
Impact of failure mode and effects analysis-based emergency management on the effectiveness of craniocerebral injury treatment
2022-01-24 09:24XiaoLanShaoYaZhouWangXiongHuiChenWenJuanDing
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Craniocerebral injuries are clinical emergencies that mainly occur as a direct result of external violence to the head,and include brain injuries,skull fractures,soft tissue injuries,and others.In recent years,increases in the numbers of traffic accidents and aerial work injuries has resulted in an increased incidence of craniocerebral injuries,threatening the physical and mental health of patients and limiting their quality of life[1-3].Moreover,craniocerebral injuries are complex,progress rapidly,and have high disability and mortality rates.Failure to provide timely and effective intervention may affect the effectiveness of subsequent interventions,and may even be life threatening[4-6].Therefore,timely and effective emergency care affects the prognosis and recovery of patients with craniocerebral injuries.
Yes, Tsarevitch Ivan, the Gray Wolf said, and thou wouldst have slept forever had it not been for me. For thy brothers cut thee to pieces and took away with them the beautiful Tsar s daughter, the Horse with the Golden Mane and the Fire Bird. Make haste now and mount on my back, for thy brother Tsarevitch Vasilii today is to wed thy Helen the Beautiful.
The man answered that he had a little hut in the forest, and that she could rest there; but he also said that he was one who lived entirely27 apart from men, and owned no more than the hut, a horse, and a dog, and supported himself by hunting
Failure mode and effects analysis (FMEA) is a clinically important care management model that can prospectively quantify the risk and causes of healthcare process failures;it also facilitates the development and implementation of interventions to reduce the incidence of events that put the health of patients at risk,thereby helping to ensure patient safety[7,8].In addition,FMEA includes potential failure evaluation and analysis,and may be used to assess the consequences of and the implementation of interventions to address the occurrence of such failures.The use of FMEA has played an important role in the development of many disease interventions[9].
This study aimed to assess 84 cases of craniocerebral injury involving patients treated in our hospital,and explored the value of implementing an FMEA-based emergency management strategy using a group-control format.
MATERIALS AND METHODS
Selection criteria
Five indicators were reviewed.(1) The emergency care of patients in both groups was assessed,including the duration of pre-hospital emergency response measures,and time spent receiving the patient,reporting imaging findings,and reporting clinical test findings;(2) Levels of inflammatory stress indicators [Interleukin-6 (IL-6),C-reactive protein (CRP),and procalcitonin (PCT)] were measured in both groups pre-and postintervention.Blood samples were centrifuged (3500 rpm,15 min) and an enzymelinked immunosorbent assay was used to determine levels of stress indicators in sample supernatants;(3) The incidences of complications,in both groups,were determined;(4) The prognoses of the patients in both groups were assessed using the Glasgow prognostic score,as follows:grade 5,good (able to work and study);grade 4,moderate disability (able to live on their own);grade 3,severe disability (requires care for daily work and life activities);grade 2,vegetative survival;and grade 1,death from disease;and (5) Statistics regarding satisfaction with nursing care were assessed in both groups using the Newcastle Satisfaction with Nursing Scale,which contains 19 items out of 95.Scores>85 indicated that patients were very satisfied,67-85 indicated that patients were generally satisfied,and scores<67 indicated patient dissatisfaction.Satisfaction was calculated as follows:satisfaction=(generally satisfied+very satisfied)/total number of cases in the group × 100%.
The next day the old dame6 who looked after the house handed her all the keys, but pointed7 her out one that she would do well never to use, for if she did the whole palace would fall to the ground, and the grass would grow over it, and the damsel herself would be remembered no more
The exclusion criteria included transferring out/dying during the study period,>12 h between injury and admission,breastfeeding or pregnancy,poor compliance,and inability to complete the study.
So the girl seated herself on the horse, and rode for a long, long way, and at last she came to the mountain, where an aged woman was sitting outside with a gold carding-comb.52 The girl asked her if she knew the way to the castle which lay east of the sun and west of the moon; but she said what the first old woman had said: I know nothing about it, but that it is east of the sun and west of the moon, and that you will be a long time in getting to it, if ever you get there at all; but you shall have the loan of my horse to an old woman who lives the nearest to me: perhaps she may know where the castle is, and when you have got to her you may just strike the horse beneath the left ear and bid it go home again. Then she gave her the gold carding-comb, for it might, perhaps, be of use to her, she said.
Methods
In recent years,traffic accidents and work-at-height injuries have increased,and the incidence of brain injuries caused by this has risen sharply.
