
Predictors of multiple injuries in individual distance runners:A retrospective study of 75,401 entrants in 4 annual races-SAFER XX
2022-06-09 09:23SonjSwnevelderNicolSewryMrtinSchwellnusEsmeJordn
Sonj Swnevelder,Nicol Sewry,Mrtin Schwellnus,d,*,Esme Jordn,e
a Biostatistics Unit,South African Medical Research Council,Parow 7575,South Africa
b Sport,Exercise Medicine and Lifestyle Institute(SEMLI),Faculty of Health Sciences,University of Pretoria,Pretoria 0081,South Africa
c International Olympic Committee(IOC)Research Centre,Pretoria 0081,South Africa
d Emeritus Professor of Sport and Exercise Medicine,Faculty of Health Sciences,University of Cape Town,Bellville 7535,South Africa
e Statistics and Population Studies Department,University of the Western Cape,Bellville 7535,South Africa
Abstract Background: There are limited data on factors that predict an increased risk of multiple injuries among distance runners.The objective of this study was to determine risk factors that are predictive of individual runners with a high annual multiple injury risk(MIR). Methods:A retrospective,cross-sectional study at 4 annual(2012-2015)Two Oceans 21.1 km and 56.0 km races in South Africa with 75,401 consenting race entrants.Running-related injury data were collected retrospectively through an online pre-race medical screening questionnaire.The average number of injuries for each runner every year was calculated by taking a runner’s race entry history and injury history into account and categorizing entrants into 4 MIR categories(high,intermediate,low,and very low(reference)).Multiple logistic regression modeling(odds ratios)was used to determine whether the following factors were predictive of a high MIR(average >1 injury/year):demographics,training and racing,chronic-disease history(composite chronic disease score(CCDS)),and history of allergies. Results:Of all entrants,9.2%reported at least 1 injury,and 0.4%of entrants were in the high MIR category;the incidence rate was 2.5 injuries per 10 runner-years(95%confidence interval(95%CI):2.4-2.7).Significant factors predictive of runners in the high MIR category were:running for >20 years:OR=2.0(95%CI:1.3-3.1;p=0.0010);a higher CCDS:OR=2.2(95%CI:2.0-2.4;p <0.0001);and a history of allergies:OR=2.8(95%CI:2.0-3.8;p <0.0001). Conclusion:Runners who have been running recreationally for >20 years and those with multiple chronic diseases or a history of allergies were at higher risk of multiple running-related injuries.This high-risk group can be targeted for further study and possible injury-prevention interventions.Keywords: Allergies;Chronic diseases;Multiple injuries;Risk factors;SAFER study
1.Introduction
In recent years, physical activity has been actively promoted, and the levels of participation by recreational runners in mass-participation events have increased.1-4
Despite obvious health benefits, running does have a high risk of injury,with 20%-80%of runners reporting a runningrelated injury in a 12-month period.5The incidence and prevalence of gradual-onset running-related injuries (RRIs) have been extensively reported,as have the demographic-(age,sex,body mass index (BMI)) and training- (mileage, frequency)related risk factors associated with these injuries.In a recent systematic review, the following general risk factors for RRIs among long-distance (>20 km/week) runners were identified:having a previous RRI was the most important risk factor,followed by a BMI greater than 26.6General risk factors among short-distance(<20 km/week)runners were:previous injuries not attributed to running, higher BMI, older age, being male,having no previous running experience, and running volume.6However, chronic disease as a risk factor for RRIs has been the subject of far less investigation.In the general population,obesity, diabetes mellitus, and hypercholesterolemia have been associated with tendinopathies,a common RRI.7-9It has also been reported for the first time recently that chronic disease can predict gradual-onset musculoskeletal injuries incyclists.10In 21.1 km and 56.0 km distance runners,the prevalence of chronic disease was shown to be as high as 13.1%.Therefore,underlying chronic disease should be considered in models when investigating predictors of RRIs.11
Other than risk factors, the methodology of studying and reporting multiple injuries among pooled individuals in only 1 season has been extensively discussed in a recent systematic review.12However,there are very few studies that investigated or reported multiple injuries per individual runner per year and over more than 1 season.12Multiple injuries in distance runners can,therefore,be defined as individual runners with more than 1 injury per year.The authors are not aware of any studies where risk factors predictive of runners with multiple injuries have been investigated.To report an individual annual injury incidence,it is important to count the number of injuries in individuals accurately and consistently.12We acknowledge studies that have recorded the number of injuries per individual; however,they have not analysed multiple injuries on the individual level.We hypothesize that a sub-group of individual runners are at greater risk of multiple injuries per year.Therefore, the aim of the present study was to determine predictors of a sub-population of runners with a high annual individual multiple injury risk (MIR) from a group who entered mass community-based running events over 4 years by using injury data obtained from a pre-race online medical-screening questionnaire.
