
The clinical outcomes of laser with suction device in mini-percutaneous nephrolithotomy
2022-03-25 06:40AbhishekGajendraSinghSundaramPalaniappanShrikantJaiGopalTakArvindGanpuleRavindraSabnisMaheshDesai
Asian Journal of Urology 2022年1期
Abhishek Gajendra Singh,Sundaram Palaniappan,Shrikant Jai,Gopal Tak, Arvind Ganpule, Ravindra Sabnis, Mahesh Desai
Department of Urology, Muljibhai Patel Urological Hospital, Virendradesai Marg, Nadiad, Gujarat,India
KEYWORDS Mini-percutaneous nephrolithotomy;Laser with suction;Stone clearance
Abstract Objective: To evaluate the safety,efficacy and feasibility of laser with suction device in mini-percutaneous nephrolithotomy (mini-PCNL).Methods: A retrospective study was conducted including 200 patients who underwent mini-PCNL for renal stones.All patients underwent PCNL using Electro-Medical Systems laser.In addition to the laser in 100 patients, a suction device was used (laser with suction [LWS]).In the other 100, suction device was not used (laser with no additional suction [LOS]).Mini-PCNL was performed using standard technique and Karl Storz minimally invasive PCNL-medium system was used.Primary end point was stone clearance.Results: Both the groups were comparable in terms of demographic data.Mean stone size was 15.24±5.90 mm and 16.16±5.53 mm in LWS and LOS, respectively.Mean Hounsfield unit of stone was 1285.64 and 1206.79 in LWS and LOS, respectively.Operative time was less in LWS group (56.89±19.65 min) as compared to LOS (62.01±28.81 min).At one-month follow-up,radiological complete clearance was 96%in LWS and 92%in LOS.On subgroup analysis of stones larger than 18 mm,the clearance rate was in favour of LWS(85.7%vs.100%)and also the need for nephrostomy placement was less in LWS group.Conclusions: LWS device is safe and efficacious when used with mini-PCNL.For stones greater than 18 mm, it has a better stone free rate as compared to using no suction.
1.Introduction
Percutaneous nephrolithotomy (PCNL) is now an established procedure.This has evolved over the years from a large 30 Fr tract, to mini- and ultra mini-PCNL.The morbidity associated with a large tract is well documented.The need for PCNL in pediatric patients led to the development of smaller tract PCNL.In 2001, Lahme et al.[1]showed that 20 Fr tract was effective in clearing stones with lower complication rates.The Clinical Research Office of the Endourological Society (CROES)study showed that transfusion rates were much lower in the smaller sheath size (1.1%) compared to the larger sheath sizes (5.9%) [2].This led to many urologists embracing the smaller tract PCNL to avoid such morbidity.In minimally invasive PCNL (MIP), tracts are often of sizes less than 20 Fr.The sheaths are placed after a single step dilatation.The most convenient size of nephroscope used with these tracts is 12 Fr nephroscope.These scopes have a 5 Fr channel for instruments.A meta-analysis by Zhu et al.[3] revealed that there was no difference in the stone free rates when comparing mini-PCNL and standard PCNL.It also showed no difference in the rates of postoperative fever.Pain scores were lower in the small tract PCNL cohort and consequently hospitalization was also shorter.
