
Quadrilateral plate fractures of the acetabulum:Classification,approach,implant therapy and related research progress
2022-01-24 09:24XueFengZhouSiChaoGuWanBoZhuJiaZhaoYangLeiXuShiYuanFang
World Journal of Clinical Cases 2022年2期
INTRODUCTION
The incidence rate of acetabular fractures is increasing year by year with the development of the society and the gradual increase of high-energy injuries caused by traffic and construction accidents and low-energy injuries in elderly patients with osteoporosis[1].The therapy of acetabular fractures has been subject to essential changes over the past 60 years,and it has always been a great challenge for orthopedists due to the complexity.Until the early 1960s,most acetabular fractures were treated conservatively.In 1964,the principle of acetabular operation was first described by Robert Judet and Emile Letournel,which brought revolutionary changes to the therapy of the injury[2].To alleviate pain and early mobilization,improve functions,reduce the risk of post traumatic arthritis,,open reduction and internal fixation (ORIF) has been gradually recognized as the gold standard for the therapy of displaced acetabular fractures[3,4].Letournel-Judet classification is clinically one of the most widely applied classifications of acetabular fractures.Acetabular fractures are divided into 10 types according to the acetabular both-column theory,including 5 types of simple fractures and 5 types of complex fractures[3].Through careful research,it's found that one of the concerns is that except simple fractures of the anterior or posterior wall,an important anatomical structure may be involved in the other 8 types of acetabular fractures,which is called the quadrilateral plate (QP).QP is located on the inner surface of the acetabulum,where the position is deep,and the bone quality is thin,and it is adjacent to a large number of peripheral nerves and blood vessels.Central dislocation of femoral head,acetabular fornix impingement and incarceration,as well as highly comminuted fractures are common in this area in case of high-energy trauma[5].Therefore,operative exposure and operations are even more difficult than those of common acetabular fractures,which leads to some controversy about open reduction and fixation strategies of acetabular fractures involving QP,serving as the hotspot of research and discussion[6,7].
Currently,there is still no consensus on the therapy of QP fractures of the acetabulum,nor is there a systematic and determinative guideline.However,the key to the successful therapy of QP fractures of the acetabulum is to apply fracture classification methods with clinical guiding significance,appropriate operative approaches,appropriate implants and internal fixation methods.In recent years,the classification system regarding QP fractures has been gradually involved in the literature,filling some deficiencies of Letournel-Judet classification.In addition,various operative approaches and new implants for internal fixation targeting at QP fractures have been proposed in more and more reports,showing different styles and unique advantages.At the same time,new requirements have been put forward in terms of the effect,prognosis and development of various implant internal fixation techniques.The purpose of this paper is to summarize the definition,classification,operative approaches,implant internal fixation methods and related research progress of QP fractures of the acetabulum,and put forward some personal opinions,so as to provide some reference and help for clinical orthopedists in the treatment of QP fractures,and provide clues and guidance for clinical research in the future.
DEFINITION AND CLASSIFICATION
QP fractures of the acetabulum are quite challenging in acetabular fractures,which is mainly caused by the lack of a unified or clear definition,and different authors have different understandings and definitions of QP fractures of the acetabulum.White[8] believed that QP fractures of the acetabulum are any acetabular fractures with medial subluxation of femoral head.However,by means of clinical case observation,it can be found that acetabular fractures combined with central dislocation of the hip joint are not necessarily accompanied with QP fractures,and QP fractures are not necessarily associated with central dislocation of the hip joint.Sen[7] interpreted QP fractures as comminuted fractures on the quadrilateral surface of the medial acetabulum,and introduced the technique of QP fracture therapy by buttress plate.QP is located on the medial surface of the acetabular fossa and is a quadrilateral area connecting the anterior and posterior columns of the acetabulum.Therefore,it is still controversial whether QP belongs to the anterior column or the posterior column.A more reasonable view is that QP is an accessory structure of the acetabulum,but some scholars have classified it as the third column separately[9].Farid[10] proposed another interpretation,noting that QP can be separated from the anterior column or the posterior column,either completely or incompletely.In a word,there is still no unified definition and no adequate guidelines in the existing literature,so there is considerable controversy about how to treat with this type of fractures.Some orthopedists suggest to apply specialized approaches or specific fixation methods,while others believe that the reduction of QP fractures mainly depends on the reduction of acetabular columns and QP fractures are independent of the hip stability or the development of post traumatic arthritis[11].
