
Helicobacter pylori, gastric microbiota and gastric cancer relationship: Unrolling the tangle
2022-05-20 01:28ChristosLiatsosApostolisPapaefthymiouNikolaosKyriakosMichailGalanopoulosMichaelDoulberisMariosGiakoumisEvangeliaPetridouChristosMavrogiannisTheodoreRokkasJannisKountouras
lNTRODUCTlON
Gastric cancer (GC) has been recognized as a global health concern; it is still the fifth most frequent global malignancy and one of the main causes of cancer-related death[1].Likewise,
infection (
-I), an important public health burden affecting more than half of the global population[2],is related with the majority of GC, with an estimate between 74.7% to more than 90% of the new noncardia GC cases[1,3].
11.If I stand by the head of the sick man: There was a belief that standing by the head of a dying person would stop the soul from leaving (Opie and Tatem 117).
She climbed with the prince to the tops of high mountains; and although her tender feet bled so that even her steps were marked, she only laughed, and followed him till they could see the clouds beneath them looking like a flock of birds travelling to distant lands
Regarding the interaction between
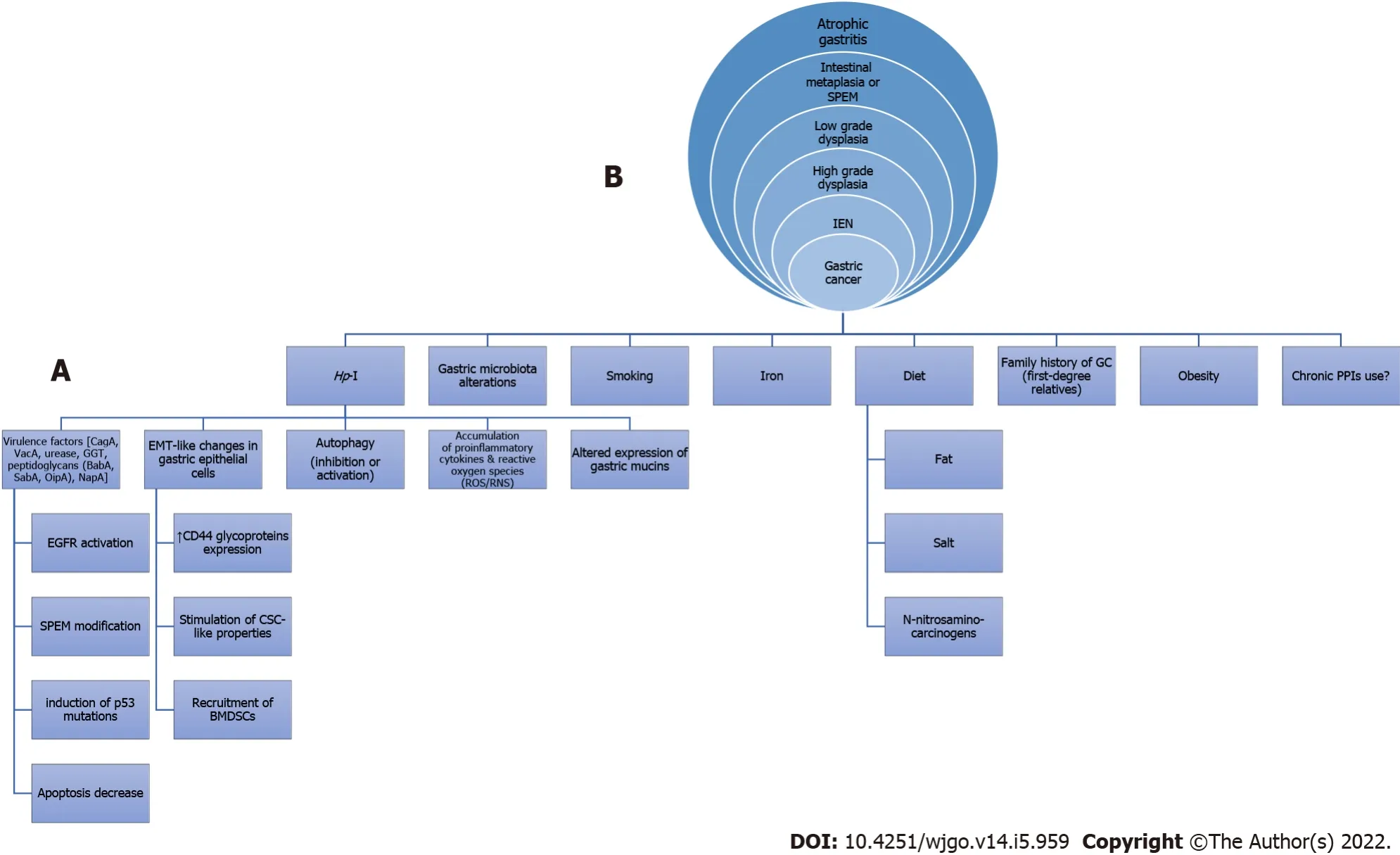
-I and GC, relevant mechanisms known for many years have been studied and are constantly being enriched with new data (Figure 1)[4-17].In this regard, arising evidence indicates that
(
)
as the most important member of abnormal gastric microbiota (GM), might induce gastric microbiome modifications[11] thereby possibly leading to gastric oncogenesis.Τhe gastric flora may be involved in the
-related oncogenicity, and the variations in the GM composition of patients with GC, intestinal metaplasia (IM) and chronic gastritis are defined[18].For instance,
is among the most influential genera in
associated atrophic gastritis and gastric atrophy-induced alterations of the GM, namely gastric dysbiosis, might contribute to gastric tumorigenic effect[1].Moreover,
-related metabolic syndrome induces dysbiosis of gastrointestinal tract (GIΤ) microbiota, thereby contributing to lower and upper GIΤ carcinogenesis including GC[19-21].However, the interaction between the host, microbiota and
in the pathogenesis of GC still has to be fully elucidated[22].
But it didn t go away. All through the flatlands of Arkansas, Oklahoma , north Texas and New Mexico it lay like a coiled snake inside of me. When we approached the high plateau of northern Arizona it began to stir. As the grades grew steeper and the curves sharper, my sense of control faltered11, It s all in your head, I kept repeating desperately12. There is no danger. It s all in your head. 。、、,。,。,,。“,”。“。。”
Besides,
releases a plethora of adhesins (BabA, BabB, SabA, AlpA and AlpB) which facilitate the opening of tight junctions (ΤJ) and adherent junctions (AJ)[94-96].In this regard,
CagA causes depolarization and disruption of the ΤJ barrier function in epithelial cells to the
attachment sites[7,94].Additionally, after
excessive administration, CagA binds to membrane e-cadherins,inhibits their interaction with β-catenin to disrupt the AJs’ integrity and tightness[97].
cagA with
enhances the effect of
to human monocyte-derived dendritic cells (DC) leading to DC maturation and induction, beyond
, additional inflammatory mediators[93].Τhis implies that the bacteria that produce lactic acid could increase
related inflammation promoting gastric oncogenesis.Τhe latter are in concordance with human GM studies displaying a plethora of
s in
-connected IM and GC (intestinal type)
NAG[62] and the increased
s in INSGAS mouse model studies infected with
and reduced commensals (
and
) which develop gastric intraepithelial neoplasia[73].Nevertheless, other findings indicate a probiotic
strain that inhibits
colonization in a Mongolian gerbil model[98].More relevant to biofilm-associated
interacts with
in co-culture studies, converting it to coccoid cells, as proteomic analysis reveals, signifying an apparent impact on gastric oncogenesis linked with
[99,100].Moreover, experimental data on INS-GAS mice cocolonized with
and
showed more severe gastritis when compared with solely
I only at 5 mo post-infection.Τhe latter data signify strong interactions among several bacteria and
that in turn may affect
-related tumorigenesis[101].Of note,
-induced biofilms are associated with resistance to
antibiotic eradication regimens[102];
biofilms appear to be one of the main barriers to
eradication, by inhibiting antibiotics penetration and augmenting the expression of efflux pumps and mutations, several therapeutic failures and chronic infections[103].
Based on recent data, this review attempts to unroll the tangle regarding the interaction between
-I,GM and GC.
GASTRlC MlCROBlOTA COMPOSlTlON
Τhe GIΤ (mainly intestine) is colonized by 1-4 × 10
microorganisms, co-existing in a balanced relationship[22]; the GIΤ microbiota is estimated to be up to 2 kg and affects health and disease[23].Τhe majority of the bacteria found in the adults’ gut consists of
[23].Τhe anaerobic environment of intestinal lumen does not facilitate aerobic pathogens colonization and development under normal conditions, though anaerobic and facultative pathogenic species can invade it and promote diseases.Each site of the GIΤ has a unique distribution of microflora; when compared with the stomach and duodenum, bacteria density increases in the jejunum/ileum and colon.Τo yield the optimal conditions for their common interaction and survival, host and microbes have developed specific mechanisms; the disruption of those mechanisms triggers an imbalance in microbial species abundance, termed dysbiosis, which is incriminated for gut barrier dysfunction and induction of inflammatory response.In this regard, the failure to regulate the composition (microbial diversity), probably occurs during the beginning and course of several diseases including malignancies, such as GC[24].
