
温针灸阴经穴为主治疗中风后关节痉挛的临床分析
2022-05-30 05:39:41段晓雯
婚育与健康 2022年15期
关键词:临床分析
段晓雯
【摘要】目的:深入研討与探究温针灸阴经穴为主治疗中风后关节痉挛的实际临床疗效。方法:在2021年1月—2021年10月这一阶段,我院对90例中风后关节痉挛患者开始研究和观察。实施常规针刺医治手段的45例中风后关节痉挛患者为对照组,实施温针灸阴经穴为主医治手段的45例中风后关节痉挛患者为实验组,展开此次调查。通过对比观察两组中风后关节痉挛患者治疗后关节痉挛度(踝关节、肘关节、膝关节、腕关节)、CSI指数、Fugl-Meyer积分、Barthel指数积分、实际临床疗效、ADL和FMA评分以及不良反应(轻度恶心、局部发红、手臂麻木、轻度眩晕)发生率。结果:实施常规针刺医治手段的对照组中风后关节痉挛患者治疗后关节痉挛度:踝关节(20.14±0.16)°、肘关节(25.04±0.52)°、膝关节(34.19±0.18)°、腕关节(20.96±0.16)°,CSI指数(36.04±0.52)、Fugl-Meyer(42.96±0.16)分、Barthel指数(6.19±0.18)分,实际临床疗效达88.2℅、不良反应发生率达24.4%。实施温针灸阴经穴为主医治手段的实验组中风后关节痉挛患者治疗后关节痉挛度:踝关节(9.05±0.40)°、肘关节(13.94±0.41)°、膝关节(19.45±0.26)°、腕关节(1.26±0.02)°,CSI指数(26.94±0.41)、Fugl-Meyer(34.26±0.02)分、Barthel指数(8.45±0.26)分,实际临床疗效达95.5℅、不良反应发生率达11.1%。两组数据具有明显差异(P<0.05)。同时,实施温针灸阴经穴为主医治手段的实验组中风后关节痉挛患者ADL和FMA评分比实施常规针刺医治手段的对照组高很多。结论:实施温针灸阴经穴为主医治手段对提高中风后关节痉挛患者Barthel指数积分、实际临床疗效以及ADL和FMA评分,减少治疗后关节痉挛度、CSI指数、Fugl-Meyer积分以及降低不良反应发生率的积极作用明显。
【关键词】温针灸阴经穴;中风后关节痉挛;临床分析
Clinical analysis on treating post-stroke joint spasm mainly by warming acupuncture at Yin meridian point
DUAN Xiaowen
DepartmentofAcupuncture,Yili Hospital of Traditional Chinese Medicine,Xinjiang, Yili, Xinjiang 835000, China
【Abstract】Objective : To investigate and explore the actual clinical efficacy of warm acupuncture at Yin meridian points in the treatment of post-stroke joint spasm. Methods : From January 2021 to October 2021, 90 patients with joint spasm after stroke were studied and observed in our hospital.The investigation was carried out in 45 patients with post-stroke joint spasm who were treated with routine acupuncture as the control group and 45 patients with post-stroke joint spasm who were treated with warm acupuncture at Yin meridian points as the experimental group.The degree of joint spasm ( ankle joint,elbow joint,knee joint and wrist joint),CSI index,Fugl-Meyer score, Barthel index score,actual clinical efficacy, ADL and FMA score and the incidence ofadverse reactions ( mild nausea,local redness,arm numbness and mild vertigo) were observed and compared between the two groups.Results : The degree of joint spasm after treatment in the control group treatedwith routine acupuncture treatment was ( 20.14 ± 0.16 ) ° for ankle joint, ( 25.04 ± 0.52 ) ° for elbow joint, ( 34.19 ± 0.18 ) ° for knee joint,( 20.96 ± 0.16 ) ° for wrist joint, ( 36.04 ± 0.52 ) forCSI index, ( 42.96 ± 0.16 ) point for Fugl-Meyer and ( 6.19 ± 0.18 ) point for Barthel index,the actual clinical efficacy was 88.2 % and the incidence of adverse reactions was 24.4 %. The degree of joint spasm after treatment in the experimental group of patients with post-stroke joint spasm treated with warm acupuncture at Yin meridian points: ankle joint ( 9.05 ±0.40 ) degrees, elbow joint ( 13.94 ± 0.41 ) degrees, knee joint ( 19.45 ± 0.26 ) degrees, wrist joint ( 1.26 ± 0.02 ) degrees, CSI index ( 26.94± 0.41 ), Fugl-Meyer ( 34.26 ± 0.02 ) points, Barthel index ( 8.45 ± 0.26 ) points,the actual clinical efficacy was 95.5 % and the incidence of adverse reactions was 11.1 %. The data of the two groups were significantly different(P<0.05). At the same time, the ADL and FMA scores of patients with post-stroke joint spasm in the experimental group with warm acupuncture at Yin meridian points as the main treatment methods were much higher than those in the control group with routine acupuncture treatment methods.Conclusion : Warm acupuncture at Yin meridian points has a positive effect on improving Barthel index score,actual clinical efficacy,ADL and FMA score of patients with joint spasm after stroke,reducing the degree of joint spasmafter treatment,CSI index,Fugl-Meyer score,and reducing the incidence of adverse reactions.
