
Modified surgical method of supra-and infratentorial epidural hematoma and the related anatomical study of the squamous part of the occipital bone
2022-01-24 09:24RuiChunLiShiWenGuoChenLiang
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Supra-and infratentorial acute epidural hematoma (SIEDH) is a common posterior cranial fossa epidural hematoma located at the inner surface of the squamous part of the occipital bone (SOB)[1-3].Most SIEDHs are caused by direct violence to the occipital bone due to traffic accidents and falls[4-6].The traditional surgical method requires a tedious combined supra-infratentorial craniotomy to evacuate the SIEDH[2,7,8].However,the SOB does not present as a single straight plane,but bends at an angle around the external occipital protuberance (EOP) and the superior nuchal lines,which divide the SOB into the supra-and infratentorial areas,respectively[9].As the angle of the SOB (ASOB) is less than 180,there is an operative angle for the SIEDH(OAS) from the supra-to infratentorial epidural space by a single supratentorial craniotomy.
In this study,the ASOB and the OAS were analyzed quantitatively.An illustrative case example is presented to demonstrate the technique nuances of the modified surgical method.
The queen and the princes were there, but she was poorly clad and so sorrowful that the king did not recognise her, neither did he think for a moment that the two children, who were dressed only in rough skins, were his own sons
Whilst I was fainting with terror he transported me here, and cried to me with his awful voice: There shall you remain, lonely and hideous84, despised even by the brutes85, till the end of your days, or till some one of his own free will asks you to be his wife
MATERIALS AND METHODS
ASOB
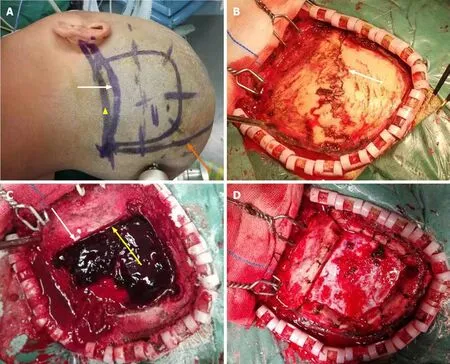
After general anesthesia,the patients were positioned laterally with the head fixed by a Mayfield head frame (Integra LifeSciences Corporation,Cincinnati,OH,United States).According to the location of the hematoma,a unilateral occipital skin flap was incised and the boundary of the bone flap was defined by 4 Lines:The midline,the lateral edge of the hematoma,the upper edge of the hematoma and the lower margin of the transverse sinus (Figure 3).Four bony holes were drilled using the Medtronic high-speed drill (Medtronic,Minneapolis,MN,United States) at the corners of the bone flap,and a supratentorial craniotomy was completed.Subsequently,the supratentorial part of the SIEDH was gradually removed by suction and forceps.When the dura mater was exposed,the bleeding arteries on the dura were immediately electrocoagulated.In the transverse sinus region,the hematoma was carefully evacuated and a gelatin sponge was used to stop the bleeding from the sinus.The inferior part of the SIEDH was then explored and evacuated.Finally,the dura mater was carefully suspended at the edge of the craniectomy and the bone flap was fixed.
On the median sagittal plane of the computed tomography (CT) scan,the ASOB was defined by two lines:One is from the EOP to the LambS,and the other is from the EOP to the posterior edge of the foramen magnum (poFM) (Figure 2A).

OAS
On the median sagittal plane of the CT scan,an angle was defined to analyze the OAS quantitatively.The OAS was determined by two intersecting lines with the vertex located at the poFM.The first line passes from the midpoint between the EOP and the LambS to the poFM,while the second line passes from the EOP to the poFM(Figure 2B).Theoretically,the OAS can represent the surgical freedom for clearance of the SIEDH from the supra-to infratentorial epidural space by a single supratentorial craniotomy.Mathematically,the greater the OAS is,the bigger the operative corridor is.
A few days later my mother died of a massive6 heart attack. It happened so suddenly that I didn t have a chance to do anything for her. At that moment I understood the importance of saying in time: I LOVE YOU and to give our loved ones the time that they deserve.
Radiological data
In this study,we found that the superior and inferior parts of the SOB were not located in one plane but were connected at an intersection angle (ASOB).The ASOB in males was smaller than that in females (118.4 ± 4.7130.4 ± 5.1).As the ASOB was less than 180 in both males and females,when elevating the dura,there was an operative corridor for evacuation of the SIEDH from the supratentorial to infratentorial epidural space in a single supratentorial craniotomy.The OAS was used to analyze this operative corridor quantitatively and the study revealed that the OAS in males was greater than that in females (15.1 ± 1.812.8 ± 2.0).These results indicated that the smaller the ASOB is,the greater the OAS is.These anatomical morphological characteristics are extremely important for modification of the surgical method.
