participation chapter,it was described as a nonparticipation item.Each item was linked independently by TE and AOF.Any discrepancies in the ICF linking process were discussed among the authors and resolved when possible.A third author (LAP) acted as a tiebreaker if discrepancies could not be resolved.Items were linked to the lowest possible ICF participation code.
2.5.Descriptive analytic approach
Descriptive statistics were used to calculate the median(interquartile range) (IQR) sample size and TESTEX score of the included studies.The type and frequency of participation outcome measures used across all studies were summarized using descriptive statistics.Additionally, studies reporting a participation outcome as their primary outcome measure were identified and tabulated.To identify which aspects of participation were captured within each measure,the linked ICF chapters(d1-d9) were tabulated, and the frequencies of items representing each ICF chapter were summarized.Items that could not be linked to a participation chapter were also tabulated.
2.6.Meta-analytic approach
Mean±SD values for participation outcomes per study were extracted and entered into the Comprehensive Meta-Analysis software (Version 2.0, Biostat; Englewood, NJ, USA).For each study, the effect sizes represent the pre/post change in participation outcomes in the exercise group compared to the non-exercise control group.When multiple measures of participation were included in a single study,an overall mean effect size was generated for that study.The aggregate effect size was estimated using a random-effects model.The random-effects model was selected due to the variance in participant and exercise-training characteristics across the studies.23Additionally,separate effect sizes were calculated by exercise type(i.e.,aerobic training,resistance training,and mixed/other training).Heterogeneity of the overall effect size was examined using the Q statistic,with a significance level of p <0.05 indicating study heterogeneity.An investigation of the potential modifying effects of participant and/or study characteristics(covariates)on the mean overall effect size was explored using meta-regression.23Disability status,disease duration,exercise modality, TESTEX scores, and clinical improvement (i.e.,reported significant improvement) in physiological fitness outcomes(i.e.,aerobic and muscular fitness)were input as categorical variables and tested as potential moderator variables.
3.Results
3.1.Literature search and quality assessment
Fig.1 provides a breakdown of the literature search and screening process.The initial database search yielded 4272 articles and was supplemented by the addition of 4 articles from the authors’ personal datebases.Following the removal of duplicates and irrelevant articles,419 full-text articles were assessed for eligibility.Following the full-text screening process, 49 articles were eligible and were included in the systematic review.24-72For the purpose of presenting the findings of the literature search, these 49 articles were subdivided into 3 categories based on exercise type: aerobic training,24-46resistance training,47-54and mixed/other training(e.g.,combination of aerobic and resistance training, yoga, Pilates).55-72A detailed description of the participants and exercise prescription per study is presented in Supplementary Table 3.The median (IQR) sample size for the included studies was 38(33),with sample sizes ranging from 6 to 314 participants.The median(IQR)TESTEX score for the included studies was 10 (4), with scores ranging from 3 to 14 points.The median TESTEX score of the current review was higher than the median TESTEX score reported in a previous review of 41 exercise trials involving people with MS(median=8).73
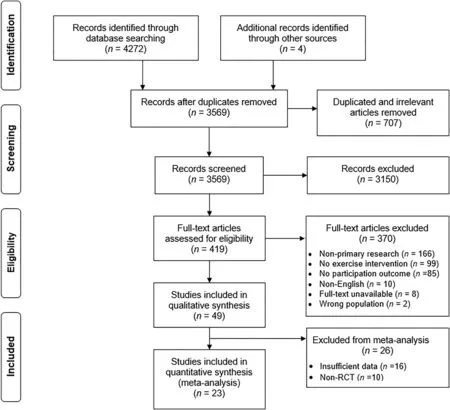
Fig.1.The Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)flowchart of the review.RCT=randomized controlled trial.
3.2.Participation outcomes
A summary of the participation outcome measures used per study is reported in Supplementary Table 4.We retrieved 16 different measures capturing participation across the 49 studies.Most studies25,7-29,31-35,37,39-43,45,47-52,54-57,59,61,63-65,68,70-72included in the review(n=35,71%)used a single outcome measure capturing participation, whereas the remaining 14 studies (29%)24,26,30,36,38,44,46,53,58,60,62,66,67,69used multiple outcome measures capturing participation.Only 6 studies(12%)31,33,36,61-63identified an outcome measure capturing participation as the primary outcome of the study.Across all retrieved outcome measures, all 9 participation chapters (d1-d9)were captured in varying capacities(range:1-7 chapters).Additionally, 89 unique participation categories were represented across the 16 included outcome measures(range:3-54 categories).The 36-Item Short Form Survey (SF-36) was the most commonly used outcome measure capturing participation, reported in 16 (33%) studies.The SF-36 contains 22 items representing 5 different participation chapters.The Multiple Sclerosis Impact Scale-29 was the most prevalent MSspecific outcome measure capturing participation and was reported in 14 studies (29%);36,43,44,46,51,52,54,60,61,66,67,69,71,72it contains 14 items representing 6 unique participation chapters.
