
Regional anesthesia for orthopedic procedures: What orthopedic surgeons need to know
2022-01-22 08:44IhabKamelMuhammadAhmedAnishSethi
World Journal of Orthopedics 2022年1期
INTRODUCTION
Orthopedic surgery is one of the most rapidly growing surgical specialties in the world.A total of 22.3 million orthopedic surgical procedures were performed worldwide in 2017.The number of annual orthopedic procedures is forecasted to increase 4.9% annually, approaching 28.3 million surgeries by the year 2022[1].Anesthetic techniques for orthopedic surgical procedures include general and regional anesthesia techniques.Over the past decades, regional anesthesia has become the anesthetic technique of choice for many orthopedic procedures.Regional anesthesia entails the injection of local anesthetic solution to interrupt signal transmission in peripheral nerves or spinal nerve roots that provide sensory and motor supply to operative structures.
The use of regional anesthesia for orthopedic procedures mitigates some of the complications associated with general anesthesia such as nausea, vomiting, airway trauma, hypoxia, respiratory depression, and the risk of pulmonary aspiration[2,3].Advantages of regional anesthesia for orthopedic surgeries include superior postoperative pain control, reduction in opioid consumption, reduced opioidassociated side effects[4-12], shorter hospital stay[7,8,11-13], early initiation of physical therapy[7,11], reduced hospital readmission rate[14], higher patient satisfaction[4,11], faster recovery[15], reduced unanticipated admissions due to uncontrolled pain[16], improved intraoperative muscle relaxation, decreased intraoperative blood loss[11,12], and a reduction in postoperative urinary retention and ileus formation[8].
Although regional blocks are often administered by the anesthesiologist, it is important for the orthopedic surgeon to have an understanding of the relevant clinical aspects of the blocks in order to optimize patient safety, maximize perioperative efficiency, and improve clinical outcomes.In this article, we review the techniques of regional anesthesia used for orthopedic procedures.
TYPES OF REGIONAL ANESTHESIA
Regional anesthesia can be broadly divided into two categories: neuraxial anesthesia [spinal, epidural, combined spinal epidural (CSE)], and peripheral nerve blocks (upper and lower extremity blocks).
Neuraxial anesthesia
Neuraxial anesthesia (NA) is the process of placing a needle or a catheter between the vertebrae and injecting medications into the epidural (epidural anesthesia) or subarachnoid space (spinal anesthesia).The target of NA is the spinal nerve root.Medication injected neuraxially is primarily local anesthetics with adjuncts such as preservative free opioids.NA is commonly used for abdominal and lower extremity surgeries.The sensory level required for a specific surgery is determined by the extent of surgical incision and surgical manipulation.Total hip arthroplasty (THA), open reduction and internal fixation of femur, and hip fractures require a sensory level of T10, whereas knee procedures require a sensory level of L1.
Well, that was a very small matter, they thought, and agreed to do it. The Princess with the long nose began to wash as well as she could, but, the more she washed and rubbed, the larger the spots grew. Ah! you can t wash at all, said the old troll-hag, who was her mother. Give it to me. But she too had not had the shirt very long in her hands before it looked worse still, and, the more she washed it and rubbed it, the larger and blacker grew the spots.
Spinal anesthesia is typically administered as a single injection, while epidural anesthesia is usually administeredan indwelling catheter for continuous infusion.CSE anesthesia is administered as a combination of both techniques.Anesthetic duration associated with the single shot approach used in the spinal technique is limited to the duration of action of the injected medication.The extent of spinal blockade (level) depends on the total dose of local anesthetic mixture, baricity of the injected solution, and patient position after the block.An epidural catheter allows for the continuous infusion of medications prolonging the duration of anesthesia.The spinal anesthesia needle is typically inserted at the level of L2-L3 interspace or below, to avoid trauma to the termination of the conus medullaris.The needle insertion point for epidural anesthesia depends on the extent of the dermatomes required to be anesthetized for the procedure.For orthopedic procedures, it is usually placed in the mid to low lumbar region.The extent of epidural blockade is determined by the volume of local anesthetic injected while density of the block is determined by the concentration of the local anesthetic.Compared to epidural anesthesia, spinal anesthesia produces a denser and more reliable block with lower incidence of block failure.
Peripheral nerve blocks
The popliteal block is performed in conjunction with the saphenous nerve block for surgery involving the foot and ankle[16].The popliteal fossa is the region where the sciatic nerve divides into its two major terminal branches, the tibial nerve and common peroneal nerve[89].The popliteal block is often performed proximal to the bifurcation of the tibial and common peroneal nerves; however, a recent study suggests that a popliteal block distal to the sciatic nerve bifurcation may result in 30% faster onset of the blockade while still achieving blockade of the terminal branches[90].Additionally, injection of local anesthetic distal to the bifurcation of the sciatic nerve provides superior sensory block of the lower extremity[91].
EVALUATING THE ORTHOPEDIC PATIENT FOR REGIONAL ANESTHESIA
Prior to considering a regional anesthetic for a patient, a thorough history and targeted physical examination should be performed to identify risk factors related to the nervous, pulmonary, cardiovascular, and hematologic systems that may affect the safety and efficacy of the nerve block.Certain patient factors may increase the potential for block failure, such as patient obesity[17].Local skin infection, or systemic infection, may preclude a patient from receiving a regional anesthetic.The decision to proceed with a regional anesthesia block should be collectively agreed upon by the patient, the surgeon, and the anesthesiologist.For patients on anticoagulation / antiplatelet medications receiving superficial peripheral nerve blocks, the decision to proceed is largely dependent on a careful analysis of factors including site compressibility, vascularity, and consequences of bleeding, should it occur.This is often determined on a case-by-case basis.
The nervous system
A comprehensive neurological evaluation should be performed to assess for any preexisting nervous system condition or nerve injury in the region of the block.Patients with multiple sclerosis may experience a flare up of symptoms with spinal anesthesia.Thus, epidural or general anesthesia may be preferable for these patients.Neuraxial anesthesia in patients with a history of extensive spine surgery with instrumentation may be technically difficult and may result in an inadequate anesthetic level.Scoliosis may increase the difficulty of placing a neuraxial anesthetic.Potential postoperative motor and sensory weakness after a regional anesthetic should be considered.For example, lower extremity motor weakness following a femoral nerve block may limit the patient’s ability to participate in therapy post-operatively; as such, an alternative motor-sparing technique should be considered[18].
She made the acquaintance of the King and the Queen without at first letting them know that she was a fairy, and they soon took a great fancy to her, and even trusted her with the precious Prince, whom she carried off to her palace, where she regaled him with cakes and tarts9 and every other good thing
The respiratory system
Patients who have a history of severe reactive or obstructive airway disease may benefit from the use of regional anesthesia to avoid airway manipulation and respiratory depression associated with general anesthesia.Pre-operative pulmonary function should be assessed, especially during the performance of upper extremity blocks that may anesthetize the phrenic nerve potentially causing respiratory distress.This may have significant impact on the respiratory function in patients with asthma, chronic obstructive pulmonary disease, or pre-existing diaphragmatic dysfunction[19].An alternative regional anesthetic approach, such as the axillary block, may be performed in these patients[19].
The cardiovascular system
Patients with a history of severe cardiovascular disease often have an elevated risk of major complications after receiving general anesthesia.Regional anesthesia remains an excellent alternative for these patients and can be associated with lower rates of major cardiac complications[20].It is important to consider cardiac contraindications for certain regional techniques.Neuraxial anesthesia has widely been contraindicated in the case of severe aortic stenosis and congestive heart failure, due to the sudden decrease in vascular tone and cardiac output.However, a carefully managed neuraxial anesthetic may be appropriate for some of these patients[21,22].Patients with significant cardiac disease benefit from the gradual onset of epidural anesthesia allowing for careful and slow titration of LA rather than the rapid onset block induced by a single-shot spinal anesthetic.
