
High-resolution, three-dimensional magnetic resonance imaging axial load dynamic study improves diagnostics of the lumbar spine in clinical practice
2022-01-22 08:44TomaszLorencMarekGobiowskiWojciechMichalskiWojciechGlinkowski
World Journal of Orthopedics 2022年1期
INTRODUCTION
Lower back pain (LBP) remains a major worldwide public health problem that has increased substantially over several decades[1].The problem of LBP affects epidemiology[2-5], health economics[6,7] and social aspects (disability, inability to work, limited daily activity)[8].LBP is a common problem affecting most adults at some point during their lifetime[3,4,9].More than half of the population may experience a pain relapse within a year, and 8% of people will have chronic pain[10].In their systematic review, Meucci[11] revealed that chronic LBP prevalence was 4.2% in individuals aged between 24 and 39 years.The LBP prevalence equals 19.6% between 20 and 59 years of age and increases linearly from the third decade of life until 60.Chronic LBP is a significant contributor to the global disability burden[12].Disability besides pain due to LBP is reported frequently and continues to be the leading cause of years lived with disability[13].
The vertically-oriented human spine acts as a dynamic and static column connecting the skeletal system.Substantial forces act on the longitudinal axis of the spine in the human’s upright position.Spinal compression is traditionally considered the primary biomechanical mechanism associated with work-related LBP[14,15].Human erect position can lead to increased axial compression in the lumbar spine and several side effects, including back pain.The lifting of objects raises the axial compression in the lumbar spine and increases LBP risk[16-19].
1. Castle: According to Jack11 Zipes, the original Grimms manuscript did not mention a castle and offers an ambiguous setting. The later versions of 1812 and 1857 have integrated the castle and made the princess a more obviously wealthy and spoiled child (Zipes 1983).Return to place in story.
The classic works of Nachemson[20,21] from the early 1960s showed that the highest degree of intradiscal pressure in the lumbar spine occurs in standing and sitting positions, mainly when a person leans forward.The intradiscal pressure is lower when an individual is in the lying position than in the sitting and standing positions[22].These observations were confirmed by Rohlmann[23,24] using wireless measurement.Schonstrom[25] showed that the intradiscal force difference measured at rest and axial loading acting on the spine reaches 500 N on human spine segments.The difference in intradiscal pressure observed in the spine segments is comparable to the values found in volunteers subjected to different loads and different body positions[21].
Correct, quick and precise determination of the underlying causes of back pain symptoms is crucial for many patients.Imaging for LBP is considered appropriate when clinical suspicion of severe pathology or surgery addresses a specific pathology[26,27].Imaging may also be used to diagnose chronic LBP; however, particular indicators for appropriate imaging use are less well defined, with pain lasting longer than 6 weeks being an indicator for imaging in some guidelines but not in others[26].Axial compression imaging may improve the diagnostics in clinical management of LBP and improve appropriate treatment decisions[28-30].
Even though the highest spinal loading occurs in the upright and sitting positions, a typical magnetic resonance imaging (MRI) examination is performed with the patient lying supine when no loads are exerted on the spine.As a result, the lying position of the examined patient poses a limitation on magnetic resonance tomography.An attempt at overcoming MRI limitations caused by the patient being in a lying position led to the introduction in clinical practice of an examination performed in the supine position with axial loading, simulating physiological loading.The load distribution among lumbar spinal structures, in general, is still an unanswered question and should be the focus of biomechanical testing.Previous studies showed that axialloaded MRI could simulate the standing position and reveal additional valuable pathological findings not detected by conventional recumbent MRI[31,32].Compressive loads on the vertebral discs are not the only ones occurring in the spine; load indicators other than disc compression are at least equally relevant, so attention should be paid to them.Few studies simultaneously investigated several anatomical structures in the lumbar spine using upright, open and low-field MRI[33] or axial loaded MRI[16].However, these studies did not use dynamic three-dimensional (3D) high-resolution images and failed to measure the ligamentum flavum area, foraminal area and lumbar lordosis.