A visualization of the frequency of linked ICF participation chapters is presented in Fig.2.“Mobility” was the most commonly represented ICF participation chapter, captured in 108 items across 14 different outcome measures.There were 34 unique ICF participation categories represented across the 108 items capturing mobility.Conversely, communication was the least frequently represented ICF participation chapter, captured by only 4 items across 2 outcome measures.Nonparticipation items accounted for 143 items across the 16 outcome measures.
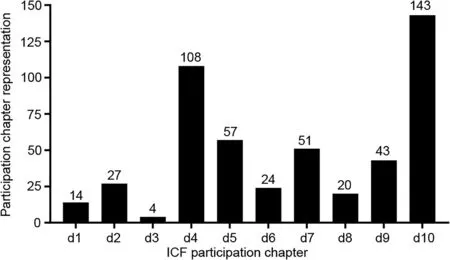
Fig.2.Frequency of ICF participation chapters represented across the retrieved participation outcome measures.d1=learning and applying knowledge;d2=general tasks and demands; d3=communication; d4=mobility; d5=self-care; d6=domestic life; d7=interpersonal interactions and relationships; d8=major life areas;d9=community,social and civic life;d10=nonparticipation item;ICF=International Classification of Functioning,Disability and Health.
3.3.Meta-analytic approach
A subsample of 23 articles was included in the meta-analysis.Mean values for participation outcomes (pre and post)for all 23 RCTs are presented in Supplementary Table 5.Overall,78 individual effect sizes were retrieved from 1093 individuals with MS (exercise training=558; control=535).The overall weighted mean effect size (Hedges’ g) was 0.60 (standard error (SE)=0.12, 95% confidence interval (95%CI):0.36-0.84,z=4.9,p <0.001),indicating a moderate,positive effect of exercise training on participation(Fig.3).The overall effect was heterogeneous(Q=79.7,I2=72.4,p <0.001).The mean effect size for aerobic training(n=13 studies),resistance training(n=4 studies),and mixed/other training(n=6 studies)was 0.68 (SE=0.21, 95%CI: 0.27-1.1, z=3.3, p=0.001),0.47 (SE=0.15, 95%CI: 0.14-0.97, z=3.1, p=0.002), and 0.56 (SE=0.21, 95%CI: 0.18-0.77, z=2.6, p=0.009),respectively.The heterogeneity of effect sizes (I2) for aerobic training, resistance training, and mixed/other training were 80.2 (Q=60.7, p <0.001), 0.00 (Q=0.8, p=0.86), and 71.8(Q=17.8,p=0.003),respectively.
Meta-regression indicated that clinical improvements in physiological fitness accounted for a significant amount of the variation in the observed effect of exercise training on participation (R2=0.42, p < 0.01).Conversely, baseline disability status (R2=0.00, p=0.68), disease duration(R2=0.01, p=0.58), study quality (R2=0.00, p=0.18), and exercise type (R2=0.01, p=0.60) accounted for minimal variability in the observed effects of exercise training on participation.
4.Discussion
The findings from this review indicate considerable breadth and variability in the ways in which participation is captured in studies of exercise training involving persons with MS,as is reflected by the number of outcome measures and the heterogeneity of participation categories represented across the retrieved studies.Further, mobility was the most commonly represented participation chapter.The meta-analysis of 23 RCTs determined that there was a moderate positive effect of exercise training on participation when compared to a nonexercise control condition.Although there is variability in how participation is captured in the MS exercise literature, there appears to be an overall positive effect of exercise training for improving involvement in daily life for persons with MS.