QP refers to the relatively flat surface of the true pelvis,which is located on the medial acetabulum and is often involved in acetabular fractures[11],but it is not taken as a separate parameter in most classification systems.In clinical practice,Judet-Letournel classification is still the most widely used classification of acetabular fractures,but both the Judet-Letournel classification and the AO classification are marked by column and wall injuries,with less consideration of QP.QP is not taken as an independent parameter,and there is a lack of unified quantitative indicators.Hirvensalo reported that QP fractures were always associated with acetabular fractures of the same type.However,in recent years,there have been simple QP fractures that cannot be summarized by the existing fracture classification systems among the cases reported by Laflamme[12],indicating that the current classification methods fail to evaluate the severity of QP fractures in an accurate and effective manner.
Prasartritha[13] suggested to include QP in the classification after reviewing the three-dimensional (3D) CT images of the medial surfaces of 84 acetabular fractures in research,and believed that complex acetabular fractures can be classified by the classification of the QP.
Then Grannonia knelt down before the fox, and begged him in her sweetest way to catch the birds for her and procure30 their blood, promising31 at the same time to reward him richly
Einahal[11] proposed the definition of QP fractures and conducted classification by analyzing the anatomical and radiological features of QP in research.In the research,it was pointed out that QP fractures are generally simple fractures or comminuted fractures and can be separated from the anterior and posterior columns of the acetabulum completely or incompletely,and QP fractures of the acetabulum were accordingly divided into 4 types.Based on this,the definition and classification system of the QP fractures of the acetabulum in Cairo University Hospital (CUH) was put forward,which is the first classification system proposed for QP fractures of the acetabulum.
Those would have been my thoughts, yet Annie Mae had other thoughts -- thoughts the world could truly use. She sacrificed. She struggled. And finally, when the beds were truly hers, she let her sons, Paul and John, sleep in them. She was a living example of absolute honesty, the honesty that should characterize all who claim to be Christian.
What is noteworthy is that in a study involving 32 patients with acetabular fractures,Wu[19] introduced a QP anterior dynamic plate-screw system with "QP screws" in the treatment of complex acetabular fractures involving QP through a single ilioinguinal approach,achieving the same result by different methods from the CUH support screw technique proposed by Karim[38] mentioned above,and its safety and effectiveness were validated.During operation,the femoral head and QP fractures medially dislocated are first reduced by instruments or operations,and then the straight reconstruction plate is pre-bent into an S-shape or C-shape and placed along the edge of pelvis passing through the pubic region,the upper edge of QP and the iliac region.After that,they are not firmly fixed on the bone surface,but can be pressed on the bone surface during screwing with special equipment.The screw placement order should follow certain rules.First,the screws are fixed in the iliac region and pubic region to stabilize the acetabular anterior column.Then,QP screws are successively placed in the middle of the QP surface using a special method.QP screws are inserted along the edge of pelvis parallel to the QP surface,and they penetrate into the bone by only 1/3-1/2 of transverse diameter to avoid entering the joint cavity.During screwing,strong clamping force can be provided by the torsion and elastic recoil of the plate for QP screws.

OPERATIVE APPROACH
In general,QP fractures will cause medial displacement of the femoral head,or central dislocation in severe cases,resulting in protrusion of the femoral head into the pelvic cavity.If the femoral head is incarcerated,reduction is difficult to be realized by traction.It is of vital importance to reconstruct the anatomical structure of the acetabulum and femoral head,and the center of rotation of the femoral head should coincide with that of the acetabulum for normal anatomical structure.Moreover,after reduction and fixation of the QP fractures,the QP needs to counteract the inward and upward force of the femoral head.However,due to the special bone morphology,the special position and anatomical structure of the QP,the reduction and fixation of the QP fractures have always been the difficulties in trauma orthopedic operations[15].
The selection of operative approaches is very important in operative treatment,which is mainly performed pursuant to the type of QP fractures.When the QP fracture fragment is connected to the anterior column,the anterior approach can be applied,and reduction and fixation can be conducted through the screw-plate system and the anterior column.When the QP fracture fragment is connected to the posterior column,the Magic screws or posterior column screws can be used for reduction and fixation in case of available closed reduction,or screw plate can be used for fixation.For floating and comminuted fractures,an anterior and posterior combined approach can be applied for reduction and fixation[15].
To be specific,it is best to expose posterior fractures (posterior column,posterior column/posterior wall),transverse fractures involving the posterior wall,and specific transverse and T-shaped fractures by traditional posterior approaches.In these cases,ischiatic notch palpation can be employed to evaluate the fracture lines across the QP[16].
