
Molecular mechanisms of liver carcinogenesis related to metabolic syndrome
2022-05-05 08:41ClaudiaCampaniJeanCharlesNault
Hepatoma Research 2022年1期
Claudia Campani, Jean-Charles Nault
1Team of Functional Genomics of Solid Tumors, Centre de Recherche des Cordeliers, Sorbonne Université, Inserm, Université de Paris, Paris F-75006, France.
2Equipe labellisée Ligue Nationale Contre le Cancer, Labex OncoImmunology, Paris F-75006, France.
3Department of Experimental and Clinical Medicine, University of Florence, Florence 50139, Italy.
4Service d’hépatologie, Hôpital Avicenne, Hôpitaux Universitaires Paris-Seine-Saint-Denis, Assistance-Publique Hôpitaux de Paris, Bobigny 93000, France.
5Unité de Formation et de Recherche Santé Médecine et Biologie Humaine, Université Paris 13, Communauté d’Universités et Etablissements Sorbonne Paris Cité, Bobigny 93000, France.
Abstract Global prevalence of non-alcoholic fatty liver disease (NAFLD) and of NAFLD-hepatocellular carcinoma (HCC) is estimated to grow in the next years. The burden of NAFLD and the evidence that NAFLD-HCC arises also in noncirrhotic patients, explain the urgent need of a better characterization of the molecular mechanisms involved in NAFLD progression. Obesity and diabetes cause a chronic inflammatory state which favors changes in serum cytokines and adipokines, an increase in oxidative stress, DNA damage, and the activation of multiple signaling pathways involved in cell proliferation. Moreover, a role in promoting NAFLD-HCC has been highlighted in the innate and adaptive immune system, dysbiosis, and alterations in bile acids metabolism. Several dietary, genetic, or combined mouse models have been used to study nonalcoholic steatohepatitis (NASH) development and its progression to HCC, but models that fully recapitulate the biological and prognostic features of human NASH are still lacking. In humans, four single nucleotide polymorphisms (PNPLA3, TM6SF2, GCKR, and MBOAT7) have been linked to the development of both NASH and HCC in cirrhotic and non-cirrhotic patients, whereas HSD17B13 polymorphism has a protective effect. In addition, higher rates of somatic ACVR2A mutations and a novel mutational signature have been recently discovered in NASH-HCC patients. The knowledge of the molecular pathogenesis of NAFLD-HCC will be helpful to personalized screening programs and allow for primary and secondary chemopreventive treatments for NAFLD patients who are more likely to progress to HCC.
Keywords: Hepatocellular carcinoma, mouse model, genetic predisposition, cirrhosis, non-alcoholic fatty liver disease, immune system
INTRODUCTION
Non-alcoholic fatty liver disease (NAFLD) is the liver manifestation of metabolic syndrome and encompasses a large spectrum of clinic-pathological entities including steatosis, nonalcoholic steatohepatitis(NASH), and cirrhosis and its complications[1]. Recently, the term metabolic dysfunction-associated fatty liver disease (MAFLD) has been proposed to better define the liver manifestations of metabolic disorder[2].As opposed to NAFLD, which is a diagnosis of exclusion, MAFLD is defined by positive diagnostic criteria and do not exclude chronic alcohol intake[2]. NAFLD affects 25%-35% of the worldwide adult population and up to 50% of type 2 diabetes and up to 90% of morbidly obese patients[3]. It has been estimated that the prevalence of NAFLD will increase exponentially in the next few years and this will probably lead to an increase in the incidence of hepatocellular carcinoma (HCC) in both men and women[3]. NAFLD-related HCC incidence is extremely variable[4]. In patients with NAFLD-related cirrhosis, annual incidence of HCC ranges from 0.7% to 2.6% in USA and Europe and from 0.5% to 11.3% in Asia. Lower incidence values are reported in patients without cirrhosis (0.1-1.3 per 1000 patients-year in USA and Europe and 0.04%-0.6% in Asia)[4]. Interestingly, both in the Western and Eastern countries, the prevalence of HCC without cirrhosis is higher compared to other aetiologies [e.g., alcohol liver disease (ALD), hepatitis B virus, and/or hepatitis C virus chronic infection][4]. Due to the high prevalence of NAFLD without cirrhosis and the low incidence of HCC in this population, a systematic HCC screening targeting non-cirrhotic NAFLD patients is currently not considered cost-effective[5]. A risk stratification to guide targeted screening among these patients requires the characterization of the mechanisms underlying the development of HCC.