Moreover, previous studies were performed in a young, small group of asymptomatic volunteers[33], or simultaneous measurements were not correlated between the sets of variables[16].No study has simultaneously compared dural sac size, ligamenta flava thickness, foraminal dimensions and lumbar sagittal alignment between axial-loaded and recumbent MRI in a large group of LBP patients to identify dynamic changes and associations between morphology and demography.Therefore, this study’s objective was to evaluate and measure the changes presented by MRI of selected lumbar spine structures upon axial-loading compared with recumbent MRI and correlate them to morphologic changes and demographic data.Additionally, the study aimed to assess the value and potential use of axial loading in lumbar spine examinations.The detailed evaluation seems crucial for spinal surgery decisionmaking.The spinal injections or transforaminal[34,35] or interlaminar spinal endoscopy[36,37] can be used to relieve symptoms due to the intervertebral foramen narrowing or spinal canal stenosis caused by the thickening of the ligamentum flavum.
MATERIALS AND METHODS
We enrolled 90 patients diagnosed at the Magnetic Resonance Laboratory with LBP inclusion criteria as an indication.Exclusion criteria included significant spinal injury, osteoporosis, previous spine surgery, lack of good patient cooperation, a body mass below 40 kg and a lack of written consent from the patient.General contraindications for MRI examinations (, pacemakers, ferromagnetic implants, foreign bodies and claustrophobia) were also considered.A total of 46 (51%) men and 44 (49%) women were included in the study with an age and body mass index (mean ± standard deviation) of 49 ± 16 years and 26.0 ± 4.2 kg/m, respectively.The study was conducted according to the Declaration of Helsinki guidelines and approved by the Institutional Bioethical Review Board at Medical University of Warsaw (AKBE/100/13 — obtained on December 10, 2013).Informed consent was obtained from all subjects involved in the study.
Lumbar spine MRI examination protocol without and after axial loading
The examination was performed using a 1.5 T MRI (Ingenia; Philips Healthcare, Eindhoven, The Netherlands).After performing recumbent MRI examinations, axial loading was applied using an external commercially available nonmagnetic DynaWell (DynaWell L-Spine; DynaWell Diagnostics, Las Vegas, NV, United States) compression device.The phase without axial loading was identical to a standard lumbar spine examination.Both the axial-loaded