
A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
2022-04-28 08:40:52SiQiXiongJieLiSiLiLiPingChenYuanTingYan
Nursing Communications 2022年2期
关键词:参考文献
Introduction
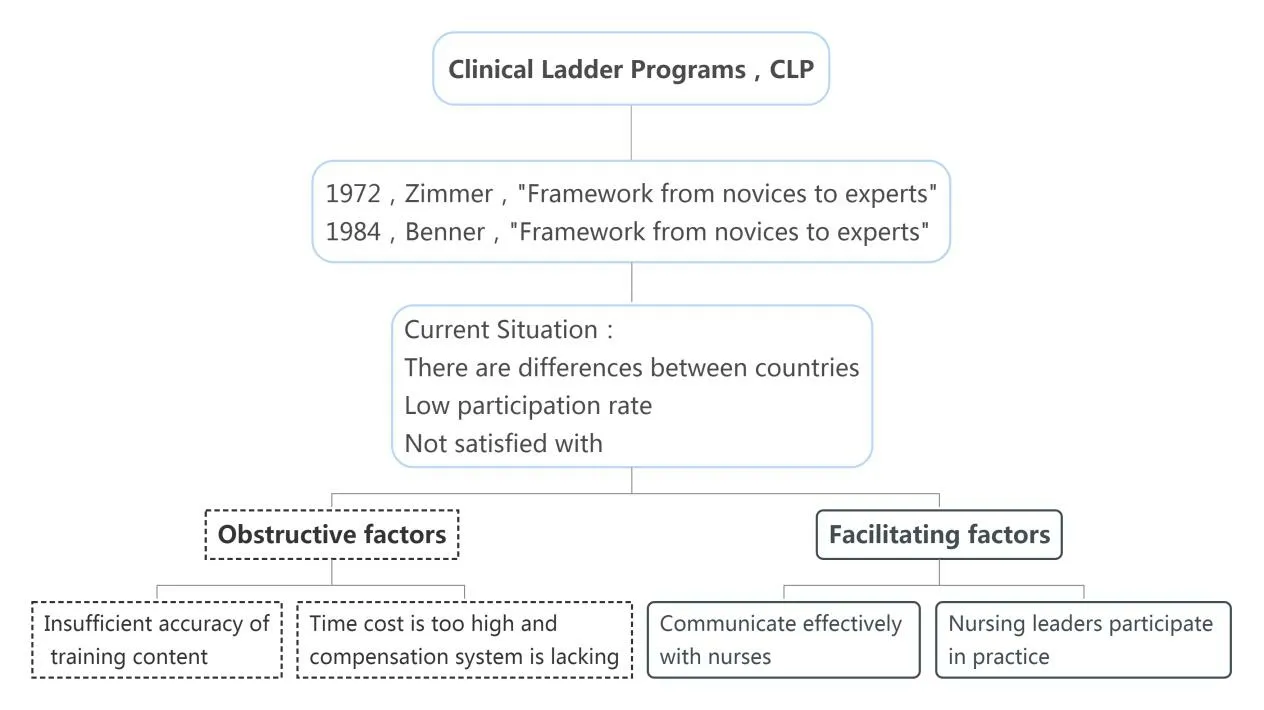
After entering the hospital, nurses still need to continue to receive on-the-job training, including clinical skills, management, scientific research, education and other contents, which is conducive to nurses to update relevant knowledge, improve their own career planning,and enhance their core competitiveness [1].As the advancement of quality nursing services, nurse training methods have shifted to competency-based layered training [2].Clinical Ladder Programs refer to the development of different training Programs according to different levels of nurses.The "Framework from novices to experts"proposed by Benner in 1984 is the basis of the Clinical Ladder Programs.A relatively complete Clinical Ladder Programs system has been established in the United States [3].This program has also been widely applied by domestic and foreign researchers in the training of nurses in pediatrics, cardiothoracic surgery, ICU, orthopedics and other departments [4-6].This program is conducive to improving the professional identity and skills of nurses.With the promotion of quality nursing services, the training method of nurses has also shifted to competency-based layered training [7].However, studies have shown that clinical nurses are not satisfied with the current Clinical Ladder Programs and the participation rate is low.Clinical nurses believe that hospitals should provide more reasonable and clear ClinicalLadderProgramsmethodstopromotenurses'self-improvement [8, 9].Therefore, this paper summarizes the current situation of the application of Clinical Ladder Programs in clinical nursing at home and abroad, to understand the obstacles and promoting factors affecting the implementation of Clinical Ladder Programs, in order to provide reference for the establishment of a perfect hierarchical nurse training model in China(Figure 1).