4.1.Capturing participation in exercise training interventions
The 49 retrieved studies included 16 different outcome measures that captured participation to some extent.Given the broad definition of participation within the ICF framework,7such variability in how participation has been captured in exercise studies involving persons with MS is unsurprising.All participation chapters (d1-d9) were represented across the retrieved outcome measures,but there was a noticeable disparity in the frequency of these chapters.For example, mobility(Chapter d4) was by far the most commonly represented participation chapter(108 items),whereas communication(Chapter d3) was represented by only 4 items.There was further variability in the number of participation categories capturedacross outcome measures, ranging between 3 (Godin Leisure-Time Exercise Questionnaire) and 54 items (Sickness Impact Profile),which suggests that some tools may capture participation in a more comprehensive manner than others.The heterogeneity in ICF chapter representation across the retrieved outcome measures reflects that these tools capture differing aspects of participation.Such variability in participation chapter and category representation may impact interpretations of how interventions, including exercise training, influence participation in daily life.Given the heterogeneity in the presentation of MS,certain outcome measures may have greater relevance than others,based on clinical disease characteristics.For instance,an outcome measure composed primarily of mobility items (e.g.,Late Life Function and Disability Inventory)would not be relevant for those with MS and substantial mobility impairment.Instead, an outcome measure composed of a variety of participation chapters(e.g.,Functional Independence Measure or Barthel Index)may be more appropriate.Future studies may benefit from including multiple tools when attempting to capture aspects of participation.Collectively, when selecting outcome measures intended to capture participation, it is important to consider which chapters and categories are represented, and whether a selected tool is aligned with intervention content and participant characteristics.
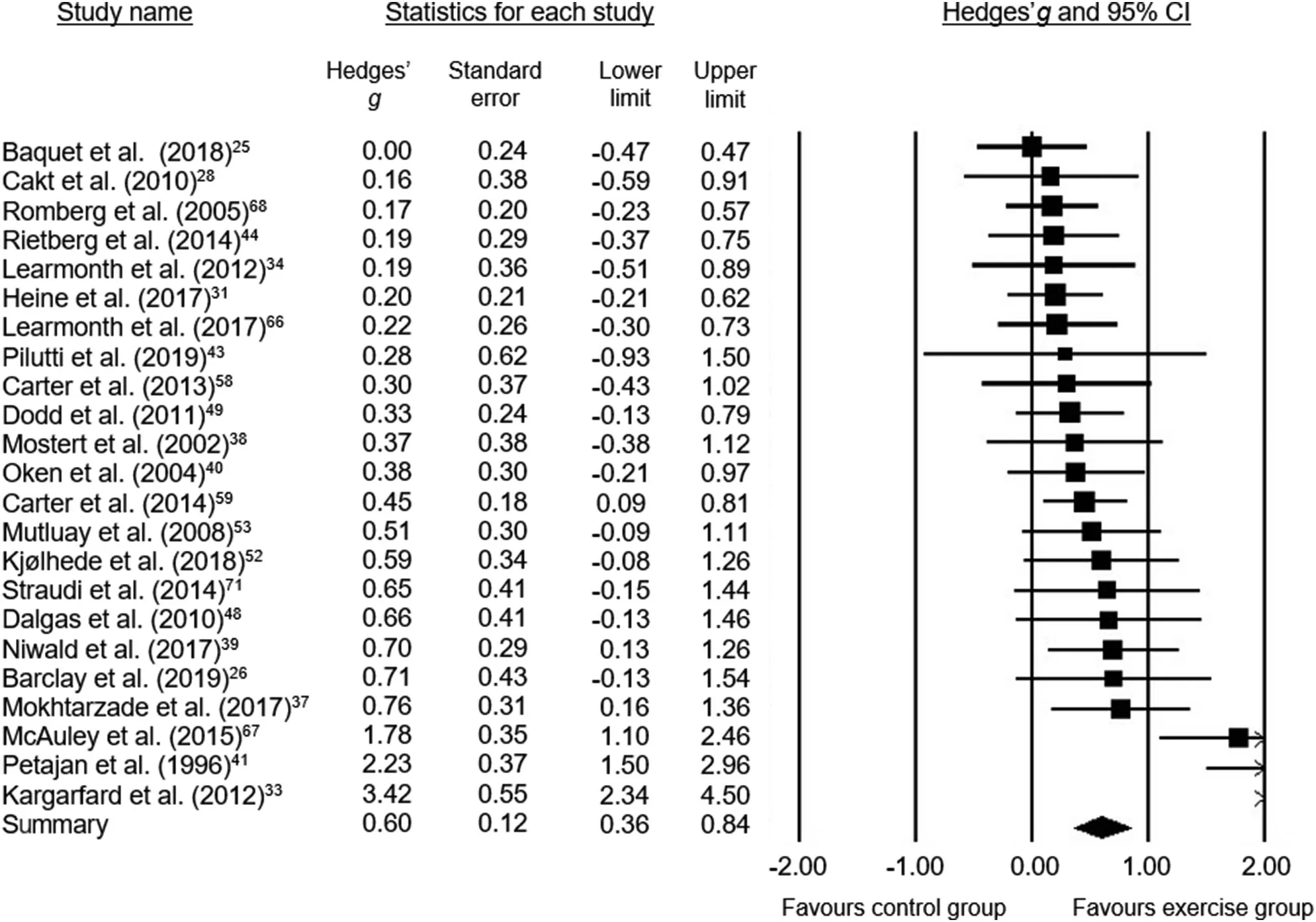
Fig.3.A visual representation of the overall effect size(Hedges’g)for all 23 studies included in the meta-analysis.95%CI=95%confidence interval.