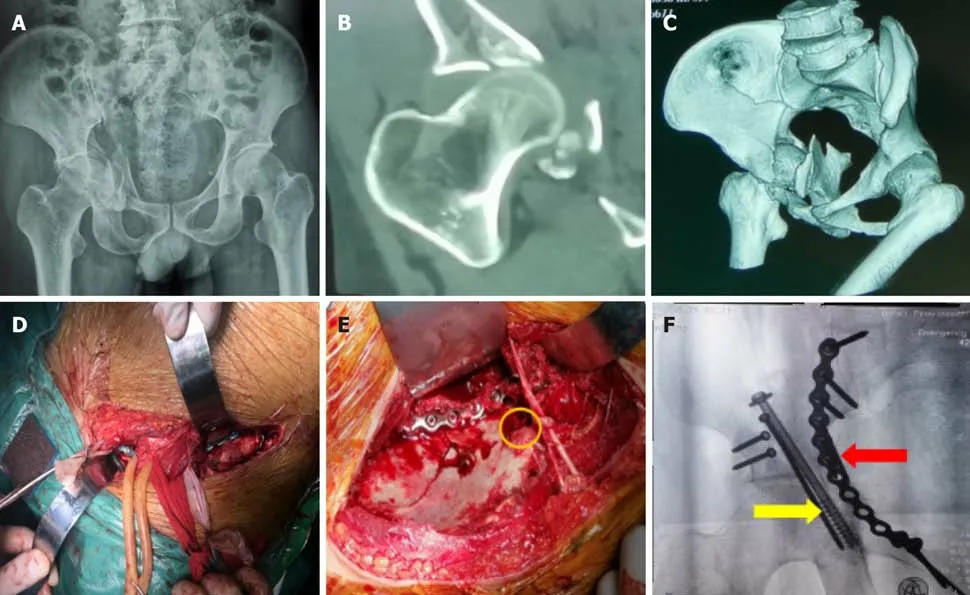
Other types,such as anterior column fractures,anterior wall fractures,anterior column and posterior half transverse fractures,combined both-column fractures and partial T-shaped fractures,can be well exposed by the ilioinguinal approach.In traditional ilioinguinal approaches,QP can be exposed directly through the medial window after the separation of the external iliac vessels and their related lymphatic vessels.Through the retrospective analysis of 13 patients with acetabular fractures involving QP,Peter[17,18] believed that classic exposure by the ilioinguinal approach is still the preferred method for the therapy of anteromedial displaced fractures of the acetabulum,which controls the displacement and comminution of the medial area and the QP surface of the acetabulum with the help of the buttress plate.Wu[19]applied the QP anterior dynamic plate-screw system developed by his/her team on 32 patients with acetabular fractures by the unilateral ilioinguinal approach,and verified the safety and effectiveness of the unilateral ilioinguinal approach for the therapy of complex acetabular fractures involving QP.Tosounidis[20] reported the mid-term efficacy of 30 cases whose acetabular fractures involving QP were reconstructed with the buttress plate/steel spring plate by the ilioinguinal approach.The results showed that the reconstruction of QP fractures of the acetabulum with the buttress platethe ilioinguinal approach is an effective method for fixation(Figure 2).
I will send an abundance of gifts, and a string of camels laden36 with flashing stones and rubies37 of Badakhsham In this way I will bring her and her suite38, and I will give her to you to be your solace39
Zhang[44] proposed a kind of novel QP anatomical plate in the treatment of displaced acetabular fractures involving QP,trying to solve the problem of difficulty in obtaining satisfactory fixation effect using conventional reconstruction plates.A total of 26 patients with QP fractures underwent QP anatomical plate fixation through the Stoppa approach.It was found by postoperative X-ray and CT scan that anatomical reduction and good reduction rates are 88.46% and 11.54%,respectively.No screw loosening is observed after operation,and all fractures are healed well.The Merled'Aubigné score is satisfactory at the end of more than 2 years of follow-up.
