
Primary adrenal diffuse large B-cell lymphoma with normal adrenal cortex function:A case report
2022-01-24 09:24ZhiNanFanHongJinShiBoBoXiongJinSongZhangHaiFengWangJianSongWang
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Diffuse large B-cell lymphoma (DLBCL),which accounts for approximately 30% to 40% of non-Hodgkin’s lymphoma,is the most common type among the aggressive Bcell lymphomas[1].Diffuse large B-cell lymphomas that originate in the adrenal glands are rare.Primary adrenal DLBCL (PADLBCL) is a highly malignant tumor with no specific clinical manifestations and thus,requires early diagnosis and treatment.The main manifestations of PADLBCL in patients are abdominal pain,fatigue,fever,night sweats,weight loss,and adrenal cortex insufficiency.Imaging often shows adrenal occupancy;however,clear diagnosis requires adrenal biopsy or postoperative specimen examination.To date,no unified treatment standard exists,and PADLBCL is mainly treated with immunochemotherapy,and yet has poor prognosis.Currently,there have been only few reports on PADBCLD.We here report a case of bilateral PADLBCL.Combined with related literature and our observations,we have analyzed the clinical,imaging,and pathological characteristics of PADLBCL,and discussed the current related treatment methods and prognostic factors,with an aim to deepen the understanding of this disease.
Ah! Beauty, have you the heart to desert an unhappy Beast like this? What more do you want to make you happy? Is it because you hate me that you want to escape? No, dear Beast, answered Beauty softly, I do not hate you, and I should be very sorry never to see you any more, but I long to see my father again
CASE PRESENTATION
Chief complaints
A 73-year-old man was admitted in our hospital with abdominal pain and fatigue lasting 1 mo.
Far from avoiding her, he now sought her company and seemed to take pleasure in talking to her, and yet the Princess did not for a moment flatter herself with the idea that he was in love with her, though it did not take her long to decide that he certainly loved someone
History of present illness
One month before his admission,the patient developed persistent abdominal pain without obvious incentives,such as tolerable dull pain on the left side,without abdominal distension,lethargy,cold sensitivity,itchy skin,and change in skin color,among other symptoms.Since the start of the symptoms,the patient had poor appetite and spirit,and lost more than 10 kg weight.
History of past illness
Imaging is an indispensable auxiliary diagnostic tool for PADLBCL,and the commonly used clinical examinations include CT and magnetic resonance imaging(MRI)[10].In particular,in CT PADLBCL usually manifests as a low-density adrenal mass,which is moderately enhanced during enhanced scanning,revealing necrosis.In contrast,MRI examination shows a T1 phase low signal and T2 phase high signal.The T1 phase low signal can be distinguished from the T1 phase high signal caused by the hemorrhage of adrenal sarcoma.Besides,FDG-PET is more accurate in evaluating tumors and involved parts for determining extra-adrenal lesions[11,12].In this case,only a CT examination was performed.However,it is deemed necessary to perform FDG-PET examinations in all PADLBCL cases.Moreover,histopathological examination are required for final diagnosis.
Personal and family history
Routine blood tests,liver and kidney function test,blood coagulation function test,hormone-related examination,and tumor marker analysis showed no obvious abnormalities.In addition,the level of serum potassium was normal.
Physical examination
Anyone but Prince Vivien would have been terrified by such an uncanny sight, but he strode stoutly49 forward till he reached the second gate, which was opened to him by sixty black slaves covered from head to foot in long mantles50
Laboratory examinations
There was no history of hereditary diseases.No family members had similar symptoms.