Lithotripsy can be achieved with laser, ultrasonic or pneumatic energy, however laser is the most commonly used lithotripsy device in mini-PCNL as it is small diameter energy source.Holmium laser has been very effective in the fragmentation of stones of varying hardness and very safe due to its low penetration depth.Removal of smaller fragments is made possible using vacuum cleaner effect where the fragments move from a high-pressure zone in the pelvicalyceal system (PCS) to a lower pressure zone in the sheath.When the fragment load is high,multiple insertions and withdrawals of the nephroscope to facilitate the retrieval of all the stone fragments may be required.Furthermore, some fragments as well as blood clots still require the use of the forceps.On rare occasion this may lead to slipping of guide wire.A new device in the stone treatment armamentarium has made the process of stone extraction less tedious by combining suction with the laser.This allows the continuous evacuation of small fragments and stone dust which may enhance the speed at which the procedure is completed.Though laser coupled with suction has been available previously, these devices had an outer diameter of more than 11 Fr [4].As such they are compatible only with larger nephroscopes, not the mininephroscopes.The current prototype device is manufactured by Electro-Medical Systems (EMS) (S.A., Nyon,Switzerland) and has a metallic tube with outer diameter of 4.5 Fr.This tube houses a metallic suction tube and laser sheath (Fig.1).The device is connected to suction with a suction pressure capacity of 200 mmHg (1 mmHg=0.133 kPa).The device is clutch controlled so that the suction of 0-200 mmHg can be achieved,and the device has a locking mechanism in case the surgeon wants to have a full power of suction (Fig.2).The clutch control enables the surgeon to deliver requisite amount of suction,and it is not an all or none phenomenon.Laser sheath allows the passage of 365 μm laser fiber.This device will fit into the working channel of a 12 Fr mini-nephroscope which is usually used together with a 16.0 Fr or 17.5 Fr sheath.
The aim of this study was to evaluate the safety, efficacy, and feasibility of laser with suction device in mini-PCNL and compare it with a laser without suction group.The primary end point of the study was stone clearance.
2.Patients and methods
This was a retrospective study of patients who underwent mini-PCNL for renal stones at our center, from February 2014 until January 2017.The study was performed in accordance with Good Clinical Practice guidelines and the principles of the Declaration of Helsinki.The study was approved by institution ethics committee.The patients with an age >18 years and <60 years,cumulative maximum stone diameter of <3.5 cm, without any history of past percutaneous renal surgery were included in the study.Patients were excluded if they underwent any prior procedure for the existing stone,or had an active urinary tract infection or bleeding diathesis.The patients were divided into two groups, of which one group underwent the procedure using the new device,EMS laser with suction(LWS),whilst the remaining patients with standard Holmium laser with no additional suction (LOS) device.One hundredconsecutive retrospective patients meeting the inclusion criteria were included in each of the arms.During the said period, 367 patients underwent mini-PCNL at our institute,out of which 105 patient underwent mini-PCNL using LWS device, and five patients did not meet the inclusion criteria, therefore, they were excluded.In the LOS groups starting from January 2017 backwards, 100 consecutive cases meeting the inclusion criteria were included out of the 262 patients.
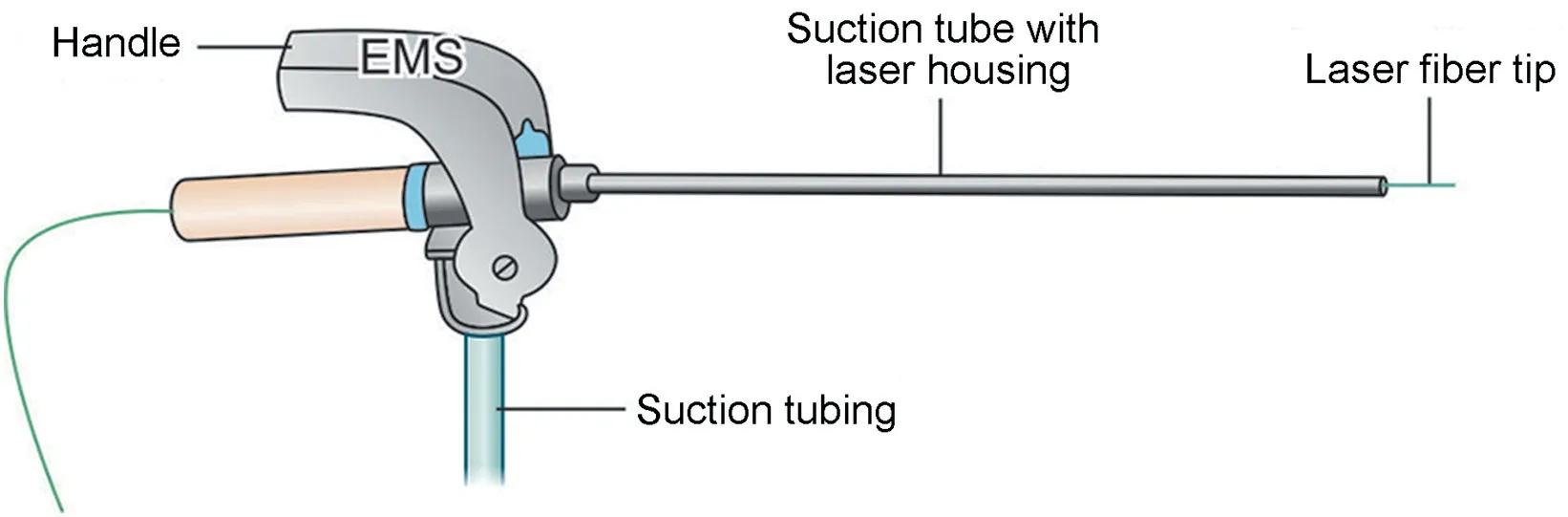
Figure 1 The diagrammatic representation of laser with suction device.EMS, Electro-Medical Systems.
