
A low-grade cerebral arteriovenous malformation suspected of being a metastatic tumor: A case report and literature review
2022-03-10 07:02TingPanGangLuLiangGeYeqingJiangHailinWanShuXuXiaolongZhang
Ting Pan, Gang Lu, Liang Ge, Yeqing Jiang, Hailin Wan, Shu Xu, Xiaolong Zhang
Department of Radiology, Affiliated Huashan Hospital, Fudan University, Shanghai, China
Keywords:Cerebral arteriovenous malformation Large-area brain edema Low-grade
ABSTRACT Cases of low-grade cerebral arteriovenous malformations (cAVMs) showing dynamic changes and large areas of brain edema on short-term MRI follow-up have rarely been reported. This report describes an incidentally discovered and initially misdiagnosed cAVM in a patient with malignancies. The presence of abnormal signals surrounded by large areas of brain edema combined with tortuous or dilated vessels indicates the possibility of an AVM, especially in young people.
1. Introduction
Cerebral arteriovenous malformations (cAVMs) are uncommon dysmorphic vascular connections that usually present with intracranial hemorrhage, epilepsy, headaches, and focal neurological deficits.Computed tomography(CT)and magnetic resonance imaging(MRI)are the most commonly used non-invasive diagnostic tools. CT findings usually include punctate or linear isodensities,calcifications and/or lowdensity encephalomalacia. Diagnostically, MRI scans characteristically display black or low-signal areas (flow voids). Computed tomography angiography (CTA)and magnetic resonance angiography (MRA) enable the visualization of dilated vessels. However, cAVMs are relatively rare and can easily be missed or misdiagnosed due to atypical medical imaging and nonspecific clinical manifestations. Digital subtraction angiography (DSA) is the most reliable and accurate method for cAVM diagnosis,and is capable of visualizing abnormal vessels,dilated feeding arteries,and early venous drainage.The Spetzler-Martin grading system is most commonly used that considers the size and position (noneloquent or eloquent brain region) of lesions, and venous drainage patterns. More complex cAVMs have higher S-M grades, indicating more difficult treatment and greater risk of post-operative complications.1A dynamic low-grade cAVM with extensive edema is prone to misdiagnosis,particularly in patients with malignant tumors.In this case,a progressive lesion with a large area of cerebral edema was incidentally discovered in a 30-year-old woman with pulmonary metastasis of rectal cancer. The lesion, initially misdiagnosed as a metastasis,was in fact a cAVM.
2. Case report
Cerebral MRI in November 2019 incidentally detected a lesion in the right frontal subcortex (Fig. 1) of a 30-year-old female patient with pulmonary and hepatic metastases of rectal cancer who underwent routine examination. The patient underwent radiotherapy, chemotherapy (Folfox6), and surgery between December 2017 and March 2018. Targeted and immunotherapy drugs (Keytruda plus regorafenib and herceptin)were administered in November 2019.
Two months later, in January 2020, the lesion had become more extensive,with large areas of edema and dilated vessels around the lesion on cerebral MRI (Fig. 2). The initial diagnosis was an intracranial metastasis. In March 2020, MRI captured mixed signals on T1WI and T2WI (Fig. 3). During this time, the patient continued antitumor treatment as before. The patient did not present with common clinical or hereditary syndromes, and her physical neurological examination was negative.
Due to the presence of dilated tortuous vessels around the edema,medical imaging specialists recommended a DSA examination,and a lowgrade cAVM was confirmed (Fig. 4). Rapid dynamic changes, artery ectasia,and a single tortuous drainage vein are predictive of a high risk of rupture. After conferring on the patient and her family, transarterial embolization treatment was decided (Fig. 4) and six-month follow-up was scheduled(Fig.5)(see Fig.6).