Overview of Clinical Ladder Programs
Clinical Ladder Programs are the basis of the position management of nursing staff, and the Clinical Ladder Programs of nursing staff is an inevitable requirement for the implementation of the position management of nurses.The establishment of the level system of nursing staff is an important measure to stabilize the nursing team and an important link to implement the long-term mechanism of high-quality nursing service [7].Energy level promotion plan is defined as a nurse promotion plan which gives different vocational knowledge and training tasks according to the position of nursing staff, and promotes them to the next level after passing the assessment,and then carries on the new stage of training and learning.Clinical Ladder Programs (CLP) refers to the promotion method of clinical nurses designed by nursing leaders.The purpose is to improve the clinical skills and abilities of nurses while reducing the turnover rate of clinical nurses.In 1972, Zimmer [10] proposed that identifying and motivating nurses through clinical ladder would help reduce the turnover rate of nurses and improve their satisfaction.Since then,clinical ladder program has been used to promote the development of nursing profession.In 1984, Benner [11] proposed the framework of"from novice to expert" and believed that the clinical progression mode should go through five stages.For example, novice, advanced beginner, competent, proficient and expert, nurses gain corresponding knowledge and confidence at different stages through formal training to improve their professional skills.This framework has been used by many institutions as the basis for designing clinical ladder plans, not only to improve the clinical skills of nurses, but also to promote the scientific research ability of nurses [12].
Stratified training status of clinical nurses
Researchers at home and abroad have constructed a hierarchical training system for nurses based on the Clinical Ladder Programs to improve the practical skills of nurses, promote the promotion of nurses and reduce their attrition rate.There are differences in stratification, training content, promotion methods and years of nurses in different countries and regions, such as: Most American take 3-5 N layered management, hospital nurses after corresponding levels of training learning could satisfy the requirement of education,working years, will be able to apply for promotion to the hierarchical management committee, at the same time submit letters of recommendation, the self-assessment report, work plan, etc., after the promotion level promotion [13].The national university of Singapore,according to the request of the ministry of health from Singapore will nurse nine grades are divided into three levels,and in accordance with the education, working years, and determine the nurse's promotion system training completion, from the lowest level (grade 2B low qualification registered nurse Ⅱ) promotion to 4B care experts,bachelor's degree in the shortest possible work eight years can be achieved, One year of work for master's and doctor's degree can lead to level 4B [14].Nurses in Australia are divided into nurse assistant,enrolled nurse, junior registered nurse, registered nurse and practical nurse according to their educational background and work experience.Nurses at each level have clear educational requirements and responsibilities.They can achieve promotion by completing corresponding training and learning at each level.In Japan, nurses are divided into clinical nursing experts, specialist nurses and life nurses according to their educational background, nursing practice ability and work experience.Nurses at different levels can be promoted through regular training and assessment, and they can be promoted to specialist nurses in about 8 years [15].
Notice on Further Strengthening the Nursing Work of Medical Institutions from the National Health Commission of the People's Republic of China clearly requires that nursing post management should be implemented and a job-based employment evaluation,training and cultivation, professional title promotion, performance appraisal and salary distribution system should be established to stimulate the vitality of the nurse team [16].Most hospitals, such as hospitals in Fujian Province and Jiangsu Province, will divide nurses into N0-N4 or N1-N5 levels according to their working years,educational background and professional title.The admission standards, training objectives and assessment standards of nurses at each level are formulated.Training manuals are prepared according to different departments and levels, and regular assessment is conducted.Promote the improvement of nurses' ability and complete the promotion among nurses' levels [5, 17].
At present, a relatively perfect management mode of nurse Clinical Ladder Programs has been established at home and abroad, but some nurses are not satisfied with the current Clinical Ladder Programs, and the participation rate is low [8].Therefore, summarizing the factors hindering the implementation of Clinical Ladder Programs and exploring its promotion factors is one of the key issues of research attention.
