
Using a fretsaw in treating chronic penial incarceration:A case report
2022-01-24 09:25YiZhaoXiaoQiangXueHouFengHuangYiXieZhiGangJiXinRongFan
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Penial incarceration (PI) is a rare clinical situation that was firstly reported in 1755[1].It is usually caused by a foreign object that strangulates at the base of the penis[2].PI may derive from pranks,sexual demand,mental disease,or intention to prohibit urinary disease[1].In most cases,the strangulating objects would block venous and arterial blood supply and result in ischemic necrosis.Hence,PI usually requires immediate intervention to save the penis function[1,3].Depending on the material and hardness,strangulating objects can be either metallic or non-metallic[4].Studies report that PI is usually caused by non-metallic foreign objects in younger patients,such as hair and rubber bands.In contrast,in elderly patients,metallic foreign objects are more likely to be found[5].
When I woke up that morning all I wanted to do was walk. It was winter my favorite season. This walk would change my life forever and I would remember for years to come. On that one special walk is where I meet the love of my life and lose my love. I remember it like it was yesterday.
Herein,we report a rare case of a patient with chronic PI for three months.The strangulation was treated by operation successfully,and the patient's penial function was not affected.Published approaches on evaluating and treating PI are reviewed,and our experience on this case is shared.
CASE PRESENTATION
Imaging examinations
No specific imaging examination was taken for diagnostic purposes as the diagnosis was not ambiguous.
Laboratory examinations
Nothing abnormal was shown in the laboratory examinations.
Albeit cases of penial strangulation and its treatments had been sporadically reported,there are no universal treating protocols due to the differences in patients'status,strangulating objects,and medical conditions.Various objects could induce the strangulation of the penis.Based on the material,they could be roughly classified as metallic and non-metallic[7].Trivedi[3] suggested that the duration of incarceration was an essential factor affecting the prognosis.Namely,suppose the penile strangulation cannot be relieved in time,it may lead to irreversible ischemic necrosis,gangrene of the penis,even penile self-amputation,urethral fistula,and penile erectile dysfunction.
Physical examination
Considering the familiarity with available equipment in the operating room,we also invited several scrubbing nurses for surgical instrument preparation.The fretsaw,which had been commonly used in the field of orthopedics and neurosurgery,was recommended.

A close physical examination found that the metallic hoop could be rotated slightly at the incarceration location.However,it could not be removed directly whatsoever.The patient's vital sign was stable.
“Now listen,” said the robber-girl; “all our men are gone away,— only mother is here, and here she will stay; but at noon she always drinks out of a great bottle, and afterwards sleeps for a little while; and then, I’ll do something for you.” Then she jumped out of bed, clasped her mother round the neck, and pulled her by the beard, crying, “My own little nanny goat, good morning.” Then her mother filliped her nose till it was quite red; yet she did it all for love.
Personal and family history
The patient had no markable personal and family history.
History of past illness
The patient reported multiple comorbidities,including diabetes,high blood pressure(up to 190/110 mmHg),and coronary heart disease with four stents implanted.The patient took aspirin and clopidogrel routinely for secondary prevention purposes.
History of present illness
We wrapped the distal penis with a bandage preoperatively to alleviate regional edema and placed a thin catheter between the penis and the hoop as a retraction.The catheter was pulled out intraoperatively,and then a condom was cautiously placed.Nevertheless,because of the edema of the prepuce,we failed to take the hoop off by hand,even with lubrication.
I just live for the day when I ll get a new startnd the dreams I still hold deep in my heart.I hope I can make it, I at least have to tryBecause I m heading toward6 death, and I don t want to die.
Chief complaints
So it was settled, and then the king bade one of his lords go to Don Giovanni and ask him when the wedding day was to be, so that the princess might make ready
MULTIDISCIPLINARY EXPERT CONSULTATION
Aspirin and clopidogrel had been ceased seven days before the operation.Both the cardiology department and anesthesia department regarded the risk to anesthesia as acceptable for surgery.Firefighters stated that they had no experience in handling such cases.