2.Methods
2.1.Study design
This retrospective,cross-sectional study used pre-race questionnaire data collected at 4 annual(2012-2015)Two Oceans 21.1 km and 56.0 km races.
2.2.Participants and data collection
This study forms part of a series of studies known as the SAFER (Strategies to reduce Adverse medical events For the ExerciseR) studies.Potential participants for this study were all entrants for 4 annual (2012-2015) Two Oceans Marathon(21.1 km and 56.0 km) running events in South Africa.Both races are run on the same day every year, so a specific runner could have entered only between 1 and 4 times.In each of the 4 annual races, the race entrants’ demographic data and raceday data on starters and finishers were obtained with permission from the race organizers.Demographic and race data are in the public domain and are available on the race website.13Entries for the ultra-marathon (56.0 km) race required a sub-5 h 42.2 km qualifying time; however, entry to the halfmarathon (21.1 km) event was open to all.Consenting entrants—defined as any runner registering for any of the annual races from 2012 to 2015—who gave online signed consent for his/her data to be used for analyses were considered as participants for this study.
2.3.Pre-race medical screening data
As part of the entry process for the 4 annual races from 2012 to 2015,a compulsory online pre-race medical screening questionnaire and an educational intervention were implemented.Previously described in detail, data collection consisted of information obtained from a compulsory pre-race medical screening questionnaire or“self-assessment of risk”.14Injury-related questions were asked, and data were collected retrospectively.This questionnaire was based on the European Society of Cardiology(ESC)and the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) guidelines15and has been described in depth previously, as has the educational intervention.11,14Upon completion, participants were given the opportunity to consent to their data being used for research purposes.
The Research Ethics Committee of the University of Cape Town(REC 009/2011,REC 030/2013)approved the protocol,and the University of Pretoria (REC 433/2015) approved the on-going data collection and subsequent analysis of the data.
2.4.Self-reported injury data,definition of chronic injury,and the outcome question
For each of the 4 annual races, when completing the compulsory pre-race medical questionnaire,entrants were asked to retrospectively self-report on any chronic injuries in the past year.The definition of a chronic injury was included in the specific question that each runner was asked: “Do you or did you suffer from any symptoms of a chronic(no accident)running injury (muscles, tendons, bones, ligaments, or joints) in the past 12 months or currently?Note:Only if an injury is/was severe enough to interfere with running or require treatment,e.g., use medication or require you to seek medical advice from a health professional”.Following this initial question,entrants then had to report detailed information on the specific injury.An entrant could have reported no injuries,1 injury,or up to 3 injuries in any of the years over the 12 months preceding each of the 4 annual races.The questionnaire therefore allowed entrants to report multiple injuries to a maximum of 3 injuries in a year for each of the 4 years.This meant an entrant could potentially report between 0 and 12 injuries in the 12 months preceding each of the 4 annual races.Injuries included first injuries and subsequent injuries(new,recurrent,re-injury,or exacerbation of an injury).16The recorded chronic injury/injuries information was used to define the “entrant’s injury history” for a specific year.It took into account that year and the preceding years’injuries,namely,cumulative injuries over preceding years and the current year, which resulted in an entrant’s injury history changing from 1 year to the next year they entered,akin to a“moving”injury history.
2.5.Definition of MIR as the primary outcome
The average number of injuries in the preceding 12 months was calculated for each entrant every year by dividing the number of multiple injuries an entrant reported over the years(up to the race’s entry year)by the number of years the entrant accumulated the injuries (Supplementary Table 1).The average was reported for each of the possible 4 years the entrant entered the race and could range from 0(never injured)to 3(3 injuries per year and entered for 4 years).We categorized theaverage number of injuries for each entrant every year (avg)into 4 MIR categories as follows: very low (never injured,avg=0),low(avg <1),intermediate (avg=1),and high (avg>1)(Supplementary Table 2).The analysis focused on determining risk factors predictive of a high MIR.High-MIR entrants have,on average,reported more than 1 annual injury.The severity of the injury as self-assessed and reported by the runner had no influence on the calculation and subsequent categorization of MIR.