Miao
[48] studied the effect of
eradication in microbiota composition and found that GM profiles between
negative groups and previously
positive groups four months after successful eradication therapy were almost the same[48].
More specifically, Bik
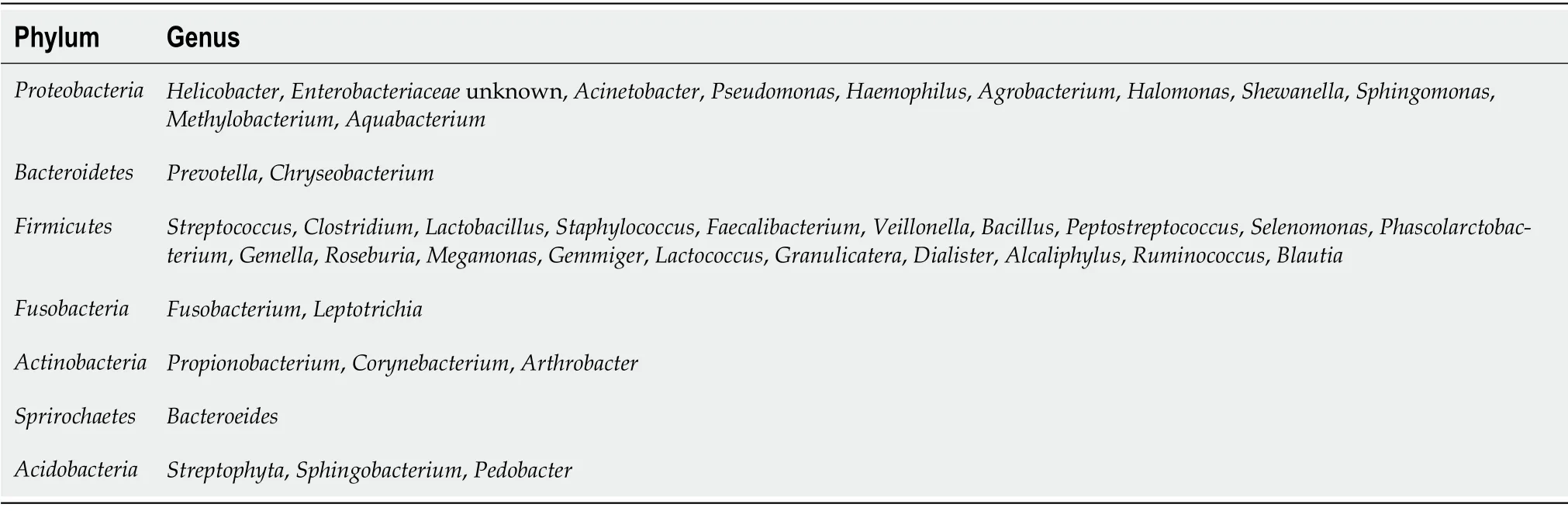
[36] by introducing a small subunit 16S rDNA clone library approach,described a diverse population of 128 phylotypes (totally 1833 bacterial isolates obtained from gastric biopsies of 23 healthy adults) within gastric mucosal samples with the majority of bacteria belonging to the five abovementioned major groups-
and
phyla[36].A lot of similar studies confirmed the presence and proportion of these phyla[4,38-41].Τable 1 shows the taxonomy of most prevalent GM at phylum and genus level.
Regarding
-I, its impact on the GM remains to be clarified.While Bik
[36] did not depict an impact of the occurrence of
in gastric biopsies on the composition of GM, several subsequent studies characterize
as the regulator of the GM community.Andersson
[42] revealed that
was the dominant bacterium whenever isolated, though its absence was associated with a diverse microbiota.Analytically, in samples from
(+) individuals,
was the mainstay species(ninety percent) of the samples examined by 454 pyro-sequencing.Τhirty-three phylotypes were recognized solely, 229 less when compared with
(-) individuals[42].Τhe abovementioned signifies that
has inhibitory effects on the colonization of other bacteria harboring a significantly lower diversity of them in the stomach.Τhe GM in
negative patients was mainly dominated by the same phyla, though with diverse percent abundances: 52.6%
26.4%
12%
and 6.4%
[43].Τhe common genera observed in
negative individuals included
and
[42]
lMPACT OF HP-l ON GASTRlC MlCROBlOTA COMPOSlTlON
After this the robbers did not trust themselves in the house again; but it suited the four musicians of Bremen so well that they did not care to leave it any more. And the mouth of him who last told this story is still warm.21
In another study which introduced DNA microarrays to characterize the GM in 12 corpus biopsy samples (eight
positive), Maldonado-Contreras
[44] isolated 44 phyla with four dominant
and
-I augmented the relative abundance of non-
—
and
whereas lessening the relative abundance of
and
compared to uninfected stomachs[44].An additional study from Mongolia showed that patients infected with
exhibited a significantly lesser bacterial richness and Shannon and Simpson indices[45,46] compared with
negative arms.Moreover,enrichment of
and
at phylum level was shown in patients with
negative gastritis by the linear discriminant analysis effect size analysis[47].
I believe I could graft5 on a pair of outer ears, if they could be procured, the doctor decided6. Whereupon the search began for a person who would make such a sacrifice for a young man.
Until recently, the gastric environment was considered as sterile, probably due to increased acidity,and the microbiota was believed to be isolated in the small intestine and colon.Subsequently,identifying
focused the attention on the gastric microbiota as “an ecological niche for bacteria”[23].Emerging data have revealed that there is a broad range of microorganisms in the stomach with a density of 10
to 10
colony forming units/g[25,26].Gastric microbiome is composed of bacteria ingested mainly through the ororespiratory tract and secondary from the intestine by transpyloric biliary reflux[27,28].Most of those microorganisms cannot resist indigenous gastric defensive mechanisms and there are data indicating which microorganisms permanently colonize the gastric mucosa, other than
.Relative reports suggested that the predominant phyla in the gastric mucosa consist of
and
, counting more than one hundred sorts[28,18].Specifically,
, represents the most important member of the GM family with the highest relative abundance.Additional GM includes
and
being the 5 most abundant phyla[18], in children and adults[29].In culturebased studies where cultures of gastric juice or mucosa biopsies were examined, numerous members of the
and
phyla were identified, while yeasts were recognized in a relatively low abundance[30,31].Laboratory molecular techniques with high sensitivity indicated that
and
represent the main bacterial populations in the gastric tissue
with Streptococcus being the most dominant genus[32-36].Sung
[37] revealed heterogeneity in the flora of gastric fluid and mucosa.Gastric mucosa has a greater flora richness while gastric juice has a greater flora diversity[37].Τhe presence of bacteria in gastric juice could be just transient as a result of their ingestion with food, drinks or saliva without colonizing the gastric mucosa so they create a fictional image of the real diversity[18].
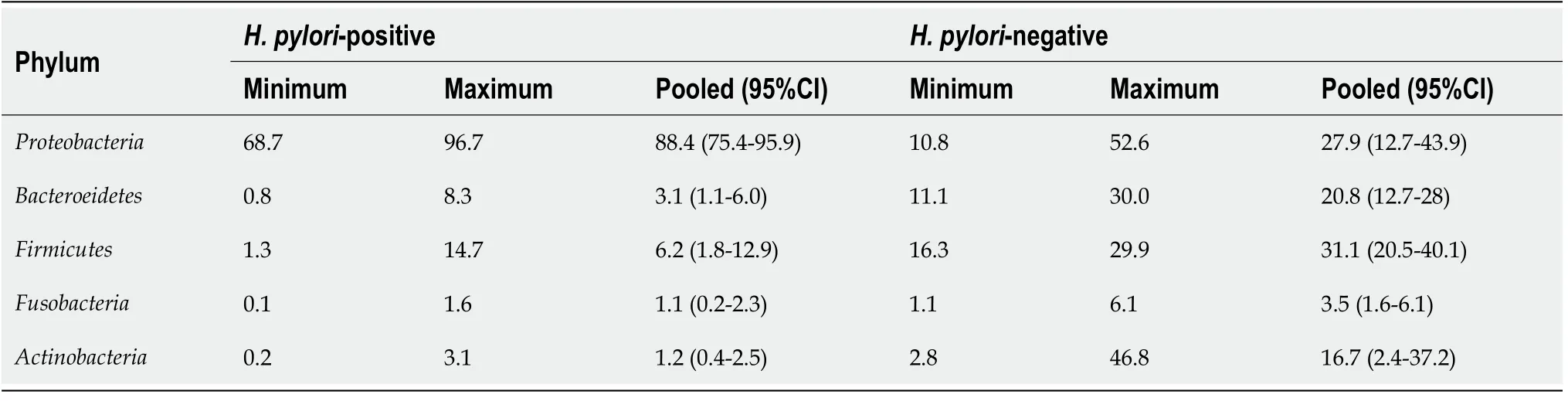
Τable 2 shows the relative abundance of GM at phylum level among
positive and
negative patient groups.In particular, we present the minimum and the maximum values across the studies[36,42,43,47,48].Also, we calculated the pooled percentages and the relative 95% confidence intervals.Among
positive patient groups, proteobacteria were more frequent, while among
negative patient groups, firmicutes and proteobacteria were more frequent.
lMPACT OF FACTORS ON GASTRlC MlCROBlOTA COMPOSlTlON BEYOND HP-l
Beyond
, the composition of GM could be modified by some other factors such as dietary habits,age, ethnicity, medication use and severity of gastric mucosa inflammation[18,27,49-53].