She promised42 her godmother she would not fail of leaving the ball before midnight; and then away she drives, scarce able to contain herself for joy. The King s son who was told that a great princess,43 whom nobody knew, was come, ran out to receive her; he gave her his hand as she alighted out of the coach, and led her into the ball, among all the company. There was immediately a profound silence,44 they left off dancing, and the violins ceased to play, so attentive31 was everyone to contemplate32 the singular beauties of the unknown new-comer. Nothing was then heard but a confused noise of:
Dentists suggested that the fixed dental drill might be an alternative,as they had previously tested its efficiency and feasibility on a stainless-steel nut.It could cut a 1 mm deep gap on the nut within 25 s,let alone the softer copper hoop in this case.However,since the head of the dental drill was easily destructed,this plan was eventually abandoned.
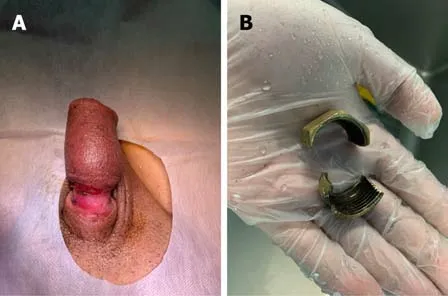
Physical examination demonstrated a swollen penis at the distal end of the metallic ring,no skin necrosis or numbness was reported,nor stinky odor was smelt.This copper hoop was 40 mm in the external diameter,with a 10 mm width and a 2 mm thickness (Figure 1).
FINAL DIAGNOSIS
The final diagnosis of the presented case is chronic PI with a metallic hoop.
A 73-year-old man visited the outpatient department of our hospital with a copper hoop strangulating around the base of his penis.
TREATMENT
The patient reported that he "accidentally" put the copper hoop in his penis three months ago,and it was challenging to be taken off.As there was no acute pain,bleeding,or any other uncomfortable symptoms at that moment,he decided to do the self-observation rather than visit the emergency department.During his observation period,he found that his penis gradually became swollen,and thereafter the urination gradually became arduous.After three-mo-long consideration,he decided to visit the outpatient department of our medical center on his own.
Therefore,penile aspiration was performed to reduce the edema.Meanwhile,we exploited a pincher to fix the hoop,an intestinal spatula to protect the underlying skin,as well as sterile water for cooling secondary heat damage.A video clip of the surgical procedure could be found online as the.The foreign object was finally removed after 100 min of fretsaw cutting (Figure 2).There was scarcely any bleeding during the surgery.A urinary catheter was indwelled in case of temporary dysuria.The catheter was withdrawn and the patient was discharged in good condition two days after surgery.
OUTCOME AND FOLLOW-UP
There were no complications like dysuria,erectile dysfunction,urinary irritation,or urethral fistula through telephone follow-up on the exact time of one month and one year after surgery.
DISCUSSION
As far as we are concerned,the penis injury can be divided into different grades,varying from edema,skin loss,urethral fistula to complete amputation[8],that is:Grade 1:simple distal prepuce edema without penile skin ulcer or urethral injury;Grade 2:skin injury and cavernous compression,penile prepuce edema,accompanied by decreased sensation,but no urethral injury;Grade 3:urethral injury,loss of distal penile sensation,but no urinary fistula;Grade 4:the rupture of the cavernous urethral body and result in urinary fistula,further compression of the penile cavernous body with loss of sensation;and Grade 5:necrosis or spontaneous disconnection of the distal end of the penis.In our experience,anti-infection and decompression are basic principles to deal with such cases.At the same time,the severity of strangulation is mainly related to the foreign object itself,such as hardness,size,and smoothness.More specifically,when the surface between the incarcerating object and the penis is not smooth or too tight,the penis would present acute edema,ulcer,and even necrosis.However,long-term strangulation may only cause edema of the prepuce and local skin superficial ulcer when the incarceration is not severe,rather than penial necrosis and urinary fistula.This situation might be partial because,at this time,penial and urethral cavernous bodies are shielded from edematous skins.
It was only then that I realized I did not teach my father. He taught me. It was he who had engaged me in the conquest of language. It was he who told me to be direct, to be watchful25, to listen with my eyes and to ask with my mouth. From his silence, my father taught me the true power of speech.
A few days after the crash, Sonali s brother Chris, concerned that Sonali might not understand what was really happening, asked her, Do you know where Daddy is?