Imaging examinations
PADLBCL is a rare disease.To date,only more than 100 cases have been reported in the PubMed database[2].PADLBCL mainly affects middle-aged and elderly men,with an average age of more than 60 years,and a male-to-female sex ratio of 2.93:1.In addition,the bilateral involvement of adrenal glands is common[3].At present,the etiology and pathogenesis of PADLBCL remain unclear and have been suggested to be related to autoimmune deficiency,HIV,or EBV infections[4].There are two viewpoints regarding the pathogenesis of PADLBCL.First,it may be related to the genetic predisposition of patients,such as mutations in the p53 and c-kit encoding genes as reported in adrenal lymphomas[5].The second view suggests the initial occurrence of lymphoma outside the adrenal glands followed by their subsequent affliction,with chemokines and microRNAs driving this process,which can explain the bilateral involvement of the adrenal glands[6].
FINAL DIAGNOSIS
The patient was diagnosed with non-GCB primary adrenal diffuse large B-cell lymphoma.
TREATMENT
We performed a left adrenalectomy under laparoscopic surgery.During the surgery,an irregular mass was observed in the left adrenal area.The mass was strongly adhered to the upper pole of the left kidney,and it pressurized the left kidney in forward and downward direction.No detectable lymph node enlargement was observed.The upper pole of the left kidney was damaged during the laparoscopic separation of the mass,so the wound surface was sutured continuously with 3-0 absorbable suture.After the separation of the tumor from the upper pole of the left kidney,due to excessive blood on the wound surface and compromised visibility,the tumor vessels were perturbed during the operation leading to the rupture of associated blood vessels.Due to the excessive blood loss,the laparoscopic surgery was reallocated to open abdominal surgery.The intraoperative blood loss was approximately 1300 mL,and blood transfusion was prescribed to overcome the loss.
OUTCOME AND FOLLOW-UP
Pathological diagnosis identified the presence of non-GCB diffuse large B-cell lymphoma in the left adrenal gland.Light microscopy observation revealed diffuse infiltration and growth of tumor cells in normal adrenal tissues.Tumor cells were composed of medium to large lymphoid cells.Most cells were round or oval in shape,double chromotropic or basophilic,containing less cytoplasm and larger nuclei(Figure 2A and B).Immunohistochemical analysis revealed tumor cells to be CD19 (+),CD20 (+),PAX-5 (+),CD79a (+),Ki67 (70%),CD43 (+),MUM1 (+),bcl-6 (+),CD45RO(focus+),CD3 (scattered+),cyclinD1 (-),CD10 (-),and CD30 (-) (Figure 2C and D).After the pathological diagnosis was confirmed,the patient was immediately notified telephonically.However,due to the patient's personal reasons,the return visit was delayed,and the patient returned to the hospital for further treatment a month later.Re-examination of the patient with abdominal enhanced CT 1 mo after the surgery revealed multiple soft tissue shadows in the retroperitoneum on both sides,uneven enhancement,and a left retroperitoneal soft tissue mass protruding into the kidney(Figure 3).Subsequently,the patient underwent four immunochemotherapy sessions at the hematology department of our hospital.The immunochemotherapy regimen was R-CHOP (rituxan 600 mg d1;cyclophosphamide 1.2 g d1;liposomal adriamycin 40 mg d1;vincristine 4 mg d1;and prednisone acetate 100 mg d1-d5).During fourth immunochemotherapy session,the patient developed a severe pulmonary infection,and sputum culture suggested infection by fungi and multidrug-resistant bacteria.The patient coughed sputum,and his body temperature fluctuated between 37 and 38 °C,and therefore,he was treated with sensitive antibiotics.Chest CT indicated diffuse patchy fuzzy shadows in both lungs,indicating inflammation.Hematologists did not rule out lung damage caused by immunochemotherapy drugs,and symptomatic treatment was continued.On January 22,2019,the patient was required to receive 9 L/min oxygen by mask,with his oxygen saturation being 85%.Re-examination of the chest CT revealed further aggravation of the infection.Antibiotic treatment and oxygen therapy were strengthened further,with the oxygen saturation of the patient reaching 92%.Subsequent treatment continued according to patient’s symptoms.However,at 03:37 on January 27,2019,his oxygen saturation dropped to 60%.His oxygen saturation could not be monitored further,his heart rate decreased gradually,and his both pupils were dilated.The patient was declared dead and the cause of his death was determined as respiratory failure.