2.6.Primary objective:Risk factors predictive of a high MIR
Using data from the screening questionnaire, 4 individual broad categories of risk factors predictive of high MIR were explored in this study: Demographics, training load-related variables,history of chronic diseases,and allergies.More specifically, demographic variables included sex, age group, and race distance (half- or ultra-marathon).Training load-related variables included years of recreational running, frequency of training/racing per week, weekly training mileage, average self-reported training speed(km/h),and Two Ocean race experience (namely, number of times run).The number of years running recreationally was categorized into 3 categories:>20 years, 10-20 years, and <10 years.A race entrant was categorized as “experienced” if the entrant had run 2 or more Two Ocean races in the past and as “inexperienced” if the entrant was either a novice to the Two Ocean races or had run only 1 previous race.Histories of chronic diseases and allergies were obtained from the pre-race medical screening variables: history of cardiovascular disease (CVD), CVD symptoms, CVD risk factors, other chronic diseases (metabolic/endocrine, respiratory, gastro-intestinal disease (GIT),nervous system/psychiatric, kidney/bladder, hematological/immune, cancer), and allergies.A composite chronic disease score (CCDS) was calculated as the sum of an individual’s answers to the 10 chronic-disease questions(CVD risk factors,CVD symptoms, CVD history, metabolic/endocrine, respiratory, GIT, nervous system/psychiatric, kidney/bladder, hematological/immune,cancer),and it ranged from 0 to 10.10,17-19
2.7.Statistical analysis
All data from the 2012-2015 runner and medical questionnaire database were entered into an Excel spreadsheet(Microsoft Excel,Microsoft 2010,Redmond,Washington,USA)and then analyzed using the STATA/SE statistical program (Version 15.1,StataCorp LLC,College Station,TX,USA).
The primary outcome (MIR with 4 responses) was previously described.Because of the multiple outcomes,a multiple logistic regression was used to estimate odds ratios (ORs) for 3 of the MIR outcomes (high, intermediate, low) in comparison to the very low MIR (reference group).Demographic risk factors that were individually investigated were: sex (unadjusted),age group(unadjusted),and race distance(adjusted for sex and age group because the sex and age profiles differed between the race distances).The models for “years of recreational running”, experience, CCDS, and allergies were adjusted for sex,age group,and race distance.The 2 older-age categories(41-50 years and >50 years)were combined into a>40 years category because their results were similar.Although the CCDS was modeled as a numerical risk factor(0,1-10)(as described in a previous section),for the purpose of statistical analysis the CCDS is reported only at scores of 1,2,and 3 because of the small frequencies of scores of ≥4.
The correlated structure of the data(i.e.,the same runner could run more than 1 year and have multiple injuries)was accounted for by specifying that the standard errors allow for intragroup correlation and, thus, specifying that runners with the same ID belong to the same cluster.Odds ratios (ORs) and (95% confidence intervals(95%CIs)were reported for all results.
A final multiple logistic regression model (ORs, 95%CI)was run to confirm the results of the univariate analyses.It included all the univariate risk factors that were significant(p <0.01), adjusting for sex, age group, and race distance.The risk factor “experience” was removed from the final model because “experience” and “years running recreationally” are correlated, and “years running recreationally”had a stronger association with a high MIR.
3.Results
Runners (n=106,743) entered the 4 annual races(2012-2015), and 75,401 runners gave consent for their questionnaire data to be analyzed.To determine whether the consenting participants from this study were representative of all race entrants,the 2 groups were profiled by age group,sex,and race distance,as shown in Supplementary Table 3.There was a small but significantly higher (p=0.0009) percentage of halfmarathon entrants (0.7%) who participated in this study, compared to all race entrants.However, the age and sex of all and consenting entrants were similar.Of the 75,401 consenting race entrants who took part in this study, 47,333 were unique runners.Of the 10,576 ever-injured race entrants,7281 entrants had been injured in the preceding 12 months, and they reported 7623 injuries in total.Although 90% of race entrants were not injured in the 12 months preceding each of the 4 annual races,6959 entrants (9.2%) reported 1 injury, 302 entrants (0.4%)reported 2 injuries, and only 20 entrants (0.03%) reported 3 injuries during this period.The most common anatomical region where injuries were reported was the lower limb (93% of all injuries).The 5 most common lower-limb injuries (by body area) were: knee (32%), shin/calf (20%), foot/ankle (17%),achilles tendon(10%),and hamstring(8%).
