
Safety and efficacy of Endovascular Management of high-grade blunt renal injury
2022-03-10 07:01BinWngChongpeiWenSonglinSongGuilinLiYnggngYnShouciChengJunmeiZengZhidongLinYongWng
Bin Wng, Chongpei Wen, Songlin Song, Guilin Li, Ynggng Yn, Shouci Cheng,Junmei Zeng, Zhidong Lin, Yong Wng,c,d,*
a Department of Interventional Radiology, The Second Affiliated Hospital of Hainan Medical University, China
b Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, China
c Key Laboratory of Emergency and Trauma (Hainan Medical University), Ministry of Education, China
d Department of Emergency, Hainan Clinical Research Center for Acute and Critical Diseases, The Second Affiliated Hospital of Hainan Medical University, China
Keywords:Blunt renal injury High grade Renal arterial embolization Endovascular treatment
ABSTRACT
1. Introduction
Blunt renal injury is a common clinical emergency,and the treatment options, including conservative measures, endovascular treatment, and surgery, are selected on the basis of the classification of the American Association for The Surgery of Trauma (AAST).1Generally, it has been proven that conservative management can achieve satisfactory clinical results for grade I-III blunt renal injury.Until recently,no consensus had been reached for grades IV to V. Whether to perform nonoperative management or surgery also remains controversial.2-4Renal artery embolization(RAE)is widely applied in patients with acute renal injury as a nonsurgical treatment; however, its efficacy and safety for the treatment of high-grade blunt renal injury are still not well established in literature.5While there have been a number of single-center reports on the results of RAE for renal trauma,few have focused on high-grade renal injuries.This article describes our experience with high-grade blunt renal injury, focusing on the medium to long-term outcomes of endovascular treatment.
2. Materials and Methods
2.1. Patients
This was a cohort study conducted as a retrospective analysis of a prospective database in a single level 1 trauma center. A total of 78 patients with blunt renal injury were registered accordingly, and 31 consecutive patients with renal injury were admitted to undergo endovascular treatment between July 2014 and December 2019. Fifteen patients with high-grade blunt renal injury(AAST grades IV-V)during that period were included in this study, while 14 patients with low-grade blunt renal injury and two patients with penetrated renal injury were excluded accordingly(Fig.1).The decision whether to perform RAE was made by the trauma MDT team, including urologists, trauma surgeons and interventional radiologists, mostly based on clinical symptoms, hemodynamic stability,and associated injury.While the patients had given informed consent for their procedures,consent for inclusion in this study was not required due to the retrospective nature of the study. Data of patients were used confidentially and anonymously. The study protocol followed all appropriate guidelines according to the Declaration of Helsinki and was approved by the Ethics Committee.
2.2. Angiography and endovascular treatment
All interventions were completed by three interventional physicians,who had more than 10 years of medical experience. The patients were placed in the supine position. The right or left femoral artery was punctured by the modified Seldinger technique after the induction of local anesthesia. Abdominal aortic angiography was conducted first to confirm the number and position of the renal arteries. Selected renal artery angiography was then performed to confirm the involved artery;subsequently, a progreat microcatheter (Terumo, Tokyo, Japan) was superselectively inserted into the involved artery. Embolization was performed with different embolic agents, including gelatin sponge (GS)particles,microcoils,and n-butyl cyanoacrylate glue.Finally,renal artery angiography was repeated to confirm that embolization was complete.
2.3. Assessment and follow-up
Changes in hematuria and blood hemoglobin were evaluated after surgery. Clinical success was defined as cessation of hematuria and stabilization of hemoglobin and/or hematocrit without the need for ongoing blood transfusions. When recurrent bleeding was recognized in the patient, the decision to administer further treatment was made after discussion with a multidisciplinary team composed of urologists and interventional radiologists. Blood pressure, renal function (e.g., creatinine, blood urea nitrogen), and related symptoms post-procedure (such as fever, pain, persistent hematuria) were recorded accordingly. Color Doppler ultrasound and/or CT with or without enhancement were performed within 3 months. Patients were followed until they were lost to follow-up, or in case they died, or up to December 31, 2019. Complications, such as urinoma, urinary tract infection, renal failure, and secondary hypertension,and all further required interventional procedures,such as repeated RAE or local drainage, were documented for these patients.