The participation chapters and categories captured in the retrieved outcome measures have considerable overlap with those identified in the brief and comprehensive ICF core sets for persons with MS.6Indeed, the brief ICF core set for MS identifies solving problems, carrying out daily routines,walking, family relationships, and remunerative employment as the essential participation categories that should be used when characterizing participation in those with MS.6
When examining the most commonly represented participation chapters across included outcomes, walking and family relationships are found to be adequately represented as Chapter d4 (mobility) and Chapter d7 (interpersonal interactions and relationships);they were the first and third most frequently represented participation chapters, respectively.This suggests that outcome measures capturing participation in studies of exercise training are covering some relevant aspects of participation, as identified by expert consensus.However,other relevant aspects of participation may not be reflected in these outcome measures.For example,chapter d1(learning and applying knowledge)and Chapter d8(major life areas)were the second and third,respectively, least represented chapters across outcome measures in our review, despite being represented on the brief ICF core set for MS.6This seems to indicate that although many relevant categories of participation are being adequately captured, there remain some categories of participation that may be overlooked by existing tools.The ICF core and comprehensive sets for MS provide direction concerning potential categories of relevance,but it is also important to consider participants’ perspectives when selecting outcome measures as endpoints for research and clinical practice.
One cross-sectional study involving 113 persons with MS sought to identify the patient-reported aspects of participation most intensely impacted by MS.7In that study, community,social and civic life (Chapter d9), mobility (Chapter d4), anddomestic life(Chapter d6)were identified as the most strongly impacted aspects from a patient’s perspective.Conversely,communication (Chapter d3) was cited as the least impacted.It is interesting that although mobility categories were adequately represented in items across the outcome measures retrieved in our review, items representing community, social and civic life (Chapter d9), and domestic life (Chapter d6)were relatively scarce.The incongruence between categories identified as most strongly impacted by persons with MS and those captured by current outcome measures highlights the potential need for inclusion of different or new tools to capture participation and the impact of interventions on engagement in daily life.For instance, an outcome measure describing community, social, and civic life (Chapter d9) or domestic life(Chapter d6)may capture more meaningful changes in participation from a participant’s perspective compared to some of the currently used outcome measures.
Despite the importance of participation outcomes, 85 articles of 419 full-text articles were excluded from the current review because of the absence of any outcome capturing participation.Furthermore, only ~10% of the included articles identified an outcome capturing participation as its primary outcome, indicating that participation outcomes have been largely overlooked in the existing literature concerning exercise training in those with MS.Ideally, the results from this review can facilitate more frequent inclusion of outcomes that capture participation in future studies of exercise training in MS by providing a detailed breakdown of which participation chapters and categories have been captured in current outcome measures.Results from this review can be further cross-referenced with the established ICF core set for MS6as well as with patient-reported chapters and categories of relevance.7Our analysis can be used by clinicians and researchers to identify which outcome measures capture the most relevant aspects of participation.Ultimately, the strategic inclusion of these outcomes can provide greater insight into the benefits of exercise training on everyday life for persons with MS.