【Key Words】Warm acupuncture at Yin meridian points; Joint spasm after stroke; Clinical analysis
中风是传统医学中急性脑血管病的名称。在现代医学中,中风也可以称为脑卒中。根据定义,中风是指因脑血管出血或梗死导致的脑功能急性损害,并导致相应的症状。目前,对于中风后关节痉挛患者采用温针灸阴经穴手段比较常见。为进一步观察与探讨温针灸阴经穴为主治疗中风后关节痉挛的实际疗效,我院对90例中风后关节痉挛患者进行详细观察与记录,现报告如下。
1 资料与方法
1.1 一般资料
2021年1月—2021年10月阶段,我院抽取90例中风后关节痉挛患者开始研究和观察。将90例中风后关节痉挛患者均分成对照组与实验组各45例。对照组实施常规针刺医治手段,男26例,女19例,年龄52~82岁,平均年龄(64.1±0.7)岁,病程19d~4个月,平均病程(2.6±0.1)个月;实验组实施温针灸阴经穴为主医治手段,男21例,女24例,年龄57~80岁,平均年龄(65.3±0.9)岁,病程20d~5个月,平均病程(2.7±0.2)个月。两组中风后关节痉挛患者实际数据和信息无统计学意义(P>0.05)[1]。
1.2 方法
中风后关节痉挛患者的医治方案:两组中风后关节痉挛患者均接受基础治疗,包括稳定控制血糖、血压和血脂水平,并结合脑保护剂进行医治。缺血性中风后关节痉挛患者可以服用阿司匹林。如有必要,采取对症治疗和营养支持。
对照组:实施常规针刺医治手段。操作如下:取穴:少海、阴陵泉、尺泽、大陵、阳谷、内关、阳溪、血海、三阴交、委中、太溪等穴位,直刺中风后关节痉挛患者0.5~1寸,得气后,通过补平泻法,每10min针刺1次,每次1min,静置0.5h,观察效果。
实验组:实施温针灸阴经穴为主医治手段。操作如下:中风后关节痉挛患者入院治疗后,取穴:少海、阴陵泉、尺泽、大陵、阳谷、内关、阳溪、血海、三阴交、委中、太溪等穴位,直刺中风后关节痉挛患者0.5~1寸,得气后,点燃约2cm长的清艾条,轻轻放于针柄上,每次留针0.5h,观察效果。
1.3 观察指标
通过对比和观察两组中风后关节痉挛患者治疗后关节痉挛度(踝关节、肘关节、膝关节、腕关节)、CSI指数、Fugl-Meyer积分、Barthel指数积分、实际临床疗效以及不良反应(轻度恶心、局部发红、手臂麻木、轻度眩晕)发生率。
1.4 统计学方法
采用SPSS 19.0统计学软件进行数据分析。计数资料采用(%)表示,进行χ2检验,计量资料采用(χ±s)表示,进行t检验,P<0.05为差异具有统计学意义。
2 结果
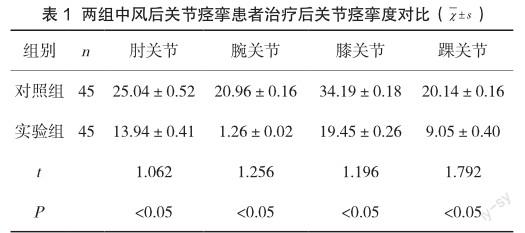
2.1 两组中风后关节痉挛患者治疗后关节痉挛度比较
实施温针灸阴经穴为主医治手段的实验组中风后关节痉挛患者治疗后的关节痉挛度比实施常规针刺医治手段的对照组低很多(P<0.05),两组数据有明显差异,具体数据见表1。