3.1.The frequency and incidence of multiple injuries
Most entrants reported a very low MIR (n=64,825;MIR=83.7%; 95%CI: 83.2-84.2), whereas a few entrants reported a high MIR(n=301;MIR=0.4%;95%CI:0.4-0.5).All other entrants reported an intermediate (n=5035) or low(n=5240) MIR.(Further details of the MIR categories are to be found in Supplementary Table 4).

Table 1The frequency(%),OR,and 95%CI for each MIR category in race entrants by years of recreational running(adjusted for sex,age group,and race distance).
The incidence rate (IR) of multiple injuries was 2.5 injuries per 10 runner-years(95%CI:2.4-2.7),and the IR for ultra-marathon runners (2.6 injuries per 10 runner-years; 95%CI:2.5-2.8)was significantly higher than the IR for half-marathonrunners (2.3 injuries per 10 runner years; 95%CI: 2.2-2.5)(incidence risk ratio=1.1;95%CI:1.1-1.2;p=0.0002).
3.2.Risk factors predictive of a high MIR:Univariate analyses
3.2.1.Demographic factors(sex,age groups,and race distance)
Male runners relative to female runners had similar odds for being in the high MIR category compared to the very low MIR category(OR=1.0;95%CI:0.8-1.3;p=0.9280)(Supplementary Table 5).The odds for males compared to females in the low MIR category were higher when compared to the very low MIR category(OR=1.2;95%CI:1.1-1.2;p <0.0001).
The frequency,OR,and 95%CI for each MIR category in race entrants by 3 age groups is shown in Supplementary Table 6,and by 4 age groups in Supplementary Table 7.
Runners older than 40 years relative to runners ≤30 years have significantly higher odds of being in the high MIR category compared to runners in the very low MIR category(OR=2.4;95%CI:1.7-3.5;p <0.0001).
The frequency, OR, and 95%CI for each MIR category in race entrants by race distance(adjusted for sex and age group)are shown in Supplementary Table 8.
Ultra-marathon runners(56.0 km)relative to half-marathon(21.1 km) runners have significantly higher odds of being in the high MIR category compared to the very low MIR category(OR=2.1;95%CI:1.5-2.9;p <0.0001).Both the intermediate and low MIR categories,relative to the very low MIR category, have an OR=1.5 (p <0.0001) when comparing the ultra-marathon runners to the half-marathon runners.
3.2.2.Training load,racing history,and Two Oceans experience
Of the measures of training load that were investigated,the following were not significantly associated with a high MIR(p >0.05): frequency of training or racing per week, weekly training mileage, and average self-reported training speed(km/h).However, “years of recreational running” and Two Ocean’s race experience were both significantly associated with a high MIR.The frequency, OR, and 95%CI for each MIR category in race entrants by “years of recreational running” (adjusted for sex, age group, and race distance) are reported in Table 1.
Runners who have been running recreationally for >20 years have significantly higher odds than runners running recreationally for <10 years of being in the high-MIR category as opposed to in the very low-MIR category,irrespective of age group,sex,or race distance (OR=2.5; 95%CI: 1.7-3.7; p <0.0001).However,runners who have been running recreationally for between 10 and 20 years did not have significantly higher odds of being in the high-MIR category as opposed to the very low-MIR category compared to runners running recreationally for < 10 years(OR=1.2; 95%CI: 0.8-1.6; p=0.4160).The higher the MIR,the higher the OR is among runners who have run recreationally for >20 years.Therefore, a runner with a longer running career has a higher risk of being in the high-MIR category.
The frequency, OR, and 95%CI for each MIR category in race entrants by Two Ocean’s race experience (adjusted for sex,age group,and race distance)are reported in Table 2.
Experienced Two Ocean’s runners, compared to inexperienced Two Ocean’s runners,have significantly higher odds of being in the high MIR category as opposed to the very low MIR category, irrespective of age group, sex, or race distance(OR=1.7;95%CI:1.3-2.2;p <0.0001).
3.2.3.History of chronic disease and allergies
In our study population, 74.2% of the entrants had a composite chronic disease score(CCDS)of 0(no chronic disease),18.5 % had 1 chronic disease, 5.5% reported 2 chronic diseases, and 1.8% had ≥3 chronic diseases (Supplementary Table 9).All the chronic diseases that contribute to the CCDS are reported in Supplementary Table 10.For runners with an RRI who had up to 3 chronic diseases (CCDS=1; 2; 3), the specific chronic disease risk factors that contributed the most to the CCDS were: “any CVD risk factors” (19.4%),“respiratory disease”(14.9%),and“GIT disease”(5.7%).