Immediately he took the shape of a harpy, and, filled with rage, was determined53 to devour54 his son, and even the Princess too, if only he could overtake them
Patients with SIEDH
A total of 8 patients with SIEDH were surgically treated from July 1,2017 to March 31,2020.These patients consisted of 6 males and 2 females,aged from 23 to 49 years(mean 32.5 ± 10.5 years).Seven cases were admitted following traffic accidents and 1 case following a fall injury.Three of these patients had occipital and frontal lobe contusion and laceration.The admission Glasgow Coma Score (GCS) was 9 points in 3 cases,10 points in 4 cases and 11 points in 1 case (median 10 points).
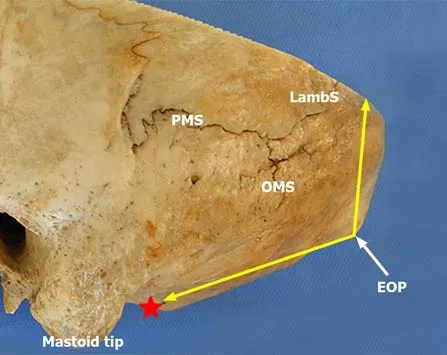
According to Rhoton's research,the occipital bone is divided into a SOB part located above and behind the foramen magnum,a basal part situated in front of the foramen magnum,and paired condylar parts located lateral to the foramen magnum[9,12].The SOB extends from the foramen magnum inferiorly to the LambS superiorly.The EOP and the superior nuchal lines divide the SOB into superior and inferior parts which locate up and down to the transverse sinus,respectively.The inferior part of the SOB is also called the suboccipital area with a rough outer surface which serves as the site of attachment of numerous muscles including the trapezius,sternocleidomastoid,splenius capitis and semispinalis muscles,.[9].
Modification of the surgical method
The SOB is located above the posterior edge of the foramen magnum and articulates with the parietal bone at the lambdoid suture (LambS).The EOP,with the superior nuchal lines radiated laterally from it,is situated at the central part of the external surface of the SOB and divides the SOB into superior and inferior parts.The two parts form an angle with the EOP at the vertex (schematic representation in Figure 1).
Statistical analysis
The SOB does not present as a single straight plane but bends at an angle around the EOP and the superior nuchal lines,and the smaller the ASOB was,the larger the OAS was.These morphological characteristics of the SOB make it possible to evacuate the SIEDH from the supra-to infratentorial epidural space by a single supratentorial craniotomy.
RESULTS
Statistical analysis of the ASOB and OAS
The ASOB of male patients was smaller than that of female patients (118.4 ± 4.7130.4 ± 5.1),while the OAS of males was greater than that of females (15.1 ± 1.812.8± 2.0).These data are shown in Table 1.These results indicated that the smaller the ASOB was,the greater the OAS was.
Clinical presentation
A skull CT examination was performed within 24 h postoperatively.The SIEDH was totally removed in all 8 cases.The postoperative GCS scores were 10 in 4 cases,11 in 2 cases,12 in 1 case and 13 in 1 case 72 h after surgery.The median score was 10.5,which was significantly higher than that before surgery (Table 2).Postoperatively,one patient developed pneumonia which was cured by antibiotic treatment within 2 wk.Intracranial infection,subcutaneous effusion and cerebrospinal fluid leakage were not observed.


Illustrative case
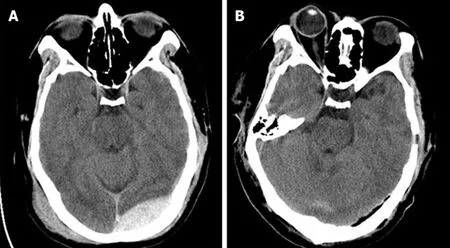
A 29-year-old man was admitted to hospital 3 h after a traffic accident.The admission GCS score was 10.The CT examination revealed a left SIEDH and scalp hematoma(Figure 4A).Surgical treatment was carried out according to the method described above.Intraoperatively,a linear fracture of the occipital bone extended from the LambS to the mastoid (Figure 3B),which was the source of the epidural hematoma.The hematoma covering the transverse sinus area separated the dura from the inner surface of the skull,which created a surgical corridor from supratentorial to infratentorial (Figure 3C).The hematoma was completely cleared,which was confirmed by a postoperative CT scan (Figures 3D and 4B).The bone flap was perfectly reset and fixed without any obvious bone defects (Figure 4B).
I was young then, some 20 years ago, and in pretty good shape. I d been putting in a solid eight hours of Aikido training nearly every day for the past three years. I liked to throw and grapple. I thought I was tough. The trouble was my martial10 skill was untested in actual combat. As students of Aikido, we were not allowed to fight.
DISCUSSION
The SIEDH,which traverses the transverse sinus from the supa-to inferior tentorial,represents 11%-64% of all posterior fossa epidural hematomas[2,3,6].Due to potential severe brain edema due to compression on the transverse sinus by the hematoma,some scholars have suggested aggressive surgical treatment even if the hematoma volume is small[6-8].Traditionally,a combined supra-inferior craniotomy was recommended.The supratentorial bone flap was reset at the end of surgery,while the infratentorial bone,in the suboccipital area,was removed.The purpose of the traditional method was to maximize exposure of the hematoma and thoroughly remove it[8,10].However,the combined supra-inferior craniotomy has the following disadvantages:Firstly,it requires the cutting of multi-layer muscles in the suboccipital area,which can be time-consuming and increase blood loss;secondly,a suboccipital craniotomy is often accompanied by a subsequent large bone defect[11].To avoid a large bone defect in the suboccipital area,Wang and Guoping[7] recommended a single supratentorial craniotomy to remove the SIEDH.Their research showed that this technique led to efficient total evacuation of the SIEDH.