and unloaded MRI examinations were performed with a 3D T2-weighted Volume ISotropic Turbo spin-echo Acquisition sequence (Table 1).According to previous disc pressure measurements[21] the chosen load was equal to 40%-50% of the patient’s body weight, with equal load distribution on both legs (20%-25% of patient body mass per leg).The patient was subjected to this load in the lying position for at least 5 min before the examination.
53.A golden spinning-wheel: Spinning wheels have long been important in folklore, especially in tales like Sleeping Beauty and Rumpelstiltskin. A spinning wheel is a small domestic spinning machine with a single spindle that is driven by hand or foot (WordNet). It is used to produce flax for cloth production, a traditionally feminine domestic chore.Return to place in story.
Image analysis
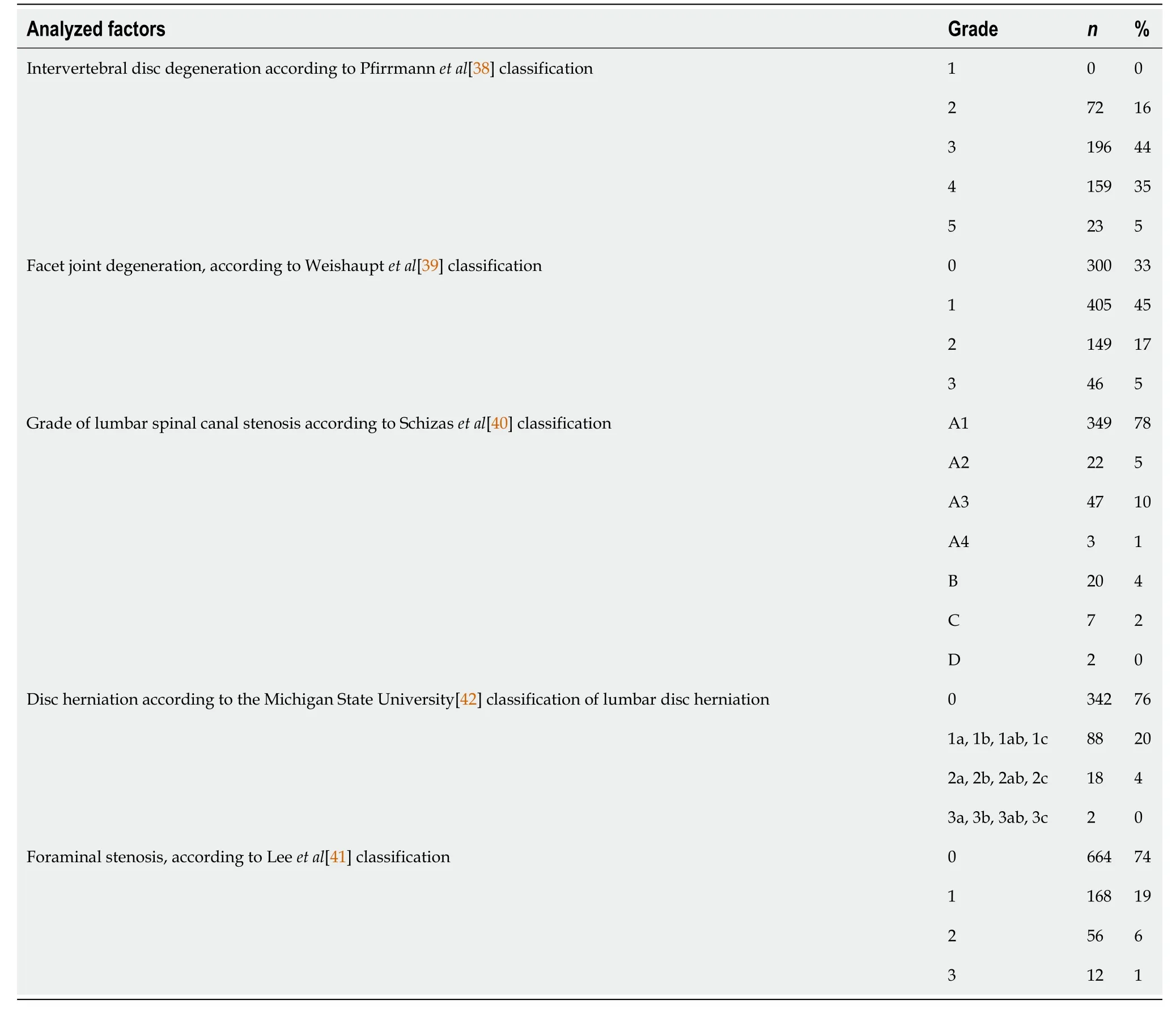
Images were assessed on a dedicated workstation (IntelliSpace Portal; Philips Healthcare, Eindhoven, The Netherlands) at a single center.Based on recumbent and axial-loaded MRIs, the lumbosacral angles between the superior vertebral endplate of L1 and superior vertebral endplate of S1 were measured, enabling the observation of spine adaptations at a whole lumbar level (Figure 1).The dural sac cross-sectional area was calculated for each level from L1-L2 to L5-S1 for examination with and without axial loading.Measurements were performed by encircling the dural sac transverse area, capturing T2-weighted MRI at the same levels for phases without and with axial loading with the plane precisely positioned parallel to the midplane of the intervertebral disc (Figure 1).The vertebral foramina sagittal cross-section area was determined for each level, from L1-L2 to L5-S1, on both sides.Measurements were performed by encircling the vertebral foramina area in sagittal cross-sections on the same levels for the phase with and without axial loading (Figure 1).The cross-sectional area of the ligamentum flavum was determined for levels from L1-L2 to L5-S1 on both sides.The measurements were captured by encircling the area of the ligamentum flavum in cross-sections at facet joint levels with and without axial loading (Figure 1).The degree of disc and facet joint degeneration, the degree of spinal canal stenosis, the degree of foraminal stenosis and the degree of disc herniation were assessed on recumbent images on all disc levels according to the classifications of Pfirrmann[38], Weishaupt[39], Schizas[40], Lee[41] and the Michigan State University classification of lumbar disc herniation[42].