GENETIC PREDISPOSITION TO NAFLD-RELATED HCC
Numerous genetic and epigenetic determinants of NAFLD and NAFLD-related HCC have been discovered over the years and some common single nucleotide polymorphisms (SNP) have been robustly validated as associated with the risk of HCC development in NAFLD [Figure 1].
Patatin-like phospholipase domain-containing protein 3
Patatin-like phospholipase domain-containing protein 3 (PNPLA3), also known as adiponutrin, is a protein encoded by a gene located on chromosome 22. It is expressed in the endoplasmic reticulum and at the surface of lipid droplets both in hepatic stellate cells and hepatocytes[6].PNPLA3plays a role in hydrolysis of triglycerides and retinyl esters[7]and is regulated by nutritional status, being decreased during fasting and increased with carbohydrate-refeeding through the transcription induced by sterol regulatory elementbinding protein-1c[8]. In a genome-wide association study, the rs738409 C>G SNP has been the first genetic variant found to be associated with NASH predisposition[9]. It is characterized by a loss of function due to the substitution of isoleucine in a methionine at position 148 (p.I148M) which restricts the access of triglycerides to the catalytic serine at residue 47[9]. Moreover, the mutated protein evades ubiquitination and inhibits the activity of adipose tissue triglyceride lipase (ATGL/PNPLA2)[10]. The rs738409 C>G SNP was strongly associated to the amount of hepatic fat regardless of diabetes, body mass index (BMI) values, and lipoprotein levels[9]. The rs738409 C>G (p.I148M) variant has been linked to fat accumulation[11], lower secretion of very low density lipoprotein (VLDL)[12], higher alanine aminotransferase (ALT) levels[13], and the full spectrum of NAFLD, both in children and adults[9,14-17]. PNPLA3 rs738409 C>G (p.I148M) has been also associated to HCC development regardless of the aetiology with a higher association in “fat-derived”HCC (i.e., NASH and ALD)[18,19]; its association with hepatitis C virus related HCC has been discussed in a meta-analysis[19]. Regarding NAFLD patients, Burzaet al.[20]demonstrated the association between the rs738409 C>G variant and HCC development in obese patients. Furthermore, Liuet al.[21]demonstrated that the G allele was associated with an increased risk of HCC development independently of potential confounders including age, gender, BMI, presence of type 2 diabetes, and presence of advanced fibrosis or cirrhosis. These data have also been confirmed in a Japanese retrospective study which described an odds ratio (OR) of 6.36 for homozygousPNPLA3p.I148M[22].

Figure 1. Multifactorial pathogenesis of NAFLD-related HCC. Single nucleotide polymorphism (GCKR, MBOAT7, PNPLA3, and TM6SF2)have been associated to the development of both NAFLD and HCC and the NASH-HCC mutational profiling (TERT promoter, CTNNB1,TP53, and ACVR2A) and signature (MutSig-NASH-HCC) have been recently described. Hyperinsulinemia and obesity favor chronic liver inflammation and DNA damage through ROS production, ER stress and inhibition of fatty free acid oxidation. The higher levels of IL-6 and TNF-α promote the activation of STAT-3, a transcription factor which is involved in HCC development. Hyperinsulinemia induced IGF1 expression that phosphorylates insulin receptor substrates 1 leading to the activation of mTOR and MAPK pathways and therefore to cell proliferation, inhibition of apoptosis and HCC development. A role for the immune system has also been described, involving the intratumor CD8+ PD1+ cells, platelet (PLT) and IgA plasma cells and the circulating NET. In addition, dysbiosis and gut hyperpermeability expose the liver to bacterial metabolites and MAMPs promoting HCC development. EC: Enterocyte cell; ER:endoplasmic reticulum; FFA: free fatty acid; GCKR: glucokinase regulator; HCC: hepatocellular carcinoma; HSC: hepatic stellate cell;HSD17B13: 17β-hydroxysteroid dehydrogenase 13; IgA: immunoglobulin A; IGF: insulin-like growth factor; IGFBP: insulin-like growthfactor binding protein; IGFR: insulin-like growth-factor receptor; IL: interleukin; IRS: insulin receptor substrate; MAMPS: microbeassociated molecular pattern; MAPK: mitogen-activated protein kinase; MBOAT7: membrane-bound O-acyltransferase domain containing 7; mTOR: mammalian target of rapamycin; NAFLD: non-alcoholic fatty liver disease; NET: neutrophil extracellular traps;PD-1: programmed cell death 1; PLT: platelet; PNPLA3: patatin-like phospholipase domain-containing protein 3; ROS: reactive oxygen species; STAT: signal transducer and activator of transcription; TM6SF2: transmembrane6, superfamily member 2; TNF-α: tumor necrosis factor alpha.