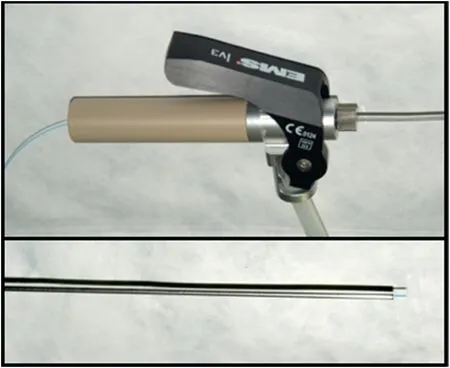
Figure 2 The laser with suction device.
Age of patient,stone size and Hounsfield unit(HU)were recorded.Primary outcomes assessed were duration of surgery and stone free rate.In addition, any complications were graded according to Clavein-Dindo classification.
Mini-PCNL was performed using standard method by means of the Karl Storz MIP-medium (MIP-M) set.The procedure was performed under general anesthesia in prone position after the insertion of the ureteric catheter in a lithotomy position.Access to the PCS was achieved using fluoroscopy guidance with an 18-gauge needle.Terumo guidewire was manipulated such that it was placed down the ureter or coiled in the system.Subsequently, the entry was dilated using a 12 Fr screw dilator,followed by a single step dilator which accompanies the MIP-M(15 Fr/16 Fr,16.5 Fr/17.5 Fr) sheath.The 12 Fr nephroscope was advanced through the sheath and once the stone was visualized,laser lithotripsy was initiated using the EMS LaserClast system(Electro-Medical System™,Nyon,VAUD,Switzerland).Laser setting was kept at a long pulse width, with frequencies ranging from 6 Hz to 20 Hz and energy ranging from 0.5 J to 1.5 J.Initial settings were 0.5 J and 15 Hz.If found less effective,the power and frequency were increased serially.For dusting,0.5-0.7 J and 15-20 Hz setting were used.For fragmentation, 0.9-1.5 J energy and 10-15 Hz frequency were chosen.LWS allowed stone fragments/dust and clots to be concurrently evacuated while the lasing of stone was carried out.The irrigation was only by gravity and no pressurized irrigation was used.In the group of patients who underwent LOS, the stone dust was left to pass spontaneously whilst clots were removed with graspers.A ureteric catheter was placed in an uneventful case,whereas a double-J stent was placed in cases with impacted pelvi-ureteric junction (PUJ) stone, excessive manipulation of PUJ and injury to Pelvis or PUJ.Routinely,no nephrostomy was placed unless there was a perforation in the PCS, infected urine, or brisk bleeding.Postoperatively, a kidney urinary bladder (KUB) X-ray and ultrasound of the kidneys were performed on post-operative Day 1 and at the end of the first month.Pain was assessed using the visual analogue score.Complete clearance was defined as the inability to detect stone on both modalities or a presence of stone fragment measuring less than 2 mm at the end of 1 month.If there were residual fragments,additional auxiliary procedures were carried out.Statistical analysis was performed using SPSS software version 24(IBM,Armonk, NY, USA).For comparison of two groups, independent two sample t-test was applied, with p<0.05 being statistically significant.