To combine clinical nursing experience,a systematic assessment of the physical and mental status of patients,and the potential risk factors were identified using possible failure mode crisis values (RPNs).RPNs are calculated as severity × frequency of occurrence × difficulty of failure detection,with each factor scored from 1 to 10;higher scores indicate a greater likelihood of occurrence.Failure modes with high RPN scores in a comprehensive assessment were considered most important.The final analysis of failure modes included cumbersome procedures and resuscitation plans,and negative emotions.In response to the assessment of the above failure modes,care improvement focused on optimizing emergency procedures and protocols,alleviating negative emotions,restoring patient bodily functions,and developing targeted intervention plans.
In conclusion,FMEA-based emergency management of craniocerebral injury patients has the potential to effectively shorten the amount of time spent on emergency care,alleviate inflammatory stress,reduce the risk of complications,and improve patient prognoses,while also achieving high levels of patient satisfaction.However,the observation and study time of this study was relatively short.Therefore,whether patients with craniocerebral injuries can benefit from FEMA-based emergency management needs to be further explored and confirmed using extended clinical follow-ups.
The patient’s stay in the observation room was also optimized.After the resuscitation was complete,the following were monitored:patient condition,degree of consciousness,presence of adverse event precursors related to craniocerebral injury,immediately informing the physician of problems and providing assistance with response measures.Finally,health education and psychological interventions were strengthened.After the patient’s condition was stabilized,the patient's education level,personality characteristics,and acceptance level were considered when providing health education and psychological guidance.Each patient was confirmed to have a basic knowledge of the disease,rehabilitation process,and precautions that should be taken.Further,each patient was encouraged to undergo treatment and rehabilitation with a positive and optimistic outlook.
Indicators
The inclusion criteria included a clear history of the causative injury;age>18 and<70 years;patients and family members able to understand the study;and voluntary provision of signed informed consent.
Suddenly my tiredness vanished. I smiled back, and later, when the manager asked me how I d liked my first day, I said, Fine! Those few words of praise had changed everything.
Statistical analysis
Data were analyzed using SPSS 22.0 (IBM,Armonk,NY,USA).Measurements were compared using the-test (means ± SD) or theχtest [(%)];ranked data were evaluated using the rank sum test;values<0.05 were considered statistically significant.
RESULTS
In the study group,satisfaction with nursing care was higher (95.24%) than in the control group (78.57%,<0.05;Table 5).
Between-group comparison of emergency care
Pre-hospital emergency response time,consultation time,imaging reporting time,and test reporting time values determined for the study group were shorter than those for the control group (<0.05),as shown in Table 1.
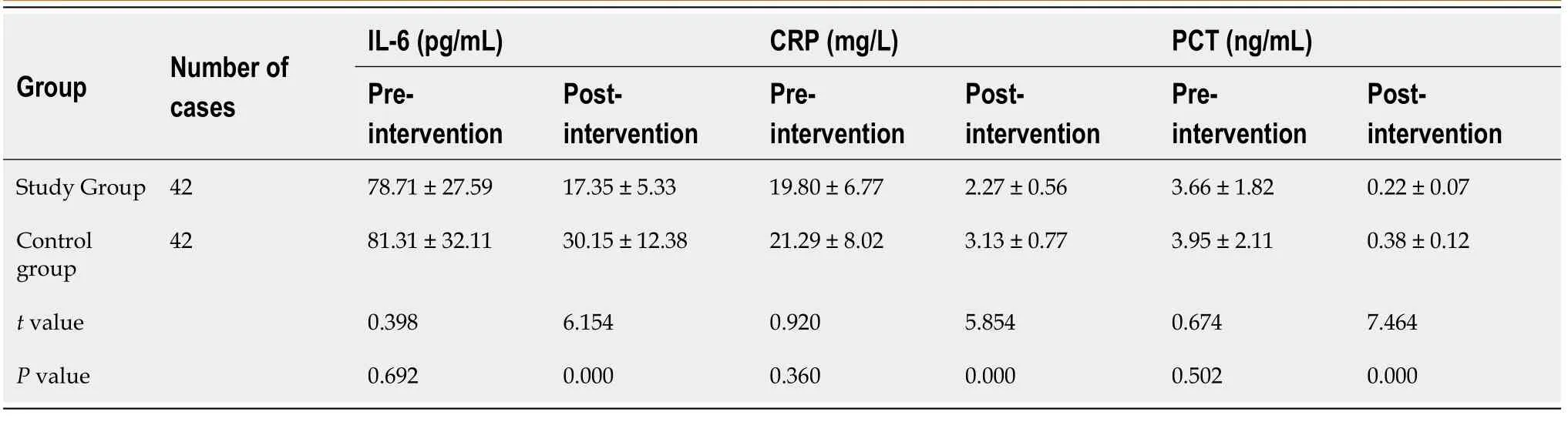
Between-group inflammatory stress response indicator level comparisons,pre-and post-intervention
Craniocerebral injuries are critical conditions caused by external violence,and are associated with a high rate of disability and death due to the potential effects on the central nervous system[10,11].Due to the critical nature and rapid progression of craniocerebral injuries,it is important to intervene early with effective care plans[12].