Transmembrane 6, superfamily member 2
Transmembrane 6, superfamily member 2 (TM6SF2) is a transmembrane Golgi protein encoded by a gene on chromosome 19p12 involved in lipid synthesis and in the enrichment of triglycerides to apolipoprotein B(ApoB) 100 in the VLDL secretion from hepatocytes[23,24]. The rs58542926 C>T variant causes the substitution of glutamate with lysine at residue 167 and leads to a 50% reduction in protein production compared with the wild type. It reduces triglyceride rich lipoproteins secretion and promotes the accumulation of lipid droplets within hepatocytes[23]. The rs58542926 C>T variant has been linked to fatty liver disease development and progression to cirrhosis, and to a lower risk of cardiovascular disease[25]. TheTM6SF2rs58542926 C>T variant has also been associated with the development of HCC both in ALD and NAFLD patients[26-28].
Membrane-bound O-acyltransferase domain containing 7
Membrane-bound O-acyltransferase domain containing 7 (MBOAT7) gene encodes for lysophosphatidylinositol acyltransferase 1, a membrane-anchored enzyme which preferentially incorporates arachidonic acid in phosphatidyl inositol (PI), a component of membrane phospholipids[29]. Dysregulation of its expression and/or function, may change the amount of free arachidonic acid that could trigger hepatic inflammation and fibrosis[30]. The rs641738 C>T variant leads to a reduction at both the mRNA and protein level, and it has been associated with the pathogenesis of alcohol-cirrhosis, fibrosis in hepatitis B virus and hepatitis C virus infection, and prognosis of patients with primary sclerosing cholangitis[31-33]. Moreover, the variant induces the increase in oleyl-PI and linoleyl-PI and a decrease in arachidonoyl-PI within hepatocytes fostering fat accumulation and the production of inflammatory mediators[34]. Teoet al.[35]have recently observed that the rs641738 C>T SNP is associated with high level of fat at computed tomography/magnetic resonance imaging scan, having NAFLD (OR = 1.17), having advanced fibrosis, and higher ALT levels in adult patients. An increased risk of evolution both to fibrosis and HCC development has also been described in an Italian cohort of 132 NAFLD-patients among whom the rs641738 C>T variant has been found to increase the risk of HCC by approximately 80%, especially in patients without advanced fibrosis[34].
17β-Hydroxysteroid dehydrogenase 13
17β-Hydroxysteroid dehydrogenase 13 (HSD17B13) gene is located in chromosome 4q22.1 and belongs to a family of 15 enzymes which catalyzes the conversion from the 17-keto to 17 hydroxysteroids. In 2019, Abul-Husnet al.[36]observed that the rs72613567 T to TA insertion variant, adjacent to the donor splice site downstream of exon 6, causes the production of a truncated and unstable protein with reduced enzymatic activity. This SNP was associated with a reduction in the risk of ALD and NAFLD. These data have been confirmed in a cohort of 356 patients with biopsy-proven metabolic disease; a protection against NAFLD,NASH, ballooning degeneration, lobular inflammation, and fibrosis has been recognized[37]. TheHSD17B13rs72613567 loss of function variant has been also identified to be protective of HCC development in patients with ALD, independent of the degree of liver fibrosis[27,38]. A role in protecting against the development of chronic liver disease has also been demonstrated for another variant ofHSD17B13, characterized by a frameshift deletion at position 192 which causes the production of a truncated protein[39].
Glucokinase regulator
The role of glucokinase regulator (GCKR) in accumulation of fat in the liver and in a higher level of VLDL and triglycerides has been revealed in a large study enrolling 455 obese children and adolescent of different ethnicity[40]. The rs1260326 variant has been associated with the production of P446L protein which is unable to inhibit glucokinase in response to fructose-6-phosphate, resulting in an uncontrolled glucose uptake in the liver[40]. The sustained activation of glycolysis leads to a reduction in glycemia and to an increase in malonyl-COA levels which favor fat accumulation acting both as a substrate for lipogenesis and as an inhibitor of carnitine-palmitoyl transferase-a, an enzyme involved in fatty acid oxidation[40]. In 366 NAFLD patients, the rs780094 C>T variant has been associated with the severity of liver fibrosis and with higher serum triglyceride values[41], whereas the role of this SNP in determining the progression of NAFLD to HCC has not yet been clarified.