Results for the CCDS are reported in Table 3, which displays the CCDS number and OR (95%CI) for each MIR category for a CCDS of 1, 2, and 3 (adjusted for sex, age group,and race distance).

Table 2The frequency(%),OR,and 95%CI for each MIR category in race entrants by Two Ocean’s race experience(adjusted for sex,age group,and race distance).

Table 3The OR and 95%CI for each MIR category in race entrants by their composite chronic disease score(adjusted for sex,age group,and race distance).
These data show that if a runner with a CCDS of 1 increases his/her CCDS by 1 unit,the risk of being in the high MIR risk category as opposed to the very low MIR category increases by a factor of 2.4(p <0.0001).Similarly,if a runner with a CCDS of 2 increases his/her CCDS by 1 unit, the risk of being in the high MIR category as opposed to the very low MIR category increases by a larger factor of 5.7(p <0.0001).Also,the higherthe MIR is,the higher the OR is among runners with increased CCDSs.This means that an increase in the CCDS correlates with an increased risk of being in the high MIR category.Fig.1 shows the steeper increase in risk for runners in the high MIR category compared to the intermediate and low MIR categories.
The MIR category by history of allergies (adjusted for sex,age group,and race distance)is reported in Table 4.
Runners with histories of allergies have significantly higher odds than runners with no histories of allergies of being in the high MIR category as opposed to the very low MIR category(OR=4.5;95%CI:3.4-6.1;p <0.0001).The higher the MIR,the higher the OR is among runners with histories of allergies.The risk of being in the high MIR category is also significantly different from that of both the intermediate(OR=1.9;95%CI:1.4-2.5; p <0.0001) and the low MIR categories (OR=2.5;95%CI:1.8-3.4;p <0.0001).
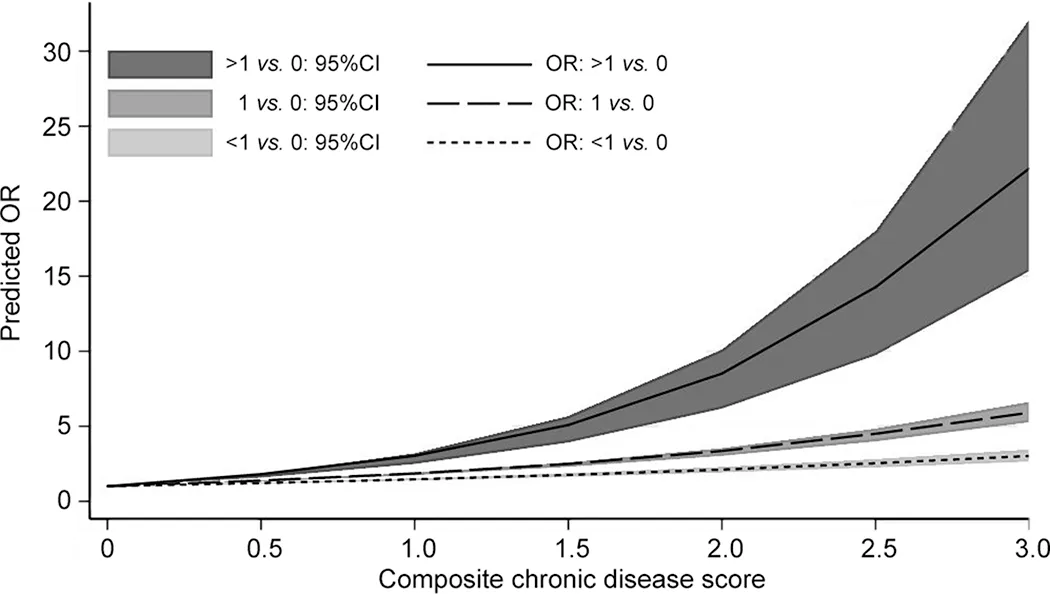
Fig.1.The predicted OR for the CCDS for each MIR category compared to the very low MIR.Continuous composite chronic disease score reported only up to 3(right-censored at 3)to make the graph more clear.95%CI=95%confidence interval; CCDS=composite chronic disease score; MIR=multiple injury risk;OR=odds ratio.
3.3.Risk factors predictive of a high MIR:Multivariate analysis
The final multiple logistic regression model included all significant univariate risk factors (p < 0.01) except for“experience”, adjusting for sex, age group, and race distance.The adjusted odds ratios(ORs;95%CI)of runners with a high MIR are reported in Table 5.