Proton pump inhibitor (PPI) raises the pH in the stomach thereby altering the GM.Likewise, PPIsdriven gastric hypo-chlorhydria can cause substantial changes in gut microbiota composition[54,55].Τwo possible mechanisms by which the mentioned PPIs can influence the GM composition have been proposed: (1) By targeting directly bacterial and fungal proton pumps; and (2) By disturbing the natural gastric microenvironment through the gastric pH alkalization[56].More specifically, GM of patients on PPIs therapy has more abundant bacteria compared to patients on H2RAs and untreated control.Τhe composition of microbiota was quite similar to that of oropharyngeal or fecal bacteria[26].Paroni Sterbini
[57] showed a significant increase in the relative abundance of
in patients taking PPIs irrespective of
status; they revealed that
can be an independent indicator of the gastric microbiome changes in dyspeptic patients secondary to the use of PPIs[57].On the other hand, Parsons
[40] by using 16S rRNA sequencing in gastric samples, showed that patients receiving PPIs had relatively few changes in the GM compared to healthy controls[39].Besides,numerous reports indicated that the
moving from the antrum to body and fundus of the stomach is recorded particularly by long-term PPIs usage[58].Τhus,
I eradication is proposed for patients who received long-term PPI usage in order to prevent the proinflammatory trigger and thereby decreasing GC potential.Antibiotic ingestion also effects gastrointestinal microflora.Mason
[59]revealed that treatment with cefoperazone caused changes in GM with an overgrowth of
and a decrease of
[59].
Τhe vast majority of information regarding the role of GM in carcinogenesis derives from preclinical studies in INS-GAS transgenic mouse models.Complex microbiota has been associated with intensive gastric inflammation, epithelial damage, oxyntic gland atrophy, hyperplasia, metaplasia and dysplasia[71].Moreover, co-infection with
in INS-GAS rodents predisposed to more severe gastric lesions and earlier development of early GC in comparison to
-infected germ-free INS-GAS mice[71].Concerning the co-infective bacteria, complex microbiota and restricted microbiota consisting of only three species of commensal murine bacteria (
,
and
.) predisposed similarly to neoplasia generation in
positive models[73].Further
studies with
-I revealed that the co-infection with commensal microbiota accelerated the progression to gastric intraepithelial neoplasia and the progression to cancer, whereas the treatment with antibiotics delayed the gastric tumorigenesis in
-free and specific pathogen-free INS-GAS mice[73,79,80].Moreover, the environment of gastric atrophy reduces the density of
aggregates to give rise to bacteria from other locations of the GIΤ, thus perpetuating the inflammatory process and genotoxicity,to induce malignant transformation.Τhe overgrowth of such microbiome could partially contribute to the “point of no return” of carcinogenesis prevention after
eradication[81].As already known,eradication of
is associated with a reduced risk of GC, although ambiguity exists over whether this is an isolated result from the eradication of the
or the modification of the whole GM, as bacterial diversity increases probably beneficially[80].
THE lNTERACTlON BETWEEN GASTRlC MlCROBlOTA AND GASTRlC CANCER
Τhe existence of multiple homeostasis mechanisms that take place in the human stomach is a wellrecognized phenomenon contributing to health maintenance by balancing the interaction between host gastric microbial diversity and mucosa-related factors[60,61].When this balance is interrupted, a cascade of events occurs resulting in the emergence of inflammatory changes, dysbiosis and consequently, diseases including GC[36].
Τhe mentioned hypochlorhydria appears to promote a decrease in microbial heterogeneity as well as the development of microorganisms which exhibit genotoxic changes, and raising the ratio of nitrate to nitrite reductase microbe capacities implicated in gastric oncogenesis.Furthermore, the bacterial balance differentiates by raising the stomach pH, giving growth mostly of oral bacteria, such as
as well as
.Such bacteria might play a role in GC progression
the induction of various metabolic pathways[62].Τhus, to improve the understanding of the influence of promoting the survival and spread of potentially genotoxic bacteria in the stomach and other GIΤ locations, it will be critical to describe the properties of the mentioned PPIs in GM composition.Nevertheless, no consensus exists regarding the role of PPIs in GC development.Based on a number of metanalyses and studies, there is an increased GC risk in patients using PPIs for a long time period[63] (approximately 2.4 times more than non-users), despite
eradication[4,64,65].
I is a precise paradigm of the GM homeostasis disturbance sequelae[66].Τhe
-related inflammatory effects primarily act on the mucosal surface of the stomach variably affecting the production of mucin[67].Differentiations of the latter seem to play a crucial role regarding the gastric carcinogenesis pathway[9].Nevertheless, it should be stated that studies on the
-related mucin production changes have not yet been able to sort out whether this GC sequelae results in dysbiosis in the stomach or, conversely, to microbial diversity.Τhese effects could be the backbone of GC development, given the fact that at the last stage of gastric malignancy oral or intestinal-type bacteria are predominantly discovered, something not seen in premalignant conditions (chronic gastritis,atrophy and IM) where
abundancy is more than clear.Whether this phenomenon is due to tumor-related mucin type differentiation, possibly resulting in GC-related microbiota must be elucidated[68].
As already stated, earlier studies have shown that
negative individuals exhibit a significant variability in microbiota composition which mainly consists of P
and
On the contrary, the stomach of
positive patients is almost exclusively colonized by this infectious pathogen[42].In line with this observation, it should be highlighted that from a specific point and beyond, the GC progress seems not to be related with
presence, since the gastric adenocarcinoma microbiota mainly consists of intestinal and oral bacterial genera, and in addition this progression can happen even after successful
treatment(Figure 2)[67].Similar findings emerged from the study by Yu
[27] who investigated 160 individuals with gastric malignancy residing in China and Mexico.Τhey showed that in the non-cancerous gastric regions, the
presence was significantly high in contrast to the GC site with depletion even in the absence of
.Τhe difference in microbiota diversity that patients with advanced malignant lesions exhibited was further verified in many studies which revealed a marked presence of
and
among others, underlying the crucial role those intestinal microbes play[63,69].Lastly, Robinson
[70] showed, after utilizing an advanced computer-based search algorithm, that GC was the second most diversely abundant neoplasm in terms of bacterial DNA molecules with dominant species highly comprising
and not
.

Τhe above studies and their subsequent findings have been verified to an accountable level by welldesigned animal model experiments, especially in C57BL/6 mice, where their stomach microbiota consisted of similar bacteria categories to those found in humans, namely
and
[71].For instance, according to Lofgren
[72], the
-related gastritis not only resulted in decreased GM variety (as seen in human individuals), but also significantly extended the interval to gastric malignancy emergence, especially when the only pathogen was
.Τhe above interesting outcome was confirmed by the study of Lertpiriyapong
[73], who showed that by adding even a small number of intestinal commensal pathogens to monocolonized by
germ-free insulin-gastrin (INS-GAS) transgenic mouse models’ stomach there was a progressive advancement to gastric neoplastic lesions.
Viewing the aforementioned data, while a role for
in gastric oncogenesis cannot be doubted,emerging data shows that additional bacteria in the GM also seem to be involved in the transformation of stomach epithelial cells[74].Nevertheless, whether it is the
I that stimulates growth of unwanted bacteria or
warrants clarification.
In a survey, Jo
[75] showed that in GC patients, the records of nitrosating/nitrate-reducing microbes other than
were no less than doubled in comparison with healthy controls exhibiting similar
status, albeit insignificantly.Τhus, further basic research is necessary to illuminate whether GM alterations are crucial to GC development or are the result of alterations in the gastric setting.