17. Three: The number and/or pattern of three often appears in fairy tales to provide rhythm and suspense. The manikin assists the daughter three times over three nights and then later gives her three days to discover his name. The pattern adds drama and suspense while making the story easy to remember and follow. The third event often signals a change and/or ending for the listener/reader.


DISCUSSION
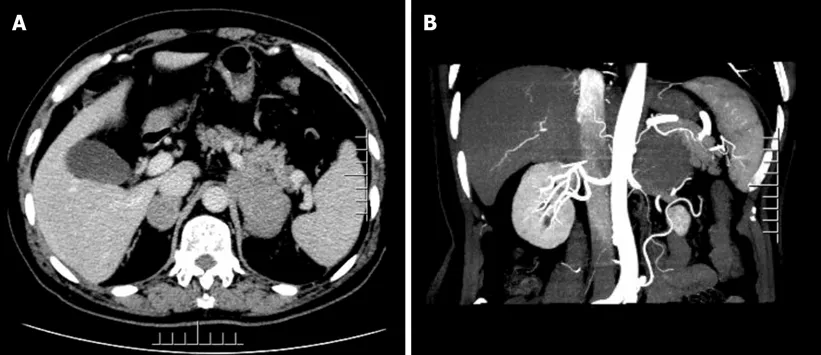
The adrenal enhancement computed tomography (CT) scan showed the presence of irregular masses in the adrenal glands on both sides,with the larger one being located on the left side.Its size was approximately 8.0 cm × 4.3 cm,its border was irregular,and the surrounding tissues were compressed.We did not observe any obvious enhancement in the arterial phase,nor any obvious swollen lymph nodes were noted later on (Figure 1).
The physical examination of the patient was unremarkable.
The clinical manifestations of PADLBCL lack specificity.Most patients experience pain around the waist and abdomen as the first symptom,accompanied by fatigue,fever,and night sweats[7].When the bilateral adrenal glands are involved,most patients can have symptoms of adrenal insufficiency,manifested as skin pigmentation,hypotension,and fever[8].In addition,PADLBCL involves the hypothalamic-pituitary axis,leading to adrenal insufficiency[9].Therefore,for PADLBCL with adrenal insufficiency,systematic endocrine assessment should be performed.As our patient had PADLBCL with normal adrenal cortex function,his case relied on imaging examinations,providing lesser diagnostic information from the clinical symptoms and signs.
The patient had no history of surgery,trauma,or other diseases.
Pathological examination remains the gold standard for the diagnosis of PADLBCL.More specifically,observation under a light microscope reveals the destruction of the adrenal tissue structure,often accompanied by large lamellar necrosis and diffuse infiltration of large lymphocytes.In addition,immunohistochemical analysis of cells often reveals the expression of the CD19,CD20,CD22,CD45,CA79a,and PAX5 markers,and sometimes the expression of CD10 and CD5 proteins.In particular,CD5+lymphomas are more malignant and associated with a poor prognosis[13].Immunohistochemistry can also be used to classify the molecular types of PADLBCL.For this purpose,Hans algorithm is most extensively used in routine practice,and it consists of three markers (CD10,Bcl6,MUM1).Based on the combination of these three markers,Hans algorithm could divide DLBCL into two groups (GCB and non-GCB subtype)[14].Non-GCB type PADLBCL is clinically common and often related to poor prognosis[15].In recent years,studies have reported that non-GCB patients are often characterized by a higher expression of the proliferation index (Ki-67),with standard R-CHOP immunochemotherapy regimen being less effective in such patients[16].However,other studies have reported that R-CHOP immunochemotherapy may achieve complete remission of PADLBCL[8].