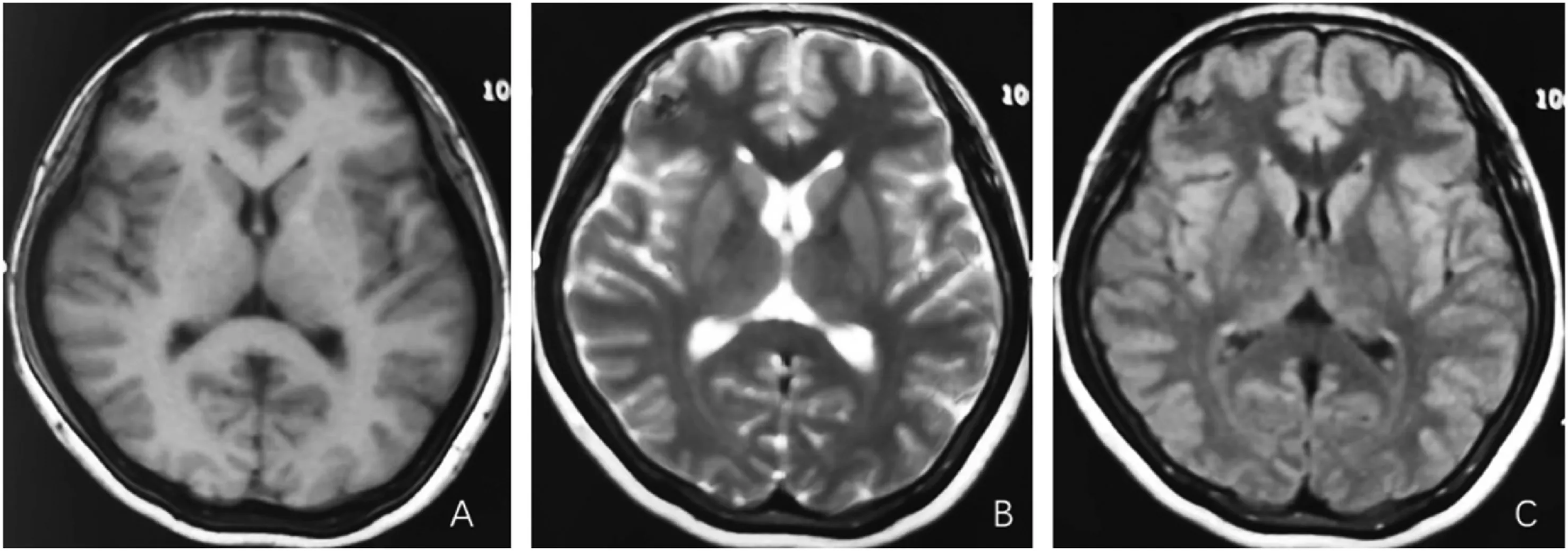
Fig. 1. Unenhanced MRI (2019.11) showed hypointensity at the right frontal subcortex. No edema was detected surrounding the small lesion.
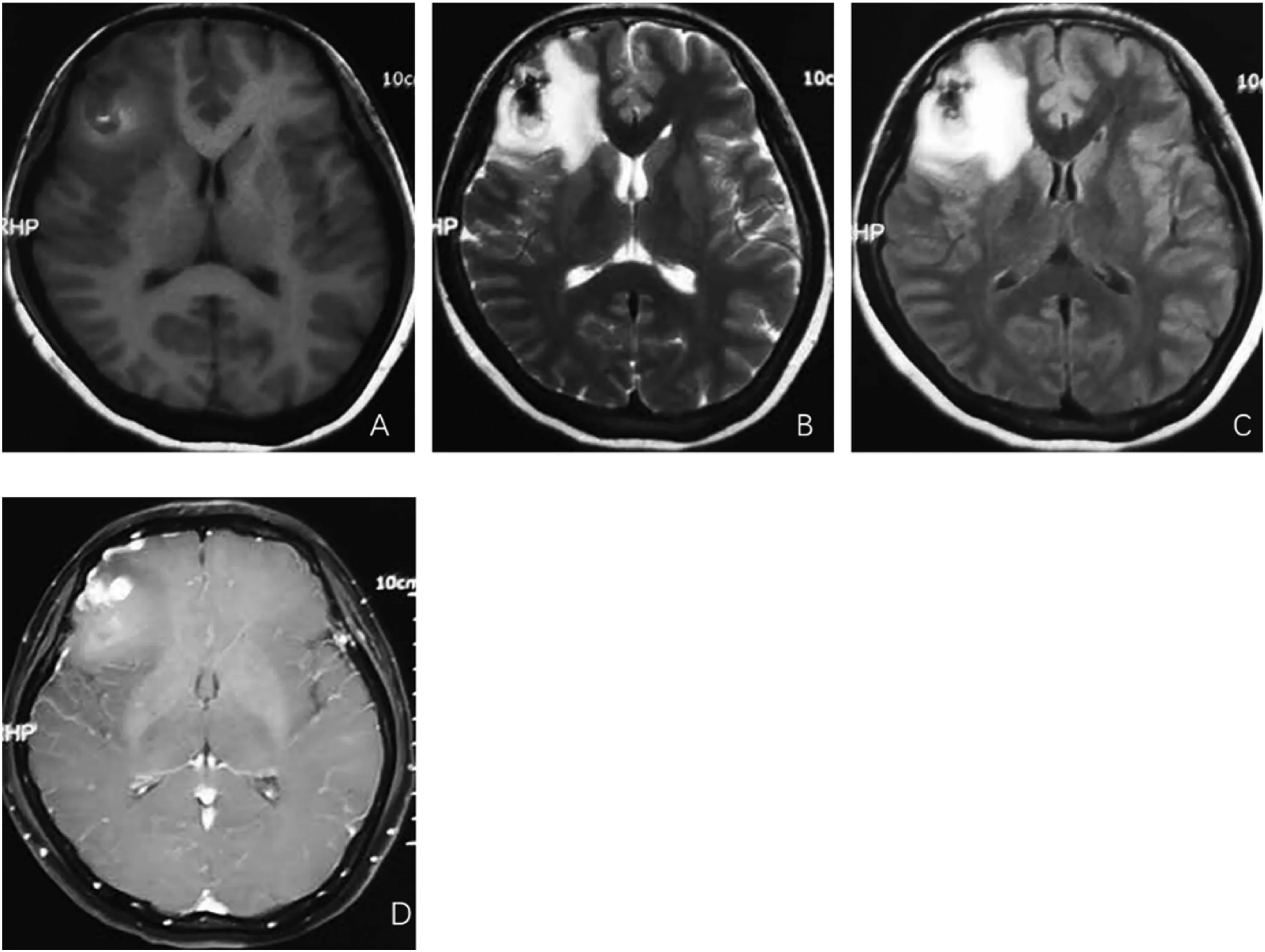
Fig. 2. Two months later (2020.01), MRI demonstrated a larger lesion with significant brain edema. Enhanced MRI (Fig. D) depicted dilated tortuous vessels.
3. Discussion
cAVM in a patient with a peripheral malignant tumor was initially misdiagnosed as a metastatic neoplasm. During the short-term MRI follow-up, dynamic changes and flow voids were observed. DSA confirmed an S-M grade I cAVM in the right frontal lobe, and embolization was performed. Roughly six months after the operation, medical imaging confirmed that the lesion was cured.
Medical imaging plays an important role in the diagnosis of cAVM.CT and MRI are important non-invasive diagnostic techniques,whereas DSA remains the gold standard. Unenhanced