Other
The rs599839 A>G polymorphism, in the cluster of cadherin EGF LAG seven-pass G-type receptor 2 -proline and serine rich coiled-coil 1 - sortilin 1 (CELSR2-PSRC1-SORT), composed of genes involved in lipid handling and cell proliferation, has been linked to a lower risk of dyslipidemia and cardiovascular diseases and to an increased risk of HCC, regardless of fibrosis[42]. Truncating mutations inAPOB, and consequently a dysfunctional ApoB 100 protein, have been related to the development of HCC in NAFLD patients, probably due to an increase in the oxidative stress and loss of the tumour suppressive activity of ApoB[43]. The same authors observed that variants inSQSTM1gene lead to the cytoplasm accumulation of p62 favouring the hepatocyte transformation through the activation of oxidative stress and mammalian target of rapamicin (mTOR) pathways[43].
MOLECULAR MECHANISMS OF HCC DEVELOPED ON METABOLIC SYNDROME
Diabetes, insulin resistance, obesity, older age, male gender, ethnicity, and limited physical activity have been associated with the development of NAFLD-HCC regardless of the presence of cirrhosis[3]. The role of obesity as an independent risk factor in HCC development has been described in various cohort from Korea, the United States, and Sweden with a relative risk from 1.5 to 3.1[44]. Similar to obesity,hyperinsulinemia and diabetes are independent risk factors for HCC development ranging from 2 to 8 times in non-cirrhotic and cirrhotic patients respectively[45]. Overall, the risk is higher if other metabolic risk factors coexist and with increased length of exposure to these risk factors[3,45,46].
Insulin resistance and HCC development
Hyperinsulinemia and obesity lead to low-grade chronic systemic inflammation and may promote HCC development through various mechanisms. Lipid accumulation into hepatocytes, in particular free fatty acid, causes the generation of lipotoxic metabolites, reactive oxygen species and ER stress, dysregulation in gene transcription and signaling pathways, and mechanisms overall termed as lipotoxicity[6,44]. Hepatokines and adipokines expression is altered with reduced levels of the anti-inflammatory adiponectin and increased values of the proinflammatory leptin[6,44,47]. Consequently, the activation of the Janus kinase pathway is observed in NASH with signal transducer and activator of transcription (STAT)-1 activation which is involved in NASH development and STAT-3 in HCC occurrence[6,44,47,48]. Levels of tumor necrosis factor(TNF)-alpha and interleukin (IL)-6 are frequently increased in NAFLD-HCC patients[6,44,47]. These cytokines promote, together with the reduction of adiponectin, the development of insulin resistance. Insulin resistance inhibits free fatty acid oxidation and, as a consequence, leads to increased hepatocytes exposure to free fatty acid, leading to oxidative DNA damage[3]. Hyperinsulinemia favors HCC development through direct effects on transformed hepatocytes. Moreover, hyperinsulinemia plays an indirect role in carcinogenesis and lead to an increase in insulin-like growth factor 1 (IGF1) which levels are often reduced in patients with chronic liver diseases due to a reduced synthesis capacity of the cirrhotic liver[49]. In particular, hyperinsulinemia increases the expression of growth hormone receptor which controls the IGF1 production and secretion and reduced the synthesis of insulin-like growth factor-binding protein type 1 and 2, which negatively regulates the pathway[50]. IGF1 phosphorylates insulin receptor substrates 1 leading to the activation of mTOR and mitogen-activated protein kinase pathways and therefore to cell proliferation,inhibition of apoptosis and HCC development[6,44]. Finally, the uncontrolled cytokines production promotes the activation and proliferation of myofibroblasts, including hepatic stellate cells, leading to the deposition of fibrillar collagens and consequently to the development of cirrhosis and HCC occurrence[6,44].