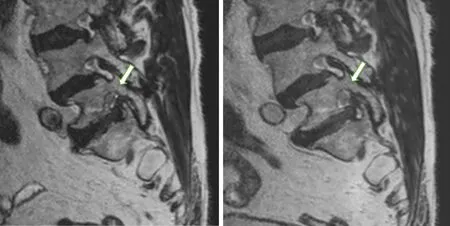
Intervertebral foramina are triangular or oval at the lumbar level and broader in the coronal than the sagittal plane.Measurements recorded by encircling the intervertebral foramina sagittal cross-sections were proposed as the most accurate[53].Our analysis of lumbar neural foramina showed that variation in the cross-sectional area of the neural foramen in the lumbar spine was significantly axially-loaded-dependent.We identified a statistically significant decrease in average percent foraminal area from recumbent to axially loaded at all levels except at L5-S1.Surprisingly, intervertebral foramina at L5-S1 widened after axial loading by 2%, on average (Figure 3).
The Prince s next idea for Potentilla s amusement was to cause a fleet of boats exactly like those of Cleopatra, of which you have doubtless read in history, to come up the little river, and upon the most gorgeously decorated of these reclined the great Queen herself, who, as soon as she reached the place where Potentilla sat in rapt attention, stepped majestically37 on shore and presented the Princess with that celebrated38 pearl of which you have heard so much, saying: You are more beautiful than I ever was
Statistical analysis
The assessment criterion used was the percentage difference of measured parameters with a 95% confidence interval (CI).A pairedtest was applied at an α = 0.05 level to verify the hypothesis regarding the statistical significance of changes observed.The Pearson correlation test was used to explore the mutual relations of the spine structural parameters.A pairedtest was applied to determine the relationship between age and sex for each measured parameter.The statistical methods of this study were reviewed by Wojciech Michalski from the Department of Mathematical Oncology, Maria Skłodowska-Curie National Research Institute of Oncology, Warsaw, Poland.The IBM SPSS Statistics (IBM Corp., Armonk, NY, United States) version 20 for Linux OS was used for statistical analysis.
RESULTS
Ligamentum flavum
Upon axial loading, the area of the ligamenta flava was statistically significantly increased on average by 3.8% (95%CI: 2.5%, 5.2%,< 0.001; Table 2).
Dural sac
Upon axial loading, the dural sac area significantly decreased on average by 5.2% (95%CI: 4.1%, 6.2%,< 0.001; Table 3).
Intervertebral foramen
The area of the intervertebral foramina decreased on average by 3.4% (95%CI: 2.7%, 4.1%,< 0.001) except for the L5-S1 section of the spine, which increased by 2.0% on average (95%CI: 0.5%, 3.9%,= 0.045; Table 4).
Lumbosacral angle
The lumbosacral angles increased, on average, by 7.7% (95%CI: 5.7%, 9.6%,< 0.001; Table 5).
Holding the Prince by the arms, not so much to do him honour as to restrain his impatience, they proceeded by slow degrees up the steps of the Temple, and when they at last reached the top he thought his long waiting must be at an end


Correlation analysis
Degenerative changes of the lu mbar spine are listed in Table 6.
Degenerative changes
A statistically significant correlation between exaggerated lumbosacral angle and age was found (Pearson correlation coefficient () = -0.253,< 0.05).The negative correlation indicated that axial force on increasing lumbar lordosis in older patients isless than in younger patients.Neither the area of the intervertebral foramina nor the area of the dural sac was correlated with age.Additionally, a percentage difference of the sagittal cross-section area of vertebral foramina, the cross-section area of the dural sac and ligamenta flava and the percentage difference of the lumbosacral angles did not significantly correlate with sexThe relationship testing between spine structure parameters did not deliver any significant association between any variables.



DISCUSSION
Compression devices can be applied to high-field units.Therefore, high-resolution, 3D MRI might be obtained.This advantage of recumbent axially loaded MRI creates possibilities in determining the precise measurements and making an accurate diagnosis.The upright MRI would be a theoretically ideal diagnostic tool to simulate the spinal column under physiological conditions, but those systems are low-field MRI, which provides low image quality.Other studies have simultaneously analyzed several anatomical structures in the lumbar spine using upright, open and low-field (0.5T1.5T in our study) MRI[33].