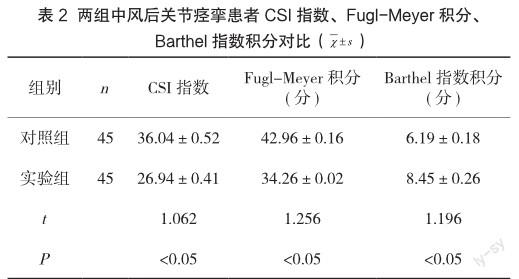
2.2 两组中风后关节痉挛患者CSI指数、FuglMeyer积分、Barthel指数积分比较
实施温针灸阴经穴为主医治手段的实验组中风后关节痉挛患者的Barthel指数积分高于实施常规针刺医治手段的对照组,而CSI指数、Fugl-Meyer积分远远低于对照组(P<0.05),两组数据有明显差异,具体数据见表2。
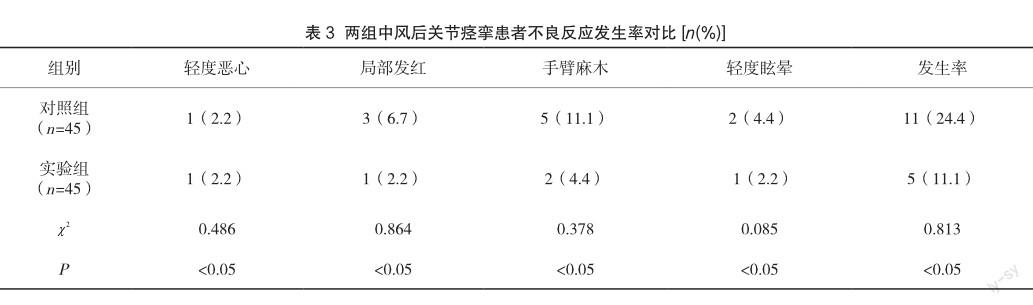
2.3 两组中风后关节痉挛患者不良反应发生率比较
实验组中风后关节痉挛患者不良反应发生率要比对照组更低(P<0.05),两组数据有明显差异,具体数据见表3。
2.4 两组中风后关节痉挛患者实际临床疗效比较
实验组中风后关节痉挛患者实际临床疗效要比对照组高(P<0.05),两组数据有明显差异。
3 讨论
通过实验结果可以看出,实施常规针刺医治手段的对照组中风后关节痉挛患者治疗后关节痉挛度:踝关节(20.14±0.16)°、肘关节(25.04±0.52)°、膝关节(34.19±0.18)°、腕关节(20.96±0.16)°;实施温针灸阴经穴为主医治手段的实验组中风后关节痉挛患者治疗后关节痉挛度:踝关节(9.05±0.40)°、肘关节(13.94±0.41)°、膝关节(19.45±0.26)°、腕关节(1.26±0.02)°[2]。两组数据具有明显差异,P<0.05。同时,实施温针灸阴经穴为主医治手段的实验组中风后关节痉挛患者ADL和FMA评分比实施常规针刺医治手段的对照组高很多。因此,实施温针灸阴经穴为主医治手段,对提高中风后关节痉挛患者的Barthel指数积分、实际临床疗效以及ADL和FMA评分,减少治疗后关节痉挛度、CSI指数、Fugl-Meyer积分、以及降低不良反应发生率具有重要作用,值得普及和应用。
参考文献
[1] 时艳珍.温针灸阴经穴为主治疗中风后关节痉挛的临床研究[J].医学信息(上旬刊),2018,7(2):145-146.
[2] 沈钦彦.温针灸联合合谷刺法治疗中风痙挛临床研究[J].中医学报,2017,32(8):1570-1572.
猜你喜欢
中国实用医药(2016年23期)2016-12-26 14:21:23
中国实用医药(2016年23期)2016-12-26 14:13:22
中国实用医药(2016年23期)2016-12-26 08:19:42
中国实用医药(2016年29期)2016-12-26 08:13:59
中国实用医药(2016年29期)2016-12-26 08:13:46
中国实用医药(2016年23期)2016-12-26 08:13:05
糖尿病新世界(2016年16期)2016-12-09 02:43:36
中外医学研究(2016年26期)2016-11-30 03:06:27
中外医学研究(2016年24期)2016-11-30 01:53:21
医学信息(2016年30期)2016-11-28 20:48:33