Between-group complication rate comparison
The incidence of complications in the study group (9.52%) was lower than that in the control group (26.19%,<0.05;Table 3).
Between-group comparison of patient prognoses
The patient prognoses in the study group were better than those in the control group (<0.05,Table 4).



Between-group comparison of nursing satisfaction
Eighty-four patients with craniocerebral injuries,treated at our hospital from November 2019 to March 2021,were selected and assigned,using the random number table method,into study (=42) and control (=42) groups.Twenty-three males and 19 females were included in the study group.The study-group patients were 22-68 years old (mean.45.91 ± 13.19 years);had injuries caused by traffic accidents (21 cases),falls from heights (15 cases),heavy object trauma (5 cases),and other (1 case);and had primary school (13 patients),junior high school and high school (18 patients),or college and above (11 patients) education levels.In the control group,there were 26 males and 16 females who were aged 21-69 years (mean,47.61 ± 11.95 years).The causes of injury in the control group included traffic accidents (18 cases),falls from heights (14 cases),heavy object trauma (7 cases),and others (3 cases).The highest education levels of control-group patients were primary school (11 patients),junior high and high school (21 patients),and college and above (10 patients).The clinical data regarding sex,age,cause of injury,and educational level were not significantly different between the two groups (>0.05).

DISCUSSION
Pre-intervention serum IL-6 (78.71 ± 27.59 pg/mL),CRP (19.80 ± 6.77 mg/L),and PCT(3.66 ± 1.82 ng/mL) levels in the study group were not significantly different from those of the control group (81.31 ± 32.11 pg/mL,21.29 ± 8.02 mg/L,3.95 ± 2.11 ng/mL;>0.05).However,the levels of serum indicators of both groups were lower post-pre-intervention.In the study group,post-intervention serum levels of IL-6 (17.35 ±5.33 pg/mL),CRP (2.27 ± 0.56 mg/L),and PCT (0.22 ± 0.07 ng/mL) were lower than those in the control group (30.15 ± 12.38 pg/mL,3.13 ± 0.77 mg/L,0.38 ± 0.12 ng/mL;<0.05;Table 2).
When the traditional model of care is employed,nursing staff tend to passively implement relevant interventions in accordance with departmental requirements and disease commonalities.Therefore,the traditional model fails to address issues in a systematic and timely manner,making it difficult for patients to benefit from the treatment provided[13,14].FMEA is an important clinical quality management model that integrates root cause analysis,hazard analysis and critical control points,failure modes,and effects analysis to quantitatively and prospectively assess possible process failures,identify factors contributing to and the effects of failures,and develop practical solutions for failures in accordance with findings[15].This study used a FMEA-based method to reveal the severity or likelihood of emergency care delays.As a result,screening of high-risk aspects of care could be performed,and intervention plans could be assessed to ensure treatment improvement.Potential factors leading to failure may also be explored.Further,the medical resources availablemanagement support,divisions of responsibilities,management strategies,and action strategies can also be used to optimize and implement intervention strategies.These strategies have the potential to improve the quality of medical services[16,17].
The present study findings showed that the pre-hospital emergency responses,consultations,and imaging and test report delivery times were shorter for patients in the study group than for those in the control group.Further,the prognoses of patients in the study group were better than those of the patients in the control group.Study group levels of serum IL-6,CRP,and PCT were lower than those in the control group (<0.05),confirming the value of FMEA-based emergency management in patients with craniocerebral damage.The implementation of the FMEA-based strategy shortened the time spent on diagnosis and treatment,better controlled the degree of inflammatory stress experienced,reduced the complication risks,and promoted disease regression compared with the traditional model.FMEA-based strategy implementation also shortened the time the patients spent in the clinic,controlled their inflammatory stress indicator levels,reduced complication risk,and promoted good disease outcomes.
The FMEA-based model is an important tool for facilitating risk assessment,improving treatment,and managing the treatment process.The FMEA model is designed to prevent issues before they happen and continuously improve the quality of care by adjusting for process and system deficiencies.The strategy effectively exposes deficiencies and defects in process control and project management,and may be used to achieve standardized management strategies and improved care using the quantifiable indicator,RPN.The admission process used in traditional emergency care is cumbersome and complex,with the receiving nurse implementing admission placement only after admission to the department.The process relies on the provision of a bed,lacks good proactive reception,and results in low nursing efficiency.In contrast,FMEA-based emergency management has the potential to simplify admission procedures and open green channels,shortening the time needed to perform emergency care and ensure that patients are treated effectively and early[18,19].In addition,in traditional emergency nursing management,nursing staff are encouraged to complete tasks in a mechanical manner when receiving patients,and their levels of active service consciousness and enthusiasm are low.In addition,some nursing staff lack professional knowledge and the ability to disseminate information,which has the potential to affect patient compliance to varying degrees.When using FMEA theorybased nursing management,job objectives are clear,promoting nursing staff attentiveness and responsibility.In this situation,the nursing staff have the ability to actively acquire needed professional knowledge within the department and improve their professional status,which is conducive to ensuring quality clinical nursing care[20].