The hematologic system
Patients who have a history of bleeding disorders or are currently receiving anticoagulants or antiplatelet medications are at an increased risk of bleeding complications after receiving a regional anesthetic.It is important to perform a thorough review of the patient’s current medications prior to proceeding with a neuraxial anesthetic or peripheral nerve block.With the advent of novel anticoagulants, perioperative guidelines for regional anesthesia should consistently be adhered to[23].
10.The goose hopped down from the dish, reeled about on the floor with knife and fork in its breast: Vision number two. This vision directly addresses the girl s hunger. Goose is a traditional meal served during the Christmas and New Year holidays, but one the matchgirl s family could ill afford.
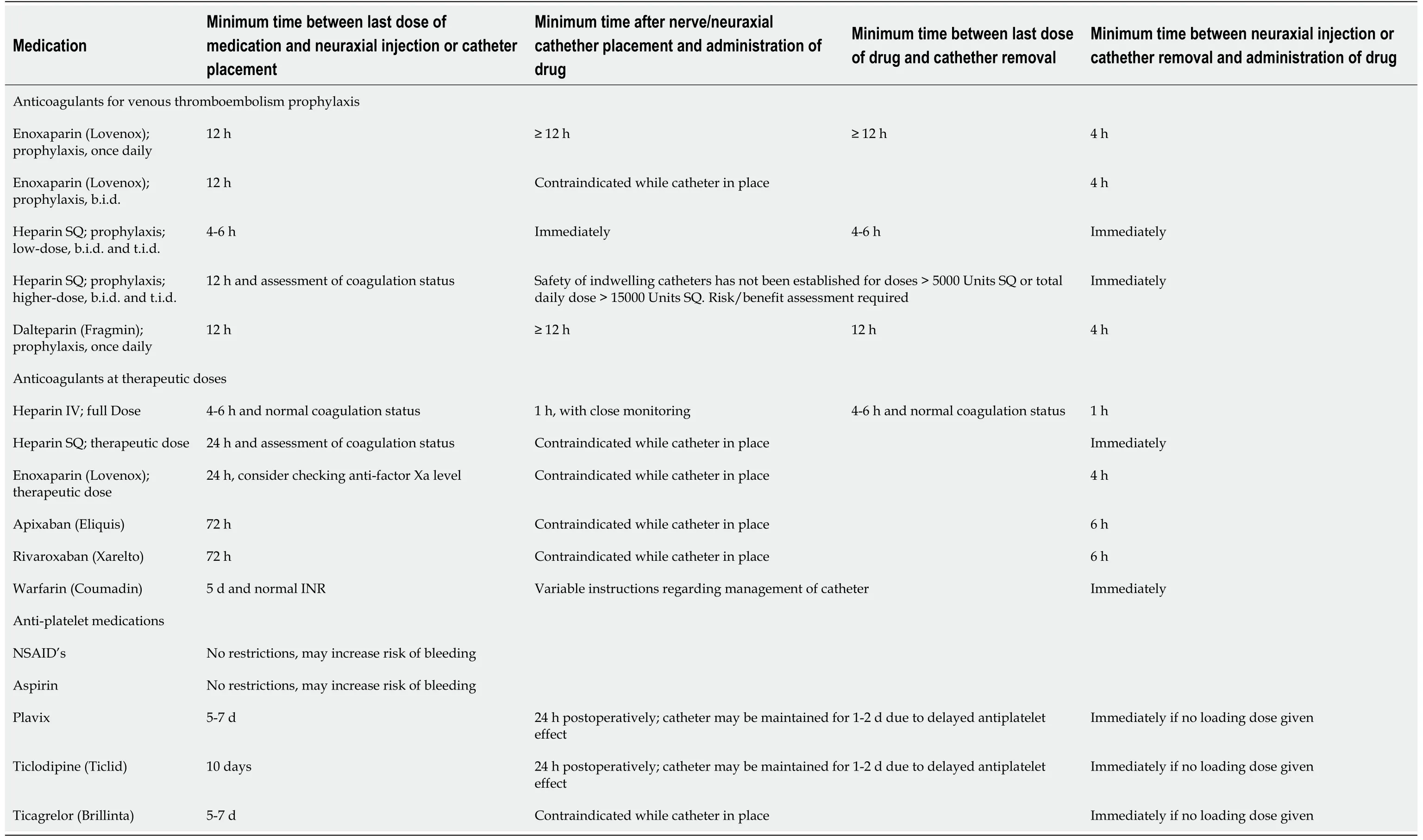
Laboratory findings consistent with thrombocytopenia or coagulopathy may preclude the administration of regional anesthesia, due to the increased risk of bleeding.Excessive bleeding in neuraxial anesthesia may lead to a spinal hematoma and subsequent adverse neurological consequences.The American Society of Regional Anesthesia (ASRA) has published guidelines for the management of patients receiving antithrombotic or antiplatelet medications[23].The ASRA guidelines are reviewed in Table 1.Patients who are on certain antiplatelet medications, such as low dose aspirin, may be candidates for peripheral nerve blockade or neuraxial anesthesia[23].This decision is based on a risk-benefit assessment, taking into account considerations such as site compressibility and underlying bleeding disorders.
BLOCKS FOR UPPER EXTREMITY ORTHOPEDIC PROCEDURES
Understanding upper extremity peripheral nerve blockade requires a detailed knowledge of the brachial plexus anatomy.The muscular and the cutaneous nerve supply of the upper extremity derives mostly from the brachial plexus.The brachial plexus is comprised of ventral nerve roots (rami) of 5 spinal nerve (C5-T1) giving rise to trunks, divisions, cords and terminal branches.The nerve roots merge to form upper, middle and lower trunks.The 3 trunks split to form 6 divisions which merge to form 3 cords; lateral, posterior and medial cords.The nerves supplying most of the upper extremity are the terminal branches of the 3 cords.The cutaneous portion of the shoulder and upper arm is supplemented by nerves that are not part of the brachial plexus[24].The superior aspect of the shoulder receives sensory innervation by the superficial cervical plexus (C3-C4)the supraclavicular nerve.Seventy percent of the sensory innervation to the shoulder comes from the superior trunkthe suprascapular nerve with most of the contributions being from the C5 and C6 nerve roots[25].The axilla is innervated by the second thoracic nerve root.The brachial plexus is blocked at four different levels: At the level of roots-trunksthe interscalene block, at the level of trunks-divisionsthe supraclavicular block, at the level of cordsthe infraclavicular block, and at the level of the terminal branchesthe axillary block.A summary of upper extremity peripheral nerve blocks is included in Table 2.

Interscalene block
The interscalene block is performed at the level of roots-trunks of the brachial plexus.The interscalene block results in anesthesia of C5 through C8, and also blocks the supraclavicular branches of the cervical plexus C3 and C4, which supplies the skin over the acromion and the clavicle.The inferior trunk (C8-T1) is usually spared; an effect referred to as ulnar sparing.Thus, if this block is performed for procedures at or distal to the elbow, an additional ulnar nerve block is required.The coverage of this nerve block makes it effective for procedures involving the shoulder, proximal aspect of humerus and the distal aspect of the clavicle[25].
In general, fairy godmothers are supernatural benefactors78 to their human charges. The fairy godmother figure is derived79 from the three Fates who were thought to visit a newborn baby and bestow80 good or ill fortune upon it, such as in the Sleeping Beauty tale. The fairy godmother is a wholly benevolent character, however, while the Fates were capable of causing good or evil to occur. Gail Carson Levine explores the possibility of a harmful gift from a fairy godmother in her Cinderella novel, Ella Enchanted.Return to place in story.