Table 4The frequency(%),OR,and 95%CI for each MIR category in race entrants by history of allergies(adjusted for sex,age group,and race distance).
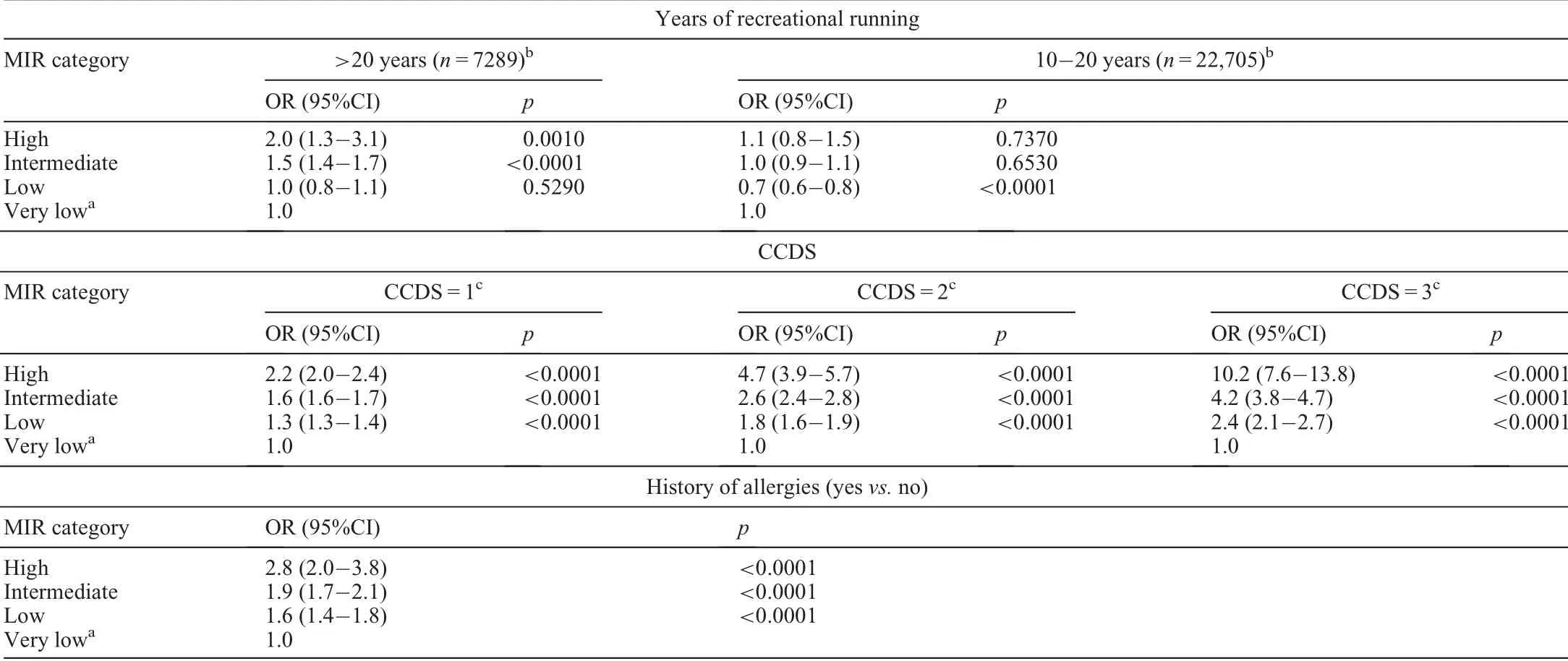
Table 5Final multiple logistic regression model:OR and 95%CI for each MIR category in race entrants(adjusted for sex,age group,and race distance).
Three risk factors were significantly associated with a high MIR: (1) running recreationally for >20 years as opposed to<10 years(OR=2.0;95%CI:1.3-3.1;p=0.0010);(2)higher ORs among runners with increased CCDSs (i.e., if a runner with a CCDS of 1 increases his/her CCDS by 1 unit to 2 chronic diseases, the risk of being in the high MIR risk category as opposed to the very low MIR category increases by a factor of 2.2(OR=2.2;95%CI:2.0-2.4;p <0.0001);if a runner with a CCDS of 2 increases his/her CCDS by 1 unit to 3 chronic diseases,the risk of being in the high MIR category as opposed to the very low MIR category increases by a factor of 4.7 (OR=4.7; 95%CI: 3.9-5.7; p <0.0001); and if a runner with a CCDS of 3 increases his/her CCDS by 1 unit to 4 chronic diseases,the risk of being in the high MIR category as opposed to the very low MIR category increases by a factor of 10.2(OR=10.2;95%CI:7.6-13.8;p <0.0001);and(3)a history of allergies as opposed to no history of allergies(OR=2.8;95%CI:2.0-3.8;p <0.0001).