3.Results
A total of 200 patients included in the study were divided into two equal groups, LWS (n=100) and LOS (n=100) groups.Table 1 shows the patient demographics such as age,gender,and stone size of both the groups.The mean ages of enrolled patients in both the groups were comparable(41.2 years vs.43.3 years).There were significantly more patients with multiple stones in the LWS group than in the LOS group.In LWS group,two patients required two punctures and one patient required three punctures.Three patients in LOS group required two punctures.In addition,the stones were denser with a marginally higher HU in the LWS group(HU 1286)when compared to the LOS group(HU 1207).
Table 2 displays variables with regards to safety and efficacy of mini-PCNL with and without laser suction.The mean operative time was longer in the LOS group(62.0 min)as compared to LWS group(56.9 min),though it was not statistically significant.The pain scores assessed by visual analogue score at 6 h,12 h and 24 h after surgery were similar between the two groups.Post-operatively,the decrease in hemoglobin was assessed on the first post-operative day.Bleeding rates were very low and hence no significant difference was observed between the two groups(1.2 g/dL vs.1.2 g/dL,p=0.86).No significant difference in overall post-operative complications was noted.Each group had four patients who had fever(Grade 1) during the post-operative period while the three patients developed a urinary tract infection (Grade 2)requiring a course of antibiotics in the LWS group.There was one patient in each group who underwent angioembolization.Both of them presented with episodic hematuria 1 week after the surgery and were diagnosed to have arterio-venous fistula of computerised tomography (CT)angiography.None of the patients needed blood transfusion.The other Grade 3 complication in the LOS group was in a patient who developed clot retention requiringbladder irrigation.Nephrostomy placements in the two groups were similar.None of the patient in the LWS group required any auxiliary procedure but one patient in the LOS group underwent second look nephroscopy for residual fragments.Complete clearance of stone at 1 month was in favor of LWS at 96%,whereas in the LOS group,only 92% of the patients achieved complete clearance without statistical significance.