As an alternative method to the medial window of the traditional ilioinguinal approach,the modified Stoppa approach has been described and used by many surgeons subsequently[23-27].With obvious value,80% of the QP can be displayed directly,and the application of subpubic fixation is relatively easy by this method[28].The modified Stoppa approach can be used alone,or in combination with the transverse medial window of the ilioinguinal approach,or in combination with the subilioinguinal approach[7,26].Its overall advantage is that the joint fractures can be released and reduced by virtue of the open fracture lines across the surface of the QP[29].In the retrospective analysis by Andrés-Peiró[30],16 cases with acetabular fractures involving QP were treated by the anterior modified Rives-Stoppa approach,and the results showed that the Stoppa approach is an effective and recommendable method,which has the advantages of easy,extensive and safe exposure and can control the fractures involving QP during operation in a bid to achieve anatomical reduction and stable fixation.
Peter[17] first supported the bent 7-10-hole 3.5 mm reconstruction plate at the medial QP through the anterior approach and then fixed it on the iliac ala of 13 patients with acetabular fractures involving QP,and then placed another reconstruction plate on the upper edge of the arcuate line to increase the mechanical stability of QP fixation.Some scholars used special-shaped blade plates to increase their contact area with QP,further raising the stability of QP fracture fixation.Sen[7]retrospectively analyzed the data of patients with comminuted fractures involving iliopubic eminence,QP and anterior column.The surgical technique included rightangle fixation of the spring plate (Allis T-type plate) and the subpubic support plate,and the vertical part of the T-type plate was fixed on the iliopubic eminence,while its horizontal part supported the QP.This technique is a little similar to that of Peter,but it solves the possible concurrent fracture at the iliopubic eminence,and also increases the contact area of the plate with the QP,thereby improving the mechanical stability of internal fixation.
The implant internal fixation techniques mainly include the classic reconstruction plate technique with a medial support effect,and the subpubic buttress plate technique[7,42].Kistler[6] applied hook-shaped reconstruction titanium plate combined with arc-shaped titanium plate vertical crossing internal fixation in the treatment of acetabular anterior column and QP fractures,and the curative effect is good,proving that QP reconstruction with buttress plate through the ilioinguinal approach remains an effective fixation method for acetabular QP fracture surgery.Qureshi[36] proposed that the subpubic plate technique is suitable for patients with moderate displacement of the femoral head and QP entering the true pelvis,and also for periprosthetic fracture patients with well-fixed acetabular structure but moderate displacement to the true pelvis.Subpubic plates placed on a plane parallel or perpendicular to the displacement plane provide strong fixation for QP fractures,which significantly prevent secondary displacement fractures of the acetabulum.In a 10-year early observation,450 cases have no reduction and fixation loss.Laflamme[43] used subpubic plates through the modified Stoppa approach in the treatment of 21 elderly patients with displaced QP fracture in a retrospective study,and the curative effect is satisfactory among 70% of the patients.It can be seen that proper surgical treatment with appropriate internal fixation techniques can still obtain satisfactory effects on elderly patients with osteoporosis,and the location of femoral head and acetabular top in the same center of rotation is highly important for the prognostic function.

In addition,with the promotion of minimal invasion concepts and the development of endoscopic techniques,orthopedists have started to explore the feasibility and effectiveness of pelvic or acetabular operation under the endoscope.In the anatomical research,Trulson[35] established complete pelvic rings on 4 cadavers endoscopically and carried out internal fixation with steel plates along the iliopectineal line from the public symphysis to the iliosacral joint,covering QP and ischiadic nerve,which verified the feasibility of fully endoscopic exposure of the pelvic brim and QP with the existing standard laparoscopic instruments.In addition,the internal fixation
with steel plates can be performed under the endoscope.However,it's believed that further research on reduction techniques is necessary when this technique is planned for clinical application.
IMPLANT INTERNAL FIXATION TECHNIQUE
There are many optional internal fixation devices,but the joint has a risk to be penetrated by the implant due to the deep location and thin texture of QP[36].Severe comminution,osteoporosis and delayed fixation will cause additional technical difficulties during fixation.
Kirschner wire and screw fixation
Okelberry used screws and Kirschner wires in QP fixation in 1956 for the first time.He fixed one screw on the posterior medial acetabulum through the iliofemoral approach.Multiple screws or Kirschner wires may be needed in the case of severely comminuted fractures,but it is often difficult to achieve complete reduction or maintain better reduction.Larson[37] reported that the curative effect is satisfactory among 66% of the 6 patients,and proposed that the ability to maintain the comminuted fracture fragments is the key to the success of screw fixation.A variety of supplementary screws have been applied to strengthen traditional posterior column screws.In particular,Judet and Letournel described an additional screw channel for posterior column fixation,which extended through the edge of pelvis at the iliopubic eminence or lay in the middle of QP.The clinical effectiveness of these screw fixation techniques has been verified by Karim[38] in a recent study.