Obstacles to the application of Clinical Ladder Programs
The content of layered training is not accurate enough
But if Uraschimataro was astonished at the beauty of the outside, he was struck dumb at the sight of the hall within, which was lighted by the blaze of fish scales
High time cost and lack of compensation system
Here the king shouted in wonderment: Explain yourself, young man! What negro does my daughter hide beneath her throne? That, said the prince, you will see if you order to be brought here the negro who will be found beneath the throne of the princess
Nurses of different levels have different requirements for training content, so training emphases for nurses of different levels are different [18].There are, however, investigation shows that clinical nurses and nursing leaders have differences in cognitive Clinical Ladder Programs: only 28.6% of the nurses agreed Clinical Ladder Programs to improve their ability of nursing practice, and more than half (55%) of nursing leaders believe in Clinical Ladder Programs did raise the level of the practice of clinical nurses[9].As a result,nursing leaders are not careful enough to take into account the needs of nurses at different levels when developing the hierarchical training content based on the Clinical Ladder Programs.If the hierarchical training content is not refined enough, the enthusiasm of nurses with strong ability to participate in the training will be reduced, and nurses with weak ability will fall behind the progress of the training [7].Carrier proposed that the job satisfaction of nurses can be effectively improved and the career promotion of nurses can be promoted if the energy Clinical Ladder Programs can be formulated based on the actual needs of clinical nurses [19].The researchers found that although a large number of hospitals are implementing Clinical Ladder Programs, the promotion of nursing staff reduces their turnover rate.However, most of the research content is formulated on the basis of the lowest level of evidence, which cannot provide evidence to guide the best implementation practices.The content of nurses' hierarchical training cannot meet their actual needs, and it is difficult to achieve the purpose of improving the practical ability of clinical nurses, and the participation rate of the Clinical Ladder Programs is also not up to expectations [20].Moreover, Geri-Anne et al.proposed that the Clinical Ladder Programs should be a process of continuous improvement, and managers should constantly improve the Clinical Ladder Programs system based on clinical practice and in combination with evidence and research [21].
Promoting factors for the application of Clinical Ladder Programs
Communicate effectively with nurses
Communicating with caregivers about the changes to the Clinical Ladder Programs program is a key factor in the successful implementation of the Clinical Ladder Programs program.Effective information transmission and communication can improve employees'confidence, enthusiasm and dedication, and help reduce the incidence of resignation, leave and absenteeism [25].Research and experience show that clinical nurses have their own views and opinions on existing or potential problems in clinical work, but they may reserve their own views for various reasons, resulting in organizational silence[26].Organizational silence can avoid direct conflict between organizations and individuals to a certain extent, but it will have a negative impact on organizational learning and innovation behavior,so that leaders cannot get real feedback [27].Susan et al.[28] found that when the hospital implemented a hierarchical training system for nurses based on the Clinical Ladder Programs for a long time, the system was not well applied due to the lack of effective participation and follow-up investigation and maintenance.Therefore, the research team revised the hospital's Clinical Ladder Programs: Established a shared governance committee and MAPP club; Held an information collection meeting to understand nurses’ opinions on stratification;Actively communicated with clinical nurses; Announced the plan revisions on the hospital's intranet and canteens.These methods have increased the participation rate and core competence of the nurses'Clinical Ladder Programs, and at the same time promoted the progress of the Clinical Ladder Programs of specialist nurses.Knoche et al.[9]revised the original Clinical Ladder Programs and invited more than 115 clinical nurses for thematic discussion through focus group interview, which promoted the further improvement of Clinical Ladder Programs and built nursing literacy tools for clinical implementation.
A number of studies have shown that clinical nursing workers believe that excessive time investment is the main obstacle to the implementation of Clinical Ladder Programs [8, 20, 22].Zehler et al.,by using the method of focus group interview to 35 registered nurses,found that clinical nurses believe that participating in the energy-level advancement program requires a lot of training and learning, and frequent meetings, occupying clinical work time, resulting in decreased patient satisfaction [8].As patients' acuity becomes more and more complex, although the intensity of clinical nursing is also increasing, nurses are rarely able to carry out training and learning during normal working hours, which generally occupy the time of nurses' daily rest [23].However, after nurses spend a lot of time to complete the training of Clinical Ladder Programs, the hospital only provides low salary compensation [8].Although some studies suggest that the degree of compensation will change with the progress of the project, many participants believe that the compensation is not proportional to the amount of work required for the progress of the project [12, 22].Korean researchers investigated the expectation level of nursing staff in small and medium-sized hospitals on Clinical Ladder Programs, and found that nurses at different levels had inconsistent expectations on salary, suggesting that appropriate salary compensation system should be established to compensate nurses for the time and energy they spent in Clinical Ladder Programs [24].