Therefore,based on the anatomical characteristics of the SOB,this study theoretically demonstrated the feasibility of single supratentorial craniotomy in the treatment of SIEDH.
In one hand she held a sceptre, and in the other the imperial globe, and on either side of her stood two rows of halberdiers, each smaller than the other, from a seven-foot giant to the tiniest little dwarf25 no higher than my little finger
The skull CT scans of 32 adult patients (16 males and 16 females,aged from 18 to 65 years) were collected in the Neurosurgical Department of Xi’an Jiaotong University from January 1,2019 to January 31,2020.These patients included 22 cases of intracranial aneurysms and 8 cases of acoustic schwannomas.The ASOB and OAS were measured on the median sagittal plane of the CT scans and the data were analyzed statistically.
Intraoperatively,we performed a single craniotomy above the transverse sinus.After the supratentorial part of the SIEDH had been cleared,the dura of the transverse sinus was often found to be peeled off from the inner surface of the skull.In the 8 cases included in this study,all the infratentorial part of the SIEDHs were explored and removed completely.This modified surgical method of the single supratentorial craniotomy omitted the tedious steps of infratentorial craniotomy and its complications were also avoided.
However,the number of cases in this study was relatively small,and there were no cases with transection or laceration of the transverse sinus.In such situations,the combination of supra-inferior tentorial craniotomy should be performed to control the abundant bleeding through a greater range of exposure[13].
Promises, while important today, were more powerful in the past when honor was a great motivator. Also, before the time of literacy among the masses and written contracts, verbal promises were given greater weight. A promise was a contract and actionable by law if broken. Folklore emphasizes the importance of a promise by meting punishment upon those who do not keep their promises. One has the sense that the king is in a no-win situation. He will suffer if he breaks his promise and he will suffer if he doesn t as the tale will show.Return to place in story.
CONCLUSION
The Shapiro-Wilk test was used to analyze the normality of the data,and Levene’s test was used to analyze the homogeneity of variance.The-test was used for comparisons between the two groups when the data were in accordance with normal distribution and homogeneity of variance,otherwise the Rank sum test was used.A two-tailed<0.05 indicated statistical significance.All statistics were performed with R version 4.0.2.
ARTICLE HIGHLIGHTS
Research background
Traditional surgical treatment of the supra-and infratentorial acute epidural hematoma (SIEDH) requires a combined supra-infratentorial craniotomy.
In the early 70 s my mother attended college during the day while my sister was in school and I was in daycare. One day at daycare I watched an extremely tired mother attempt to pick up her daughter. The little girl asked, Momma are we going to McDonalds for dinner? The mother replied, Honey, not tonight. Momma has to run a few errands and then we have to go home and cook dinner for Daddy. But I wanna go. Susie, I said not tonight. Maybe, if you are a good girl we can go tomorrow. Susie immediately dropped to the floor, kicking and screaming, I want to go to McDonalds.
Research motivation
To modify the surgery method according to the results of anatomical research.
Research objectives
To analyze the morphological characteristics of the squamous part of the occipital bone (SOB) and introduce a single supratentorial craniotomy for SIEDH.
Research methods
Skull computed tomography scan data from 32 adult patients were collected.The angle of the SOB (ASOB) and the operative angle for the SIEDH (OAS) were measured and analyzed.
Research results
For males,the ASOB was 118.4 ± 4.7 and the OAS was 15.1 ± 1.8;for females,the ASOB was 130.4 ± 5.1 and the OAS was 12.8 ± 2.0.The smaller the ASOB was,the larger the OAS was.Based on the anatomical study,a single supratentorial craniotomy was performed in 8 patients with SIEDH,and the SIEDH was completely removed.
Research conclusions
The single supratentorial craniotomy for SIEDH is reliable and effective.
Research perspectives
It is hoped that the results of this study can improve the efficiency of surgical treatment of SIEDH.
We thank Professor Wang Y,the Department of Anatomy of Medical College of Xi’an Jiaotong University,for providing radiological data for this study.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- New trends in treatment of muscle fatigue throughout rehabilitation of elderlies with motor neuron diseases
- What emotion dimensions can affect working memory performance in healthy adults? A review
- Quadrilateral plate fractures of the acetabulum:Classification,approach,implant therapy and related research progress
- Methylprednisolone accelerate chest computed tomography absorption in COVID-19:A three-centered retrospective case control study from China
- Analysis of photostimulable phosphor image plate artifacts and their prevalence
- N6-methyladenine-modified DNA was decreased in Alzheimer’s disease patients