It never entered the fox s head that even foxes can be outwitted, so after a bit he consented to go with her; but he hadn t gone far before the cunning girl seized a stick, and gave him such a blow with it on the head, that he dropped down dead on the spot
The interscalene block targets the brachial plexus between the anterior and middle scalene muscle, lateral to the carotid artery and internal jugular vein, directly above the clavicle.Complications associated with the interscalene block include phrenic nerve blockade with an incidence near 100 percent[26,27], sympathetic chain blockade causing Horner’s syndrome, inadvertent injection in the vertebral artery, recurrent laryngeal nerve blockade causing hoarseness, and peripheral neuropathy[28].Rare complications include pneumothorax, epidural injection, intrathecal injection leading to total spinal anesthesia, spinal cord damage, and dorsal scapular or long thoracic nerve injury.Due to the high incidence of phrenic nerve blockade, the interscalene block is contraindicated in patients with severe pulmonary disease due to elevated risk of respiratory compromise.In an otherwise healthy individual, respiratory compromise is uncommon and the block is well-tolerated.
Supraclavicular block
The supraclavicular block targets the brachial plexus superior to the clavicle at the level of the trunks and divisions.It involves the C5-C7 distribution from the more superficial and lateral branches which supply the shoulder, lateral aspect of arm, and forearm, as well as the deeper and more medial contingent branches of C8 and T1 which supply the hand and medial aspect of forearm.Adequate spread of local anesthetic in both areas is necessary for successful nerve block of the arm and hand[25].The supraclavicular block involves injection of local anesthetic between anterior and middle scalene muscles at the level of the first rib, where the subclavian artery crosses posterior to the midpoint of the clavicle.
The supraclavicular block results in anesthesia of the upper limb that includes the shoulder because all the trunks and divisions of the brachial plexus are tightly packed and can be anesthetized at this location.Due to the density and extent of the supraclavicular block, it is colloquially known as the “spinal of the arm”.Indications of this nerve block include surgery of the hand, forearm, elbow, and arm.The proximal medial side of upper arm is spared since that is supplied by the intercostobrachial nerve (T2), which can be anesthetized separately.
They are small in stature26, yet somewhat larger than the Elf, being the size of children three years [old], gray and old looking hairy men and clad in moss (230)
Complications associated with supraclavicular block include pneumothorax (0.6% to 6.1%) as the apical pleural is in close proximity to the nerve block.The prevalence of pneumothorax can reach 0% with proper ultrasound usage[29].Other complications of the supraclavicular block include phrenic nerve blockade resulting in hemidiaghragmatic paresis (17% to 50%) and recurrent laryngeal nerve blockade leading to hoarseness in (22 %)[30,31].
Infraclavicular block
To perform iPACK block the needle is inserted in the medial thigh under ultrasound guidance.Typically, a total volume of 15-20 cc of a local anesthetic solution is utilized for this block.During the performance of this block, it is important to avoid inadvertent local anesthetic spread to the tibial or common peroneal nerve, which may result in undesirable motor weakness[88].
The infraclavicular block involves the injection of local anesthetic surrounding the axillary artery below the clavicle.Under ultrasound guidance, the local anesthetic is injected surrounding the axillary artery in a U-shaped pattern covering the all three cords of the brachial plexus.The infraclavicular block has a low prevalence of pneumothorax at 0.7%[32].
Axillary block
The axillary block is performed at the level of the branches of the brachial plexus.It anesthetizes the median nerve, the ulnar nerve, the radial nerve, and the musculocutaneous nerve, resulting in anesthesia of the upper limb from mid-arm extending distally to the elbow, forearm, and hand.It is to note that this block does not block the axillary nerve; rather the name of this regional technique is derived from the approach.In order to perform this block, the patient is positioned supine with the arm abducted to 90 degrees.Under ultrasound guidance the median, ulnar and radial nerve are identified surrounding the axillary artery.The nerve bundles are surrounded by three muscles-the biceps is located anterior and superficial, the coracobrachialis is located anterior and deep and the conjoined tendon of the teres major and latissimus dorsi is located medial and posterior.The musculocutaneous nerve is located between the fascial layers of coracobrachialis and biceps muscles.If required, the medial side of upper arm can be blocked separately.The axillary nerve block carries the risk of hematoma formation and intravascular injection, due to its close proximity to the axillary artery and vein.The need to abduct the arm to perform this block may be difficult with certain upper extremity injuries.In such case, other upper extremity blocks such as supraclavicular block can be utilized.
BLOCKS FOR LOWER EXTREMITY ORTHOPEDIC PROCEDURES
Neuraxial blocks for lower extremity procedures
Neruraxial anesthesia results in the blockade of sympathetic, motor, and sensory nerves, which leads to unopposed parasympathetic tone.Major physiologic effects of neuraxial anesthesia include hypotension, bradycardia, hypothermia, nausea and vomiting, and high neuraxial blockade leading to respiratory depression[33,34].There are several benefits to using neuraxial anesthesia for lower extremity orthopedic surgery that include reduced incidence of deep venous thrombosis in patients undergoing hip and knee replacement surgery, decreased intraoperative blood loss and transfusion requirements, and improved postoperative cognition[2,3,35,36] .Decreased intraoperative blood loss is likely due to a reduction in venous pressure from the sympathetic blockade.Multiple studies have showed that neuraxial anesthesia reduces the risk of postoperative deep venous thrombosis by at least 50%[36].
Spinal anesthesia
Spinal anesthesia is used for orthopedic procedures including total knee arthroplasty (TKA) and THA.Spinal anesthesia is usually performed with the patient in the sitting position while being continuously monitored.Also, it can be performed in the lateral decubitus position when the patient’s condition does not permit sitting.
The complications and adverse effects associated with spinal anesthesia include: high spinal anesthesia, inadequate or failed spinal anesthesia, nerve injury, urinary retention, postdural puncture headache, transient neurologic symptoms, infection, and spinal-epidural hematoma
Epidural anesthesia
Epidural anesthesia and analgesia can be utilized as an effective technique to either supplement general anesthesia or as the primary anesthetic approach for lower extremity orthopedic surgical procedures.Moreover, epidural anesthesia may be supplemented with peripheral nerve blockade to decrease postoperative pain.Common indications for epidural anesthesia in orthopedic surgery include THA, TKA, foot/ankle surgery, and major knee surgery.
Epidural anesthesia is better suited for elderly patients with cardiac comorbidities that limit their ability to tolerate the sudden sympathetic blockade and the resulting hypotension associated with spinal anesthesia[37,38].An epidural catheter may be incrementally dosed to slowly obtain an adequate surgical anesthetic level, thereby decreasing major rapid fluctuations in blood pressure[39].Additionally, the epidural catheter can be continuously dosed during the surgery and may remain in place postoperatively for analgesic purposes[39].
The adductor canal block has been evaluated for its potential analgesic use in patients undergoing ACL reconstruction.The adductor canal block has theoretical advantages for this patient population, including preserved quadriceps strength fulfilling the requirements of short hospital stay and immediate mobilization for outpatient ACL reconstruction.Currently, the data has been inconsistent in supporting the routine use of the adductor canal block over the femoral nerve block for ACL reconstruction with regards to analgesic equivalence; as such, the femoral nerve block for ACL reconstruction remains an appropriate option[60,76-78].