2.4. Statistical analysis
Quantitative variables, such as blood pressure(systolic and diastolic blood pressure)and creatinine values before and within 7 days after the procedures,were compared by the Student t-test using SPSS version 13.0(SPSS Inc.,Chicago,Illinois).A P <0.05 was considered to be statistically significant.
3. Results
3.1. Patients’ demographics
According to the AAST classification,11 patients with grade IV and 4 patients with grade V blunt renal injury, who received endovascular treatment, were included in this study. Further, the study sample consisted of 13 men and 2 women,with an average age of 41.6 years(range 8-73 years).Ten cases of injury occurred in the left kidney and 5 in the right kidney.The modes of injury included falls(n =11) and traffic accidents(n=4).Hemodynamics were stable in 4 patients and unstable in 11 patients. All patients had flank pain and 6 patients had gross hematuria. Associated injury included lumbar or rib fracture (n = 4), pelvic fracture(n=2),spleen injury(n=2),adrenal injury(n=1),and aorta dissection (n = 1). Previous diseases related to renal function included diabetes in 2 patients,hypertension in 3 patients,and hydronephrosis in 1 patient.All the patients showed normal renal function before treatment except for 1 patient with diabetes(CKD stage II).
3.2. Endovascular treatment and follow-up
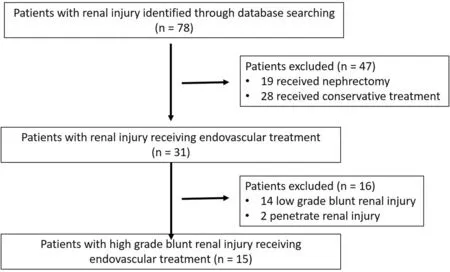
Fig. 1. Flowchart of patient selection.
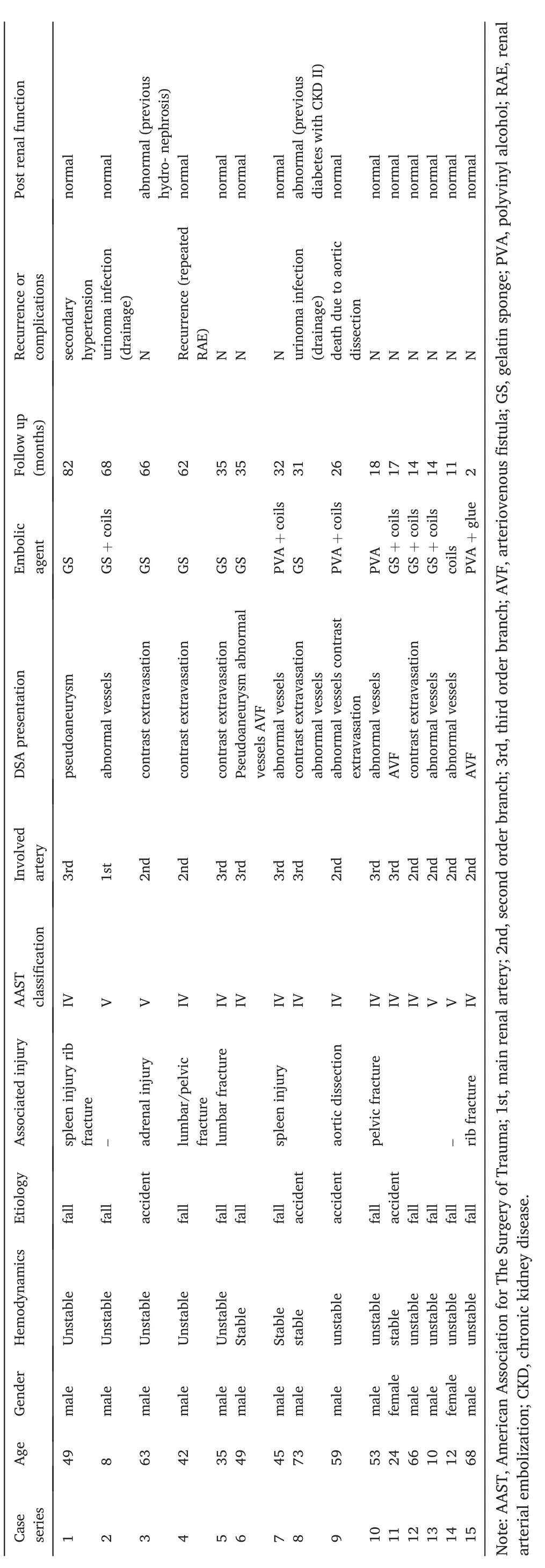
Table 1 Patients demographics, endovascular treatment and follow up.