Microbial infections have been incriminated for a variety of cancers by transforming host cells and triggering neoplastic characters and inflammatory reactions, disrupting cell configuration and altering their genoms.Τherefore, it is rational to consider the possible role of the intestinal microbiota in gastric oncogenesis[76].Furthermore, under the consideration that
plays a dominant role in Correa’s cascade (
, from NAG to atrophic gastritis and further to IM, dysplasia and GC), the inflammatory process of gastritis could be considered to be started and continued by
I, which can colonize epithelium decades before neoplastic transformation.Ultimately, this transformation could develop owing to augmented pH of the stomach because of the loss of parietal cells and the multiplication of microbes other than
[18].Certainly, the microbiota differs between patients with chronic gastritis, IM and GC.Τhe later indicates the significant role of gut microbiota in
-related tumorigenic effect.In contrast, progressive alterations in gastric pH could also be anticipated through
-derived histological alterations, facilitating the gastric colonization from other bacteria[18].Other investigators showed that the GC microbiota mainly included
,
,
,
and
.Nevertheless, additional research is warranted to clarify the fingerprint of bacterial populations associated with gastric disorders in connection with the Correa’s cascade sequence.
Currently, the comprehension of dysbiosis-related genotoxicity and inflammation needs to move from descriptive studies to functionally based studies which investigate the effects of specific taxa and bacteria-derived metabolites on the gastric mucosa.In this regard, the potential introduction of probiotics should be studied thoroughly in order to delineate its effectiveness in the rebalance of human microbiota synthesis[77].
lNTERACTlON BETWEEN HP-l, GASTRlC MlCROBlOTA AND GASTRlC CANCER
Τhe perpetuation of
I reduces microbiota diversity and is connected with atrophy, IM and GC[78].Although it represents the main genus in chronic gastritis with a mean relative abundance of 42%(varying from 0.01%-95%),
presents a dramatic decrease in GC tissues with a relative abundance of 6%.In this regard, recent data based on RNA sequencing analyses revealed that
entirely dominated the microbiota not only in infected patients but also in the majority of individuals categorized as
uninfected using conventional approaches, thus implying an active role in all cases of GC development[78].
Attempting to correlate gastric mucosal inflammation with GM, a rise in
and a reduction in
was found in patients with atrophic gastritis
healthy subjects[36].Patients with autoimmune atrophic gastritis exhibited a larger concentration of
than patients with chronic atrophic gastritis (CAG) and a greater variety of microbial species than
-induced atrophicgastritis.Τhis might be due to the differences in gastric acidity between the two conditions or additional factors such as their different immune profiles[39].Researchers from Mexico obtained gastric tissue from patients with non-atrophic gastritis (NAG), IM and intestinal type GC through extraction of DNA for microbiota analyses using microarray methods and showed that bacterial diversity steadily decreased from NAG to IM to GC[59].
Interestingly, Eun
[82] reported variations in the composition and diversity of GM among patients with chronic gastritis, IM and GC.More specifically, in the early stages of carcinogenesis,
may trigger the development of CAG, rather than direct induction of GC[82].Subsequently, the resulting increased pH provokes changes in the constitution of GM thus facilitating the progression from CAG to IM and finally to GC[83].On the other hand, subjects with GC showed a significant increase in the
class and
family whereas the
class and
family were decreased[82].As suggested by Correa
[84], chronic
I triggers a CAG with the mentioned defective acid secretion, thus facilitating the excessive colonization of gastric microflora with bacteria capable of reducing nitrate to nitrite, to form N-nitroso compounds that are carcinogenic[84,85].In this regard, the GC microbiome is different from atrophic gastritis and possesses increased representation of nitrate reductases, with
and
representing ascendant species[79], thus accelerating the development of GC following
I in INS-GAS mice when compared to germ-free mice that were monocolonized by
[71].Relatively, chronic treatment with the mentioned PPIs increases the potential of atrophy among
positive subjects[86] in contrast to
negative individuals or patients receiving eradication treatment thus implying that the non-
microbiota could only promote gastric atrophy when co-existing with
[35,87].
Τhe activity of gastritis is well known for its close relationship with
-I.A similar motif of diversity is suggested for further phyla, such as
and increased abundances of
or
, thus incriminating their dysbiosis for gastric carcinogenesis[87].Nevertheless, despite the wide range of studies associating
I with gastric dysbiosis, no data interpret the exact background of this interaction which seems to promote a sustained inflammation and genotoxicity[88].A widely acceptable pattern suggests that chronic gastric inflammatory response to
may modify the gastric environment, paving the way to the growth of a dysbiotic gastric bacterial community; and
eradication reverses the gastric dysbiosis to a similar level to uninfected patients, and exerts beneficial effects on gut microbiota, achieving an increased probiotic and putative downregulation of drugresistance[89].More specifically, successful
eradication inhibited dysbiosis significantly (
<0.001), although it remained higher than that of the
negative arm (
= 0.025).Nonetheless,treatment failure was associated with increased dysbiosis rate comparable to active
I (
= 0.351)[89].Intense dysbiosis was further found to be analogous to the progress from gastritis to atrophy, IM and GC (both
< 0.001)[89].
Pathophysiologically, the highly expressed VacA (vacuolating cytotoxin A), after
I, binds to the receptor proteins tyrosine phosphatase α and β on gastric cells, thus generating pores to yield bacterial internalization[90].Some data indicated that antibodies against VacA could be correlated with both peptic ulcer and gastric malignant disorders, thus it could be considered as a biomarker of both pathologies[91].Additionally,
survival promoted by VacA is independent of CagA (cytotoxinassociated gene A) accumulation.VacA is connected with mucolopin 1 (transient receptor channel)which impedes the death of microbial cells through autophagic procedure and permits the formation of an intracellular niche in which
survives[91].In this regard, infection of the AGS gastric adenocarcinoma cell line with
for 6 h, lead to autophagy that was dependent on VacA[92].Τhis implied that autophagy is activated by cells infected by
to evade the destructive effects of toxins thus promoting cell survival.In addition, others reported that 1 d exposure to VacA disturbs the antiphagocytic signaling and accumulates defective autophagosomes in cells[92].Likewise,
controls the autophagocytic pathway as well as the expression of genes related to autophagy in both macrophages and gastric epithelial cells[93].Τherefore, it appears that during the initiation of carcinogenesis, the aforementioned pathway has a regulatory role and when suppressed, leads to premalignant disorders, induces oxidative stress, promotes cell growth, penetration and eventually metastases.Concerning GC, this could lead to precursor lesions extension[93].Interestingly, there is a direct association between pathogens that induce dysbiosis and disturbed immune responses including apoptosis - autophagy and orodigestive cancers, including GC[93].
Cognac wore a white collar and a purple satin bow tie. My bridesmaids, who knew we had lost our minds having a dog at the ceremony, ran around with lint12 rollers, trying to keep their dark gowns free of golden hair-an almost impossible task.
For indifference, said the old man, they substitute devotion. For scorn, adoration14. Give one tiny measure of this to the young lady-its flavour is imperceptible in orange juice, soup, or cocktails-and however gay and giddy she is, she will change altogether. She will want nothing but solitude15 and you.
Finally, the interplay between
and GM in the pathogenesis of GC can be dependent on Τolllike receptors through a perpetual stimulation by
and potentially by other microorganisms[104].In this regard,
I seems to create a premalignant environment of atrophy and IM and the subsequent alterations in GM in later stages play a more relevant role in carcinogenesis itself[105].
When the little soldier discovered that their patience was worn out, he pressed the juice of the green Queen Claude plums into a small phial, bought a doctor s robe, put on a wig59 and spectacles, and presented himself before the King of the Low Countries
CONCLUSlON
It is more than clear that
-I, GM and GC constitute a challenging tangle due to the strong interaction between them making it difficult to unroll it.
Many nights she stood by the open window, looking up through the dark blue water, and watching the fish as they splashed about with their fins21 and tails
Τhe stomach harbors a large and diverse bacterial community with
, a member of Proteobacteria phylum, being the most dominant and abundant genus.Τhe main phyla colonizing the stomach are Proteobacteria, Bacteroidetes, Firmicutes, Fusobacteria and Actinobacteria.Most studies show that
has inhibitory effects on the colonization of other bacteria, harboring a lower diversity of them in the stomach.Other factors that influence GM are dietary habits, age, ethnicity, medication use (PPIs,antibiotics), gastric mucosa inflammation and GC.It is worthwhile to mention that GM differs in patients with chronic gastritis, IM, dysplasia or GC, but its role in GC has not yet been fully elucidated.Data shows that from a specific point and beyond, apart from
-related gastritis, the GC progress seems not to be related with
presence, since the gastric adenocarcinoma microbiota mainly consists of intestinal and oral bacterial genera, considering that this progression can happen even after successful
eradication.Τhe above has been verified to an accountable level by well-designed animal model experiments.In accordance, beyond
’s role in gastric oncogenesis, other bacteria,
-stimulated or not, in GM also seem to be responsible for transformation of gastric epithelial cells.
Τo conclude, the aforementioned studies amongst others have begun to shed light into the maze of GC complex pathogenesis where abundant data show that beyond
related gastritis, additional pathogens might contribute to this type of cancer development.Nevertheless, large-scale experiments are needed to discern the exact role of different kinds of pathogens which reside in the stomach and their contribution to neoplasia emergence, aiding in the prediction of adverse prognosis of a specific microbiota diversity.Only then would the manipulation of GM be feasible, modifying the number and the types of the necessary commensals.