CT is highly sensitive in detecting hemorrhage,but is not very successful in detecting unruptured AVMs. cAVMs usually appear as isodense areas or areas of low density without a mass effect and some of them develop calcifications.Additionally,cAVMs should be suspected in young patients with cerebral hemorrhage, particularly parenchymal hemorrhage with calcification.The literature indicates that ruptured cAVMs account for 33% of intracerebral hemorrhage in people under 40 years of age and 47%of people under the age of 20 years.2MRI has higher sensitivity and specificity than CT.cAVMs characteristically appear as black or low-intensity signals on the T2 weighted images.Generally,DWI does not demonstrate restricted diffusion.3Enhanced CT and contrast-enhanced MRI can assist in the visualization of abnormal lesions and dilated vessels. Enhanced MRA is not affected by blood flow rate,and a short time of echo(TE)reduces the turbulence influence on signals and is able to display vascular structures more clearly than unenhanced MRA. CTA and MRA are suitable for imaging feeding arteries and drainage veins.
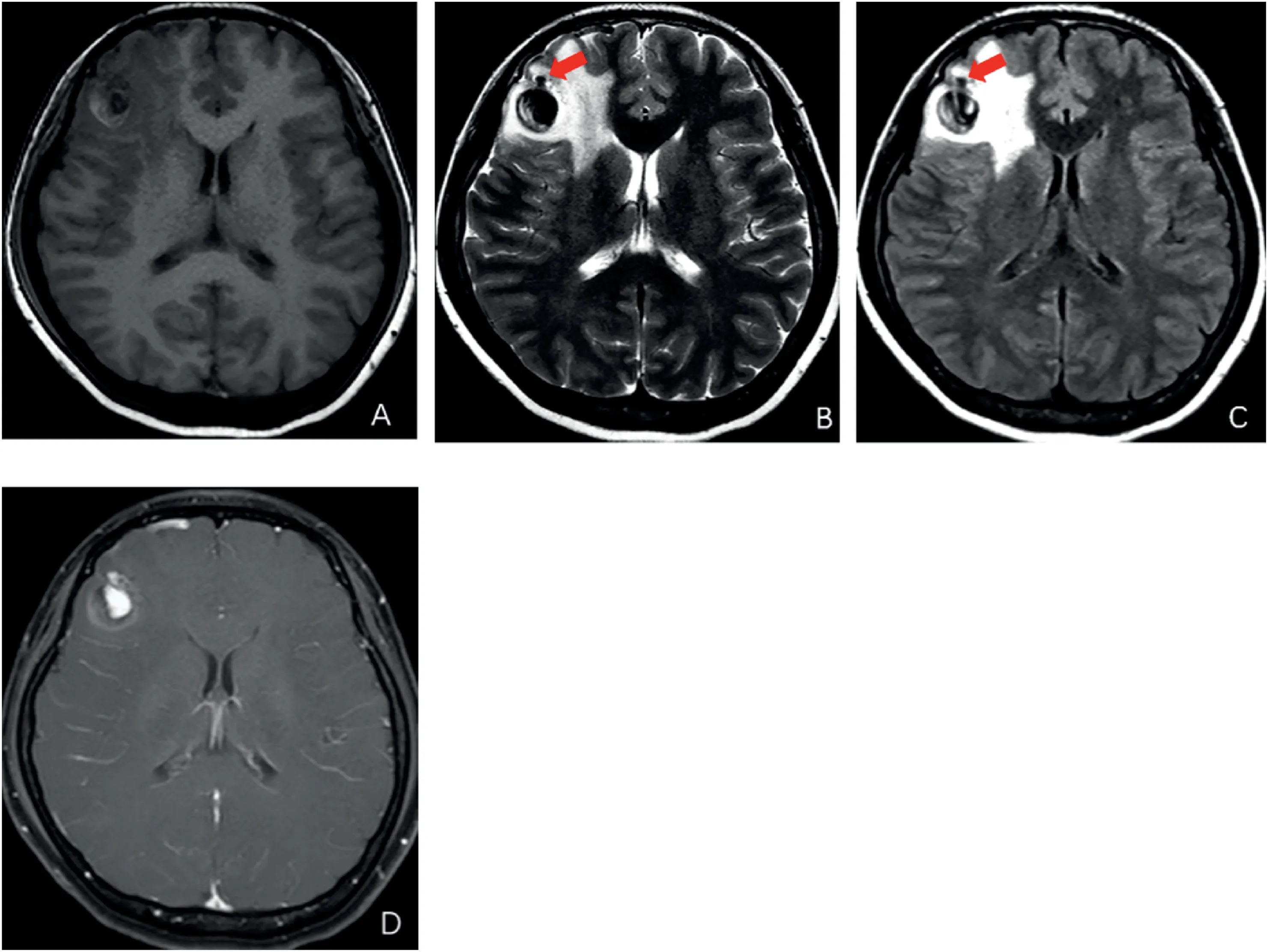
Fig.3. Four months later(2020.03),the lesion was more extensive with pseudoaneurysm formation.Flow void was revealed on T2WI and T2-flair(arrow).Figure D exhibited thrombosis and turbulence within the ectasia.
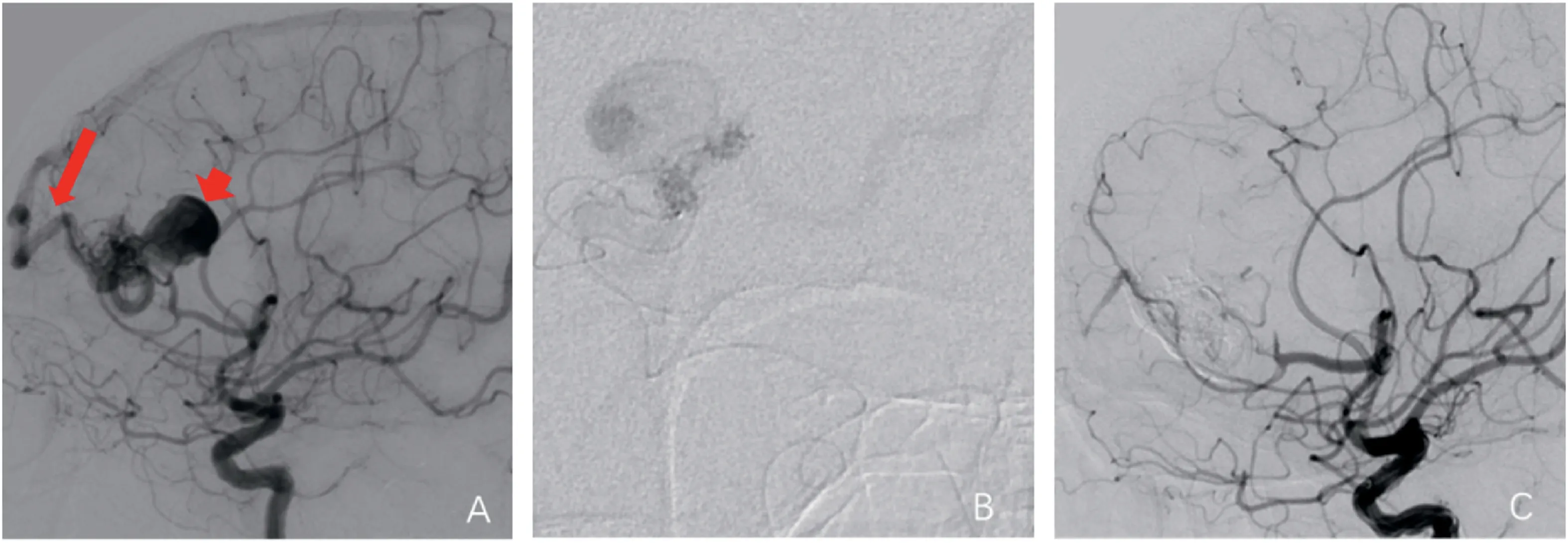
Fig. 4. Cerebral angiography and embolization were conducted in May 2020. Figure A displayed an aneurysm and single tortuous drainage vein of the low-grade cAVM, fed by the right middle cerebral artery branches with drainage into the superior sagittal sinus. Figure B showed a microcatheter advanced into the nidus via the feeding artery. Figure C revealed the cAVM was embolized successfully after 1.6ml Onyx-18 was cast into the drainage vein and nidus.
