
Occupational fibrotic hypersensitivity pneumonia in a halogen dishes manufacturer:A case report
2022-01-24 09:24MinWangHaoHuiFangZiFengJiangWeiYeRongYuLiu
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Fibrotic hypersensitivity pneumonitis (FHP) is a chronic and fibrosing interstitial lung disease caused by inhaled antigen exposure which can develop in people working in specific environments or with specific career[1].The commonly known form is Farmer's lung[2].Halogen dishes are Chinese cuisines in which long-term boiling of various spices powder is required before meat and vegetables are added.Each halogen maker has a so-called secret recipe,but almost all contain ginger,pepper,soy sauce,and other spices.A single case of hypersensitivity pneumonitis (HP) associated with curry powder and ground pepper in a potato chip factory has been described[3].We herein report a case of FHP in a halogen dishes manufacturer,which may have been caused by the inhalation of spices.
FHP can lead to impaired respiratory function,reduced disease-related quality of life,and early mortality.Management of FHP should start with exposure remediation once the source of allergy is identified.A high index of suspicion is important to diagnosis,even after innocuous and apparently trivial exposures to potential antigens.We herein report a case of FHP in a halogen dishes manufacturer,which may have been caused by inhalation of spices.
CASE PRESENTATION
Imaging examinations
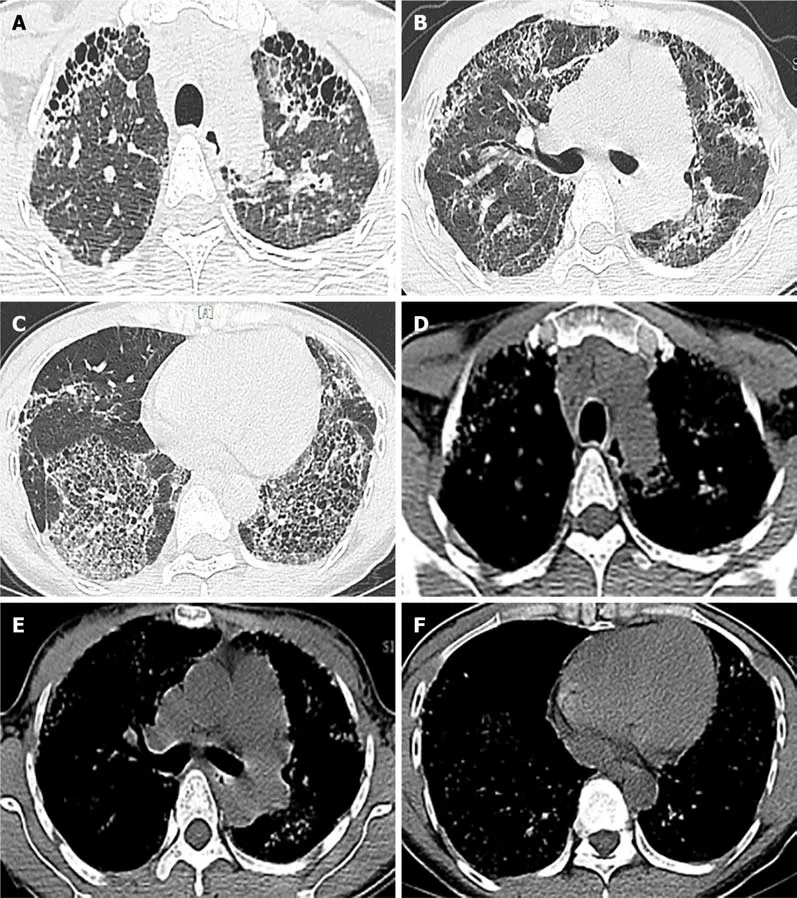
High resolution computed tomography (HRCT) of the chest showed thickening of interlobular septa and central lobular nodules which revealed honeycomb changes in severe areas (mainly in the lung base),as well as traction bronchiectasis (Figure 1).
If anyone deserves a special day, it s these brave souls who ve had to carve out a place for themselves in readymade families with the care and caution of a neurosurgeon.