Starr[39] reported many surgical techniques in the treatment of acetabular fractures with percutaneous screws,and proposed that Magic percutaneous screws can be applied in QP fracture fixation,but there were no related cases reported.According to their report,Magic screws can be used to treat simple QP transverse fractures,but it is difficult to use percutaneous screws for reduction and fixation in the case of comminuted and floating QP medially displaced fractures.Mouhsine[40]used percutaneous screws in the treatment of 18 elderly patients with transverse,"T"-shaped and double-column micro-displaced fractures.The efficacy is satisfactory in 17 cases,no complications occur,and the fractures are healed without secondary displacement and screw failure.With the advancement of 3D navigation techniques,Ruan[41] applied them in the treatment of acetabular fractures accompanied by QP fractures.The efficacy is satisfactory and no postoperative complications occur.However,it is generally believed that there may be technical difficulties of screw fixation or insufficient fixation effect in the case of severely comminuted fractures and osteoporosis.
Screw-plate system internal fixation
Just then the laughing and shouting of drunken soldiers could be heard coming down the road. Carl Meier fled. With no time to summon her father, Albertha scrabbled in the dirt with her bare hands, scooped19 up the bulbs from their hiding place, and reburied them in the rubble next door.
What's more,there are the classic Kocher-Langenbeck approach and the anterior and posterior combined approach.All the above approaches,especially the anterior approaches,possess their respective advantages and limitations,as well as corresponding indications and contraindications (as shown in Table 1).No matter what approach is applied,it should be selected flexibly based on the actual fracture conditions of the patient and the degree of familiarity of the surgeon with the operative approach.
Recently,Karim[38] proposed a new implant fixation technique for acetabular QP fixation,which is called the CUH support screw technique.This technique involves the anterior column fracture reduction and reconstruction plate fixation (3.5 mm or 4.5 mm),in which the plate needs to be carefully placed on the edge of pelvis,and must be partially extended inward into the true pelvis (a key step for the success of this support screw technique),followed by QP reduction.QP can be reduced temporarily by pelvic reduction forceps,after which two or three screws are inserted through the plate to keep the QP fracture fragments in place by their friction force on the inner surface of QP.The number of screws can be increased based on the degree of QP comminution when this technique is used,and the direction of screws can also be adjusted according to the position of QP fracture fragments,so that the plate and screws can support the fracture as a separate unit.After the screws are tightened for the first time,screw loosening may occur due to reduction of fracture fragments,so the screw must be tightened again in place finally,forming a three-point fixation between the plate and the bone.One of the advantages of this technique is that it needs no special methods or additional time-consuming steps in the reduction and fixation of QP fractures.In addition,as a new general technique,it can be effectively applied to various anterior approaches.Other advantages are as follows:It can avoid the risk of joint penetration and is suitable for severely comminuted QP fractures difficult to keep reduction.Its disadvantage is that the plate must be correctly positioned on the edge of pelvis and partially extended inward into the true pelvis,so as to insert the appropriate screws.
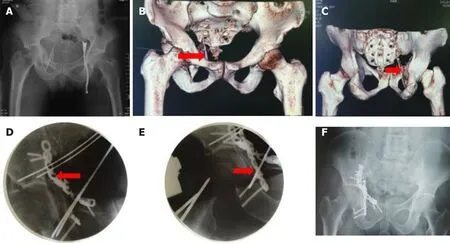
Yang[14] introduced the pelvic 3D CT images of 238 cases with QP fractures into computer software for pelvic modeling,and divided the line from the ischial spine to the iliopubic eminence in the QP into two parts.In the research,the fracture line involving the posterior half of the QP was Type A fracture,the fracture line involving the anterior half was Type B fracture,and the fracture lines involving both the posterior and anterior half of the QP were Type C fractures.Then,the frequency distribution image was obtained by the density distribution of the fracture lines.Finally,the Type A,Type B and Type C fractures accounted for 25%,10% and 65% respectively according to statistics.At present,although none of the research can influence the status of Judet-Letournel classification,it supplements some deficiencies of Judet-Letournel classification to a certain extent,and advances clinical orthopedists to deepen understandings of QP fractures,so as to help them choose more appropriate operative approaches,fixation methods and implants(Figure 1).