This cAVM initially misdiagnosed as a metastasis is mainly due to medical history and lesion imaging modalities. In terms of medical history,brain lesions are frequently misdiagnosed as cerebral metastasis by radiologists and physicians because of their atypical appearance on MRI.cAVM presents as a small lesion surrounded by a large area of edema.This presentation shows similarity to that of brain metastasis. Although multiple brain metastases are most common; however, many malignancies have a propensity for singular metastasis. With an incidence of 25-45%4and a tendency to be round,they are typically hypointense on T1WI with variable signals on T2WI.Metastases are often surrounded by extensive vasogenic edema,displaying a high signal on T2WI and T2-flair but a low signal on T1WI and DWI. Edema is typically confined to the white matter, and the involvement of the cortex should spur the search for other pathologies.5Neither plain CT scans nor enhanced CT scans were important limitations in our case. A mixed and relatively high density may help in the diagnosis of advanced lesions with aneurysm and thrombosis formation. Furthermore, a signal void caused by vessel structures containing flowing blood was absent on unenhanced MRI scans. Small cAVMs typically have low blood flow rates, making it challenging or difficult to detect abnormal vessels using routine MRI.As the cAVM grows its hemodynamics become more readily observable on imaging.6,7As the internal environment and hemodynamics change,cAVMs progress and become more detectable.
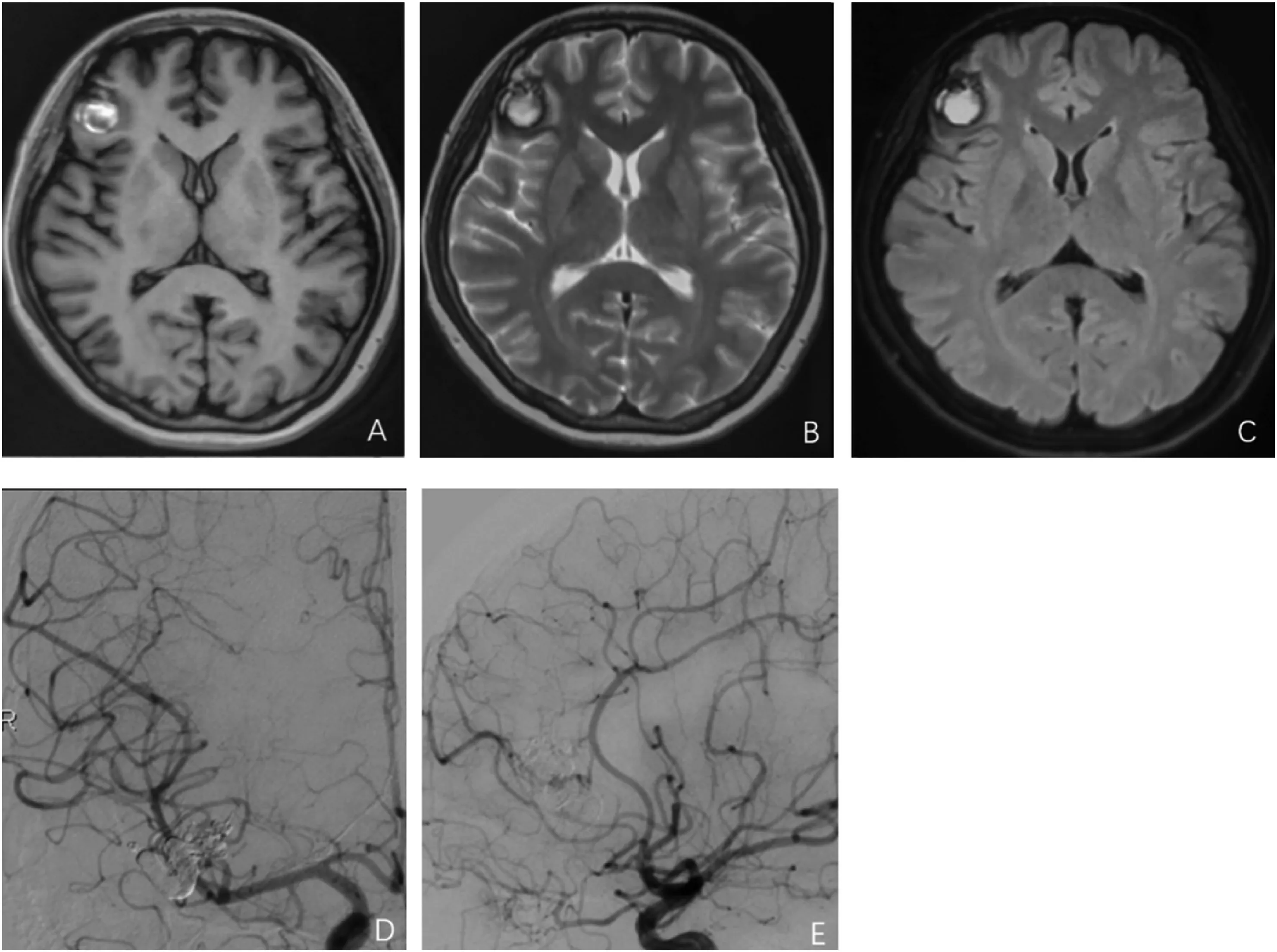
Fig. 5. Six-month follow-up after embolization (2021.12.09). Figure A, B and C showed thrombus formation in the aneurysm along with edema disappearance.
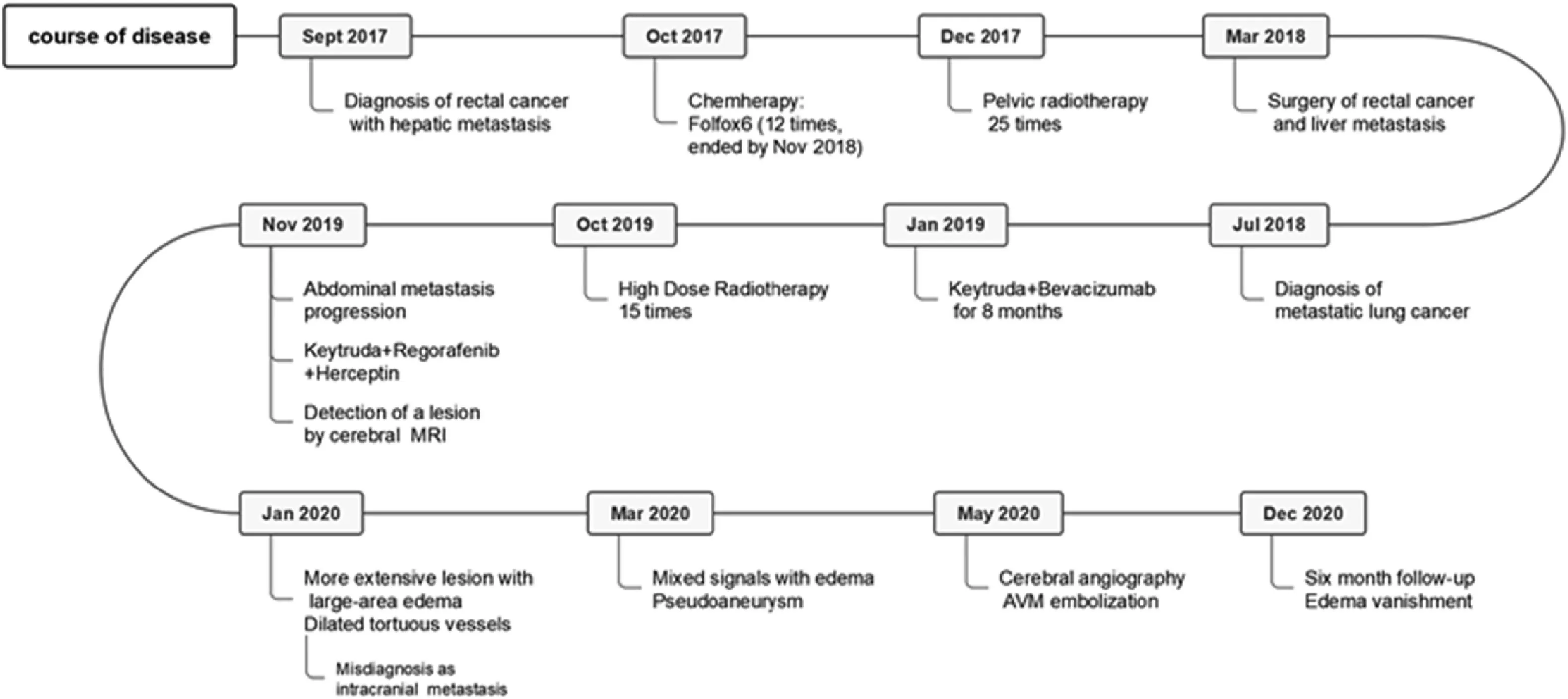
Fig. 6. The detailed information of the case.