The role of the immune system
The immune system contributes to NASH-driven liver damage and HCC[51]. Emerging data have suggested that CD8+ T cells play a key role in hepatocarcinogenesis in NASH patients[52]. In particular, Pfisteret al.[52]have observed a high number of activated CD8+ T cells expressing the programmed cell death protein 1(PD1) in a NASH-HCC mouse model, but despite the abundance of these cells, the anti-PD1 antibody did not reduce the number and/or size of tumours and moreover, an increase in liver fibrosis has been observed. The authors confirmed an enrichment of CD8+ PD1+ T cells with the same non-proliferative and tissue residency phenotype in NASH-HCC patients. They also conducted a meta-analysis of phase III randomized controlled trials showing that patients with HCC who had underlying NAFLD had significantly shorter overall survival after immunotherapy compared with other HCC aetiologies suggesting that NASH could promote resistance to immunotherapy[52]. T regulator cells are increased in NASH-HCC and play an important role both in the initiation and progression of the tumour. Recent evidence from mouse models,show that neutrophils extracellular traps favour the progression of NASH to HCC promoting the differentiation of naïve CD4+ to T regulator cells by increasing the expression of oxidative phosphorylation genes[53]. Moreover, elevated serum levels of neutrophils extracellular trap marker have been described in NASH patients who underwent liver resection, suggesting that the mechanism described in the preclinical model, could also promote hepatocarcinogenesis in humans[53]. Shalapouret al.[54]suggested a role for immunoglobulin A (IgA)+ plasma cells in the development of NAFLD-HCC suppressing CD8+ T cells via programmed cell death ligand 1 (PD-L1) and IL-10 expression, both in mice and humans. Preclinical models highlighted the possible role of platelets in NASH development and progression to HCC. Higher intrahepatic platelet levels have been found in the livers of mice fed with a choline deficient high-fat diet(CD-HFD) and not in mice fed with a lower calorie high fat diet, suggesting a specific link with NASH rather than with steatosis and/or insulin resistance. Moreover, glycoprotein Ib alpha (GPIba)-/- mice do not develop HCC, suggesting a possible role for antiplatelet and anti-GPIb alpha therapy into preventing NASH and NASH-HCC[55]. To date, robust clinical data about the role of antiplatelet therapy in prevention NASHHCC development are not available even if some studies suggest a reduced HCC occurrence on cirrhosis or after a curative treatment for HCC in patients taking aspirin[56,57]. A role for myeloid cells in the progression of obesityrelated NAFLD to NASH has been also described, although the role of these cells in promoting HCC development has not been established yet[58].
The role of gut microbiota and bile metabolism
Gut microbiota and gut-liver axis influences the pathogenesis and the progression of various liver diseases,including NAFLD and HCC. A different microbial profile and alterations in intestinal permeability are usually found in NASH-cirrhosis, independent from the association with HCC, although specific differences in gut microbiota composition of NAFLD-HCC patients have been recently described[59]. Among these patients, an increase inBacteroidesand Ruminococcaceae and a decrease ofBifidobacteriumhave been reported. Additionally, increased levels of calprotectin have also been found[59]. The changes in gut microbiota composition have been linked to an increased production of secondary bile acids (BAs) (e.g.,deoxycholic acid) which may reduce natural killer T cell recruitment and directly activate mTOR signaling fostering the HCC development[60]. Moreover, Beharyet al.[61]have recently observed that the microbiota may modulate the immune peripheral response in HCC-NAFLD patients, promoting the expansion of T regulator cells, reduction of CD8+ T cells, and attenuation cytotoxic CD8+ T cells and total CD4+ T cells expansion. Pathogen-associated molecular patterns promote cytokine and chemokine production through the activation of toll-like receptors promoting oxidative stress and DNA damage, besides the activation of hepatic stellate cells which may promote hepatocyte proliferation[60].Bile acids are involved in fat digestion and vitamin metabolism, and gene expression regulation targeting both nuclear farnesoid X receptor and membrane receptors G-protein-coupled bile acid receptor (TGR5).In NASH-HCC patients, an increased expression of BAs pool and steroidogenic acute regulatory protein 1(STARD1), involved in the alternative mitochondrial pathway of BAs synthesis, has been observed,suggesting the role of BAs in HCC occurrence[62]. Moreover, in mice, STARD1 overexpression has been associated with multifocal carcinogenesis and the incubation of tumour-initiated stem-like cells or primary mouse hepatocytes with BAs seems to stimulate the expression of genes involved in stemness and inflammation[62]. The activation of farnesoid X receptor has been also linked to the increase in fibroblast growth factor (FGF) 19 blood levels[63]. FGF19 binds FGF receptor 4-b-Kloto complex expressed at hepatocyte surface inhibiting BA and reducing liver steatosis and insulin resistance[63]. These mechanisms represent the rationale of randomized clinical trial testing a humanized FGF19 analogue for NAFLD treatment (NCT03912532). Further research is needed to evaluate their role in NAFLD and NAFLD-HCC,considering that FGF19 is often overexpressed in these tumors[63].