4.2.Effects of exercise training interventions on participation
This review is the first to demonstrate the effects of exercise training on participation in persons with MS.The magnitude of the effect size reported herein is somewhat larger than previous meta-analyses examining the effects of exercise training on physical fitness,symptoms of fatigue,and mobility.11,74,75From a clinical perspective,this novel finding is particularly important because persons with MS have demonstrated restricted levels of participation compared to controls without MS.4Indeed, a cross-sectional study involving 105 people with MS reported that approximately 77% of the sample had significantly restricted societal participation—as measured by the Community Integration Questionnaire—when compared to age- and sex-matched controls without MS.8The findings from our review provide evidence for the role of exercise training in increasing and maintaining engagement in everyday life and,consequently,they add to the body of literature supporting exercise training as a disease-management strategy for MS.76
In the current analysis, clinical variables, such as baseline disability and disease duration, had no statistically significant influence on the effect of exercise training on participation,which suggests that improvements in participation may be possible, irrespective of disability or disease burden.Studies involving aerobic exercise training had the largest effect size when compared to resistance and mixed/other exercise types,although there were no statistically significant differences in the overall effect by exercise type.Further, clinically relevant improvements in physiological fitness accounted for significant variation(>40%)in the observed effect of exercise training on participation, suggesting a relationship between improved physiological fitness and increased participation.Interestingly, people with progressive MS have demonstrated greater oxygen requirements when completing activities of daily life compared to controls without MS.77Further, crosssectional associations have been reported between cardiorespiratory capacity and instrumental activities of daily living in persons with MS.78It is important to note that we recognize the potential bidirectional nature of the relationship between physiological fitness and participation, and such associations should be examined in future intervention trials.
4.3.Limitations
The current systematic review and meta-analysis have limitations that must be considered when interpreting the results.First,the identification of outcome measures that capture participation can be challenging, with the potential for overlap with other component levels, particularly activities.Therefore, there may have been reviewer bias in the selection of studies included in the review.As a result,measures that capture some elements of participation may not have been included in the final analysis.Additionally, many of the retrieved studies included participation-outcome measures as secondary outcomes,likely resulting in many studies that were underpowered to detect potential changes in these outcomes.It is also important to acknowledge that despite widespread use, there are no published cut-points for the TESTEX scale, limiting the classification of articles in terms of study quality.The sample size of many of the retrieved studies was relatively small,which may be problematic in terms of power and responsiveness,as the time-courses of changes in participation outcomes may differ from those of other outcomes(i.e.,may evolve more slowly).Finally,there was a small number of heterogeneous studies within each exercise-type subgroup.Consequently, these effects should be interpreted with caution at this stage.
5.Conclusion
The findings from this review demonstrate considerable variability in the ways in which participation has been captured in studies of exercise involving those with MS.A range of participation categories was represented across the identified outcome measures, with a notable focus on involvement in mobility.Our characterization of outcome measures that capture participation using established ICF coding rules can be used to inform the selection of outcomes in future studies ofexercise training in people with MS.Additionally, exercise training had a moderate positive effect on participation.Given the importance of participation for people living with MS,such outcomes deserve more attention and inclusion in future exercise studies involving people who have MS.
Acknowledgment
Funding for this review and collaboration were provided by the Canadian Institutes of Health Research Canada Graduate Scholarships and the Michael Smith Foreign Study Supplement program(Funding number:162728).
Authors’contributions
TE conceptualized the idea and objective of the review,performed the literature searches,data extraction,methodological quality assessment, ICF coding, and meta-analysis and was responsible for drafting the manuscript; ASM performed data extraction and methodological quality assessment; AOF performed data extraction and ICF coding; UD conceptualized the idea and objective of the review; LAP conceptualized the idea and objective of the review and assisted in methodological quality assessment and ICF coding.All authors provided feedback and critically revised the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2021.07.007.
 Journal of Sport and Health Science2022年3期
Journal of Sport and Health Science2022年3期
- Journal of Sport and Health Science的其它文章
- The secrets to running economy
- Metabolic and performance responses of male runners wearing 3 types of footwear:Nike Vaporfly 4%,Saucony Endorphin racing flats,and their own shoes
- Longitudinal bending stiffness does not affect running economy in Nike Vaporfly Shoes
- Can changes in midsole bending stiffness of shoes affect the onset of joint work redistribution during a prolonged run?
- Metabolic cost of level,uphill,and downhill running in highly cushioned shoes with carbon-fiber plates
- Systematic reduction of leg muscle activity throughout a standard assessment of running footwear