Many people thanked Amy for being brave enough to speak up. Others encouraged her to ignore teasing and to carry her head high. Lynn, a sixth-grader from Texas, sent this message:
Combining the medical history of the patient,imaging,pathological morphology,and immunophenotype facilitates the correct diagnosis of PADLBCL;however,attention should be paid to exclude the following possibilities:(1) Secondary lymphoma,that is,that no other lymphomas existed before diagnosis;and (2) Other adrenal tumors including adrenocortical carcinoma,pheochromocytoma,malignant melanoma,and neuroendocrine tumors.Early diagnosis of PADLBCL is generally difficult until the tumor has grown substantially and compresses the peripheral nerves or organs,causing corresponding symptoms or damage to the adrenal tissue and adrenal insufficiency.
That went on for several years and each year, the guy would get a different girl to pose as his romantic interest. So whenever the ex-girlfriend came to visit him, she would be led into believing that it was all over between her and the guy.
Currently,there is no unified treatment regimen for PADLBCL.Most of the therapeutic strategies are developed based on the summary and comparison of the treatment experiences of lymphoma.PADLBCL is usually treated as a systemic disease,and early diagnosis and treatment can significantly prolong the patient’s survival.Since lymphoma is a systemic disease,the invasiveness of PADLBCL is generally extends beyond the visual limit,and it is difficult to achieve complete resection.Therefore,surgery is mainly used to diagnose the disease,and further immunochemotherapy is recommended post-surgery.R-CHOP immunochemotherapy is generally recommended as the first choice,and rituximab combined with second-line chemotherapy,such as bendamustine,DAEPOCH,DHAP,GDP,and GEMOX,is recommended for patients with relapsed/refractory PADLBCL.Patients with relapsed/refractory PADLBCL are known to exhibit a generally rapid progress of the disease and cannot tolerate chemotherapy drugs[17].
As mentioned,PADLBCL has a poor prognosis,Kim[18] reported 31 cases of primary adrenal DLBCL with overall 2-year and progression-free survival rates of 68.3% and 51.1%,respectively.A few reports have reported that patients with PADLBCL receiving R-CHOP immunochemotherapy have a better prognosis and can achieve long-term remission or even complete remission[8,19].It has also been reported that the treatment of surgery,chemotherapy,and autologous peripheral blood stem cell transplantation could retain a patient in remission for 2 years[20].Many factors,such as the IPI score,non-GCB type,pathological type,treatment of the patient abandonment,and non-standard treatment can affect the prognosis of patients.In addition,adrenal lymphoma is one of the major risk factors for the recurrence of central nervous system (CNS) lymphoma[21].In the study by Kim[18]13% of patients with adrenal lymphoma had CNS lymphoma recurrence.Therefore,systemic methotrexate or intrathecal injection of methotrexate may be administered during the treatment to prevent the involvement and recurrence of the central nervous system.
In this case,preoperative examination indicated normal adrenal cortex function,which impeded the preliminary diagnosis of PADLBCL by the physician-in-charge.Postoperative pathology indicated non-GCB PADLBCL,and the patient received RCHOP immunochemotherapy;however,the effect of immunochemotherapy was not beneficial.Possibly,the age of the patient and the impact of the disease and chemotherapy resulted in impaired immune response,leading to the patient acquiring severe lung infection and dying of respiratory failure.
CONCLUSION
The incidence of PADLBCL is low,and clinical symptoms are not typical.It is necessary to improve CT and FDG-PET examinations used for the evaluation of tumor staging,which would be helpful in standardizing treatment.Conventional immunochemotherapy includes the R-CHOP regimen,and surgery is mainly used to diagnose the disease,while the prevention of central nervous system lymphoma also needs to be considered.Thus,the ideal treatment plan needs to be strategized based on further research.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- New trends in treatment of muscle fatigue throughout rehabilitation of elderlies with motor neuron diseases
- What emotion dimensions can affect working memory performance in healthy adults? A review
- Quadrilateral plate fractures of the acetabulum:Classification,approach,implant therapy and related research progress
- Methylprednisolone accelerate chest computed tomography absorption in COVID-19:A three-centered retrospective case control study from China
- Analysis of photostimulable phosphor image plate artifacts and their prevalence
- N6-methyladenine-modified DNA was decreased in Alzheimer’s disease patients