Table 1 Demographic characteristics of patients (n=200).
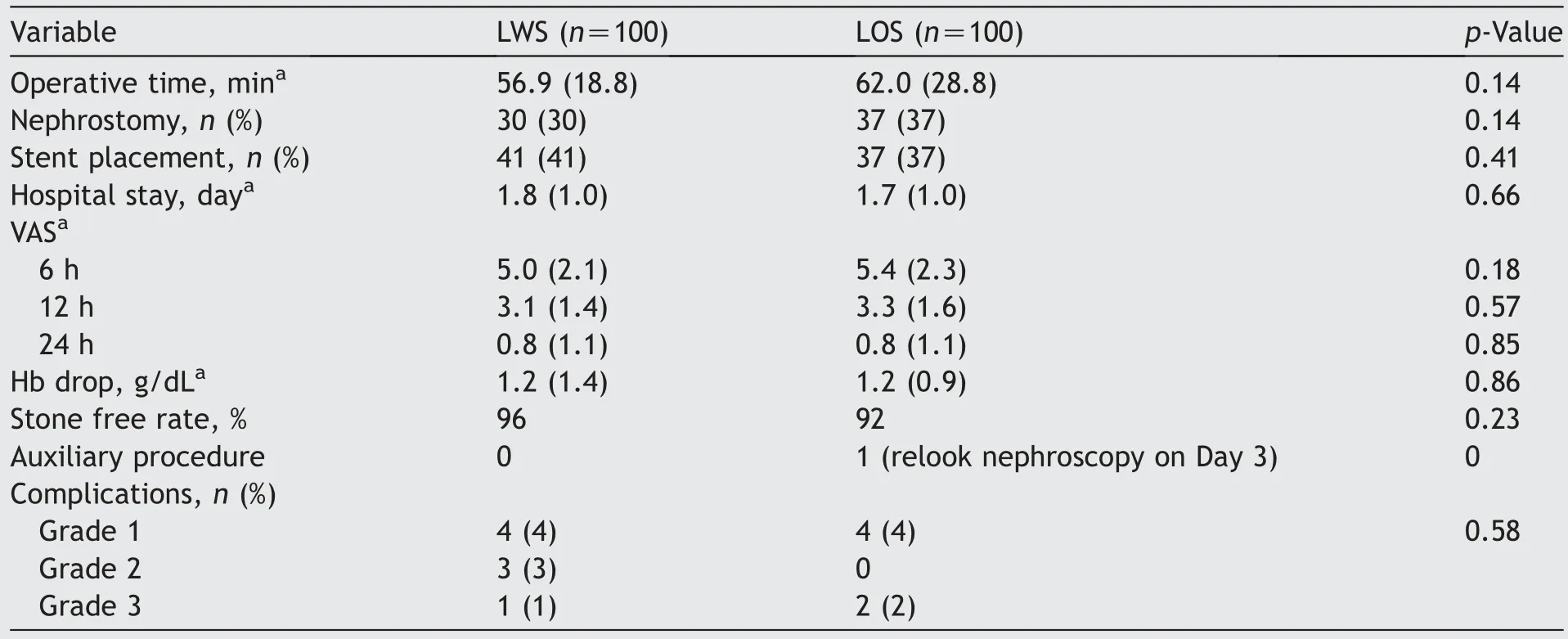
Table 2 Comparison of mini-PCNL with and without laser suction (N=200).
A subgroup analysis was performed for different stone sizes namely >15 mm,>18 mm,and >20 mm.It was found that in patients with a stone size of more than 18 mm with comparable mean stone size, there were some differences between the two groups.A significant difference was seen with more patients having complete clearance in the LWS group(100%)compared to the LOS group(85.7%).The need for nephrostomy was less in the LWS group(20.7%)whereas it was placed in 57.1%of patients in the LOS group.Hence,the initial pain scores were less in the LWS group than in the LOS group (4.7 vs.6.0, p=0.02) (Table 3).
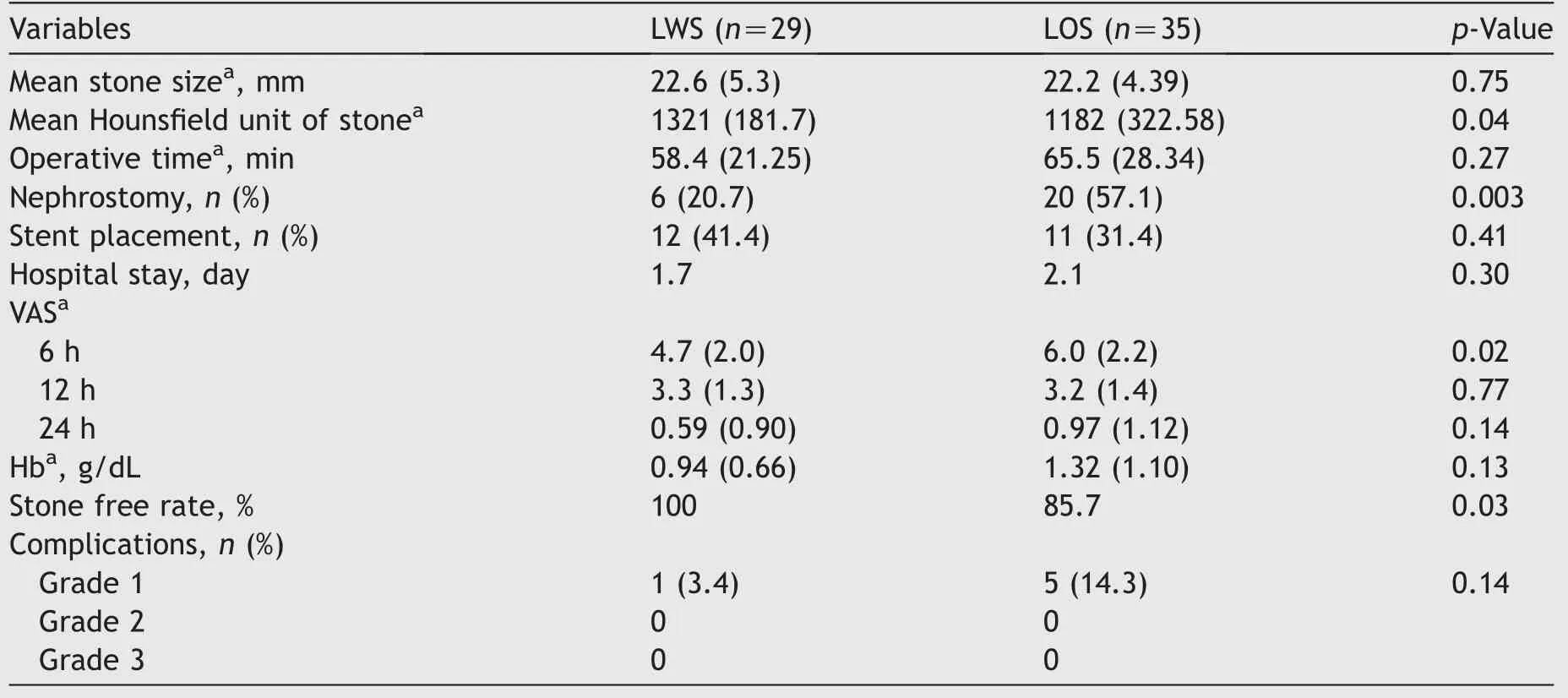
Table 3 Comparison of mini-PCNL with and without laser suction in patients with stone size >18 mm.
4.Discussion
PCNL has evolved through the years and certainly the miniaturization of instruments, optics and accessories was an essential part of this evolution.The most commonly reported drawbacks of PCNL include pain associated with the nephrostomy tube and bleeding [5].Both can be addressed with mini-PCNL,especially in the hands of skilled surgeons where these adverse effects are minimal.
Mini-PCNL uses a very small access tract hence nephrostomy need not be placed in most cases unless there is brisk bleeding.It is well accepted that the size of nephrostomy tube is the main determinant of pain and analgesic requirements in patient after PCNL [6].Hence, tubeless PCNL will reduce the pain related to the procedure.Secondly, despite the best access to the kidney, a large dilatation results in greater bleeding.Kukreja et al.