Serious complications of epidural anesthesia are extremely rare (0.03%), but can be potentially devastating[42].These complications include epidural hematomas, epidural abscesses, nerve damage, infection, and cardiovascular instability[42].Absolute contraindications to epidural anesthesia include patient refusal, local infection at puncture site, and severe coagulation disorders.Relative contraindications include sepsis, elevated intracranial pressure, anticoagulant use, bleeding disorders, fever, aortic stenosis, pre-existing neurologic injury, prior spine surgery, and placement in anesthetized individuals[43].
COMBINED SPINAL-EPIDURAL
The CSE anesthetic is a technique which combines many of the benefits of epidural and spinal anesthetics in a single approach.It may be utilized in patients undergoing lower extremity orthopedic procedures who require surgical anesthesia with the added ability to add epidural anesthetics for intraoperative or postoperative uses[44].As with alternative neuraxial techniques, the CSE may be utilized for patients undergoing hip and knee arthroplasty, femur fractures, major knee surgery, and foot/ankle surgery[45].
This technique is performed by injecting an anesthetic solution in the subarachnoid space (coaxial needle placementepidural needle), followed by placing an indwelling epidural catheter.The CSE technique provides the rapid onset of spinal anesthesia with the prolonged and flexible duration of an epidural catheter[46].With the CSE technique, surgical anesthesia is achieved rapidly, saving 15-20 min compared to epidural anesthesia[44].The epidural catheter may be left in place to supplement inadequate spinal anesthesia, prolong surgical anesthesia, and to provide postoperative pain control[44].
A mist of sadness clouded the king s mind, and he said to his son: If this thing is so, I will in the first place send a courier with friendly letters to King Quimus, and will ask the hand of his daughter for you
The CSE can be used in high-risk patients, in order to facilitate careful titration of epidural anesthetics after surgical anesthesia is initiated with a reduced dose of intrathecal local anesthetic[44].This can prevent sudden decreases in systemic blood pressure.
Caution should be exercised when intrathecal or epidural long-acting opioids are administered, due to the risk of delayed respiratory depression[47].The success rate of CSE is higher than has been demonstrated with epidural anesthesia alone[44].There is a theoretical risk that the epidural catheter may migrate or is non-functioning, which will only be discovered once the spinal blockade begins to diminish, thereby necessitating conversation to general anesthesia[44].Overall, the CSE remains an excellent anesthetic and analgesic technique in patients undergoing lower extremity orthopedic surgery.While the combined spinal-epidural approach has several benefits over spinal or epidural anesthesia, there is a risk that the epidural may become dislodged during patient positioning.This may not be detected until later in the case, as the spinal anesthetic will provide reliable anesthesia for the first portion of the case, and may mask a poorly-functioning epidural.This may necessitate the administration of sedatives or the conversion to general anesthesia depending on the surgical case.Patients should be considered fall-risks until their neuraxial anesthetic has completely worn off.Moreover, return of motor function often occurs prior to the recovery of functional balance.As such, the first ambulation following neuraxial anesthesia should be performed with caution.
He cried so much that the glass splinter swam out of his eye; then he knew her, and cried out, Gerda! dear little Gerda! Where have you been so long? and where have I been? And he looked round him
LOWER EXTREMITY PERIPHERAL NERVE BLOCKS
Peripheral nerve blocks may be utilized either as the primary anesthetic modality or as adjuncts to general or neuraxial anesthesia.Due to anatomical limitations in successfully achieving adequate surgical anesthesia through peripheral nerve blockade, lower extremity nerve blocks are typically utilized as an adjunct to general or neuraxial anesthesia.Advances in regional anesthesia have allowed for increased applications of peripheral nerve blocks while minimizing potential side effects such as undesirable motor blockade[16].A summary of lower extremity peripheral nerve blocks is included in in Table 3.

Femoral nerve block
The sciatic nerve may be blocked in several locations, depending upon the region of the limb requiring anesthetic blockade.The anterior approach of the sciatic nerve block is performed on the proximal medial thigh.The transgluteal approach is performed on the posterior buttock, between the ischial tuberosity and greater trochanter.The subgluteal approach is performed posteriorly on the gluteal crease.Commonly, the sciatic nerve block is performed at the level of the popliteal fossa, known as the “popliteal block”.
The femoral nerve block has been reported to effectively reduce pain and assist with rehabilitation after TKA[48,49].Patients who received femoral nerve block for knee surgery had fewer unplanned hospital admissions during outpatient surgery [50].At one major academic center, patients who underwent anterior cruciate ligament (ACL) repair with the assistance of regional anesthesia for postoperative pain control were able to bypass the PACU 82% of the time and were able to avoid hospital admission 96% of the time; both of these values translated into significant hospital cost savings[51].
Absolute contraindications to femoral nerve block include patient refusal and allergy to local anesthetics.Relative contraindications to femoral nerve block include concurrent anticoagulation use, coagulopathy, previous ilioinguinal surgery, local infection, preexisting femoral neuropathy, or large inguinal lymph nodes[16].
Anatomically, the femoral nerve is the largest branch of the lumbar plexus and arises from the ventral rami of the L2-L4 spinal nerve roots[16].It enters the femoral triangle directly inferior to the inguinal ligament and lies lateral to the femoral artery[52].The femoral nerve splits distally to the anterior and posterior divisions.The anterior division, gives rise to the medial femoral cutaneous nerve while the posterior
division gives rise to the saphenous nerve.
The femoral nerve provides sensory innervation to the anterior thigh and medial aspects of the calf, foot, and ankle[16].The femoral nerve additionally provides motor innervation to muscles of the lower extremity, including the quadriceps, sartorius, and pectineus muscles.As such, the femoral nerve block will cause weakness of the quadriceps muscles[53-55].This may result in decreased patient mobility and may potentially increase the risk of falls.Thus, patients should not be ambulating without assistance after a femoral nerve block[18].
Of course not, said the old man. But, if it did, you need not worry. She would never divorce you. Oh, no! And, of course, she will never give you the least, the very least, grounds for-uneasiness.
The quadriceps weakness associated with the femoral nerve block has decreased its clinical use for providing post-operative analgesia for patients undergoing TKR.Motor-sparing regional anesthesia techniques are often favored for these patients, such as blocks targeting the saphenous nerve which provides sensory innervation to the anterior and medial aspects of the knee[56,57].Weakness induced by a femoral nerve block may be assessed by manual muscle testing[58].Recommendations to minimize post-operative falls in patients receiving this block include utilizing ambulationassistive devices, patient and staff education, and considering post-operative immobilization until muscle strength is regained[16].Data supports the use of femoral nerve block over adductor canal block for ACL reconstruction, despite the increased risk of quadriceps weakness[59,60].
The femoral nerve block is often well-tolerated by patients, as the needle only traverses through the skin and adipose tissue of the inguinal region.Complications associated with the femoral nerve block are rare, and include nerve injury, intravascular injection, and quadriceps weakness[61].The femoral nerve block is performed by positioning the patient in a supine position with the targeted limb placed slightly abducted and externally rotated.The femoral nerve is identified lateral to the femoral artery.The femoral nerve is located deep to the fascia lata and fascia iliacia, and superficial to the iliopsoas muscles.
Fascia iliaca block
The fascia iliaca block is a regional anesthetic technique which provides anesthesia to the femoral nerve and lateral femoral cutaneous nerve[62].It is used in patients who have sustained traumatic hip fractures or for analgesia following hip surgery.This block may be performed pre-operatively while the patient is awaiting their surgery, and has been shown to provide rapid analgesic benefit[63].Moreover, patients reported improvements with passive hip flexion, which allowed them to sit up in bed pre-operatively[64].Faster time to fascia iliaca block has been shown to reduce opioid use, pain, and hospital length-of-stay in patients with hip fractures[65].Pain relief after fascia iliaca block has been shown to be superior to systemic intravenous opioid therapy and this block can be performed upon presentation to the emergency department[66].The fascia iliaca block may also assist with optimally positioning these patients for spinal anesthetic placement for surgical femur fracture repair[67,68].