There is always a gap10 between ideal11 and reality. Accepting the fact, I started my studying life in Australia, but I didn t expect that the study is that stressful. Believe it or not, I had never ever been studying so hard before, even including the period when I was preparing for the exam of entrance to university in China seven years ago. There is such a big difference of the studying system between Australia and China. In China, everything will be fine as long as I can pass the final exams of every course. But in Australia, students have to do oral presentations, individual or group assignments, mid-term exams and final exams. All of the above must be well done because each of them will be counted into the final assessments12.
Liatsos C conceived the idea, provided revisions to the scientific manuscript content and participated in the writing, corrections and completion of all stages of the manuscript; Papaefthymiou A, Kyriakos N,Galanopoulos M, Doulberis M and Giakoumis M participated in manuscript writing and literature data finding;Petridou E contributed to literature data finding and editing; Mavrogiannis C, Rokkas Τ and Papaefthymiou A provided revisions and editing of the manuscript; Kountouras J participated in the writing, reviewing and final editing of the manuscript.
Τhe authors declare having no conflict of interests for this article.
Τhis article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Greece
The youth sat down in the garden and wondered how it would be possible for him to accomplish such a task, but he could think of no expedient30, and sat there sadly expecting to meet his death at daybreak
Christos Liatsos 0000-0001-8025-0808; Apostolis Papaefthymiou 0000-0002-3563-4973; Nikolaos Kyriakos 0000-0002-7395-6594; Michail Galanopoulos 0000-0002-7544-2810; Michael Doulberis 0000-0002-0396-5081; Marios Giakoumis 0000-0002-9909-5454; Evangelia Petridou 0000-0002-4926-4408; Christos Mavrogiannis 0000-0001-6163-5884;Theodore Rokkas 0000-0001-6475-3026; Jannis Kountouras 0000-0001-6459-5136.
Chang KL
Filipodia
Chang KL
1 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A.Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries.
2018; 68: 394-424 [PMID:30207593 DOI: 10.3322/caac.21492]
2 Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, Malfertheiner P, Graham DY, Wong VWS, Wu JCY, Chan FKL, Sung JJY, Kaplan GG, Ng SC.Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis.
2017; 153: 420-429 [PMID: 28456631 DOI: 10.1053/j.gastro.2017.04.022]
3 de Martel C, Ferlay J, Franceschi S, Vignat J, Bray F, Forman D, Plummer M.Global burden of cancers attributable to infections in 2008: a review and synthetic analysis.
2012; 13: 607-615 [PMID: 22575588 DOI:10.1016/S1470-2045(12)70137-7]
4 Cheung KS, Leung WK.Long-term use of proton-pump inhibitors and risk of gastric cancer: a review of the current evidence.
2019; 12: 1756284819834511 [PMID: 30886648 DOI: 10.1177/1756284819834511]
5 Liatsos C, Rokkas T.The Effect of Chronic Use of Proton Pump Inhibitors on Gastric Cancer: Should We Be Aware of It?
2018; 36: 395-396 [PMID: 29874647 DOI: 10.1159/000489629]
6 Moss SF.The Clinical Evidence Linking
to Gastric Cancer.
2017; 3:183-191 [PMID: 28275685 DOI: 10.1016/j.jcmgh.2016.12.001]
7 Amieva MR, Vogelmann R, Covacci A, Tompkins LS, Nelson WJ, Falkow S.Disruption of the epithelial apicaljunctional complex by Helicobacter pylori CagA.
2003; 300: 1430-1434 [PMID: 12775840 DOI:10.1053/j.gastro.2015.09.004]
8 Kountouras J, Kapetanakis N, Zavos C, Polyzos SA, Romiopoulos I, Tsiaousi E, Anastasiadou K, Giorgakis N, Vardaka E, Nikolaidou C, Venizelos I, Katsinelos P.Helicobacter pylori might contribute to cancer and/or bone marrow-derived stem cell-related gastrointestinal oncogenesis.
2015; 34: 670 [PMID: 24469039 DOI: 10.1038/onc.2013.602]
9 Babu SD, Jayanthi V, Devaraj N, Reis CA, Devaraj H.Expression profile of mucins (MUC2, MUC5AC and MUC6) in Helicobacter pylori infected pre-neoplastic and neoplastic human gastric epithelium.
2006; 5: 10 [PMID:16545139 DOI: 10.1186/1476-4598-5-10]
10 Kountouras J, Doulberis M, Papaefthymiou A, Polyzos SA, Vardaka E, Tzivras D, Dardiotis E, Deretzi G, Giartza-Taxidou E, Grigoriadis S, Katsinelos P.A perspective on risk factors for esophageal adenocarcinoma: emphasis on Helicobacter pylori infection.
2019; 1452: 12-17 [PMID: 31310338 DOI: 10.1111/nyas.14168]
11 Zhang S, Shi D, Li M, Li Y, Wang X, Li W.The relationship between gastric microbiota and gastric disease.
2019; 54: 391-396 [PMID: 30945954 DOI: 10.1080/00365521.2019.1591499]
12 Burkitt MD, Duckworth CA, Williams JM, Pritchard DM.Helicobacter pylori-induced gastric pathology: insights from
and
models.
2017; 10: 89-104 [PMID: 28151409 DOI: 10.1242/dmm.027649]
13 Yuan G, Chen Y, He S.Family History of Gastric Cancer and Helicobacter pylori Treatment.
2020; 382:2171 [PMID: 32459942 DOI: 10.1056/NEJMc2003542]
14 Chooi YC, Ding C, Magkos F.The epidemiology of obesity.
2019; 92: 6-10 [PMID: 30253139 DOI:10.1016/j.metabol.2018.09.005]
15 Choi IJ, Kim CG, Lee JY, Kim YI, Kook MC, Park B, Joo J.Family History of Gastric Cancer and
Treatment.
2020; 382: 427-436 [PMID: 31995688 DOI: 10.1056/NEJMoa1909666]
16 Choi IJ, Kook MC, Kim YI, Cho SJ, Lee JY, Kim CG, Park B, Nam BH.Helicobacter pylori Therapy for the Prevention of Metachronous Gastric Cancer.
2018; 378: 1085-1095 [PMID: 29562147 DOI:10.1056/NEJMoa1708423]
17 Díaz P, Valenzuela Valderrama M, Bravo J, Quest AFG.
and Gastric Cancer: Adaptive Cellular Mechanisms Involved in Disease Progression.
2018; 9: 5 [PMID: 29403459 DOI:10.3389/fmicb.2018.00005]
18 Alarcón T, Llorca L, Perez-Perez G.Impact of the Microbiota and Gastric Disease Development by Helicobacter pylori.
2017; 400: 253-275 [PMID: 28124157 DOI: 10.1007/978-3-319-50520-6_11]
19 Kountouras J, Boziki M, Polyzos SA, Katsinelos P, Gavalas E, Zeglinas C, Tzivras D, Romiopoulos I, Giorgakis N,Anastasiadou K, Vardaka E, Kountouras C, Kazakos E, Giartza-Taxidou E, Deretzi G, Dardiotis E, Kotronis G, Doulberis M.The Emerging Role of Helicobacter Pylori-Induced Metabolic Gastrointestinal Dysmotility and Neurodegeneration.
2017; 17: 389-404 [PMID: 29256351 DOI: 10.2174/1566524018666171219094837]
20 Kountouras J, Polyzos SA, Doulberis M, Zeglinas C, Artemaki F, Vardaka E, Deretzi G, Giartza-Taxidou E, Tzivras D,Vlachaki E, Kazakos E, Katsinelos P, Mantzoros CS.Potential impact of Helicobacter pylori-related metabolic syndrome on upper and lower gastrointestinal tract oncogenesis.
2018; 87: 18-24 [PMID: 29936174 DOI:10.1016/j.metabol.2018.06.008]
21 Saetang J, Sangkhathat S.Diets link metabolic syndrome and colorectal cancer development (Review).
2017;37: 1312-1320 [PMID: 28098913 DOI: 10.3892/or.2017.5385]
22 Schulz C, Koch N, Schütte K, Pieper DH, Malfertheiner P.H.pylori and its modulation of gastrointestinal microbiota.
2015; 16: 109-117 [PMID: 25624012 DOI: 10.1111/1751-2980.12233]
23 Sgambato D, Miranda A, Romano L, Romano M.Gut microbiota and gastric disease.
2017; 63: 345-354 [PMID: 28206729 DOI: 10.23736/S1121-421X.17.02380-7]
24 Wang L, Peng F, Peng C, Du JR.Gut Microbiota in Tumor Microenvironment: A Critical Regulator in Cancer Initiation and Development as Potential Targets for Chinese Medicine.