Contrary to our study, the previous study group was limited to young (any age in our study), less populated (1290 in our study) asymptomatic volunteers.No 3D high-resolution images and failure to measure several anatomical structures were reported.The proposed idea of applying axial-loaded MRI aimed to mimic as close as possible the load conditions occurring in the upright position.That position is currently impossible to apply in conventional recumbent high-field MRI.Devices intended for axial loading are commercially available and approved by the United States Food and Drug Administration.They also meet the New Approach Directive requirements of the European Union; yet, according to many authors, they are still in their experimental stage[43].As a result, biomechanical testing has focused on many spinal structures simultaneously.The load distribution among the dural sac, ligamenta flava, intervertebral foramina and lumbar sagittal alignment was considered in thisspinal biomechanical assessment.
Dural sac
The dural sac occupies the most significant part of the spinal canal.Therefore, spinal stenosis mainly affects the dural sac, narrowed in the highest grade from all structures filling the spinal canal (Figure 2).The cross-sectional dural sac area measurement provides the most precise assessment of the spinal canal, but its time consumption is the main disadvantage of this method[44].The results in this study showed that the mean dural sac cross-sectional area was significantly lower when loaded than relaxed at all lumbar spine levels from L1-L2 to L5-S1 (Figure 2).The rates of dynamic change were the highest at L4-L5 (mean of 8.1%; range of 5.7%-10.5%) and the lowest at L1-L2 (mean of 2.6%; range of 1.6%-3.6%).


The high sensitivity and specificity of axial-loaded MRI for detecting severe constriction were demonstrated by Kanno[32].MRI examinations under axial loading are highly relevant in detecting central stenosis of the spinal canal, as to be confirmed by results reported by other authors[45].Axial-loaded MRI demonstrated a significant reduction in the dural sac size and significant correlations of dural sac diameters with the upright myelogram.Therefore, axial-loaded MRI can be used to represent positional changes in dural sac size detected by upright myelography in patients with lumbar spinal canal stenosis[32].Numerousexperiments showed that axial loading results in spinal canal stenosis.
Schonstrom[25] specified that axial loading results in a spinal canal volume reduction in a spine segment, measured at an intervertebral disc level by about 40-50 mm.In their previous studies, the authors discovered that a pressure increase in the dural sac of spinal segments reduces the spinal canal area down to approximately 79 mm[46].Based on this discovery, contemporary authors assumed that 75 mmis the borderline value of the dural sac cross-sectional area.Below this value, the authors suggested a diagnosis of absolute stenosis, and the range of 75-100 mmindicates a diagnosis of relative spinal canal stenosis.Kim[47] arbitrarily defined a 10% reduction in the dural sac cross-sectional area as a significant reduction.They found a significant reduction in the cross-sectional area of the dural sac in 42% of patients, of which severe stenosis with a cross-sectional area lower than 75 mmwas found in 25% of patients.
The results in this study showed that the most significant foraminal constriction was by 6.7% (range of 5.5%-8.0%) under loading occurred at the L2-L3 level.Diagnostic benefits with a high grade of foraminal spinal detection could be achieved if inclusion criteria were limited to the suspicion of single spinal nerve involvement, as described by Splendiani[57].They detected foraminal spinal stenosis at 61 of 230 levels and called it “hidden” stenosis, as it was not revealed on conventional recumbent MR examinations; it was only detected on examinations performed with the patient in the orthostatic position.The authors also discovered that stenosis of the intervertebral foramen was never found either in the presence of normal intervertebral discs or in the absence of facet disease in either the clinostatic or orthostatic position[57].
Ligamentum flavum
The ligamenta flava fills the space between the vertebral arches.They run just behind the facet joint and act as an extra reinforcement of the joint capsule.The ligamenta flava thickens with age.The ligamenta flava thickening is connected to fibrous tissue hypertrophy, which is a result of cyclooxygenase-2 and transforming growth factorbeta expression[49,50].The changes are prominent in the dorsal part of the ligamenta flava, where the most potent axial load forces are observed[49].This study showed that the mean cross-sectional area of the ligamenta flava was significantly higher when loaded than relaxed at all lumbar spine levels from L1-L2 to L5-S1.The rates of dynamic changes were the highest at L2-L3 (mean of 4.8%; range of 2.0%-7.6%) and the lowest at L4-L5.