The results of this study also showed that the study group patients had higher levels of satisfaction with their care than did those in the control group (<0.05),suggesting that FMEA-based emergency management is advantageous because it improves the acceptance of care by patients with craniocerebral injuries.Patients treated in accordance with the FMEA theory are treated rapidly and effectively,which reduces disease-related complications and improves patient satisfaction.Some studies have also shown that the admission process used in conventional emergency care is complex,and the lack of integration between the various tasks during examination,transfer and treatment is often due to human or systematic factors,resulting in a poor patient experience.Using FMEA theory-based methods is conducive to enhancing patient trust in healthcare professionals,improving the healthcare experience,and increasing patient satisfaction with healthcare service enhancement[21,22].
CONCLUSION
Reception protocols were optimized as follows:patients with craniocerebral injuries were sent to the emergency resuscitation room immediately after admission;physicians were informed to launch a green channel;principles of consultation,examination,and treatment priority were strictly followed during the resuscitation process;and the patient's condition was comprehensively assessed.Nurse-based resuscitation measures were optimized such that the resuscitation room nurses and mobile nurses formed an emergency care team with the following individual duties.The treatment nurse drew blood,performed electrocardiography,established intravenous access,and monitored oxygen saturation levels throughout the intervention.The resuscitation room nurse provided patient assistance to maintain a reasonable position,closely observed the patient’s condition,and maintained an open airway.The mobile nurse prepared the instruments required for resuscitation and administered oxygen,sputum inhalation prevention protocols,and other related treatments.The team leader strictly recorded the resuscitation process and the elapsed time during resuscitation.
ARTICLE HIGHLIGHTS
Research background
The control group received conventional care,which included patient admission and pre-screening by nursing staff.The nursing staff also assisted craniocerebral injury patients throughout their initial diagnoses and related auxiliary examinations,and systematically reassessed patient conditions.The study group received FMEA theorybased emergency management,based on the control group:to clarify the failure mode and nursing themes,English databases were used;to clarify the failure modes and nursing topics,literature search data from English databases (Proquest Science Journal Database,Springer Link Science and Technology Journal Database,Elsevier Database,PubMed Medical Journal Database,) were used.
But they were not very, very far from land, and there was just enough strength left in the North Wind to enable him to throw her on to the shore, immediately under the windows of a castle which lay east of the sun and west of the moon; but then he was so weary and worn out that he was forced to rest for several days before he could go to his own home again
Research motivation
Explore the application value of emergency management based on failure mode and impact analysis (FMEA) in the treatment of head injury.
Research objectives
This study aimed to explore the impact of emergency management based on FMEA on the treatment of head injury.
Research methods
A study was conducted on 84 patients with craniocerebral injury admitted to our hospital from November 2019 to March 2021.
Then she came to a royal garden, and by the shimmering11 of the moon12 she saw that trees covered with beautiful fruits grew in it, but she could not enter, for there was much water round about it
Research results
For the study group,the evaluation parameters (pre-hospital emergency response time,consultation time,time required to report imaging results,and test report time)were shorter than those of the control group.After the intervention,the serum index levels of the two groups were lower than the pre-intervention level.Study The incidence of complications in the study group was lower than that of the control group.The prognosis of patients in the study group was better than that of the control group (P<0.05).The nursing satisfaction of patients in the study group was higher than that of the control group.
Research conclusions
FMEA-based craniocerebral injury management effectively shortens the time spent on emergency care,reduces inflammatory stress and complication risk levels,and helps improve patient prognoses,while achieving high patient care satisfaction levels.
Research perspectives
Emergency management based on FMEA can be more widely used in the treatment of head injury.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- New trends in treatment of muscle fatigue throughout rehabilitation of elderlies with motor neuron diseases
- What emotion dimensions can affect working memory performance in healthy adults? A review
- Quadrilateral plate fractures of the acetabulum:Classification,approach,implant therapy and related research progress
- Methylprednisolone accelerate chest computed tomography absorption in COVID-19:A three-centered retrospective case control study from China
- Analysis of photostimulable phosphor image plate artifacts and their prevalence
- N6-methyladenine-modified DNA was decreased in Alzheimer’s disease patients