Mutational landscape of NAFLD-related HCC
Pinyolet al.[64]have recently characterized the mutational landscape in 80 human NASH-HCCs, identifyingTERTpromoter (56%),CTNNB1(28%),TP53(18%), andACVR2A(10%) mutations as the most frequently altered genes. A higher rate ofACVR2Amutations has been observed in NASH-HCC compared to HCC related to other etiologies (10%vs.3%, respectively) regardless of the presence of cirrhosis[64]. ACVR2A modulates cell differentiation and proliferation, acting as a tumour suppressor in various malignancies,including HCC. In addition, a trend towards lower rates ofTP53mutations in NASH-HCCvs.non-NASHHCC (18%vs.32%, respectively) has also been observed[64]. They have also described a novel mutational signature (MutSig-NASH-HCC) characterised by a higher frequency of C>T and C>A transitions, almost exclusively found in NASH-HCC, predominantly in female patients[64]. Regarding molecular classes, NASHHCCs have been found to be enriched in Wnt/TGF-beta class with a lower prevalence ofCTNNB1mutations. An increase in gene sets related to mTOR and mitochondria has also been observed, suggesting the involvement of bile acid and fatty acid metabolism as well as oxidative stress and inflammation in NASH-related HCC development[51]. Paradiset al.[65]reported that cullin 7, a E3 ligase that modulates cyclin D1 expression, is overexpressed in HCC arising from advanced fibrosis related to metabolic syndrome(60%). Cullin 7 was proposed to play an antiapoptotic effect through p53[65]. Among epigenetic alterations,an increased expression of lncRNA SNHG20[66]has been described in NAFLD-related patients whereas hypometilation ofTRIM4,PRC1andTUBA1B[67]has been observed in NASH-related HCC patients.
PRECLINICAL MODELS
In vitroand mouse models have improved the understanding of molecular pathways involved in liver carcinogenesis in NAFLD patients [Table 1].
Dietary models
Fructose consumption has been associated with NAFLD occurrence in humans[68]. Mice fed with HFD and fructose (40% fat, 0.2% of cholesterol, and a final fructose concentration of 42g/L), have increased body weight, increased body fat mass, and developed insulin resistance similar to HFD mice but with more liver fibrosis, inflammation, lipoapoptosis, and oxidative stress[69,70]. Moreover, Dowmanet al.[71]have demonstrated that mice fed with a diet high in trans-fats and fructose corn syrup and who lead a sedentary lifestyle [American lifestyle-induced obesity syndrome (ALIOS)] develop features of NAFLD after 6 months and NASH after 12 months; six out of ten mice also developed hepatocellular neoplasm. These results were recently confirmed by Harriset al.[72]who state that the ALIOS diet in mice recapitulates many of the clinical features of NAFLD and, therefore, represents a robust and reproducible model for investigating the pathogenesis of NAFLD and its progression, showing an increased incidence of hepatic tumours after 52weeks. The choline-deficient, L-amino acid-defined (CDAA) model develops steatohepatitis and liver fibrosis[6]. The combination of the CDAA diet with a HFD leads to obesity, NASH, and fibrosis; HCC occurs after 30 weeks in approximately 25% of mice[73]. These results have been recently confirmed by Weiet al.[74]which have observed that feeding C57Bl/6 mice with HFD-CDAA diet led to the development of NASH,cirrhosis, and liver cancer in 80% of cases within 24 weeks.
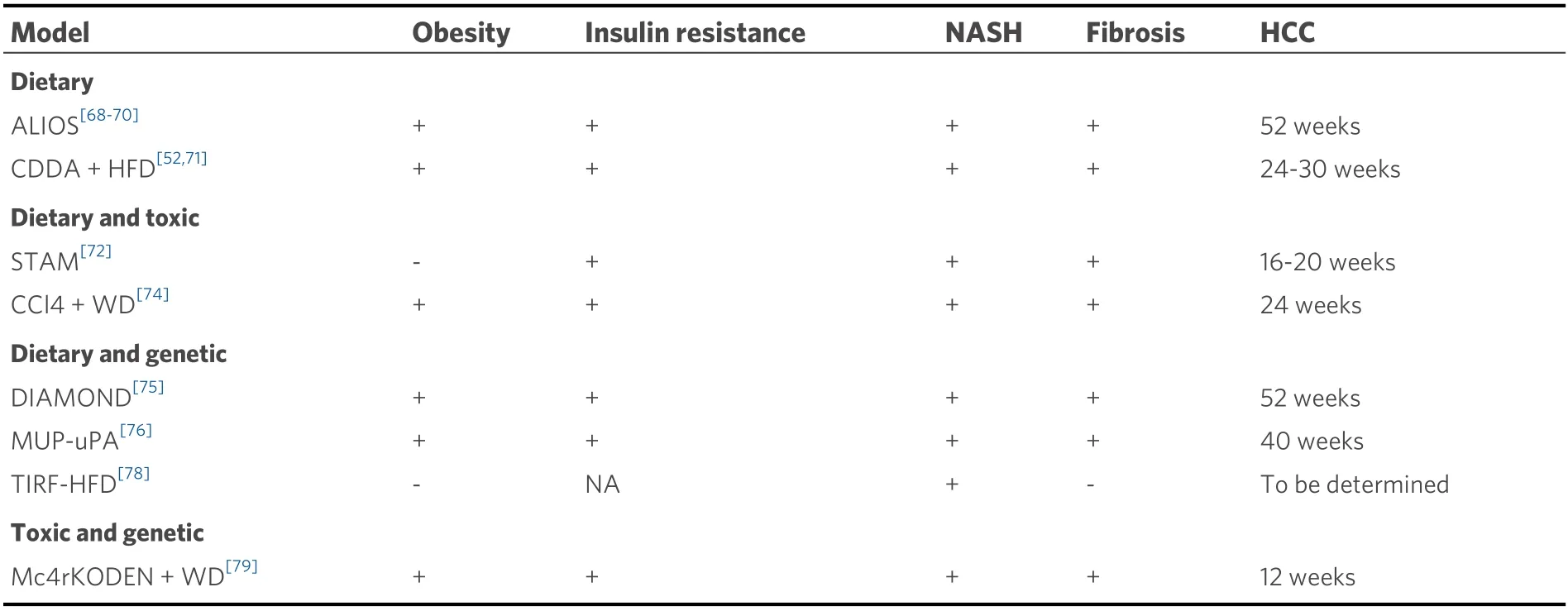