The huntsmen went in, and then came back and said, In the hollow tree there lies a wonderful animal that we don t know, and we have never seen one like it; its skin is made of a thousand pieces of fur; but it is lying down asleep
Some time ago during my vacation period, I had the pleasure of travelling to Europe to tour the various regions of France. Our tour group was comprised of forty-five travellers from a variety of countries. My three friends and myself made up the Canadian contingent1 on the bus.
According to the study of Hansson[45], it is not intervertebral discs but the ligamenta flava that have the most significant impact on spinal stenosis, being responsible for 50%-80% of spinal stenosis induced by axial loading.The case report of dynamic lumbar spinal stenosis with neurogenic claudication caused by the thickening of the ligamentum flavum, with MRI in decumbency, revealed no definite pathologic condition associated with symptoms[51].According to some authors, the pathogenesis of thickening of the ligamentum flavum is unclear, and whether ligamentum flavum thickening is due to tissue hypertrophy or buckling remains controversial.Some studies claimed that canal narrowing, in part, results from the hypertrophy of the ligamentum flavum.In contrast, others argued that the ligamentum flavum bulges inside the spinal canal and compresses nerve tissues[49,50,52].This information is relevant clinically because spinal stenosis may be underdiagnosed with regular MRI, and surgical intervention without adequate decompression may lead to poor outcomes.
Intervertebral foramen
One day, after about two weeks, Harry and I were talking and I told him about my theory. If you ll just wait long enough, I said, you ll see her coming up those stairs some day. He turned and looked at the stairs as though he had never seen them before.,,,。“,”,“,。”,。
Iwata[54] reported similar findings in computed tomography examinations using DynaWell equipment.They observed an enlargement of the intervertebral foramina area at the L5-S1 level and a simultaneous reduction in the intervertebral foramina area at L1-L2 levels to L4-L5 after axial loading.Conversely, MRI studies demonstrated a decrease in the foraminal area at all levels during weight-bearing in neutral, flexion and extension positions compared to unloaded supine imaging.The magnitude of change in the foraminal area increased as an angular motion at the segment increased.The most significant average percent decrease in the foraminal area occurs at L2-L3 and the smallest change at L5-S1, but a reduction at this level was still observed[53].Therefore, changes caused by a compression device in foraminal dimensions at L5-S1 do not simulate physiological standing conditions.
Suppose the different types of loading simulated by DynaWell equipment and those occurring in the standing position responsible for differences in foraminal stenosis observed in those methods have not yet been determined.The axial load may be transmitted to the feet and the buttocks in the supine position.A reaction force acts on the buttocks causing the posterior rotation of the pelvis.That results in a significant decrease in the pelvic angle during axial loading[55].According to Hioki[56], the disc wedge angles at the L5-S1 level with axial loading using DynaWell equipment differed from those in the standing posture.The magnitudes of changes were significantly smaller than in the standing position.They suggested that axial loading of the lumbar spine in the supine position decreases the angle between the L5 and S1[56].However, the L5-S1 angle did not significantly change in the standing posture than the controls in the supine position at rest.These observations of different lumbarpelvic angular behavior could correspond with an enlargement of the area of intervertebral foramina at the L5-S1 level observed in our study.An awareness of these phenomena is essential to allow clinicians to evaluate imaging results accurately.
Now the Simurgh had given the prince a diamond weighing thirty misqals, and he ordered this to the king, who at once recognised its value, and asked where it had been obtained
Danielson and Willen[31] described an additional significant decrease in the crosssectional area of the dural sac with axial-loading MRI as an area change more than 15 mm.They concluded that axial-loading MRI provided “additional, significant information” in 50 of 172 patients (29%).They also observed additional significant findings in 69% of patients with neurogenic claudication, 14% of patients with sciatica and 0% of patients with LBP[31].Of patients studied by Manenti[48], who were subjected to axial-loading MRI, 18 (45%) displayed cases of spinal canal stenosis emergence, 8 (20%) displayed cases of hernia enlargement, and 6 (15%) showed profound spondylolisthesis.