Laboratory examinations
Routine blood,liver function,renal function tests and serum sodium,potassium,creatinine,magnesium,and calcium were all within normal limits.Blood tumor biomarkers including anti-nuclear antibody,anti-centromere antibody,anti-neutrophil cytoplasmic antibody,and Scl-70 antibody screens and C-reactive protein were negative.Pulmonary function tests showed a forced vital capacity (FVC) of 1.75 L(51.2% predicted),a forced expiratory volume in 1 s (FEV1) of 1.63 L (55%),an FEV1/FVC ratio of 109.6%,and carbon monoxide diffusing capacity 11.9 mmHg/mL/min (39% predicted).Cytology of bronchoalveolar lavage (BAL) fluid showed a large number of lymphocytes (the total number of cells was 4.16x10/mL,lymphocytes accounted for 70.4%,of which the lymphocyte CD4/CD8 ratio was 0.94,and bronchoscopy was performed to rule out a superimposed infection.Allergen determination showed that tree,pollen,ragweed,Artemisia argyi,home dust mite,home dust,cat hair,dog hair,cockroach,mold combination,legume,egg white,milk,peanut,soybean,beef,mutton,cod,shrimp,crab,salmon,lobster,scallop,were all negative.
The main symptoms of cough and breathing difficulties gradually improved slightly three months later,but no improvement in chest HRCT was noted.No significant adverse side-effects were noticed.The patient is currently on the lung transplant list.
Physical examination
She was a self-employed worker,cooking and selling halogen dishes for over 15 years,without any measures to protect the respiratory tract.There was no history of orthopnea,chest pain,or paroxysmal nocturnal dyspnea.She denied smoking and there was no history of asthma,allergies,or any other prior pulmonary disease.
Personal and family history
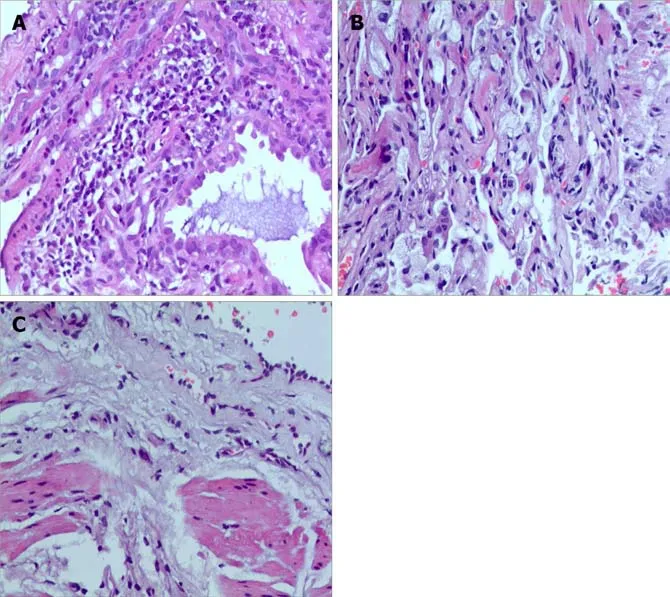
Fan-Qing Meng,MD,Professor,Department of Pathology.Fibrin-like exudation,more lymphocytes,foam-like tissue cells and a small number of macrophages were observed on histopathology of lavage fluid,suggesting persistent exposure to inhaled antigen.Transbronchial lung biopsy (TBLB) and computerized tomography-guided percutaneous lung puncture showed chronic lymphocyte and foamy macrophages infiltration,diffuse,relatively uniform alveolar septal thickness,hyperplasia of fibrous tissue in the bronchial wall,resulting in fibrosis (Figure 2).
History of past illness
On examination,her temperature was 36.7 ℃,blood pressure was 118/82 mmHg,heart rate was 74 bpm,oxygen saturation was 92% in room air,and respiratory rate was 22 breaths/min.The patient was identified as Grade 3-shortness of breath according to the mMRC (Modified Medical Research Council) dyspnea scale and lung examination revealed bilateral Velcro like crackles in the lower lung fields.The rest of her physical examination was unremarkable.
History of present illness
The Queen assured him of her eternal gratitude38, and promised, should he succeed, to give him her daughter in marriage, together with all the estates she herself owned
Chief complaints
A 35-year-old Chinese woman with no significant medical history was admitted to our hospital because of a cough and breathing difficulties.She was a self-employed cook who produced and sold halogen dishes for more than 15 years without appropriate equipment to protect the airway from inhalation.
MULTIDISCIPLINARY EXPERT CONSULTATION
This patient had no special personal and family history.
The patient took anti-inflammatory and cough medications intermittently,but there was no improvement in her symptoms.
FINAL DIAGNOSIS
The patient was started on prednisone 30 mg/d and pirfenidone anti-fibrosis treatment.Considering the side effects of high doses of hormones,the patient was discharged on a tapering schedule of prednisolone which was reduced by 5 mg every 2 wk.
TREATMENT
Occupational FHP due to probable long-term exposure of spices in a halogen dishes manufacturer.