The adductor canal block provides effective analgesia for surgery to the knee and medial aspect of the lower extremity.It may be used as part of a multimodal analgesic pathway for patients undergoing TKA to facilitate earlier ambulation, improve patient comfort, and enhance patient satisfaction[72].Over half of the patient’s undergoing TKA will likely experience moderate-to-severe post-operative pain which can subsequently result in increased length-of-stay, immobility-related complications, and decreased patient satisfaction[73].As a result, safe and effective regional anesthetic techniques are of paramount importance to these patients[73,74].
Saphenous nerve block
The saphenous nerve block is indicated for various lower extremity orthopedic procedures involving the knee, foot, or ankle.It may be used as a sole nerve block, or in conjunction with the sciatic nerve block to provide increased anatomical coverage for surgery to the medial aspect of the foot and ankle[16].The saphenous nerve block results in sensory anesthesia of the medial aspect of the leg down to the foot and ankle.
There are various approaches to performing a block of the saphenous nerve.With the use of ultrasonography, the saphenous nerve block is often performed subsartorially at the adductor canal; hence, this block is referred to as the “adductor canal block”.Alternative locations to perform a saphenous nerve block include the femoral triangle, the medial femoral condyle, or the level of the tibial tuberosity.
Adductor canal block
The fascia iliaca block is performed by injecting a relatively large volume of local anesthetic (20-30 cc) under the fascia iliaca above the level of the inguinal crease.The goal of this block is to spread local anesthetic laterally to the iliac spine and medially to the femoral nerve, and is typically performed under ultrasound-guidance[62].The femoral nerve and lateral femoral cutaneous nerve lie deep to the fascia iliaca, and as such, are blocked during this injection[69-71].The femoral nerve component provides blockade to the anterior and medial thigh, and the lateral femoral cutaneous nerve component provides anesthesia to the anterolateral thigh.
While the femoral nerve block can provide effective analgesia for patients undergoing total knee arthroplasty, it can be associated with quadriceps muscle weakness which may increase the risk of falls[18].As a result, the adductor canal block is often a favorable alternative used for post-operative analgesia for patients undergoing TKR[56,57].Compared to the femoral nerve block, the adductor canal block results in significant quadriceps motor sparing and significantly preserved balance while still maintaining a similar degree of postoperative pain relief[53-55].This allows for effective pain control with the ability to promote early mobilization and ambulation post-operatively[75].
With the advent of peripheral nerve blockade, the role of epidural analgesia strictly for postoperative pain has been decreasing in use.When comparing epidural analgesia with peripheral nerve blockade in patients who underwent TKA, a meta-analysis showed equivalent pain scores and morphine consumption between both groups up to 48 h postoperatively (Fowler, SJ 2008)[40].Additionally, the use of epidural analgesia was associated with a higher incidence of urinary retention and hypotension, suggesting that peripheral nerve blockade provides equivalent postoperative analgesia with a favorable side-effect profile[40,41].
The adductor canal block can be combined with various other regional techniques to increase the overall distribution of analgesia[16].A limitation of the adductor canal block as a sole nerve block is that it will only produce anesthesia to the anteromedial side of the knee[73].Patients undergoing knee surgery report improved pain relief by combining the adductor canal block with periarticular injections of local anesthetic by the surgeon[79-81].The addition of the iPACK block may offer patients improved pain relief and earlier ambulation by providing anesthesia to the posterior capsule of knee[82].
Complications from an adductor canal block are rare and potentially include bleeding, infection, and nerve damage[83].It is important to note that while the saphenous nerve block is a sensory nerve block, an injection of a large volume of local anesthetic into the adductor canal may result in a partial motor block of the vastus medialis due to a blockade of the femoral nerve’s branch to the vastus medialis[84].As a result, caution must be exercised with patients ambulating without support after receiving an adductor canal block.
The adductor canal block has widely become the standard of care for analgesia for total knee arthroplasty.The downside to the adductor canal block is that often times direct sonographic visualization of the saphenous nerve is not achieved; rather, local anesthetic is deposited within the anatomic region of the adductor canal.It is likely that motor-sparing blocks will increase in their use for a wide array of lower extremity surgical procedures, especially in the ambulatory surgical setting.
It was covered, and neither the servant nor anyone else had any idea what was on it, for the King never removed the cover or partook of the dish, till he was quite alone
iPACK block
The iPACK block has been increasingly utilized in TKA to provide analgesia to the posterior compartment of the knee without compromising lower extremity strength.It targets the medial and lateral superior genicular nerves to provide adequate posterior knee capsule analgesia[85].The combination of the iPACK block with the ACB provides a larger distribution of anesthetic coverage, by ensuring both anteromedial and posterior joint coverage[73,86].
Recent data indicates the iPACK block, used in conjunction with the adductor canal block and periarticular injection for TKA, substantially decreased pain at rest and on ambulation postoperatively[82,87].This resulted in earlier hospital discharge, decreased opioid requirements, and earlier ambulation[82].
The infraclavicular block t argets the brachial plexus at level of the cords before the branching of the axillary and the musculocutaneous nerves.It results in anesthesia of the upper limb below the shoulder, including the arm, elbow, forearm and hand, sparing the medial proximal upper arm, which is supplied by intercostobrachial nerve (T2)[25].
The IPACK block can be quite uncomfortable for awake patients to undergo, given the needle positioning and needle depth.As such, in certain patients, this block may be performed after the patient has been sedated in order to facilitate proper needle placement.It is likely that in the future the IPACK block will be utilized in combination with the adductor canal block as the standard of care for providing “circumferential” analgesic coverage for knee surgery.That being said, caution should be exercised to the total volume of local anesthetic utilized in order to avoid inadvertent local anesthetic systemic toxicity.
Sciatic nerve block
The sciatic nerve block is indicated for lower extremity orthopedic procedures involving the foot, ankle, and posterior knee.The sciatic nerve block may be used as a singular block, as in the case of an achilles tendon repair, or in conjunction with the femoral or saphenous nerve block to obtain anesthetic coverage for knee surgery or foot/ankle surgery, respectively[16].The sciatic nerve is formed from the anterior rami of L4 to S3 and is the largest nerve in the body[89].The terminal branches of the sciatic nerve are the tibial nerve and common peroneal nerve.The sciatic nerve block provides anesthesia to the posterior aspect of the knee, hamstrings, and the entire limb below the knee (motor and sensory innervation), with the exception of medial lower extremity and foot, which is supplied by the saphenous nerve.
The femoral nerve block is indicated for lower extremity procedures involving the anterior aspect of the thigh and medial aspect of the leg below the knee.Common uses of the femoral nerve block include providing analgesia for TKA, anterior cruciate ligament reconstruction, quadriceps tendon repair, surgery to the foot, and surgery to the ankle.The femoral nerve block may be combined with other regional anesthetic techniques, such as the sciatic nerve block, to expand the distribution of the anesthetic block, particularly below the knee[16].
Popliteal block
Peripheral nerve blocks (PNB) entails injecting a local anesthetic (LA) solution in proximity to a specific nerve or nerve bundle to produce a sensory and motor blockade of a specific region of the body.The LA blocks the transmission of painful impulse to the central nervous system.PNB can be used for surgical anesthesia or postoperative analgesia.It is commonly administered as a single shot, but a continuous infusion catheter can be placed to prolong the postoperative analgesic effect.PNB is commonly performed under ultrasound guidance to reduce the risks of intraneural and intravascular injection of LA, avoid peripheral nerve trauma, and to ensure proper delivery of the LA for a successful block.Upper extremity nerve blocks are performed at the level of the brachial plexus.Depending on the surgical site, various nerve blocks can be performed at different levels of the plexus.These blocks include interscalene block, supraclavicular block, infraclavicular block, and axillary block.Lower extremity nerve blocks include femoral nerve block, saphenous nerve block, Sciatic nerve block, iPACK (Infiltration between the Popliteral Artery and Capsule of the Knee) block, ankle block, and lumbar plexus block.