Participation of nursing leaders in practice
The leadership behavior of nursing leaders is related to nursing culture and nurse work involvement [29].Head nurses' participation in clinical practice can promote clinical nurses' understanding of Clinical Ladder Programs, better grasp the assignment of each part of Clinical Ladder Programs, and promote the effective implementation of Clinical Ladder Programs in clinical practice[9].The study of Liu et al.[30] showed that the head nurse patiently listening to the problems and needs of clinical nurses in nurse-patient communication and occupational positioning can not only improve the level of mental resilience of nurses, but also improve the organizational climate of pediatric nurses and reduce the occurrence of hidden absenteeism.In addition, Mensik et al.[31] found through the importance of nursing leaders' active participation in practice that both nursing leaders and clinical nurses should clearly understand the advantages of the energy level advancement plan that can promote the professional development of clinical nurses.The responsibilities and work of clinical nurses should be considered when formulating the goals of the energy level advancement plan, so as to promote the promotion of nurses.
5. Who could spin straw into gold: Formerly scholars concentrated on the false boasting and name of the helper aspects of the tale. For example, the Aarne-Thompson classification focuses on the name of the helper theme of the story. However, scholars such as Ruth Bottigheimer and Jack Zipes have offered newer theories concerning the spinning aspects of the story. They compare the tale to the Grimms The Three Spinners and consider the tale to be an amalgamation of literary and oral tales that the Grimms carefully reworked to represent the dilemma of a young peasant woman who cannot spin to save herself (Zipes 1994, 55). #p##e#
Summary
The implementation of Clinical Ladder Programs in clinical practice can effectively improve the clinical practice ability of nurses, and provide motivation and direction for the promotion of clinical nurses.However, the implementation of Clinical Ladder Programs in clinical practice still faces some problems, such as insufficient precision of layered training content, high time cost and lack of compensation system.In the future, researchers should focus on these problems,strengthen the communication between nursing managers and nursing staff, continuously improve the level of intensive care, seek for the level of practical plan to promote the progress and development of nursing management.
1.Sheikhi MR, Fallahi-Khoshnab M, Mohammadi F, Oskouie F.Skills Required for Nursing Career Advancement: A Qualitative Study.Nurs Midwifery Stud.2016, 5(2): e30777.
2.Cui C, Zheng XL, Song H, Wu WC.Construction and application of information system of layered training for nurses.Chinese Journal of Nursing.2016, 51(1): 66-69.
3.Evans A, Loera K, Harris D, Carson S, Boutros L, Okuhara C.Development, Implementation, and Satisfaction With a Nurse Practitioner Professional Ladder: A Children's Hospital Experience.J Pediatr Health Care.2019, 33(1): 111-116.
4.Logue, Barbara.Mentoring Nurses to Success in a Cardiothoracic Intensive Care Unit Using a Clinical Ladder Matrix.Critical Care Nurse, 2018.
5.Wang MQ, Tang XH, Peng JH, Sheng J, Tang MD, Deng H.Application of nursing clinical ladder program based on Benner theory in nurses′ stratified training.Chinese Journal of Practical Nursing.2019, 35(2): 142-146.
6.Wang JL.Application of clinical ladder hierarchical training mode in orthopedics nurses.Chin J Mod Nurs.2018, 24(20):2470-2472.
7.Peng MQ, Li M, Xie AL, Li M, et al.Application of a nurse stratified training program based on nursing clinical ladder model.Chin J Mod Nurs.2017, 23(12): 1606-1611.
8.Zehler J, Covert C, Seiler L, Lewis M, Perazzo J, Beery TA.One rung at a time:what affects clinical ladder participation?Nurs Manage.2015.46(4): 30-37.
9.Knoche EL, Meucci JH.Competencies within a professional clinical ladder: differences in understanding between nurse managers and staff nurses.J Nurses Prof Dev.2015, 31(2): 91-99.
10.Zimmer MJ.Rationale for a ladder for clinical advancement in nursing practice.J Nurs Adm.1972, 2(6): 18-24.
11.Clark B, Martha DRN.From Novice To Expert: Excellence and Power in Clinical Nursing Practice.The American Journal of Nursing,1984, 10(1): 74.
12.Esfahani S, Ignatyeva Y, Ekno M, Salinas M, Salinas N, Chechel L, et al.Use of the clinical ladder to improve capacity for nursing research.Appl Nurs Res.2020, 55: 151285.