If the peri-king allows this favour, we two will manage to be your anointers, and we will put an oil on you such that if you were a thousand years in the fire not a trace of burning would remain
However,in clinical practice,orthopedists always find it difficult to expose and reduce the anterior wall fractures of the acetabulum with transverse or longitudinal secondary fracture lines by the ilioinguinal approach,and the QP of the medial wall of the acetabulum cannot be exposed and reduced under direct vision.In addition,due to the limitation of the inguinal ligament,the anterior hip joint capsule and hip joint cannot be exposedthe ilioinguinal approach.To change the limitation of the ilioinguinal approach to the anterior exposure of the acetabulum,in April 2008,Farid[21]took the lead to report satisfactory efficacy in the therapy of 7 cases with acetabular fractures by the sub-ilioinguinal approach.According to the research about operative treatment of 34 patients with acetabular fractures,Qin[22] discussed the clinical efficacy of the therapy of acetabular fractures involving the anterior and medial walls and combined femoral neck fractures by the modified anterior sub-ilioinguinal approach without iliac osteotomy.He/she believed that the modified sub-ilioinguinal approach can maintain the integrity of the inguinal ligament and broaden the horizons of the anterior and medial walls of the acetabulum (including QP),and the anterior hip joint capsule,and the modified ilioinguinal approach was the good modification and supplement to the classic ilioinguinal approach.
In recent years,the pararectus approach has been referred to as the alternative approach to the ilioinguinal approach and the modified Stoppa approach,which supports visualization of true and false pelvic surfaces (including the QP)a single approach lateral to the rectus abdominis[31,32].Mardian[33] demonstrated that the pararectus approach presents better reduction of the acetabular fracture interspace than the classic ilioinguinal approach,but beyond that,there is little data on the effectiveness and safety of this approach.In the retrospective analysis,Xia[34] analyzed the data of 15 patients with acetabular both-column fractures combined with QP displacement treated with the pararectus lateral incision approach,and believed that the pararectus lateral incision approach can fully expose,reduce and fix the acetabular both-column fractures combined with QP fracture displacement with good efficacy.
However, whites did not do that with African Americans in the South in those days, and I conformed to the local practice -- though it conflicted with my Christian beliefs
Gillespie[45] reported that pelvic internal plate combined with pelvic external plate has a significantly better fixation effect than pelvic external plate alone in the treatment of acetabular fractures involving QP.The results showed that additional pelvic internal plate may have an apparent advantage in preventing catastrophic internal fixation failure.
Wang[46] compared the fixation effects among 4 different implants (subpubic reconstruction plate internal fixation,subpubic locking reconstruction plate internal fixation,anterior column reconstruction plate combined with QP screw internal fixation,and anterior column reconstruction plate combined with posterior column lag screw internal fixation) in a biomechanical study.The results of biomechanical measurement showed that anterior column reconstruction plate combined with posterior column lag screw internal fixation has the best stability in the treatment of acetabular QP fractures,followed by anterior column reconstruction plate combined with QP screw internal fixation.The above two methods are superior to subpubic locking reconstruction plate and reconstruction plate internal fixation.Moreover,these four fixation methods are all reliable.
In terms of the surgical approach,there are mainly three methods of steel plate internal fixation:QP fixation from the anterior approach along the arcuate line through the anterior column (or QP fixation from the anterior approach by buttress plate fixing the posterior column),fixation from the posterior approach through the posterior column,and anterior-posterior fixation[15].
In recent years,the use of titanium plate screws for direct QP fixation has been explored by some scholars,mainly including medial ilioischiatic plate[47] and subpelvic plate.The idea of direct fixation methods is to implant screws avoiding the region that cannot be implanted with screws in QP,in which the placement location of the plate and the implantation direction of the screw are special.The medial ilioischiatic is placed near the posterior boundary of QP,while the subpelvic plate is placed near the upper boundary of QP.Therefore,it is more difficult to directly fix QP fractures,especially those near the weak bone area.(Figure 3).
Wire cerclage technique
Wire cerclage combined with screw-plate fixation technique is more suitable for the fracture line between the greater sacrosciatic notch and the anterior inferior iliac spine.In related reports,there are more cases of high posterior column acetabular fracture and double-column acetabular fracture exposed through the ilioinguinal approach[48,49].Chen[49] adopted wire cerclage fixation combined with screw-plate system in the treatment of 35 cases of double-column fractures.Intertrochanteric osteotomy was performed through the radial approach,and 1-2 reconstruction plates and screws combined with wire cerclage fixation were used for treatment.As a result,the efficacy is satisfactory among all patients.Farid[10] used the steel spring plate to support the medial QP,and implanted two screws at the proximal end of the plate,while no screws were implanted at the distal end.Then the wire was passed through the hole on the plate,followed by cerclage.As a result,the effect is satisfactory in 5 cases.