In three simple steps, I eliminated 90 percent of all my blind dates, including one recommended by my old friend Karen. She called one evening to tell me that she had become good friends with a beautiful girl who reminded her of me. She said she knew we would hit it off. Sorry, I said, you re ruled out by rule number two.
Lumbosacral angle
The spine is highly resistant to axial pressure.That resistance depends on the size and shape of the spine as well as spine curvatures.The human spine, at an early stage, consists of only one curvature: spine kyphosis.The following curvatures occur when the human develops the erected position: (1) At the cervical level: lordosis (cervical lordosis); (2) At the thoracic level: kyphosis (thoracic kyphosis); (3) At the lumbar level: lordosis (lumbar lordosis); and (4) At a sacral level: kyphosis (sacral kyphosis).
Curvatures in the sagittal plane make the spine more durable compared to the straight column.Therein one function of the lumbar lordosis is to provide a higher bearing resistance.Lumbar lordosis in the sagittal plane of the spine is unique only in the human population.It is not observed in any other animal.The changes in lordosis markedly affect the stabilizing sagittal moments.
Huang[58] reported that the mean lumbosacral angle was 37° in unloaded MRI examinations and increased to 39° after axial loading.Our lumbar spine biomechanics analysis also showed that axial loading increases lumbar lordosis.According to Hioki[56], lumbar axial loading with DynaWell in the supine position can simulate the lumbar spine position in the standing position.This loading device alters lumbar sagittal alignment differently from an upright standing position at the L5-S1 level.
Our results indicated that lordosis of the spine varies from the initial sagittal curvature by +7.7° after axial loading, responsible for more lordotic posture.Older patients show lower increases in lumbar lordosis when exposed to an axial force.As we observed a decreased elasticity of the spine in the older population, it is worth proposing axial-loading MRI as elasticity imaging: an innovative “elastography” method designed for the lumbar spine to explore the age of the spine, the percentile grids of degenerative changes.
22.In losing the drops of blood the Princess had become weak and powerless: The princess has apparently78 always depended on her mother s protection and guidance. Now that she has left it behind, she is no longer under anyone else s protection. Return to place in story.
Conversely, lumbar lordosis was more extensive after the axial load in the supine position compared to the standing position, according to Madsen[59].This intriguing observation that the lumbosacral angle was 6° larger in the supine position than in the standing position, as explained by the author, was due to patients leaning against MRI walls to maintain a safe position and immobility when standing.Meakin[60] suggested that patients in the standing position are exposed to additional bearing forces.Patients with a lumbosacral angle smaller than the mean in an unloaded examination tend to straighten the spine after additional bearing forces.Patients with a lumbosacral angle greater than the mean in an unloaded examination were observed to increase lumbar lordosis after additional bearing forces.
Correlation analysis
Simultaneous measurements of the percentage difference of the sagittal cross-section area of vertebral foramina, the cross-section areas of the dural sac and ligamenta flava as well as the percentage difference of the lumbosacral angles offered new information.According to our data, a statistically significant correlation exists between exaggerated lumbosacral angle and age (= -0.253,< 0.05).A negative correlation was found and showed that older patients have a lower increase in lumbar lordosis when exposed to axial force, similar to that found in the spine in the standing position.The percentage difference of the sagittal cross-section area of vertebral foramina, the cross-section areas of the dural sac and ligamenta flava, as well as the percentage difference of the lumbosacral angles, did not significantly correlate with each other and sex.
And the Porcelain Maiden agreed to follow him, and after having given up her clothes, the young man bought a small horse for her, which went like the wind
Limitations
This study has significant limitations.The research’s main limitation is that all patients in the study were referred for MRI examinations for LBP, and there was no asymptomatic healthy control group.These results may not apply to asymptomatic, dynamic foraminal or spinal stenosis in the healthy population.Another potential limitation is that the inter-rater assessment has not been calculated.The force equal to half the body weight may not necessarily represent the lumbar spine load while standing.There may be a bias of data in the comparison between axial loading and standing conditions.Further comparative analyses between standing and axiallyloaded MRI findings in the supine position would provide more clinically relevant information.