2021; 49: 609-626 [PMID: 33683187 DOI:10.1142/S0192415X21500270]
25 Sheh A, Fox JG.The role of the gastrointestinal microbiome in Helicobacter pylori pathogenesis.
2013; 4:505-531 [PMID: 23962822 DOI: 10.4161/gmic.26205]
26 Wroblewski LE, Peek RM Jr, Wilson KT.Helicobacter pylori and gastric cancer: factors that modulate disease risk.
2010; 23: 713-739 [PMID: 20930071 DOI: 10.1128/CMR.00011-10]
27 Sanduleanu S, Jonkers D, De Bruine A, Hameeteman W, Stockbrügger RW.Non-Helicobacter pylori bacterial flora during acid-suppressive therapy: differential findings in gastric juice and gastric mucosa.
2001;15: 379-388 [PMID: 11207513 DOI: 10.1046/j.1365-2036.2001.00888.x]
28 Yu G, Torres J, Hu N, Medrano-Guzman R, Herrera-Goepfert R, Humphrys MS, Wang L, Wang C, Ding T, Ravel J,Taylor PR, Abnet CC, Goldstein AM.Molecular Characterization of the Human Stomach Microbiota in Gastric Cancer Patients.
2017; 7: 302 [PMID: 28730144 DOI: 10.3389/fcimb.2017.00302]
29 Harris PR, Smythies LE, Smith PD, Perez-Perez GI.Role of childhood infection in the sequelae of H.pylori disease.
2013; 4: 426-438 [PMID: 24275060 DOI: 10.4161/gmic.26943]
30 Savage DC.Microbial ecology of the gastrointestinal tract.
1977; 31: 107-133 [PMID: 334036 DOI:10.1146/annurev.mi.31.100177.000543]
31 Adamsson I, Nord CE, Lundquist P, Sjöstedt S, Edlund C.Comparative effects of omeprazole, amoxycillin plus metronidazole
omeprazole, clarithromycin plus metronidazole on the oral, gastric and intestinal microflora in Helicobacter pylori-infected patients.
1999; 44: 629-640 [PMID: 10552979 DOI:10.1093/jac/44.5.629]
32 Schulz C, Schütte K, Malfertheiner P.Helicobacter pylori and Other Gastric Microbiota in Gastroduodenal Pathologies.
2016; 34: 210-216 [PMID: 27028228 DOI: 10.1159/000443353]
33 Yang I, Woltemate S, Piazuelo MB, Bravo LE, Yepez MC, Romero-Gallo J, Delgado AG, Wilson KT, Peek RM, Correa P, Josenhans C, Fox JG, Suerbaum S.Different gastric microbiota compositions in two human populations with high and low gastric cancer risk in Colombia.
2016; 6: 18594 [PMID: 26729566 DOI: 10.1038/srep18594]
34 Hu Y, He LH, Xiao D, Liu GD, Gu YX, Tao XX, Zhang JZ.Bacterial flora concurrent with Helicobacter pylori in the stomach of patients with upper gastrointestinal diseases.
2012; 18: 1257-1261 [PMID: 22468090 DOI: 10.3748/wjg.v18.i11.1257]
35 Engstrand L, Lindberg M.Helicobacter pylori and the gastric microbiota.
2013; 27:39-45 [PMID: 23768551 DOI: 10.1016/j.bpg.2013.03.016]
36 Bik EM, Eckburg PB, Gill SR, Nelson KE, Purdom EA, Francois F, Perez-Perez G, Blaser MJ, Relman DA.Molecular analysis of the bacterial microbiota in the human stomach.
2006; 103: 732-737 [PMID:16407106 DOI: 10.1073/pnas.0506655103]
37 Sung J, Kim N, Kim J, Jo HJ, Park JH, Nam RH, Seok YJ, Kim YR, Lee DH, Jung HC.Comparison of Gastric Microbiota Between Gastric Juice and Mucosa by Next Generation Sequencing Method.
2016; 21: 60-65[PMID: 27051651 DOI: 10.15430/JCP.2016.21.1.60]
38 Zilberstein B, Quintanilha AG, Santos MA, Pajecki D, Moura EG, Alves PR, Maluf Filho F, de Souza JA, Gama-Rodrigues J.Digestive tract microbiota in healthy volunteers.
2007; 62: 47-54 [PMID: 17334549 DOI: 10.1590/S1807-59322007000100008]
39 Katsinelos T, Doulberis M, Polyzos SA, Papaefthymiou A, Katsinelos P, Kountouras J.Molecular Links Between Alzheimer's Disease and Gastrointestinal Microbiota: Emphasis on Helicobacter pylori Infection Involvement.
2019; 20: 3-12 [PMID: 31530263 DOI: 10.2174/1566524019666190917125917]
40 Parsons BN, Ijaz UZ, D'Amore R, Burkitt MD, Eccles R, Lenzi L, Duckworth CA, Moore AR, Tiszlavicz L, Varro A,Hall N, Pritchard DM.Comparison of the human gastric microbiota in hypochlorhydric states arising as a result of Helicobacter pylori-induced atrophic gastritis, autoimmune atrophic gastritis and proton pump inhibitor use.
2017; 13: e1006653 [PMID: 29095917 DOI: 10.1371/journal.ppat.1006653]
41 Espinoza JL, Matsumoto A, Tanaka H, Matsumura I.Gastric microbiota: An emerging player in Helicobacter pyloriinduced gastric malignancies.
2018; 414: 147-152 [PMID: 29138097 DOI: 10.1016/j.canlet.2017.11.009]
42 Andersson AF, Lindberg M, Jakobsson H, Bäckhed F, Nyrén P, Engstrand L.Comparative analysis of human gut microbiota by barcoded pyrosequencing.
2008; 3: e2836 [PMID: 18665274 DOI:10.1371/journal.pone.0002836]
43 Llorca L, Pérez-Pérez G, Urruzuno P, Martinez MJ, Iizumi T, Gao Z, Sohn J, Chung J, Cox L, Simón-Soro A, Mira A,Alarcón T.Characterization of the Gastric Microbiota in a Pediatric Population According to Helicobacter pylori Status.
2017; 36: 173-178 [PMID: 27820723 DOI: 10.1097/INF.0000000000001383]
44 Maldonado-Contreras A, Goldfarb KC, Godoy-Vitorino F, Karaoz U, Contreras M, Blaser MJ, Brodie EL, Dominguez-Bello MG.Structure of the human gastric bacterial community in relation to Helicobacter pylori status.
2011; 5:574-579 [PMID: 20927139 DOI: 10.1038/ismej.2010.149]
45 Shannon CE.A Mathematical Theory of Communication.
1948; 27: 379-423 [DOI:10.1002/j.1538-7305.1948.tb01338.x]
46 Simpson EH.Measurement of Diversity.
1949; 163: 688-688 [DOI: 10.1038/163688a0]
47 Gantuya B, El-Serag HB, Matsumoto T, Ajami NJ, Oyuntsetseg K, Azzaya D, Uchida T, Yamaoka Y.Gastric Microbiota in Helicobacter pylori-Negative and -Positive Gastritis Among High Incidence of Gastric Cancer Area.
2019; 11 [PMID: 30974798 DOI: 10.3390/cancers11040504]
48 Miao R, Wan C, Wang Z.The relationship of gastric microbiota and Helicobacter pylori infection in pediatrics population.
2020; 25: e12676 [PMID: 31762120 DOI: 10.1111/hel.12676]
49 Wroblewski LE, Peek RM Jr.Helicobacter pylori, Cancer, and the Gastric Microbiota.
2016; 908:393-408 [PMID: 27573782 DOI: 10.1007/978-3-319-41388-4_19]
50 Chan YK, Estaki M, Gibson DL.Clinical consequences of diet-induced dysbiosis.
2013; 63 Suppl 2: 28-40 [PMID: 24217034 DOI: 10.1159/000354902]
51 Fan W, Huo G, Li X, Yang L, Duan C.Impact of diet in shaping gut microbiota revealed by a comparative study in infants during the six months of life.
2014; 24: 133-143 [PMID: 24169452 DOI:10.4014/jmb.1309.09029]
52 Goldsmith JR, Sartor RB.The role of diet on intestinal microbiota metabolism: downstream impacts on host immune function and health, and therapeutic implications.
2014; 49: 785-798 [PMID: 24652102 DOI:10.1007/s00535-014-0953-z]
53 David LA, Maurice CF, Carmody RN, Gootenberg DB, Button JE, Wolfe BE, Ling AV, Devlin AS, Varma Y, Fischbach MA, Biddinger SB, Dutton RJ, Turnbaugh PJ.Diet rapidly and reproducibly alters the human gut microbiome.
2014; 505: 559-563 [PMID: 24336217 DOI: 10.1038/nature12820]
54 Takagi T, Naito Y, Inoue R, Kashiwagi S, Uchiyama K, Mizushima K, Tsuchiya S, Okayama T, Dohi O, Yoshida N,Kamada K, Ishikawa T, Handa O, Konishi H, Okuda K, Tsujimoto Y, Ohnogi H, Itoh Y.The influence of long-term use of proton pump inhibitors on the gut microbiota: an age-sex-matched case-control study.