Table 1. Animal models of NAFLD-related HCC.
Dietary and toxic models
In the STAM (stelic animal model) model, a single dose of 200 micrograms of streptozotocin is given two days after birth to C57B16 mice to reduce insulin secretory capacity of damaging pancreatic beta-cells.Surviving mice are started on a HFD at 4 weeks of age and develop NASH, fibrosis, and HCC between 16 and 20 weeks of age[75]. Although histological features resemble human NASH, the mice lost weight.Moreover, a direct carcinogenic effect of streptozotocin cannot be ruled out[6]. The above data explain why this model is often considered as not adequate for the study of NASH and its progression to HCC[6,76]. A rapid progression to NASH with stage three fibrosis (12 weeks) and HCC development (24 weeks) has been observed in the mouse model developed by Tsuchidaet al.[77]who administered to C57BL/6J mice a Western diet rich in fat, fructose, and cholesterol combined with a weekly dose of intraperitoneal carbon tetrachloride. This model mimics histological, immunological, and transcriptomic features of human NASH, and it could be used to study NASH and its progression to HCC[77]. Moreover, in a recent paper,Pinyolet al.[64]confirmed the association between Western diet + carbon tetrachloride murine model and the molecular features of both cirrhotic and non-cirrhotic human-NASH-HCC.
Dietary and genetic models
In genetic animal models of NASH, diet is used as a secondary trigger to mimic disease progression. The DIAMOND (diet induced animal model of NAFLD) model is based on an inbred isogenic strain of a C57Bl6/J and S129S1/svlmJ mice where approximately 60% of genes are from the C57Bl6/J background.When mice are fed with a high fat, high carbohydrate diet with 42% Kcal from fat and containing 0.1%cholesterol withad libitumadministration of glucose/fructose in drinking water, mice develop obesity,insulin resistance, and dyslipidemia. Moreover, after 16 weeks they develop steatohepatitis followed by stage 3-4 fibrosis (36 weeks) and HCC in 90% of cases (52 weeks)[78]. The DIAMOND model shows a strong concordance with the human NAFLD transcriptome throughout the various stages of disease development[78]. One of the mechanisms which fosters the HCC development in NAFLD patients is the ER stress consequent to the intracellular lipid accumulation. Mice which expressed high amounts of urokinase plasminogen activator in hepatocytes (MUP-uPA) has ER stress and the addition of HFD promotes expression of TNF and a spontaneous progression from NASH to HCC[79]. Moreover, in MUP-uPA mice fed with HFD, a strong p62 expression has been observed, and the p62 ablation (Sqstm1 Δhep/MUP), led to the reduction of both tumour number and size confirming the role of the autophagy adaptor p62 in NASHHCC development. Similar results have been demonstrated also in STZ-HFD mice where p62 deletion suppresses HCC development without influencing fibrosis and steatosis development[80]. Recently, Bissig-Choisatet al.[81]generated a transgene-free Il2rg-/-/Rag2-/-/Fah-/- mouse populated with human hepatocytes and fed with HFD for 12 weeks. Interestingly, metabolic and histological changes of the human hepatocytes resemble those of NAFLD patients[81]. In particular, cholesterol metabolism changes are similar to NAFLD-patients[81]. Therefore, this model could be helpful in studying the malignant transformation on NAFLD[81].