A warm glow shone in her eyes as she revealed to me her fondness for Susan. But her expression turned pensive33 when she referred briefly34 to the girl s past. In a short time, I came to respect this generous-hearted woman who had opened her home to a young girl and attempted to make a difference in her life.
One day he saw that one of the golden apples was missing. He placed guards at all gates of the garden; but in spite of this, each morning on counting, he found one more apple gone. At length he set men on the wall to watch day and night, and these reported to him that every night there came flying into the garden a bird that shone like the moon, whose feathers were gold and its eyes like crystal, which perched on the apple tree, plucked a golden apple and flew away.
Titanium mesh technique
Some scholars used titanium mesh combined with reconstruction plate in the treatment of complex acetabular fractures accompanied by QP comminution,achieving good effects.This technique has the following advantages:(1) Titanium mesh can be used to directly reduce multiple QP fracture fragments,and the internal fixation has a reliable effect;and (2) Titanium mesh can effectively and indirectly reduce the anterior-posterior columns of the acetabulum.
Preoperative anatomical shaping technique
With the increasing maturity of 3D printing,the use of preoperative anatomical shaping plates has become more and more popular,because the preoperative anatomical shaping technique and a larger coverage area offer larger-area support to QP after reduction.Taller[50] reported the use of a new 3.5 mm "Omega" plate in 15 cases of QP fractures,among which 12 cases have good or satisfactory postoperative radiological examination results.This kind of pre-shaping technique based on the preoperative CT examination technique and 3D printing technique perfects the preoperative anatomical shaping effect of the plate according to the hemipelvic mirror image on the unaffected side.Such a technical feature can satisfy the anatomical characteristics of any individual,which can shorten the operation time,and improve the adhesion of the implant to the bone and the fixation strength.
However,this method has a high cost,and most medical institutions and patients suffer from practical economic problems,so the clinical use of preoperative anatomical shaping QP implants is restricted to a certain extent currently.Boni[51] proposed that stainless steel locking calcaneal plate can cover a similar surface area to that of preoperative anatomical shaping plate,but its cost is significantly lower than that of the preoperative anatomical shaping plate based on 3D printing and CTD techniques.
This was great sorrow to the little mermaid; she knew how much more sweetly she herself could sing once, and she thought, “Oh if he could only know that! I have given away my voice forever, to be with him
DISCUSSION
In the last few decades,QP has attracted increasingly more attention[52,53].However,scholars have different definitions of QP fractures,and there is still no systemic and effective classification for QP fractures yet.Therefore,some of the work is mentioned above to help better define QP,and some attempts made by many scholars on systemic classification of acetabular QP fractures in recent years are described.A good classification method should not only leave a clear impression to doctors in distinguishing different types of fractures,but also offer good guidance in the preoperative planning of such fractures.In addition,various methods for QP exposure and fixation have been developed.Despite many techniques for QP fracture fixation,none of them have been confirmed to be absolutely superior in clinical research.Reconstruction/elastic plate fixation remains the preferred internal fixation implant by most orthopedists in the surgical treatment of acetabular QP fractures currently,and its fixation strength and stability have also been basically recognized in related biomechanical studies.
It should be noted,however,that the screws placed parallel to the QP through the edge of pelvis originally described by Judet and Letournel have the same good or better performance in biomechanical studies than fixation strategies in all other tests[45,54-56].An interesting but inconclusive question is the extent to which QP needs to be resolved during fracture fixation.In the acetabular fracture classification system,Judet and Letournel did not clearly distinguish QP fractures,but recognized that the fracture line passing through QP is a common feature of many fracture types.Fixation of simple fracture lines passing through QP combined with columnar fracture fixation is sufficient to achieve overall stability of fractures.The specific indications to QP fixation remain unclear in the case of independent QP fragments.Based on our understanding of the importance of the acetabular dome,such fractures need no special fixation in the absence of medial subluxation or instability of the femoral head[57-60].This view is supported by previous studies on the non-surgical treatment outcome of acetabular fractures[37,61].There is no femoral head subluxation in medial acetabular fractures.After conservative treatment,the functional outcome is still good even though there are displaced medial fractures.In the case of incarceration on the medial surface of acetabulum,the independent fixation of QP may be necessary.Under these circumstances,the reduction and fixation of QP are helpful for containing the displacement of fragments.In addition,the reduction of independent QP fragments can enhance the quality of reduction of adjacent columnar fractures in some cases.Further research is needed to determine the situations in which QP fixation is necessary or beneficial,and to determine whether any single technique for stabilizing QP has relative clinical benefits.Finally,the optimal approach for QP is unclear yet.The advantages and disadvantages of the ilioinguinal approach,modified Stoppa approach and pararectus approach remain to be compared in further clinical research[16].However,we can conclude the quadrilateral plate fracture classification based on the distribution frequency map of the quadrilateral plate fracture line developed by Yang[14],and combine the advantages and limitations of various anterior surgical approaches to envision an approach selection strategy corresponding to the fracture classification in the quadrilateral plate (Table 2).However,further clinical cases need to be verified.