PI is an urgent situation.If treated untimely,it can result in devastating consequences,as the persistent constriction might lead to genital vascular occlusion,further causing skin loss,urethral-cutaneous fistula,erectile dysfunction,and even penile loss[6].Given that no particular tool has been designed for relieving the strangulation,and occasionally the patient is too old with severe comorbidities,a multidisciplinary team,sometimes including firefighters,physicians,and scrubbing nurses,is suggested to be established.
Generally,the treatment attempts we take should minimize the trauma to local tissues[9].Applying lubricating oil with appropriate traction to remove foreign objects directly is preferred.For those with severe incarceration and noticeable swelling,penis piercing could be performed.The piercing sites could be either the edematous skin,the subcutaneous skin,or the penial and urethral cavernous body when necessary[10].
For less-likely removable strangulating objects,direct cutting is recommended.Under these circumstances,the hardness and thickness of the material should be taken into consideration.For non-metallic incarcerations,such as hair tourniquet syndrome[11],rubber bands for disease prevention[2],plastic bottles for sexual entertainment[12],or seal rings[13],the treatments are reported to be comparatively more straightforward.However,as the strangulating objects had a certain degree of deformability,it is crucial to restore the deformed penis after removing the strangulating objects.Due to the metallic hoop's hardness and thickness,treatments on metallic incarcerations are more complicated.Previous literature mentioned various surgical tools,mostly from orthopedics and dentistry,such as motor-operated emery wheel machine,metal cutter,grinder,hacksaw,fretsaw,industrial-grade steel bolt cutters,and marble cutting tool[4,14,15].In extreme cases such as strangulation by axletree[16] or hammerhead,cautious planning is needed before violent cutting.The heat originating from the persistent cutting procedure could cause burn injury even with additional irrigation.Subsequently,the operation might be performed in a de-gloving way[16],which can be decomposed into three steps:(1) De-gloving the skin distal to the strangulated area till the coronal part;(2) Moving the constrictive object towards the distal end;and (3)Suturing the edge of the skin back.
Extra operations are required in exceptional situations,such as PI with shallow ulcerations or urinary tract fistulae.Ulceration indicates the necrosis of penial skin or partial corpus cavernosum.Thereafter,the necrotic part needs to be debrided first.However,if the wound defect is too large to be sutured,a skin graft with radial forearm flap neophallus might be required.If deep necrosis is found in the urethra,partial or entire penectomy might be necessary[9,17,18].
There were three main benefits of using a fretsaw in this case.First,compared with a dental drill and other electric equipment,the initiation,cessation,and alteration of cutting direction could be adjusted more responsively when deploying a fretsaw.Second,there would be no inertia and electric sparks because hands drove the fretsaw.Last but not least,because the cutting direction was from the inner layer to the outer surface,the accidental injury caused by the damage of the metal structure would be avoided.
Nevertheless,the cutting efficiency of using a fretsaw is comparatively low,as it is purely powered by hands.Continuously cutting for several minutes is tiring,and thereafter loss of controllability might occur.Same as other methods,thermal damage could not be avoided.Hence,an assistant must continuously spray normal saline with a syringe to cool the metal surface.
Several limitations should be noted.First,due to the rarity of PI,more cases are awaiting to be summarized to increase credibility and generality.Specific consideration should be taken regarding patient status,the degree of edema,and the material of the incarcerating object.Systematic reviews are called for to establish higher-level evidence.Second,specific steps,in this case,could be optimized,such as a bacterial culture could be performed in case of severe postoperative skin infection,and the postoperative daily observation of the wound might be better recorded.
CONCLUSION
In conclusion,the selection of cutting tools depends on the strangulating object and the availability of equipment.Meanwhile,the concrete operation also relies on the severity of penial damage.The urination function may not be affected after three months of incarceration like in this case,but prudent measures and sufficient preparations should be taken preoperatively.Even though using a fretsaw in treating PI is comparatively less efficient,it is feasible and safe.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- New trends in treatment of muscle fatigue throughout rehabilitation of elderlies with motor neuron diseases
- What emotion dimensions can affect working memory performance in healthy adults? A review
- Quadrilateral plate fractures of the acetabulum:Classification,approach,implant therapy and related research progress
- Methylprednisolone accelerate chest computed tomography absorption in COVID-19:A three-centered retrospective case control study from China
- Analysis of photostimulable phosphor image plate artifacts and their prevalence
- N6-methyladenine-modified DNA was decreased in Alzheimer’s disease patients