Toxic and genetic models
Another more murine model has been recently proposed to assess drug efficacy in NASH-HCC. Two-weekold melanocortin-4-receptor knocked out mice receive a single intraperitoneal injection of diethylnitrosamine and are fed Western diet from 6 weeks of age up to 14 weeks. The advantage of this model is the fast development of HCC[82]with mice developing multiple liver tumours together with obesity,diabetes, and NASH in 3 months[82].
CLINICAL PERSPECTIVES AND CONCLUSION
Understanding the molecular pathogenesis of NAFLD-HCC patients could enable an early diagnosis and improve patient prognosis. It could also allow the development of HCC primary and secondary prevention strategies for patients with NASH, which to date has no approved treatment. HCC screening is recommended for cirrhotic patients, independent of the underlying aetiology[83]. As previously stated, the prevalence of NAFLD and the low incidence of HCC among patients without cirrhosis makes the surveillance in NAFLD non-cirrhotic patients not cost-effective. Moreover, sensitivity and specificity of ultrasonography may be compromised by obesity of cirrhotic NAFLD[5]. Whether non-cirrhotic NAFLD patients should undergo surveillance, which subgroup of patients should eventually be screened, and which test or combination of test should be used are questions that have still not been answered. Up to now various predictive factors have been assessed but none of these has been yet validated for clinical practice. A recent study by Youneset al.[84]evaluated non-invasive scoring systems, usually used to stratify fibrosis among patients with NAFLD [e.g., NAFLD fibrosis score-NFS, aspartate aminotransferase (AST) to platelet ratio index-APRI, Fibrosis 4-FIB-4, BMI, AST to ALT ratio, and BARD score] as predictors of long-term and extrahepatic events in a large cohort of patients. The authors identified a possible role of NFS in the prediction of HCC development (Harrell’s c index = 0.9)[84]. Moreover, the GALAD score (gender, age, lens culinaris-agglutinin-reactive fraction of AFP, AFP, and Des-g-carboxy-prothrombin) could be useful to detect HCC among NASH patients with or without cirrhosis[85]. Since no single SNP is capable of adequate HCC risk stratification due to their low odds ratio with HCC occurrence, polygenic risk scores based on the sum of risk alleles have been proposed[43,86,87]. Gellert-Kristensenet al.[87]demonstrated that a genetic risk score, based on the sum of three risk-increasing alleles (i.e.,PNPLA3,TM6SF2, andHSD17B13), predicts the risk of developing cirrhosis and HCC in NAFLD-patients. In particular, a 29-fold higher risk of developing HCC has been observed in NAFLD patients with a score of 5 and 6[87]. A different genetic risk score for hepatic fat accumulation based on well characterized variants (PNPLA3,TM6SF2,GCKR, andMBOAT7)has been proposed, and a proportional impact of genomic variants on fibrosis and hepatic fat has been demonstrated[86]. This score and its adjusted version for HSD17B13 (PRS-5) was able to predict HCC development in NAFLD and obese patients regardless of the degree of fibrosis[88]. Thresholds (≥ 0.532 for PRS-HFC and 0.495 for PRS-5) to recognise NAFLD and dysmetabolism patients with a high risk of HCC development with a good specificity have been proposed[88]. Moreover, circulating tumour DNA, circulating tumour cells, and extracellular vesicles are potential candidate biomarkers that need to be explored in NAFLD-HCC patients. Further research should be deepening their role in the surveillance among noncirrhotic NAFLD patients. Finally, more data are required in preclinical model but also in real life practice in order to confirm the link between NASH and resistance to immunotherapy for advanced HCC.
DECLARATIONS
Authors’ contributions
Conceptualization: Campani C, Nault JC
Writing - original draft preparation: Campani C
Writing - review and editing: Nault JC
Supervision: Nault JC
Availability of data and materials
Not applicable.
Financial support and sponsorship
Nault JC received research grant from Bayer and Ipsen.
Conflicts of interest
Nault JC received research grants from bayer and Ipsen. Campani C declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2022.

- Hepatoma Research的其它文章
- Robotic donor hepatectomy: a niche advancement or the way forward? A perspective from the world’s largest center
- Radiological imaging and non-surgical local treatments for cholangiocarcinoma
- Advances in Y-90 radioembolization for the treatment of hepatocellular carcinoma
- Histopathology of hepatocellular carcinoma - when and what