Potential complications from the sciatic nerve block are rare, and include nerve injury, bleeding, and intravascular injection[92].Nerve injury may be manifested as a persistent foot drop with potential pressure necrosis[16].
The popliteal sciatic nerve block is performed with the patient in the supine position with the affected limb placed in an elevated position with the assistance of blankets or towels for positioning.The knee joint is slightly flexed, and the ultrasound transducer is placed on the posterior aspect of the knee within the popliteal crease.Caution should be exercised to avoid entering the nerve bundle or inadvertently injecting the popliteal artery.
Ankle block
The ankle block can be performed to provide anesthesia to the foot.All types of foot surgery can be performed with the ankle block, including forefoot reconstruction, bunionectomy, osteotomy, and amputation.The ankle block is effective for providing pain relief for foot fractures, soft tissue injuries, and gout.The ankle block has several benefits over alternative regional techniques.It is performed through anatomic landmarks, and does not require ultrasonography to perform; however, data suggests that the addition of ultrasound-guidance may improve the clinical efficacy of the ankle block[93].The ankle block is motor-sparing; however, the ankle block may result in mild impairment to ambulation.
The ankle block is performed by blocking the five peripheral nerves at the level of the ankle.The medial aspect of the foot is innervated by the saphenous nerve, which is a branch of the femoral nerve.The remainder of the foot is innervated by branches of the sciatic nerve—the sural nerve, the posterior tibial nerve, the superficial peroneal nerve, and the deep peroneal nerve[94].
Compared to the ankle block for forefoot surgery, the popliteal block provided improved analgesia and decreased opioid requirements in the immediate postoperative period[95].
However, no studies exist yet that show how or why. These here are five different organizations that classify carcinogens. And as you can see, none of the organizations consider the compounds to be safe, which justifies the need to decrease them in our diet. Now you might wonder how a 13 year-old girl could come up with this idea. And I was led to it through a series of events.
Contraindications to the ankle block include local infection, burn, soft tissue injury, scarring, or distorted anatomy in the region of the block.Potential complications of the ankle block are rare, and include bleeding, infection, and nerve damage[96].
The ankle block is often underutilized as a technique to provide analgesia to the midfoot and forefoot.As it does not require ultrasound to perform, it can be reliably performed in settings which may not be equipped with an ultrasound.Moreover, it may be performed upon presentation to the emergency room for providing pain relief for foot fractures or soft tissue injury, as part of a multimodal analgesic plan.The ankle block may also be performed by the surgeon intraoperatively for post-operative analgesia.
Lumbar plexus block
The lumbar plexus block is indicated for lower extremity procedures and has been shown to be useful for hip surgery, including arthroplasty and fracture repair.By performing this regional anesthetic, blockade of the femoral, obturator, and lateral femoral cutaneous nerve can be achieved.Various techniques have been described for this block.The ultrasound-guided shamrock technique, first described in 2013, provides sufficient sonographic visibility of the target plexus[97].In this technique, an ultrasound-probe is placed in an axial orientation cephalad to the iliac crest approximately along the posterior axillary line.The lumbar plexus block can be combined with the sacral plexus block to provide effective anesthesia for hip surgery; this provides for an alternative to spinal anesthesia which may cause prolonged periods of hypotension[98].
With the advent of alternative regional anesthesia techniques, the lumbar plexus block has seen a decrease in clinical use.These peripheral blocks are often performed with greater ease and reliability by most anesthesiologists, and are better tolerated by patients.Moreover, the potential for serious complications is higher for the lumbar plexus block when compared to alternative peripheral nerve blocks.The fascia iliaca block can be utilized as an alternative for analgesia after hip surgery and has been shown to provide non-inferior pain relief[99,100].In Addition, the fascia iliaca block is often easier to perform from a technical perspective, which may lead to its increased use[99].Studies have shown that peripheral nerve blocks for patients who have sustained a traumatic hip fracture can reduce pain on movement and decrease the risk of developing pneumonia[101].As such, it is important to perform a technique, such as the fascia iliaca block, which can be mastered by most clinicians without advanced specialized regional anesthesia training.However, because of the decreasing utility of the lumbar plexus block, residency training programs often do not emphasize the teaching of this block.
The lumbar plexus block has the potential for causing serious complications, including inadvertent epidural spread resulting in high neuraxial anesthesia, hypotension, local anesthetic toxicity, bleeding, hematoma formation, infection, and nerve damage.In order to minimize these complications, large volumes of local anesthetic should be avoided in patients with multiple comorbidities.During performance of this block, patients should be continuously monitored for unilateral sympathectomy or hypotension due to epidural spread[102].Deformation or degeneration of spinal anatomy and musculature may result in poor ultrasound image quality, potentially leading to failed blockade[103].
COMPLICATIONS OF REGIONAL ANESTHESIA
Local anesthetic systemic toxicity
Local anesthetic systemic toxicity (LAST), is a potentially life-threatening complication that may result from unintentional intravascular injection of local anesthetic or slow absorption of an inappropriately high dose of local anesthetic injected perineurally.The ASRA publishes practice advisories for the management of patients who experience LAST[104].