Extensive edema commonly results from a ruptured cAVM.However,low-grade cAVMs without significant hemorrhage causing large areas of edema are rare. Inadequate drainage of a single tortuous vein, high expression of vascular endothelial growth factor (VEGF), and aneurysm growth are factors that cause edema.Venous congestion,usually induced by cortical drainage, venous varicosity, and drainage vein stenosis,8is considered as the primary cause of congestive edema. Chen et al.9reported a case of medium-sized cAVM with large-area congestive edema and main drainage venous stenosis that had not ruptured.Drainage vein stenosis and common drainage venous hypertension are also believed to cause cerebral edema. Li et al.10reported a high-grade cAVM with symptomatic varix. The edema and symptoms disappeared after regression of the varix by transarterial embolization.Aneurysm growth can also cause mass effects and cerebral edema.11Some targeted drugs such as bevacizumab and trametinib are believed to be promising for the treatment of cAVMs.12And some researchers believed that some sorts oftargeted drugs may provide novel opportunities for aneurysm suppression.13,14Consequently, we speculated that the rapid aneurysm progression may have had little connection with the anti-tumor drugs in our case. Additionally, VEGF can lead to abnormal vascular remodeling,damage to the vascular wall structure, and impairment of the BBB.Although VEGF was not tested in this case, VEGF expression is usually observed in patients with malignant tumors, especially those with multiple metastases. Akabane et al.15described an unruptured cAVM generating a 4 mm blood flow-related aneurysm with surrounding edema within 3 months.The authors believed that VEGF not only promotes the occurrence and growth of aneurysms but also increases the permeability of vascular walls.
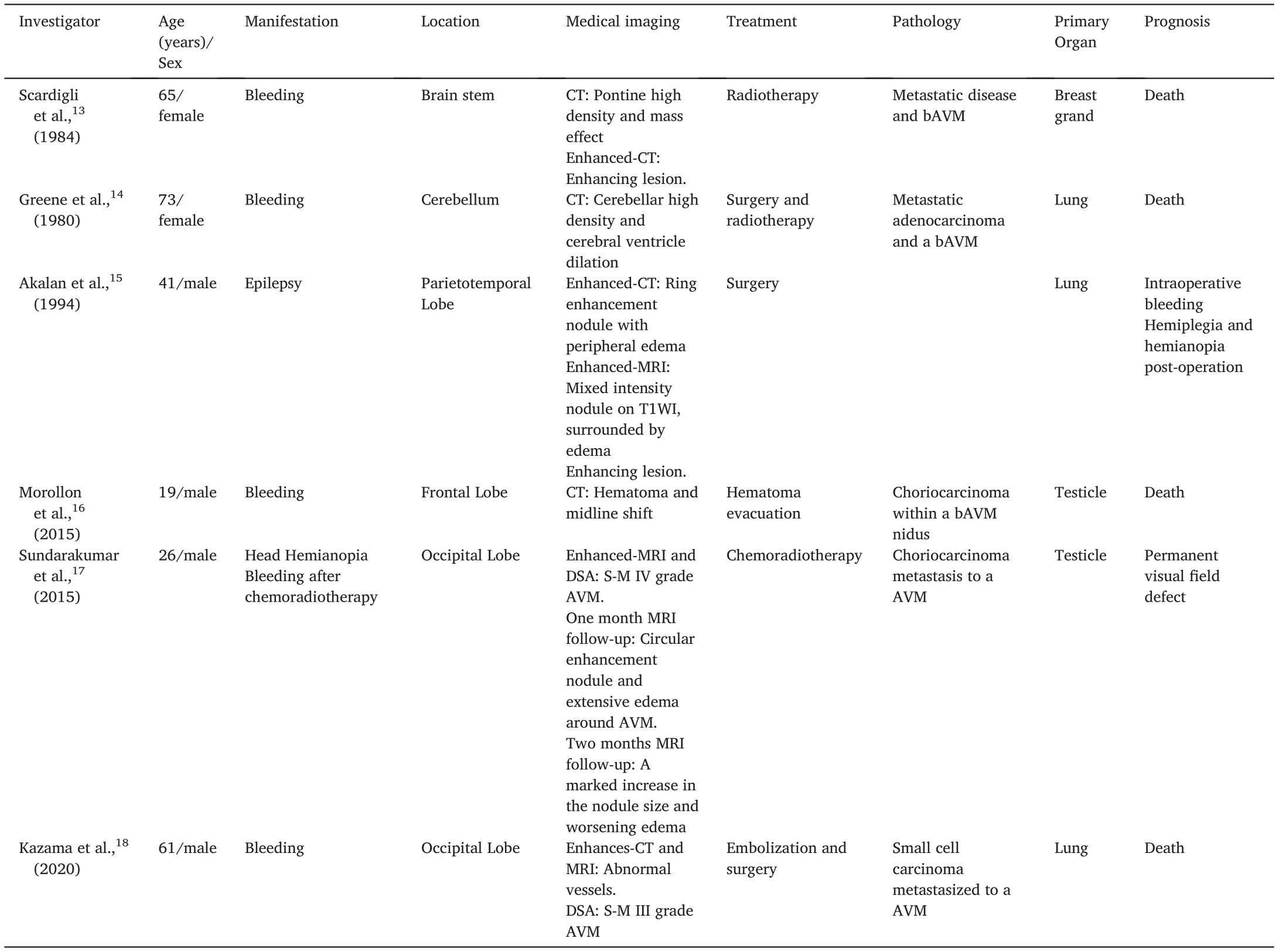
Table 1 Reported cases of metastasis to a cAVM.
In extremely rare cases, metastasis to a cAVM has been discovered,with six pathologically verified cases on record16-21(Table 1). Since intracranial metastatic tumors are apt to invade blood vessels22and endothelial cells,23,24metastasis to cAVMs is prone to hemorrhage and aneurysm formation. Five of the six known cases presented with bleeding.The other patient experienced bleeding during surgery and was hemiplegic postoperatively. Hematogenous metastasis of malignant tumors requires normal capillaries and venules; therefore, the probability of tumor cell implantation in and around a cAVM is believed to be rather low.22Some researchers have proposed that the abundant blood vessels maintained by AVMs may provide a pathway for hematogenous tumor spread.17,18,20In summary, the six reviewed cases had the following characteristics: bleeding tendency, rapid clinical progress, mass effects,and high mortality.