13.Xiang JG, Wei L.The Historical Development and Implementation Status of Nursing Clinical Ladder System in the USA and Its Enlightenment to China.Nursing Journal of Chinese People's Liberation Army.2020, 37(7): 75-78.
14.Wang ZY, Wang HW.Use and management of the nurse hierarchy system at the National University of Singapore Hospital.Chinese Nursing Research.2016, 30(9): 1147-1149.
15.Yang LM, Ye XF, Wang DF, Shen YM, Zhou S.The current application status of nursing clinical ladder program.Chin J Mod Nurs.2014, 20(33): 4161-4164.
16.Office of the National Health Commission.Circular of the General Office of the NHC on further strengthening nursing work in medical institutions.2020.
17.Liu J.Appfication and effects of clinical ladder training mode for pediatric nurses.Chin J Nurs Educ.2016, 13(3): 209-211.
18.Wen CL, Lu HY, Li XX, Li YR.Survey and analysis of training needs of nurses at different levels based on the nursing clinical ladder program.Nursing of Integrated Traditional Chinese and Western Medicine.2020, 6(6): 99-102.
19.Carryer J, Russell A, Budge C.Nurses' understandings of the Professional Development Recognition Programme.Nurs Prax N Z.2007, 23(2): 5-13.
20.Meucci J, Moore A, McGrath JM.Testing Evidence-Based Strategies for Clinical Ladder Program Refinement.J Nurs Adm.2019,49(11): 561-568.
21.Warman GA, Williams F, Herrero A, Fazeli P, White-Williams C.The Design and Redesign of a Clinical Ladder Program: Thinking Big and Overcoming Challenges.J Nurses Prof Dev.2016, 32(6): E1-E7.
22.Merritt K.Clinical Ladder Mentoring: The Impact on Nursing Professional Development.East Carolina University, 2019.
23.Moore A, Meucci J, McGrath J.Attributes of a Successful Clinical Ladder Program for Nurses: An Integrative Review.Worldviews Evid Based Nurs.2019, 16(4): 263-270.
24.Younghee H, Kyungsook K.A survey on Registered Nurses'Expectation of the Clinical ladder program in small to medium sized hospitals.Advanced Science and Technology Letters.2014, 61: 66-69.
25.Yurdakul M, Beşen MA, Erdoğan S.The organisational silence of midwives and nurses: reasons and results.J Nurs Manag.2016, 24(5):686-694.
26.Zhang WX, Zhu HB, Li J, Zhang XM, Wang S, Yu J.Research progress on organizational silence of clinical nurses.Chinese Journal of Nursing Management.2019, 19(4): 579-583.
27.Anderson J.The ethics of silence: Does conflict of interest explain employee silence? Healthc Manage Forum.2018, 31(2):66-68.
28.Winslow SA, Fickley S, Knight D, Richards K, Rosson J,Rumbley N.Staff nurses revitalize a clinical ladder program through shared governance.J Nurses Staff Dev.2011, 27(1): 13-17.
29.Zhang J, Zheng YN.Research on relationship among head nurses' authentic leadership,nursing organizational culture and nurses'work engagement.Chinese Journal of Nursing.2016, 51(9):1054-1058.
30.Liu HY, Zhu LH, Xie JH, Li Y, Xiao B, Su ZH, et al.Study on impact of Head Nurse Listening Day on pediatric nurses.Chinese Journal of Nursing.2020, 55(9): 1381-1386.
31.Mensik JS, Martin DM, Johnson KL, Clark CM, Trifanoff CM.Embedding a Professional Practice Model Across a System.J Nurs Adm.2017, 47(9): 421-425.
猜你喜欢
国际比较文学(中英文)(2020年3期)2020-11-17 21:19:36
肾脏病与透析肾移植杂志(2020年1期)2020-03-23 09:14:30
World journal of emergency medicine(2020年2期)2020-03-02 10:44:40
World Journal of Integrated Traditional and Western Medicine(2019年3期)2019-12-21 14:44:45
Defence Technology(2019年5期)2019-11-18 02:34:28
国际比较文学(中英文)(2019年1期)2019-11-12 23:08:45
国际比较文学(中英文)(2019年1期)2019-11-12 23:08:45
国际比较文学(中英文)(2018年1期)2018-11-13 05:51:57
转化医学杂志(2018年2期)2018-04-23 08:15:17
东方教育(2016年4期)2016-12-14 13:52:48