And what do you suppose this favour turns out to be--when I have been cajoled into promising14 to grant it? Nothing more nor less than a request that I will take back all my gifts-- since, says my young madam, if I have the good fortune to please you, how am I to know that it is really I, myself? And that s how it will be all my life long, whenever I meet anybody
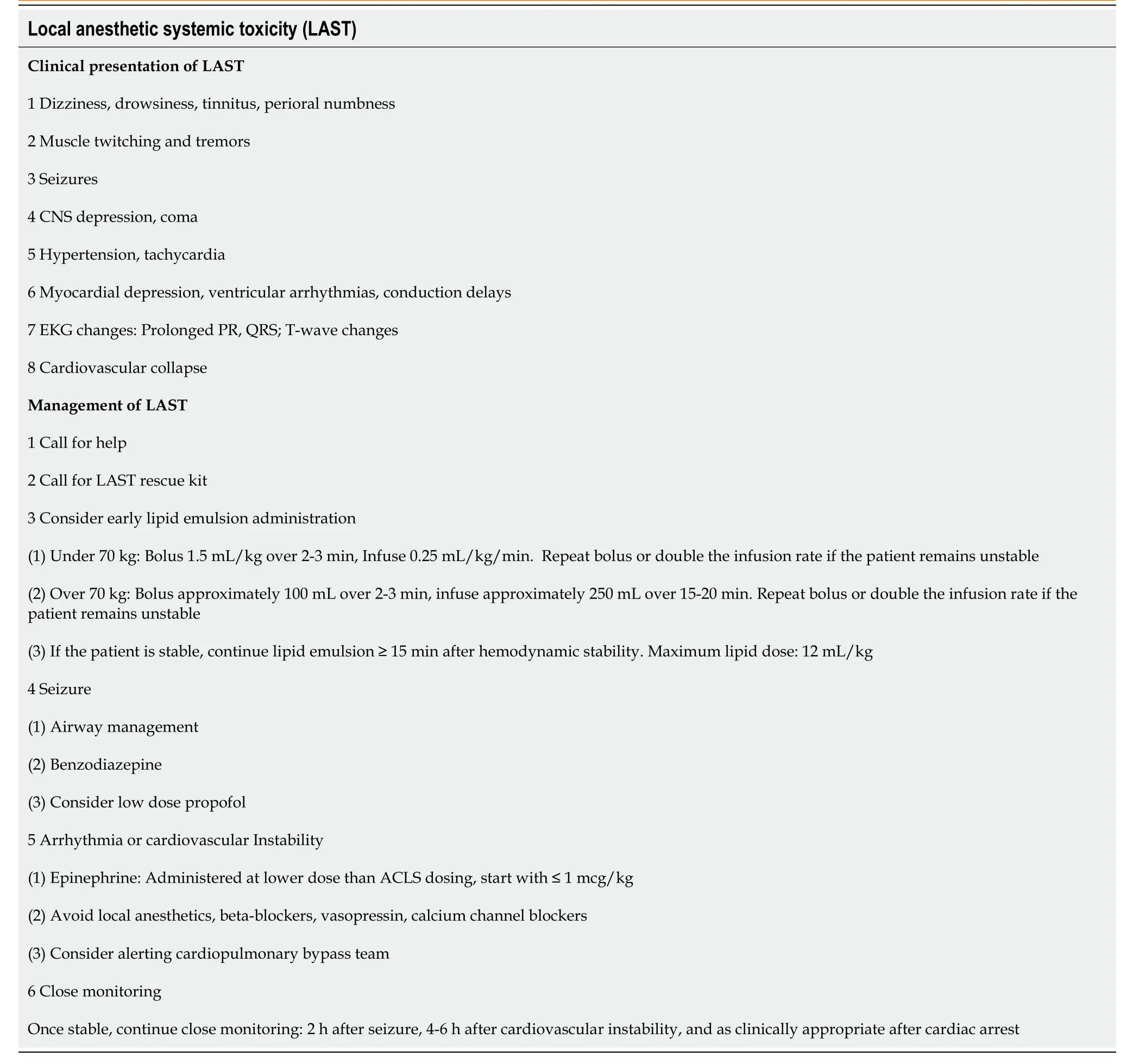
The clinical presentation and speed of onset of LAST are extremely variable.Signs and symptoms of toxicity may immediately become apparent; however, they may take as long as 30 min or more to occur[105].Symptoms typically present as a continuum; neurologic toxicity occurs at lower concentrations followed by cardiac toxicity at higher concentrations.
Early clinical signs of neurotoxicity are subjective, and include dizziness, drowsiness, perioral numbness, and tinnitus[105].These signs may be missed if the patient is sedated or under general anesthesia.Following this, with increasing plasma concentrations, muscle twitching and tremors are observed.As blood and brain levels of local anesthetic continue to increase, generalized tonic-clonic seizures occur.Finally, generalized central nervous system (CNS) depression occurs leading to a reduced level of consciousness and coma[106].
2. Woodcutter: Woodcutter was one of the lowliest, least paying occupations (Matthews 1962). Jack48 Zipes explores the tale as a story of triumph of the working or plebian class over the higher class. The family is ultimately victorious49 over poverty and the witch -- who like the richer and higher classes -- has more than enough storage of food and treasure that could be shared to lessen50 the suffering of the lower classes. The hatred51 which the peasantry felt for the aristocracy as hoarders and oppressors is represented by the killing52 of the witch (Zipes 1979). Return to place in story.
Cardiotoxicity follows a two-step pathway[107].In early cardiotoxicity, activation of the sympathetic nervous system results in hypertension and tachycardia.Following this, myocardial depression occurs leading to ventricular arrhythmias, conduction delays, contractile dysfunction, and eventual cardiovascular collapse.Inhibition of myocardial voltage-dependent sodium channels by local anesthetics may lead to a noticeable increase in the PR interval and QRS duration, as well as the presence of subtle T wave abnormalities[107].
Treatment of LAST begins with the recognition of the early signs and symptoms of toxicity, followed by immediate intervention including early administration of intravenous Intralipid emulsion.Intravenous Intralipid emulsion has been postulated to function by acting as a lipid sink to extract lipophilic local anesthetic from plasma and tissues[108].It additionally functions directly on myocardial tissue by improving cardiac output[109].Intralipid should be administered as a weight-dependent bolus followed immediately by an infusion[106].Boluses may be repeated, and the infusion rate may be doubled if the patient continues to remain unstable[104].The infusion should be continued for at least 15 min after obtaining hemodynamic stability[104].
CNS instability such as seizures should be appropriately managed with intravenous benzodiazepine administration or low doses of propofol[104].Cardiovascular collapse should be managed with careful titration of intravenous epinephrine.Individual boluses of less than 1 mcg/kg should be administered to avoid ventricular fibrillation or tachycardia[104].ACLS dosing of epinephrine (1 mg) may result in poor long-term outcomes due to the increased risk of arrhythmogenicity.A summary of the clinical presentation and treatment of LAST is presented in Table 4.
Risk factors for LAST include extremes of age, low muscle mass, female gender, and patients with cardiac, liver, and metabolic comorbidities[110].The ASRA recommendations for preventing LAST include the use of ultrasound, use of the lowest effective dose, incremental injections, aspiration before each injection, and the addition of epinephrine when employing potentially toxic doses of local anesthetic[110].The presence of epinephrine within the local anesthetic solution may cause a transient increase in heart rate if injected intravascularly, thus alerting the clinician of inadvertent intravascular injection.The risk of LAST increases with the administration of large volumes of local anesthetic to perform multiple nerve blocks at the same time.For example, patients who undergo blockade of the saphenous (adductor canal block) and sciatic (popliteal block) nerves may receive a large combined total volume of local anesthetic.As such, extreme caution should be administered to the individual and combined doses of local anesthetic, especially when there are plans to administer further local anesthetic within the surgical field intraoperatively by the surgeon.It is important to utilize the minimum effective dose of local anesthetic required to perform the nerve block.
Prevention of LAST remains a cornerstone of safe administration of regional anesthesia.Checklists and treatment algorithms of LAST should be prominently displayed in any area where regional anesthesia nerve blocks are performed, and resuscitation equipment and medications should be immediately available if required[111,112].Due to the life-threatening nature of LAST, prompt diagnosis and management of LAST should be frequently reviewed and reinforced with the use of simulation[111].All personnel, including surgical staff, nursing staff, and anesthesia staff should be trained in recognizing and treating LAST if they work in a perioperative setting where peripheral nerve blocks are performed.Moreover, resuscitative medications should be well-marked and easily accessible by all members of the treatment team.
Block failure
Regional anesthesia is often effectively utilized as the primary anesthetic or as an adjunct for postoperative analgesia; however, despite these benefits, it has an inherent failure risk even in the most experienced hands.Block failure is manifested as inadequate anesthesia or analgesia in the targeted region.This may result in poorlycontrolled pain, delayed surgical schedule, subjecting the patients to repeated block attempts, or unanticipated conversion to general anesthesia.
Certain technical variables have been found to be the cause of certain block failures.Injection of anesthetics outside of the neurovascular sheath prevents appropriate spread to the target nerve.Additionally, the utilization of a high threshold for stimulation when using a nerve stimulator technique may lead to an increased rate of failed blocks[17].The experience level of the anesthesiologist performing the block has been reported to impact the performance of a regional anesthetic[113].It is important to optimize all patient variables for increasing the rate of success.This can be achievedby proactively taking measures to optimize patient positioning with towels or pillows, using ultrasonography if available, and to take into account anatomic variation.Current graduating anesthesiology residents are receiving advanced training in peripheral nerve blockade, and are likely to be well-versed in the use of peripheral nerve blockade, which will likely decrease the rate of block failure.