Without pathological examination, we were unable to confirm the occurrence of metastasis. By six-month follow-up after transarterial embolization, the edema had disappeared. MRI and DSA did not detect any abnormalities. Consequently, metastasis can be ruled out, and our case can be classified as simple cAVM.
The etiology, diagnosis, and treatment of cAVMs have always been challenging. Unenhanced CT is not sensitive for the detection of unruptured cAVMs.The presence of a flow void is a clue to the diagnosis of an AVM.In addition,dynamic follow-up by MRI, combined with other imaging modalities such as CTA and MRA, helps diagnose cAVMs, while DSA remains the gold standard. For young patients with intracranial hemorrhage, cAVMs must be considered. Despite its rarity, cAVM metastasis should not be ruled out in patients with malignant tumors or in elderly patients.
Credit authorship contribution statement
Xiaolong Zhang: Supervision, Methodology; Ting Pan: Writingoriginal draft preparation, Visualization; Gang Lu, Liang Ge: Conceptualization, Methodology; Yeqing Jiang, Hailin Wan: Writing-Review &Editing,Resources; Shu Xu:Data Curation.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
 Journal of Interventional Medicine2022年1期
Journal of Interventional Medicine2022年1期
- Journal of Interventional Medicine的其它文章
- Safety and efficacy of Endovascular Management of high-grade blunt renal injury
- Molecular targeted therapy causes hepatic encephalopathy in patients after Transjugular intrahepatic portosystemic shunt (TIPS): A case report and literature review
- Angiography findings and endovascular management of acute nonvariceal gastrointestinal bleeding: A pictorial essay
- Comparison of tumor response following conventional versus drug-eluting bead transarterial chemoembolization in early- and very early-stage hepatocellular carcinoma
- Complications from port-a-cath system implantation in adults with malignant tumors: A 10-year single-center retrospective study
- Paclitaxel-coated balloons angioplasties for extra-long femoropopliteal artery atherosclerotic lesions(>30 cm):12 months outcomes from a single center