Of course I promised I would, for I was too happy to think of what my parents would say, or indeed of anything except Richard was not at our meeting place as he had arranged
OUTCOME AND FOLLOW-UP
I know now that the man who sat with me on the old wooden stairs that hot summer night over thirty-five years ago was not a tall man. But to a five-year-old, he was a giant. We sat side by side, watching the sun go down behind the old Texaco service station across the busy street. A street that I was never allowed to cross unless accompanied by an adult, or at the very
DISCUSSION
This patient met the diagnostic criteria for FHP as she had a cough,breathing difficulties,long-term inhalation of spices,lymphocytic cellular pattern on BAL,bibasilar rales,reduction in diffusion capacity,and compatible radiologic and histopathological findings.BAL can not only exclude other major causes of interstitial pneumonia including alveolar hemorrhage,malignancy,infection,and eosinophilic lung disease,but also exclude common allergens.While BAL lymphocyte percentage in HP can vary substantially from 1.7% to 82%[4],in this patient BAL showed an obvious lymphocytic cellular pattern (70.4% lymphocytes) defined as a BAL differential count greater than 15%[5].Additionally,aggregation of foamy macrophages and lymphocyte infiltration was observed which indicated exposure to inhalant pathogens[6].Serologic studies for spices were not performed due to the patient’s insurance status (she only had basic medical insurance and restricted economics),and had no relevance to the diagnosis even if negative as this would not exclude the clinical diagnosis of HP due to exposure to spices.Therefore,inhaled spices were the presumed cause of FHP in this case,especially given the absence of any other identifiable exposures.
Then the boy and the girl went to the palace of the King, her father, where everyone was weeping for her death, and they could hardly believe their eyes when they saw her come back well
Novel antigens and exposures related to occupation continue to be described,even innocuous and trivial exposures to potential antigens such as green tea[7],citrus[8],and pyrethrin[9] have been described.To our knowledge,this is the first case of FHP in a halogen dishes manufacturer caused by spices globally,which was confirmed by the presence of fibrosis through histological evaluation of TBLB and percutaneous lung puncture.However,it has also been pointed out that in the presence of a concomitant allergic predisposition,such as bronchial asthma,allergic rhinitis,or chronic bronchitis,the biological response to inhalation may be enhanced.There was no apparent comorbidity in our patient and she was a nonsmoker.
Heightened awareness of potential exposures is imperative in making a diagnosis and a detailed assessment of occupational exposures as well as the occupational environment is necessary as demonstrated in this case.Avoiding contact is the key for patients with HP,not only for patients but also for other individuals who may be exposed to the same allergen[9].Although there are no obvious symptoms or failure of regular occupational disease physical examination or disease detection,it is essential to remind workers of their safety during the production process[8] (respirator,masks,improve ventilation,regular monitoring of air quality) and the compliance of workers should be confirmed.For those with established allergies,there are various ways to avoid exposure,for example,by changing jobs or occupations.Clinically appreciable improvement in symptomatic,physiologic,and radiographic features may be seen only in patients with non-fibrotic HP[10].Due to the long and insidious exposure to antigen,fibrosis was observed both radiologically and pathologically in our patient.Management of FHP should start with exposure remediation where possible,oral glucocoticoids and azathioprine achieved an initial improvement in pulmonary function tests and symptoms[11],anti-fibrosis therapy should be considered in patients with symptomatic or progressive disease,and non-pharmacologic and supportive management should be offered and,in cases of treatment-resistant,progressive illness,lung transplant should be considered[12,13].Based on this,we advised our patient to change her occupation,and prednisone and anti-fibrosis therapy was given to improve her symptoms.Halogen dishes manufacture is mostly a family business in China,the patient inherited the shop from her mother and had no other life skills,although she was no longer responsible for food preparation,she still sold the halogen dishes at the counter.Following treatment,her symptoms improved slightly and requiring long-term oxygen therapy,the HRCT scan showed no improvement.The patient is currently on the waiting list for a lung transplant.
CONCLUSION
Attention should be paid to the possibility of inhalation hypersensitivity pneumonitis caused by spices.Improvements in respiratory protection measures should be suggested for workers during the production process to avoid this type of lung disease.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- New trends in treatment of muscle fatigue throughout rehabilitation of elderlies with motor neuron diseases
- What emotion dimensions can affect working memory performance in healthy adults? A review
- Quadrilateral plate fractures of the acetabulum:Classification,approach,implant therapy and related research progress
- Methylprednisolone accelerate chest computed tomography absorption in COVID-19:A three-centered retrospective case control study from China
- Analysis of photostimulable phosphor image plate artifacts and their prevalence
- N6-methyladenine-modified DNA was decreased in Alzheimer’s disease patients