4.Discussion
The aim of our study was to identify individual risk factors that may be predictive of runners with high MIRs.The main finding was that independent risk factors predictive of high-MIR runners included: runners >40 years (OR=2.4; p < 0.0001), ultramarathon runners(56.0 km)(OR=2.1;p <0.0001),recreational runners for >20 years(OR=2.0;p <0.0010),higher CCDSs(OR=2.2;p <0.0001),and histories of allergies(OR=2.8;p <0.0001).
Although the majority of runners (86%) had never been injured over the 4-year period, the overall injury IR was 2.5 injuries per 10 runner-years, and the prevalence of high-MIR runners (who reported an average >1 injury per year) was 0.4%.This incidence is relatively low compared to other studies,which have previously reported between 19.4%and 79.3%gradual-onset RRI every year, especially in the lower extremities.5,20-22Although this finding was not the primary aim of the study,this discrepancy and the possible differences in populations accounting for this discrepancy should be investigated further.
One of our novel findings was that a history of chronic disease is predictive of runners with high MIRs.Almost 19% of all study entrants reported at least 1 chronic disease;however,among entrants with high MIRs, 26% had 1 chronic disease,and 9.7%and 3.2%had 2 and 3 chronic diseases,respectively.If the number of chronic diseases in a runner increased from 1 to 2(1 unit),the runner’s odds for being in the high MIR category as opposed to the very low MIR category would increase by a significant factor of 2.2.Furthermore, 5% of runners reported 2 chronic diseases.If they should increase their score from 2 to 3(1 unit),their odds for being in the high MIR category as opposed to the very low MIR category would increase by the much larger factor of 4.7.When comparing the intermediate MIR to the very low MIR,the odds ratio is 1.6;and comparing the low MIR to the very low MIR,the odds ratio is 1.3.This means that an increase in the CCDS produces a higher risk of being in the high MIR category.Previous studies have shown that chronic diseases are common among endurance runners (an estimated point prevalence of 2.3%-13.1%) and that 16.1% of these runners had at least 1 risk factor forCVD.11Other studies also specifically report that chronic diseases like diabetes mellitus and hypercholesterolemia are associated with injury.7,9We do realize that most of the runners with chronic diseases are probably also on a number of chronic medications,which could influence the risk of injury in runners.We recently reported the relationship between chronic disease and risk of gradual-onset injury in cyclists.10In this cycling cohort,it was indicated that the potential mechanism/s for explaining the relationship between chronic disease and risk of gradual-onset injuries in recreational cyclists requires further study.10There is also evidence that medications used to treat chronic diseases can be associated with increased risk of tendinopathies,23-26ligament injuries,24,26and bone-stress injuries.27,28Hypercholesterolemia, diabetes mellitus,and metabolic syndrome are chronic diseases associated with chronic tendinopathy.23,24,29It is important to note that,because of our cross-sectional design,we cannot establish a cause-effect relationship between chronic disease and high risk of MIR in runners.
Another novel finding was that runners with histories of any form of allergy have significantly higher odds than those with no histories of allergies of being high MIR runners as opposed to very low MIR runners.We previously documented an association between a history of allergies and gradual-onset injury in other populations of recreational cyclists.10Allergies are common in the general population.In a Finnish study,non-elite long-distance runners had a prevalence of allergic disease similar to that of the general public.30In London Marathon runners, 40% of runners had allergies, as defined by both a positive Allergy Questionnaire for Athletes and elevated specific immunoglobulin E levels.31Runners with allergies are likely to be taking antihistamines, especially because endurance running is an outdoor activity.One of the oral sedating H1antihistamines, Promethazine, has been associated with severe tissue injury,including gangrene.32In future research,the relationship between injury and a history of allergies should be investigated further.