One study noted that regardless of block type, patients with a body mass index (BMI) greater than 25 kg/mare more likely than those with lower BMI to experience non-surgical anesthesia; moreover, the rate of block failure increased incrementally with BMI[17].This is likely due to the difficulty in identifying anatomical landmarks in these patients.Additionally, patients who were an American Society of Anesthesiologists class IV physical status experienced a higher degree of block failure[17].
Block failure may also occur in patients who undergo placement of continuous peripheral nerve block (CPNB) catheters.One study noted the incidence of failure for continuous peripheral nerve block with the supraclavicular approach to be 26%, the highest among the blocks evaluated[114].The infraclavicular approach was noted to have a lower failure rate, likely due to anatomical characteristics which allow for a more stable catheter placement with a lower rate of dislodgement[114].Areas with more stable anatomy, with limited range of motion, may minimize the amount of undue traction placed on catheters resulting in lower rates of catheter dislodgement.
Several mechanisms have been implicated in CPNB failure, including catheter insertion techniques, anatomic variation, and equipment malfunction.The CPNB catheter may have initially been incorrectly placed in relationship to the target nerve, or the catheter can migrate post-placement[115,116].Other causes of CPNB failure include dislodgement or obstruction of the of the catheter tubing[117].Leakage of local anesthetic solution after dislodgement may potentially increase the risk of LAST or rarely may even cause myonecrosis[114].Further upstream, the infusion pump may malfunction or disconnect, causing leakage of local anesthetic solution[118].Genetic variations in certain patients may result in abnormal metabolism of local anesthetic, which may cause inadequate sensory blockade[119].Lastly, pain is a subjective multifactorial entity.Thus perception of pain may be affected by psychological factors including anxiety and pain-sensitivity, especially in the perioperative period[114].
The advent and increased clinical use of ultrasound-guidance has been shown to increase success rates and improve the quality of sensory blockade[120].Also, ultrasound-guidance has been shown to shorten block procedural times by reducing the number of needle passes required to localize the target nerve[121].
The overall success of any regional anesthesia technique relies on the ability to correctly identify the nerves or nerve plexus involved in the surgery and place an adequate dose of local anesthetic surrounding the nerve structures.Advances in the field of regional anesthesiology have led to an increase in the use of regional anesthesia with the addition of novel block techniques, especially with the use of ultrasound-guidance[110].Given the increasing use of peripheral nerve blockade, anesthesiology training programs have drastically increased their emphasis on mastering regional anesthesia skills, leading to the development of anesthesiologists with a strong skillset of performing safe and effective peripheral nerve blocks[122].The risk of block failure should be discussed with the patient prior to performing the nerve block, so they are aware of this potential occurrence.As part of this discussion, it is beneficial to review alternative analgesics (, alternative blocks, intravenous, and oral medication) that may be administered if the block provides limited pain relief.It is important to utilize alternative methods of analgesia for patients who experience block failure.Consideration should be given to performing an alternative nerve block, if the first block technique fails while considering the total dose of local anesthetic used.
Nerve injury
Peripheral nerve injury is rare following regional anesthesia.Although the definition of injury varies between studies, the incidence of persistent symptoms of nerve dysfunction may be as high as 8 to 10 percent in the days following the block[123,124].The majority are transient, lasting days to months.Major complications resulting in permanent (greater than six months) nerve damage ranges between 0.015 and 0.09 percent[125-127].Incidence of nerve injury associated with continuous catheters is around 0.21 percent[118,128].Most nerve injuries are believed to occur secondary to intraneural injection.Intrafascicular injections, particularly at high pressure, are felt to result in greater risk of nerve damage[129,130].To minimize the incidence of intrafascicular injection, injection of anesthetic should be halted if the patient feels a paresthesia (shooting pain), or if the pressure required for injection is greater than usual.Appropriate spread of the anesthetic should be observed when ultrasoundguidance is used.Preexisting nerve pathology (including diabetes) may make a nerve more susceptible to injury.Continuous visualization of the block needle using ultrasound is presumed to decrease the risk of intrafascicular injection, but does not decrease the risk of nerve injury.Also, nerve injury can also occur as a direct effect of certain LA medications[131].
Symptoms of nerve injury are primarily sensory (pain, tingling, or paresthesias), but can include any combination of motor or sensory deficits depending on the nerve involved and severity of the injury.Most symptoms resolve within six months; if symptoms are either severe or persistent, the patient should be referred to a specialist for further evaluation and testing.
Hematoma
Inadvertent puncture of nearby vascular structures can lead to hematoma formation.It is important to avoid performing PNB’s in patients with an abnormal coagulation status in anatomic locations in which application of pressure to the puncture site is not possible.The vast majority of hematomas may be controlled with direct pressure to the needle puncture site; rarely, surgical decompression may be required.
Allergic reaction
Most adverse reactions to LAs are non-allergic.However, two different types of allergic reactions to LAs have been described: allergic contact dermatitis and delayed swelling at the site of administration within 72 h, and rarely anaphylaxis.
Infection
Infection risk for single-shot peripheral nerve block is negligible and for peripheral catheters is low (0 to 3.2 percent)[132].Risk of infection is increased in critically ill patients, admission, trauma patients, immune compromised patients, males, and the absence of antibiotics.The risk of infection may be minimized by removing the catheter within 48 to 72 h of placement.
Fall risk
Certain lower extremity nerve blocks may result in muscle weakness which can secondarily increase the risk of post-operative falls[133].
Local anesthetic-induced central nervous system toxicity (toxic left hemispheric syndrome)
Recently, severe stroke-like symptoms following intrascelene block has been reported after interscalene block.Patients had typical hemispheric symptoms in the absence of cerebral vessel occlusion.Hemispheric syndrome in the reported cases occurred in the ipsilateral side of the interscalene block.The proposed mechanism of injury in these cases was apoptotic cell death due to local anesthetic neurotoxic effects.Patient presented with impaired consciousness, slow-wave EEG activity in the affected hemisphere, epilepsy, global aphasia, dysphagia, dysarthria, facial palsy, hemiparesis, pyramidal tract signs, and complex behavioral manifestations.No abnormal computed tomography or magnetic resonance imaging (MRI) imaging was observed in the immediate postoperative period.MRI imaging abnormalities were appreciated postoperative days 1 through 5 in some patients which included hyperintensity of cortical grey matter and basal ganglia.Hospital stay ranged from 9 to 19 d with patient requiring mechanical ventilation for airway protection.Most patients experienced gradual improvement of the functional outcome after a prolonged course of rehabilitation but still has residual symtpoms[134].
CONCLUSION
Regional anesthesia is one of the cornerstones of successful perioperative orthopedic management.In addition to providing superior anesthesia for orthopedic procedures, regional anesthesia provides superior analgesia with relatively fewer side effects compared to systemic analgesia modalities.Perioperative team awareness of regional anesthesia fundamentals is one essential step towards improving clinical outcomes, lowering health care costs, and sustaining higher patient satisfaction scores.
ACKNOWLEDGEMENTS
The authors would like to thank Dr.Jon Livelsberger, DO for editorial comments and insights.
 World Journal of Orthopedics2022年1期
World Journal of Orthopedics2022年1期
- World Journal of Orthopedics的其它文章
- Three-dimensional printing in paediatric orthopaedic surgery
- Management of proximal biceps tendon pathology
- Should we use similar perioperative protocols in patients undergoing unilateral and bilateral one-stage total knee arthroplasty?
- Epidemiology and incidence of paediatric orthopaedic trauma workload during the COVID-19 pandemic: A multicenter cohort study of 3171 patients
- Can bedside needle arthroscopy of the ankle be an accurate option for intra-articular delivery of injectable agents?
- High-resolution, three-dimensional magnetic resonance imaging axial load dynamic study improves diagnostics of the lumbar spine in clinical practice