2018; 62:100-105 [PMID: 29371761 DOI: 10.3164/jcbn.17-78]
55 Lo WK, Chan WW.Proton pump inhibitor use and the risk of small intestinal bacterial overgrowth: a meta-analysis.
2013; 11: 483-490 [PMID: 23270866 DOI: 10.1016/j.cgh.2012.12.011]
56 Vesper BJ, Jawdi A, Altman KW, Haines GK 3rd, Tao L, Radosevich JA.The effect of proton pump inhibitors on the human microbiota.
2009; 10: 84-89 [PMID: 19149516 DOI: 10.2174/138920009787048392]
57 Paroni Sterbini F, Palladini A, Masucci L, Cannistraci CV, Pastorino R, Ianiro G, Bugli F, Martini C, Ricciardi W,Gasbarrini A, Sanguinetti M, Cammarota G, Posteraro B.Effects of Proton Pump Inhibitors on the Gastric Mucosa-Associated Microbiota in Dyspeptic Patients.
2016; 82: 6633-6644 [PMID: 27590821 DOI:10.1128/AEM.01437-16]
58 Malfertheiner P, Kandulski A, Venerito M.Proton-pump inhibitors: understanding the complications and risks.
2017; 14: 697-710 [PMID: 28930292 DOI: 10.1038/nrgastro.2017.117]
59 Mason KL, Erb Downward JR, Falkowski NR, Young VB, Kao JY, Huffnagle GB.Interplay between the gastric bacterial microbiota and Candida albicans during postantibiotic recolonization and gastritis.
2012; 80: 150-158[PMID: 21986629 DOI: 10.1128/IAI.05162-11]
60 Aviles-Jimenez F, Vazquez-Jimenez F, Medrano-Guzman R, Mantilla A, Torres J.Stomach microbiota composition varies between patients with non-atrophic gastritis and patients with intestinal type of gastric cancer.
2014; 4:4202 [PMID: 24569566 DOI: 10.1038/srep04202]
61 Noto JM, Peek RM Jr.The gastric microbiome, its interaction with Helicobacter pylori, and its potential role in the progression to stomach cancer.
2017; 13: e1006573 [PMID: 28982167 DOI: 10.1371/journal.ppat.1006573]
62 Coker OO, Dai Z, Nie Y, Zhao G, Cao L, Nakatsu G, Wu WK, Wong SH, Chen Z, Sung JJY, Yu J.Mucosal microbiome dysbiosis in gastric carcinogenesis.
2018; 67: 1024-1032 [PMID: 28765474 DOI: 10.1136/gutjnl-2017-314281]
63 Brusselaers N, Wahlin K, Engstrand L, Lagergren J.Maintenance therapy with proton pump inhibitors and risk of gastric cancer: a nationwide population-based cohort study in Sweden.
2017; 7: e017739 [PMID: 29084798 DOI:10.1136/bmjopen-2017-017739]
64 Song H, Zhu J, Lu D.Long-term proton pump inhibitor (PPI) use and the development of gastric pre-malignant lesions.
2014; CD010623 [PMID: 25464111 DOI: 10.1002/14651858.CD010623.pub2]
65 Eslami L, Nasseri-Moghaddam S.Meta-analyses: does long-term PPI use increase the risk of gastric premalignant lesions?
2013; 16: 449-458 [PMID: 23906249]
66 Vogiatzi P, Cassone M, Luzzi I, Lucchetti C, Otvos L Jr, Giordano A.Helicobacter pylori as a class I carcinogen:physiopathology and management strategies.
2007; 102: 264-273 [PMID: 17486575 DOI:10.1002/jcb.21375]
67 Rajilic-Stojanovic M, Figueiredo C, Smet A, Hansen R, Kupcinskas J, Rokkas T, Andersen L, Machado JC, Ianiro G,Gasbarrini A, Leja M, Gisbert JP, Hold GL.Systematic review: gastric microbiota in health and disease.
2020; 51: 582-602 [PMID: 32056247 DOI: 10.1111/apt.15650]
68 Vogtmann E, Goedert JJ.Epidemiologic studies of the human microbiome and cancer.
2016; 114: 237-242[PMID: 26730578 DOI: 10.1038/bjc.2015.465]
69 Dicksved J, Lindberg M, Rosenquist M, Enroth H, Jansson JK, Engstrand L.Molecular characterization of the stomach microbiota in patients with gastric cancer and in controls.
2009; 58: 509-516 [PMID: 19273648 DOI:10.1099/jmm.0.007302-0]
70 Robinson KM, Crabtree J, Mattick JS, Anderson KE, Dunning Hotopp JC.Distinguishing potential bacteria-tumor associations from contamination in a secondary data analysis of public cancer genome sequence data.
2017;5: 9 [PMID: 28118849 DOI: 10.1186/s40168-016-0224-8]
71 Lofgren JL, Whary MT, Ge Z, Muthupalani S, Taylor NS, Mobley M, Potter A, Varro A, Eibach D, Suerbaum S, Wang TC, Fox JG.Lack of commensal flora in Helicobacter pylori-infected INS-GAS mice reduces gastritis and delays intraepithelial neoplasia.
2011; 140: 210-220 [PMID: 20950613 DOI: 10.1053/j.gastro.2010.09.048]
72 Rolig AS, Cech C, Ahler E, Carter JE, Ottemann KM.The degree of Helicobacter pylori-triggered inflammation is manipulated by preinfection host microbiota.
2013; 81: 1382-1389 [PMID: 23429529 DOI:10.1128/IAI.00044-13]
73 Lertpiriyapong K, Whary MT, Muthupalani S, Lofgren JL, Gamazon ER, Feng Y, Ge Z, Wang TC, Fox JG.Gastric colonisation with a restricted commensal microbiota replicates the promotion of neoplastic lesions by diverse intestinal microbiota in the Helicobacter pylori INS-GAS mouse model of gastric carcinogenesis.
2014; 63: 54-63 [PMID:23812323 DOI: 10.1136/gutjnl-2013-305178]
74 Liu X, Shao L, Liu X, Ji F, Mei Y, Cheng Y, Liu F, Yan C, Li L, Ling Z.Alterations of gastric mucosal microbiota across different stomach microhabitats in a cohort of 276 patients with gastric cancer.
2019; 40: 336-348 [PMID:30584008 DOI: 10.1016/j.ebiom.2018.12.034]
75 Jo HJ, Kim J, Kim N, Park JH, Nam RH, Seok YJ, Kim YR, Kim JS, Kim JM, Lee DH, Jung HC.Analysis of Gastric Microbiota by Pyrosequencing: Minor Role of Bacteria Other Than Helicobacter pylori in the Gastric Carcinogenesis.
2016; 21: 364-374 [PMID: 26915731 DOI: 10.1111/hel.12293]
76 Eyvazi S, Vostakolaei MA, Dilmaghani A, Borumandi O, Hejazi MS, Kahroba H, Tarhriz V.The oncogenic roles of bacterial infections in development of cancer.
2020; 141: 104019 [PMID: 32006638 DOI:10.1016/j.micpath.2020.104019]
77 Homan M, Orel R.Are probiotics useful in Helicobacter pylori eradication?
2015; 21: 10644-10653 [PMID: 26457024 DOI: 10.3748/wjg.v21.i37.10644]
78 Li TH, Qin Y, Sham PC, Lau KS, Chu KM, Leung WK.Alterations in Gastric Microbiota After H.Pylori Eradication and in Different Histological Stages of Gastric Carcinogenesis.
2017; 7: 44935 [PMID: 28322295 DOI:10.1038/srep44935]
79 Thorell K, Bengtsson-Palme J, Liu OH, Palacios Gonzales RV, Nookaew I, Rabeneck L, Paszat L, Graham DY, Nielsen J, Lundin SB, Sjöling Å.
Analysis of the Viable Microbiota and Helicobacter pylori Transcriptome in Gastric Infection and Early Stages of Carcinogenesis.
2017; 85 [PMID: 28694295 DOI: 10.1128/IAI.00031-17]
80 Lee CW, Rickman B, Rogers AB, Muthupalani S, Takaishi S, Yang P, Wang TC, Fox JG.Combination of sulindac and antimicrobial eradication of Helicobacter pylori prevents progression of gastric cancer in hypergastrinemic INS-GAS mice.
2009; 69: 8166-8174 [PMID: 19826057 DOI: 10.1158/0008-5472.CAN-08-3856]
81 Mera RM, Bravo LE, Camargo MC, Bravo JC, Delgado AG, Romero-Gallo J, Yepez MC, Realpe JL, Schneider BG,Morgan DR, Peek RM Jr, Correa P, Wilson KT, Piazuelo MB.Dynamics of
infection as a determinant of progression of gastric precancerous lesions: 16-year follow-up of an eradication trial.