Another interesting result with respect to training load was that although neither weekly running mileage nor any of the other training-related risk factors were predictors of a high MIR, the number of years running recreationally was.It was specifically those runners who had been running for>20 years, irrespective of age group or sex, who had significantly higher odds of being high as opposed to very low-MIR runners, when compared to those who had been running for<10 years.It has been reported that contrary to popular beliefs,weekly mileage was not a significant factor for overuse running injuries.20Our study supports this result, in that weekly mileage, frequency of training, and racing per week were not predictive of being a high-MIR runner.However,our study does suggest that the number of years a runner has been running should be further investigated because that might be predictive of runners who sustain multiple injuries.
This study also found that ultra-marathon runners have significantly higher odds of being in the high MIR as opposed to the very low MIR category relative to half-marathon runners.A previous study reported that among recreational runners, women reported injuries at a higher rate than men.20Our study, however, did not find any association between sex and high-MIR runners, but we cannot compare these findings directly to those of previous studies because we studied runners reporting multiple injuries, and other studies reported only runners with a single injury.Last, with respect to age,all 3 older age groups had significantly higher ORs of being in the high as opposed to the very low MIR category when compared to the youngest age group(≤30 years).
The study has a few specific limitations.First,all data came from self-reported questionnaires,and the diagnoses of injuries were not confirmed by health professionals.Although the injuries were self-reported, the reported injuries were crosschecked with the detailed injury information provided, and only true injuries were reported in this study.Second, runners had to recall their training and injury history over the previous 12 months, which could potentially lead to recall bias.Third,we could not confirm any cause-effect relationships between the risk factors due to the cross-sectional design of the study.Fourth, other risk factors that could potentially play roles in MIR among runners (body mass index), specific medications,type of training/surface, biomechanics, etc.) were not addressed in our study.Fifth, we acknowledge that we have not accounted for recurrent/re-injuries, and have counted only multiple injuries to a maximum of 3 per year.Sixth, results from this study are dependent on the definition we chose for a high-MIR runner,and further investigation could be performed using different definitions to confirm the results of this study.
However,an important strength of the study is its large sample size (>75,000 race entrants), which was representative of the bigger sample of all race entrants(n=106,743)with respect to sex and age groups (although there were slightly more halfmarathon than ultra-marathon entrants in our study).Our study also included 2 endurance-race distances, a shorter half-marathon distance and an ultra-distance (56.0 km).We conducted a retrospective analysis of data collected at 4 annual races to follow-up on individual runners’ cumulative entries and cumulative injury histories,which produced individual-level incidence data.This approach addresses previous limitations in injuryincidence studies that used pooled instead of individual-level data.We also included multiple seasons as opposed to just 1.12Last, all our data are online and automated, which will further enhance analytical methods and reporting in the future.
As far as we know,“high MIR”is a novel term for runners who have on average >1 annual injury and,subsequently,has never before been investigated with respect to risk factors.
5.Conclusion
Independent risk factors that were predictive of high-MIR runners include older age, ultra-marathon distance, running recreationally for more than 20 years, an increase in the runners’CCDS, and histories of allergies.Because the term “high MIR”is relatively novel, we do acknowledge that there may be other intrinsic factors(e.g.,medication use)that could possibly contribute to being a high-MIR runner.This should be explored further in future research studies.In the future,when a larger sample size for specific injuries is available, we will report detailed results with respect to anatomical area injured and specific runningrelated injuries.We also aim to further investigate the contributing role of specific chronic diseases to a high MIR.
Authors’contributions
SS contributed to study concept,study planning,data cleaning,data analysis including statistical analysis,data interpretation, manuscript (the first draft), and manuscript editing; NS contributed to data interpretation, manuscript (the first draft),and manuscript editing; MS contributed to responsible for the overall content as guarantor, study concept, study planning,data cleaning, data interpretation, manuscript editing, and facilitating funding; EJ contributed to study planning, data analysis including statistical analysis,data interpretation,manuscript (the first draft), and manuscript editing.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2021.11.002.
 Journal of Sport and Health Science2022年3期
Journal of Sport and Health Science2022年3期
- Journal of Sport and Health Science的其它文章
- The secrets to running economy
- Metabolic and performance responses of male runners wearing 3 types of footwear:Nike Vaporfly 4%,Saucony Endorphin racing flats,and their own shoes
- Longitudinal bending stiffness does not affect running economy in Nike Vaporfly Shoes
- Can changes in midsole bending stiffness of shoes affect the onset of joint work redistribution during a prolonged run?
- Metabolic cost of level,uphill,and downhill running in highly cushioned shoes with carbon-fiber plates
- Systematic reduction of leg muscle activity throughout a standard assessment of running footwear