All the patients were treated with RAE. All the interventional procedures were performed within 2 h, and the dosing for the procedures was generally around 30-50 mGy.The main renal artery was involved in one case, while in 7 cases it was the second order branch and in the remaining 7 cases, it was the third order branch. Digital subtraction angiography (DSA) showed abnormal vessels (vessel disruption and/or abnormal stain)in 8 patients,extravasation of the contrast medium in 6 patients, pseudo-aneurysm in 2 patients, and arteriovenous fistula in 3 patients.Among them,3 patients showed mixed DSA appearance.
One patient was treated by embolization with sacrifice of the main renal artery stem, and the remaining 14 patients were treated with second/third arterial embolization.One patient was treated by embolization with microcoils,7 with GS particles or polyvinyl alcohol particles(PVA)alone, 6 with GS/PVA plus coils, and 1 with PVA and n-butyl cyanoacrylate glue.
Primary clinical success was achieved in 14 patients (93.3%),including in all patients with grade V blunt renal injury. RAE was repeated in 1 patient with persistent hematuria,which finally resulted in clinical success. No significant differences in creatinine levels were observed before and after embolization (97.33 ± 42.07 μmol/L VS 103.73±39.26 μmol/L,P=0.67).The mean follow-up period was 34.2 months (from 2 to 82 months). Only 1 patient with previous hydronephrosis in the contralateral kidney developed renal failure. Two patients required percutaneous catheter drainage/or transurethral double pigtail tube pelvic drainage due to urine leaks with infection). One patient developed secondary hypertension 6 months after RAE and required the initiation of antihypertensive therapy. No additional antihypertensive agents were needed after RAE in two patients with primary hypertension(Table 1,Examples see Fig.2).
Note: AAST, American Association for The Surgery of Trauma; 1st,main renal artery; 2nd, second order branch; 3rd, third order branch;AVF, arteriovenous fistula; GS, gelatin sponge; PVA, polyvinyl alcohol;RAE, renal arterial embolization;CKD,chronic kidney disease.
4. Discussion
According to AAST classification, operative management is recommended for those patients with grade IV and grade V renal injuries when conservative measures have failed in the early stage.RAE is attempted for those patients who refuse nephrectomy.Recently,RAE has been used as a method of nonoperative management,which is considered the standard therapy for grade I-III renal trauma.6Few studies have evaluated the outcome of RAE in patients with high-grade renal trauma.In this study,RAE showed high success rates in patients with high-grade renal injuries(grades IV-V), thereby avoiding further surgical intervention, such as nephrectomy.