The dark gallery seemed darker than ever as he turned away, but he went back to the kitchen and inquired who slept in the room at the end of the passage. The scullery maid, they told him, whom everybody laughed at, and called ‘Donkey Skin;’ and though he perceived there was some strange mystery about this, he saw quite clearly there was nothing to be gained by asking any more questions. So he rode back to the palace, his head filled with the vision he had seen through the keyhole.

Although there is a lack of definite and unified standard for the classification,operative approach and implant internal fixation methods of QP fractures,we believe that an easy-to-understand classification scheme for QP fractures to guide surgical planning is worth popularizing in the future,just as Yang[14] classified the QP fractures by taking the line from the ischial spine to the iliopubic eminence as the boundary.At the same time,we can predict that the surgical approach with clear fracture exposure,convenient and reliable fixation and less trauma will be highly respected and readily adopted by surgeons,such as the iliac fossa approach assisted the minimally invasive small incision using the Stoppa approach.
It should be pointed out that most of the above-mentioned studies w ere retrospective analyses.In some studies,the sample size was insufficient,there was no random grouping,and the duration of follow-up was different.Therefore,prospective,randomized grouping,multi-center,large-sample,long-term follow-up studies are still needed to compare advantages and disadvantages of the above various surgical approaches and implant techniques.Previous literature retrieval did not cover many studies involving acetabular QP fractures,and the treatment of QP fractures was not the focus in most of these studies.Therefore,the uniqueness of this review is that it only aims at acetabular fractures involving QP,so it is highly targeted[14].
CONCLUSION
In conclusion,with the development and advancement of medical technology,orthopedists have gained an increasingly deep understanding of acetabular QP fractures,and great progress has been made in the treatment of acetabular QP fractures,but acetabular QP fractures are still a major problem in traumatic orthopedics.It is necessary to have a basic and unified definition of QP fractures.At the same time,a more systematic classification method for QP fractures will benefit the preoperative planning of clinicians and offer guidance to the selection of internal fixation implants.In addition,there are diverse surgical approaches and implant internal fixation techniques for acetabular QP fractures,and they have their own advantages and disadvantages.Orthopedists need to flexibly grasp indications and choose more suitable surgical techniques and implants in clinic based on their own proficiency in surgical procedures and techniques combined with clinical commonality and individual difference of patients,so as to achieve the best therapeutic effect.According to related research results,the mainstream methods for QP fracture fixation currently are relatively reliable implant fixation.Many new techniques have begun to emerge in acetabular fractures involving QP,and we have good reasons to believe that this kind of surgery will develop towards smaller surgical trauma,shorter operation time,and more accurate and reliable intraoperative auxiliary system.
5. Frog: Frogs symbolize20 new life in many cultures and thus often appear helpful or kind in folklore22. However, frogs also have connections with witchcraft23, often as witches familiars, and are despised by some religious groups for that reason (Philip 1997).
The authors would like to thank Dr.Wang XJ and Dr.Li L for advice on the discussion.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- New trends in treatment of muscle fatigue throughout rehabilitation of elderlies with motor neuron diseases
- What emotion dimensions can affect working memory performance in healthy adults? A review
- Methylprednisolone accelerate chest computed tomography absorption in COVID-19:A three-centered retrospective case control study from China
- Analysis of photostimulable phosphor image plate artifacts and their prevalence
- N6-methyladenine-modified DNA was decreased in Alzheimer’s disease patients
- Inflammation-related indicators to distinguish between gastric stromal tumors and leiomyomas:A retrospective study