Another source of weakness in this study was the lack of computational approach in automatic image recognition based on machine learning and deep learning to ease radiological measurements of the lumbar spine.However, it is within the scope of our scientific interests, and we hope to expand artificial intelligence in image recognition and segmentation to automate lumbar spine assessment and to obtain a good level of clinical prediction.In our opinion, high resolution 3D imaging will make automatic image recognition more accurate.We showed in this study, that high resolution 3D MRI is feasible under axial compression.Volume ISotropic Turbo spin-echo Acquisition techniques have been used to acquire high-resolution, contiguous, thinsection isotropic images for complex spine anatomy and replace several twodimensional acquisitions.The voxels generated by the 3D acquisition are submillimeter and measure the same in each direction, allowing the images to be reformatted with equal resolution in any direction.
CONCLUSION
The lumbar spine MRI is one of the most frequently performed examinations of all MRIs, but the MRI does not correlate significantly with back pain causes.The current study may help clinical practice understand spine physiology exposed to external forces, better-clarifying indications for axial load, and help identify the relationship between imaging examination results and perceived symptoms.A comparative evaluation of images obtained before and after axial loading of the spine showed changes in lumbosacral angles between L1 and S1, the dural sac cross-sectional area, the sagittal cross-sectional area of the intervertebral foramina and the cross-sectional area of the ligamentum flavum.Consistency in detecting central stenosis and ligamenta flava thickening between studies supports using an axial load of 50% body weight to simulate relaxed standing in the supine position.Changes in foraminal dimensions at L5-S1 do not affect physiological standing conditions.Axial loading intensifies the narrowing of the intervertebral foramina.Applying an axial compressive load increases lumbar lordosis, whereas the smallest changes were observed in older patients.
The Fairy finally made Narcissus promise that he would remain invisible when he was with the Princess, since she felt sure that this would make things easier for all of them
ARTICLE HIGHLIGHTS
Research background
Biomechanics of the individual lumbar spine structures are important since the overall spinal adaptation to compressive forces is comprised of the cumulative changes of respective elements.
Research motivation
There is a lack of works simultaneously comparing dural sac size, ligamenta flava thickness, foraminal dimensions and lumbar sagittal alignment between axial loaded and recumbent magnetic resonance imaging (MRI) in an extensive group of lower back pain patients.
Research objectives
To help the surgeons in the choice of the spinal endoscopy and spinal injections.The objective of the study was to evaluate the changes depicted by MRI of chosen lumbar spine structures upon axial-loading in comparison with recumbent MRI.
Research methods
The study covered 90 individuals assessed with three-dimensional volume isotropic acquisition MRI, first imaged in the supine position with no axial load and then again following application of an axial compressive load.Based on recumbent MRI as well as axial-loaded ones, the following were measured: the dural sac area, the ligamenta flava, the intervertebral foramina from L1-L2 to L5-S1 and the lumbosacral angle.
Research results
We found out that axial loading intensifies the narrowing of the spinal canal, thickens the ligamenta flava, narrows the intervertebral foramina from L1-L2 to L4-L5 and exaggerates lumbar lordosis.
Research conclusions
Our study reveals that there is a correlation between force compression and intensification of the lumbar spinal stenosis, intervertebral foramina narrowing, ligamenta flava thickening as well as increasing lumbar lordosis due to axial loading.
Research perspectives
There is a need to introduce computational approaches in automatic image recognition based on machine learning and deep learning to ease radiological measurements of the lumbar spine and obtain a good level of clinical prediction.Moreover, it is worth proposing axial-loading MRI as an elasticity imaging: an innovative “elastography”method designed for the lumbar spine to explore the age of the spine and the percentile grids of degenerative changes.
 World Journal of Orthopedics2022年1期
World Journal of Orthopedics2022年1期
- World Journal of Orthopedics的其它文章
- Three-dimensional printing in paediatric orthopaedic surgery
- Regional anesthesia for orthopedic procedures: What orthopedic surgeons need to know
- Management of proximal biceps tendon pathology
- Should we use similar perioperative protocols in patients undergoing unilateral and bilateral one-stage total knee arthroplasty?
- Epidemiology and incidence of paediatric orthopaedic trauma workload during the COVID-19 pandemic: A multicenter cohort study of 3171 patients
- Can bedside needle arthroscopy of the ankle be an accurate option for intra-articular delivery of injectable agents?