The indication for RAE in patients with renal trauma remains controversial. Previous research showed high failure rates of RAE in patients with active vascular extravasation,as observed on the computed tomography scan taken at admission,and blood transfusion requirements during the first 24 h.7Moreover, RAE was performed in hemodynamically stable patients, and surgery remains the preferred method among patients with hemodynamic instability.8In our experience, RAE should be considered when conservative measures fail, clinical symptoms aggravate, or a relevant hemoglobin decrease occurs in patients.Furthermore, there was no large difference in the clinical success rate between patients with and without hemodynamic instability. A recent study also supports that angioembolization is an alternative method in the management of hemodynamically unstable patients with blunt renal trauma.9Finally, if the clinical course allows10and when the initial intervention fails in a patient, RAE should be attempted a second time since the success rate is equally high. Generally,the DSA appearance of renal injury can be categorized into 4 major types: extravasation of the contrast medium, pseudoaneurysm, AVF, and abnormal vessels (vessel disruption and abnormal stain). Various embolic agents have been used for RAE, and microparticles (GS or PVA) and coils seem particularly well-suited for this indication. Liquid embolic agents have also demonstrated high efficiency in generating permanent occlusion;however,they must be used with caution to avoid reflux into non-targeted arteries and to preserve renal function as much as possible.8,11
Major complications of RAE, such as renal failure and secondary hypertension, were minimal in our series. Renal failure was not only associated with contrast medium injection but also with interventional procedures.12,13This study showed no significant differences in the level of creatinine or blood urea nitrogen estimated in patients before and after RAE. Renal failure was found in 1 patient with contralateral kidney hydronephrosis and in 1 patient with abnormal renal function before the intervention.
Available evidence has also shown that kidney function after RAE is well preserved in patients.12,13,and14Collinset al.have reported either the onset of hypertension or worsening of preexisting hypertension in the follow-up of 6%of patients treated with RAE and they also reported that incomplete RAE or proximal embolization may induce distal ischemia,therebyresultinginanupregulationofthe renin-angiotensin-aldosterone system and hypertension.14Another study showed no significant differences in systolic blood pressure or blood pressure stage after RAE.15In our series, the majority of patients were embolized with GS or PVA particles and they were proximally embolized with microcoils, which ensured that embolization was complete. The result was satisfactory, and only 1 patient, in whom embolization occurred with large GS particles(diameter >1000 μm),developed hypertension.No worsening of preexisting hypertension occurred in the follow-up period.
This study has its limitation.It was a single-center retrospective study of endovascular treatment in high-grade blunt renal injury. Since only those patients who were able to undergo angiography were included,the results were limited by the small sample size.Hence,it will be valuable to design a prospective trial using both imaging and clinical parameters to predict the need for endovascular intervention.16,17
5. Conclusions
In conclusion, RAE can provide high success rates of hemostasis for both hemodynamically stable and unstable patients with high-grade blunt renal injury (AAST grades IV-V) and only minor complications are observed with this procedure.
Source of funding statement
This work was supported by a research start-up fund for talent introduction of the Second Affiliated Hospital of Hainan Medical University.
Authors contributions statement
Bin Wang and Chongpei Wen: Conceptualization, Data curation,Writing-Original draft preparation.
Songlin Song, Guilian Li, Yanggang Yan, Shoucai Cheng, Junmei Zeng,and Zhidong Lin:Visualization, Investigation.
Yong Wang:Writing-Reviewing and Editing,Supervision.
Declaration of competing interest
The authors report no conflicts of interest in this work.
 Journal of Interventional Medicine2022年1期
Journal of Interventional Medicine2022年1期
- Journal of Interventional Medicine的其它文章
- Molecular targeted therapy causes hepatic encephalopathy in patients after Transjugular intrahepatic portosystemic shunt (TIPS): A case report and literature review
- A low-grade cerebral arteriovenous malformation suspected of being a metastatic tumor: A case report and literature review
- Angiography findings and endovascular management of acute nonvariceal gastrointestinal bleeding: A pictorial essay
- Comparison of tumor response following conventional versus drug-eluting bead transarterial chemoembolization in early- and very early-stage hepatocellular carcinoma
- Complications from port-a-cath system implantation in adults with malignant tumors: A 10-year single-center retrospective study
- Paclitaxel-coated balloons angioplasties for extra-long femoropopliteal artery atherosclerotic lesions(>30 cm):12 months outcomes from a single center