[7] demonstrated reduced bleeding and lower transfusion rates when dilatation was kept to less than 22 Fr, compared to those where dilatation was more than 30 Fr.Laser technology has become an important tool in stone fragmentation over the years,especially in mini-PCNL due to the small caliber of the fiber which made it compatible with smaller size scopes.Laser also tends to produce finer fragments compared to pneumatic or ultrasonic lithotripsy.However, there was one issue that still needed resolution, that is, an increase in operative time, as the diameter of the sheath determined the size of fragment that could be pulled out through the sheath [8].
Suction coupled with other lithotripsy devices enhances the vision by clearing the blood clots and stone dust.The other added advantage is decrease in retropulsion seen when suction is used with laser.Suction effect allows the stone to stay very close to the sheath, preventing unintentional migration of the stone to other parts of PCS.Hence,the new device with its suction tube was conceived.Within the outer tube, a small internal sheath houses the laser fiber.This brings together the advantages of using laser which produces smaller fragments and suction which simultaneously evacuates stone dust and small fragments.The resultant effect is a more efficient device which shortens operative time and helps achieve better stone clearance.In our study the operative time was statistically not different between the groups, but it was still 5 min lesser in LWS group as compared to the LOS group.The stone clearance was improved in the LWS group (96%) in comparison to the LOS group (92%), though this was not statistically significant.However, in the subgroup of largerstones with size more than 18 mm, the difference was significant (100.0% vs.85.7%, p=0.03).This may be explained by the fact that larger stones result in numerous fragments and the suction effect is more pronounced,reducing the retropulsion effect.Hence this produces better and more potent clearance of stone fragments.This has been shown in the study by Zengin et al.[9].They evaluated patients who underwent PCNL using three different types of lithotripsy devices-pneumatic, ultrasonic and combination.The stone free rate was 67.7% in the pneumatic group whereas in the combination group using both pneumatic and ultrasonic with suction, the stone free rate was much higher at 85.5% (p=0.04) [9].