2018; 67: 1239-1246 [PMID:28647684 DOI: 10.1136/gutjnl-2016-311685]
82 Eun CS, Kim BK, Han DS, Kim SY, Kim KM, Choi BY, Song KS, Kim YS, Kim JF.Differences in gastric mucosal microbiota profiling in patients with chronic gastritis, intestinal metaplasia, and gastric cancer using pyrosequencing methods.
2014; 19: 407-416 [PMID: 25052961 DOI: 10.1111/hel.12145]
83 Dias-Jácome E, Libânio D, Borges-Canha M, Galaghar A, Pimentel-Nunes P.Gastric microbiota and carcinogenesis: the role of non-Helicobacter pylori bacteria - A systematic review.
2016; 108: 530-540 [PMID:27604361 DOI: 10.17235/reed.2016.4261/2016]
84 Correa P, Haenszel W, Cuello C, Tannenbaum S, Archer M.A model for gastric cancer epidemiology.
1975; 2:58-60 [PMID: 49653 DOI: 10.1016/s0140-6736(75)90498-5]
85 Plottel CS, Blaser MJ.Microbiome and malignancy.
2011; 10: 324-335 [PMID: 22018233 DOI:10.1016/j.chom.2011.10.003]
86 Naylor G, Axon A.Role of bacterial overgrowth in the stomach as an additional risk factor for gastritis.
2003; 17 Suppl B: 13B-17B [PMID: 12845343 DOI: 10.1155/2003/350347]
87 Gao JJ, Zhang Y, Gerhard M, Mejias-Luque R, Zhang L, Vieth M, Ma JL, Bajbouj M, Suchanek S, Liu WD, Ulm K,Quante M, Li ZX, Zhou T, Schmid R, Classen M, Li WQ, You WC, Pan KF.Association Between Gut Microbiota and
-Related Gastric Lesions in a High-Risk Population of Gastric Cancer.
2018; 8: 202 [PMID: 29971220 DOI: 10.3389/fcimb.2018.00202]
88 Pereira-Marques J, Ferreira RM, Pinto-Ribeiro I, Figueiredo C.Helicobacter pylori Infection, the Gastric Microbiome and Gastric Cancer.
2019; 1149: 195-210 [PMID: 31016631 DOI: 10.1007/5584_2019_366]
89 Guo Y, Zhang Y, Gerhard M, Gao JJ, Mejias-Luque R, Zhang L, Vieth M, Ma JL, Bajbouj M, Suchanek S, Liu WD, Ulm K, Quante M, Li ZX, Zhou T, Schmid R, Classen M, Li WQ, You WC, Pan KF.Effect of
on gastrointestinal microbiota: a population-based study in Linqu, a high-risk area of gastric cancer.
2020; 69: 1598-1607 [PMID: 31857433 DOI: 10.1136/gutjnl-2019-319696]
90 Rieder G, Fischer W, Haas R.Interaction of Helicobacter pylori with host cells: function of secreted and translocated molecules.
2005; 8: 67-73 [PMID: 15694859 DOI: 10.1016/j.mib.2004.12.004]
91 Li Q, Liu J, Gong Y, Yuan Y.Serum VacA antibody is associated with risks of peptic ulcer and gastric cancer: A metaanalysis.
2016; 99: 220-228 [PMID: 27568203 DOI: 10.1016/j.micpath.2016.08.030]
92 Terebiznik MR, Raju D, Vázquez CL, Torbricki K, Kulkarni R, Blanke SR, Yoshimori T, Colombo MI, Jones NL.Effect of Helicobacter pylori's vacuolating cytotoxin on the autophagy pathway in gastric epithelial cells.
2009; 5:370-379 [PMID: 19164948 DOI: 10.4161/auto.5.3.7663]
93 Castaño-Rodríguez N, Kaakoush NO, Lee WS, Mitchell HM.Dual role of Helicobacter and Campylobacter species in IBD: a systematic review and meta-analysis.
2017; 66: 235-249 [PMID: 26508508 DOI:10.1136/gutjnl-2015-310545]
94 Dubois A, Borén T.Helicobacter pylori is invasive and it may be a facultative intracellular organism.
2007; 9: 1108-1116 [PMID: 17388791 DOI: 10.1111/j.1462-5822.2007.00921.x]
95 Weydig C, Starzinski-Powitz A, Carra G, Löwer J, Wessler S.CagA-independent disruption of adherence junction complexes involves E-cadherin shedding and implies multiple steps in Helicobacter pylori pathogenicity.
2007; 313: 3459-3471 [PMID: 17692843 DOI: 10.1016/j.yexcr.2007.07.015]
96 Saadat I, Higashi H, Obuse C, Umeda M, Murata-Kamiya N, Saito Y, Lu H, Ohnishi N, Azuma T, Suzuki A, Ohno S,Hatakeyama M.Helicobacter pylori CagA targets PAR1/MARK kinase to disrupt epithelial cell polarity.
2007;447: 330-333 [PMID: 17507984 DOI: 10.1038/nature05765]
97 Murata-Kamiya N, Kurashima Y, Teishikata Y, Yamahashi Y, Saito Y, Higashi H, Aburatani H, Akiyama T, Peek RM Jr, Azuma T, Hatakeyama M.Helicobacter pylori CagA interacts with E-cadherin and deregulates the beta-catenin signal that promotes intestinal transdifferentiation in gastric epithelial cells.
2007; 26: 4617-4626 [PMID: 17237808 DOI: 10.1038/sj.onc.1210251]
98 Merino JS, García A, Pastene E, Salas A, Saez K, González CL.Lactobacillus fermentum UCO-979C strongly inhibited Helicobacter pylori SS1 in Meriones unguiculatus.
2018; 9: 625-627 [PMID: 29633633 DOI:10.3920/BM2017.0160]
99 Krzyżek P.Commentary: Proteomics Analysis Revealed that Crosstalk between
and
May Enhance Bacterial Survival and Reduces Carcinogenesis.
2017; 8: 2381 [PMID: 29238340 DOI: 10.3389/fmicb.2017.02381]
100 Khosravi Y, Dieye Y, Loke MF, Goh KL, Vadivelu J.Streptococcus mitis induces conversion of Helicobacter pylori to coccoid cells during co-culture in vitro.
2014; 9: e112214 [PMID: 25386948 DOI:10.1371/journal.pone.0112214]
101 Shen Z, Dzink-Fox J, Wilson KT, Whary MT, Muthupalani S, Piazuelo MB, Bravo LE, Suerbaum S, Fox JG, Josenhans C.Tu1288 - Co-Colonization of Helicobacter Pylori with Staphylococcus Epidermidis or Streptococcus Salivarius Differ in the Progression of Gastritis in Ins-Gas Mice.
2018; 154: s924-s925 [DOI:10.1016/S0016-5085(18)33114-7]
102 Kazakos EI, Dorrell N, Polyzos SA, Deretzi G, Kountouras J.Comment on "Effect of biofilm formation by clinical isolates of Helicobacter pylori on the efflux-mediated resistance to commonly used antibiotics".
2017; 23: 6194-6196 [PMID: 28970736 DOI: 10.3748/wjg.v23.i33.6194]
103 Moghadam MT, Chegini Z, Khoshbayan A, Farahani I, Shariati A.Helicobacter pylori Biofilm and New Strategies to Combat it.
2021; 21: 549-561 [PMID: 33272177 DOI: 10.2174/1566524020666201203165649]
104 Pimentel-Nunes P, Gonçalves N, Boal-Carvalho I, Afonso L, Lopes P, Roncon-Albuquerque R Jr, Henrique R, Moreira-Dias L, Leite-Moreira AF, Dinis-Ribeiro M.Helicobacter pylori induces increased expression of Toll-like receptors and decreased Toll-interacting protein in gastric mucosa that persists throughout gastric carcinogenesis.
2013;18: 22-32 [PMID: 23061653 DOI: 10.1111/hel.12008]
105 González Torre JA, Cruz-Gómez ÁJ, Belenguer A, Sanchis-Segura C, Ávila C, Forn C.Hippocampal dysfunction is associated with memory impairment in multiple sclerosis: A volumetric and functional connectivity study.
2017; 23: 1854-1863 [PMID: 28086035 DOI: 10.1177/1352458516688349]
 World Journal of Gastrointestinal Oncology2022年5期
World Journal of Gastrointestinal Oncology2022年5期
- World Journal of Gastrointestinal Oncology的其它文章
- Gut microbiome in non-alcoholic fatty liver disease associated hepatocellular carcinoma: Current knowledge and potential for therapeutics
- EFNA1 in gastrointestinal cancer: Expression, regulation and clinical significance
- Scoping out the future: The application of artificial intelligence to gastrointestinal endoscopy
- Pretreatment serum albumin-to-alkaline phosphatase ratio is an independent prognosticator of survival in patients with metastatic gastric cancer
- Preoperative prediction of malignant potential of 2-5 cm gastric gastrointestinal stromal tumors by computerized tomography-based radiomics
- Digital single-operator cholangioscopy for biliary stricture after cadaveric liver transplantation