The present study was in accordance with previous reported studies revealing the potential advantages of mini-PCNL such as decrease in blood loss, transfusion rate, pain, and length of hospital stay with a stone free rate of 89%[10].
There has always been controversy on high intrarenal pressures in mini-PCNL.When suction is used, it should reduce the intrarenal pressures as well as the fluid absorption during the surgery.This in turn should reduce rates of sepsis.In the subgroup of patients with stone size >18 mm,there were fewer patients in the LWS group compared to the LOS group who had fever though it did not reach statistical significance (3.4% vs.14.3%).With the addition of suction, a reduction in mucosal trauma occurred due to accurate delivery of energy to stone which would consequently reduce the risk of bleeding and perforation.Accordingly, the absence of such complications also decreases the need for nephrostomy placement.There was a minimal difference in bleeding when all stone sizes were considered but in patients with stones more than 18 mm, the LWS group had a lower drop in hemoglobin of 0.94 g/dL compared to LOS which had a decrease of 1.32 g/dL.There was no statistical difference but the trend was emerging when larger stones were dealt with the mini-PCNL instruments (Table 3).Vision was important in the smooth progress of the procedure and suction cleared the stone dust and clots more expediently,reducing injury to the urothelium.
Yang et al.[11] demonstrated the efficient use of mini-PCNL with suctioning system to control renal pelvic pressure, reduce complications, and improve operative time in renal staghorn calculi.
Recently, other laser technologies have emerged [11].The Moses technology is multiple pulse mode inbuilt in the Lumenis 120 W laser that reduces retropulsion and improves stone fragmentation by maximizing the laser energy passage through water.Moreover, thulium fiber laser has arrived into the lithotripsy scene to enable dusting with very high frequencies and extremely low energy settings.Comparison with these technologies would be pertinent to establish the role of this device when mini-PCNL is employed as a treatment option for renal stones.
There were limitations to this study.Importantly, it was a retrospective study where the groups were not randomized to either treatment arm.A cut-off size of 18 mm was used which is not in accordance to the size criteria laid down by guidelines.Despite that,as the numbers within the groups were large,the groups were found to be comparable in terms of patient age and stone size.The stone clearance at 1 month was evaluated using a kidney, ureter and bladder X-ray and an ultrasound of the kidneys.This might underestimate the number of residual stones in the kidney post-operatively.However, practically, this is the usual method of assessment of residual stones since CT imaging involves more radiation.
5.Conclusion
LWS device is safe and efficacious when used with mini-PCNL.For stones greater than 18 mm, it has a better stone free rate as compared with using no suction.This is the first clinical experience with the device.Therefore, more clinical trials are needed to validate our results.
Author contributions
Study concept and design: Abhishek Gajendra Singh.
Data acquisition: Abhishek Gajendra Singh, Shrikant Jai.
Data analysis: Abhishek Gajendra Singh, Sundaram Palaniappan.
Drafting of manuscript: Abhishek Gajendra Singh, Gopal Tak, Arvind Ganpule.
Critical revision of the manuscript: Abhishek Gajendra Singh, Sundaram Palaniappan, Shrikant Jai, Gopal Tak,Arvind Ganpule, Ravindra Sabnis, Mahesh Desai.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2022年1期
Asian Journal of Urology2022年1期
- Asian Journal of Urology的其它文章
- Chromophobe renal cell carcinoma: Novel molecular insights and clinicopathologic updates
- The role of preoperative dutasteride in reducing bleeding during transurethral resection of the prostate: A systematic review and meta-analysis of randomized controlled trials
- Efficacy and safety of desmopressin on frequency and urgency in female patients with overactive bladder and nocturia,current clinical features and outcomes: A systematic review
- The impact of the coronavirus disease 2019 pandemic on elective urological procedures in Australia
- Efficacy of a combination of dutasteride,tadalafil,and solifenacin in the treatment of previously unsuccessful patients
- Associations between IL-1RN variable number of tandem repeat, IL-1β(-511)and IL-1β (+3954) gene polymorphisms and urolithiasis in Uighur children of China