
Relationship of demoralization with anxiety, depression,and demographics of Chinese dialysis patients
2021-12-30 11:07:02CaiLanZHUANGJuanLianZHENGLeiGAOYingLingHUANGWenJingHU
Journal of Integrative Nursing 2021年4期
Cai-Lan ZHUANG, Juan-Lian ZHENG, Lei GAO,Ying-Ling HUANG, Wen-Jing HU
1Department of Nursing, Huizhou First Hospital, Huizhou,Guangdong Province, China; 2Dialysis Center, Huizhou First Hospital, Huizhou, Guangdong Province, China; 3Department of Nephrology, Huizhou First Hospital, Huizhou, Guangdong Province, China
ABSTRACT
Objective: The purpose of this study is to investigate the demoralization level of dialysis patients in China and analyze the influencing factors.
Materials and Methods: A convenience sample of 278 dialysis patients from a tertiary hospital participated in a cross-sectional descriptive study using a structured questionnaire including assessments of demographic data, Demoralization Scale-II (DS-II), and Hospital Anxiety and Depression Scale.The main analysis consisted of descriptive statistics, correlation coefficients, and multiple linear regression.
Results: The mean standard deviation DS-II score was 11.87 (7.72).Dialysis patients had a high level of demoralization.Findings from multiple linear regression indicated that demoralization was positively correlated with marital status (β = 0.141; P = 0.001), employment status(β = 0.113; P = 0.006), anxiety (β = 0.393; P < 0.001), and depression (β = 0.224; P < 0.001).These variables explained 57.1% of the variance in patient demoralization.
Conclusions: Demoralization is common in dialysis patients and is associated with marital status, employment status, anxiety, and depression.Health-care providers might regularly assess demoralization in dialysis patients, and develop related interventions to improve the quality of life.
Keywords: Anxiety, demoralization, depression, hemodialysis, peritoneal dialysis
INTRODUCTION
Chronic kidney disease (CKD) is currently defined as abnormalities of kidney structure or function that can progress to end-stage renal disease (ESRD) in which stage renal replacement therapies like kidney transplantation,hemodialysis (HD), and peritoneal dialysis are required.[1]It was estimated that the overall prevalence of CKD in China was 10.8% in 2012[2]and 16.4% in Chinese rural residents in 2019.[3]Due to the increasing prevalence of ESRD and limitations on accessibility and affordability of renal transplantation, the majority of patients depended on dialysis to maintain life.However, long-term frequent dialysis causes anorexia, fatigue,pruritus, sleep disorders, and other physical dysfunction,[4]as well as a massive economic burden, thus bringing tremendous psychological and mental pressure to those patients.[5]
Demoralization is a psychological state that has been described as helplessness, hopelessness, giving up, and subjective incompetence.[6]Consequently, patients with severe cases of demoralization may have a negative impact on quality of life, death anxiety, and major depression.[7,8]Importantly, it might engage in suicidal ideation.Demoralization shares similarities and co-occurs with depression.Indeed, some studies have pointed out that perceiving patients’ demoralization issues early can prevent the occurrence of depression effectively.[9]Depression is the most common psychiatric illness and a significant mortality predictor in ESRD.[10]Thus, dialysis patients are at heightened risk for demoralization.
Although previous studies have shown that demoralization is associated with age, education, economics, and marital status[11,12]and may occur in any type of clinical situation,such as life-threatening diseases, demoralization has not been extensively studied in Chinese dialysis patients.Therefore, the purpose of this study was to explore the level of demoralization and its association with demographic characteristics, anxiety, and depression in Chinese dialysis patients.
MATERIALS AND METHODS
Participants
We conducted a cross-sectional descriptive study.Participants undergoing peritoneal dialysis or HD were recruited through convenience sampling from a hospital-based dialysis center in Huizhou.Data were collected from April to August 2021.Patients were excluded if aged <18, received dialysis for <3 months, could not communicate in Chinese or express their own opinions, had refractory/untreated psychiatric disease or cancer, or refused to participate.
Measure
Data collection was conducted using a structured questionnaire including items assessing demographics (i.e.gender, age,marital status, education, monthly income, working status,and relationship status) and duration of receiving dialysis,Demoralization Scale-II (DS-II), and Hospital Anxiety and Depression Scale (HADS).
Demoralization Scale-II
The DS-II is developed from the initial version of the DS,comprising 24 items in 5 subscales.It is an improved and more practical measure of demoralization for research and clinical use with 16 items in 2 subscales: meaning and purpose,distress and coping ability.Each item is rated on a 3-point scale, ranging from 0 (never) to 2 (often); the total score varies between 0 and 32 points.A total DS-II score of ≥11 has been interpreted as a high level of demoralization.[13]The Cronbach’s alpha of the total scale was 0.89, and those of the two subscales were 0.84 and 0.82, respectively.[14]
Hospital Anxiety and Depression Scale
The questionnaire is a 14-item self-report scale consisting of two 7-item subscales, namely anxiety (HADS-A) and depression (HADS-D), which was developed by Zigmond and Snaith.[15]The questionnaire score ranges from 0 (no anxiety)to 3 (highest anxiety) for each question, with the higher scores indicating more severe anxiety and depression.Scores are widely used in the literature following classification: 0-7,no symptoms; 8-10, moderate levels of anxiety or depression;and 11-21, high levels of anxiety/depression.It has been proved with acceptable validity and reliability among Chinese people.[16,17]
Statistical analysis
Data input was performed using serial numbers, and analysis was conducted using SPSS 23.0 (IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY: IBM Corp).First,continuous variables were described by means and standard deviation (SD).Categorical variables were described by counts and percentages.Second, independent t-test and one-way analysis of variance (ANOVA) were used to examine differences in DS-II scores regarding demographic variables.Pearson’s correlations between the DS-II and HADS were examined.Third, multiple linear regression was performed to see the importance of each variable (R2), explaining demoralization.A significance level of P < 0.05 was established.
Ethical considerations
The participants were provided sufficient information of the research and were informed of the freedom to withdraw whenever they wanted without facing any negative consequences.Moreover, the confidentiality of the collected information and anonymity of individuals were assured.Verbal consent was obtained from all the participants prior to the study.
RESULTS
Totally, 278 dialysis patients participated in this study and completed the questionnaires.The demographic data and disease characteristics of the participants were shown in Table 1.More than half patients were male (53.6%), and the average age was 45.77 years.The majority were married (74.1%) and not working (55.0%).The independent-samples t-test and one-way ANOVA were used to test the differences in the DS-II scores of dialysis patients with different characteristics.The results showed that there were statistically differences in demoralization scores among patients living in different residences, with different marital statuses, education levels, employment status, primary caregivers, and receiving different monthly incomes (P < 0.05).These variables were then entered into the multiple regression analysis.
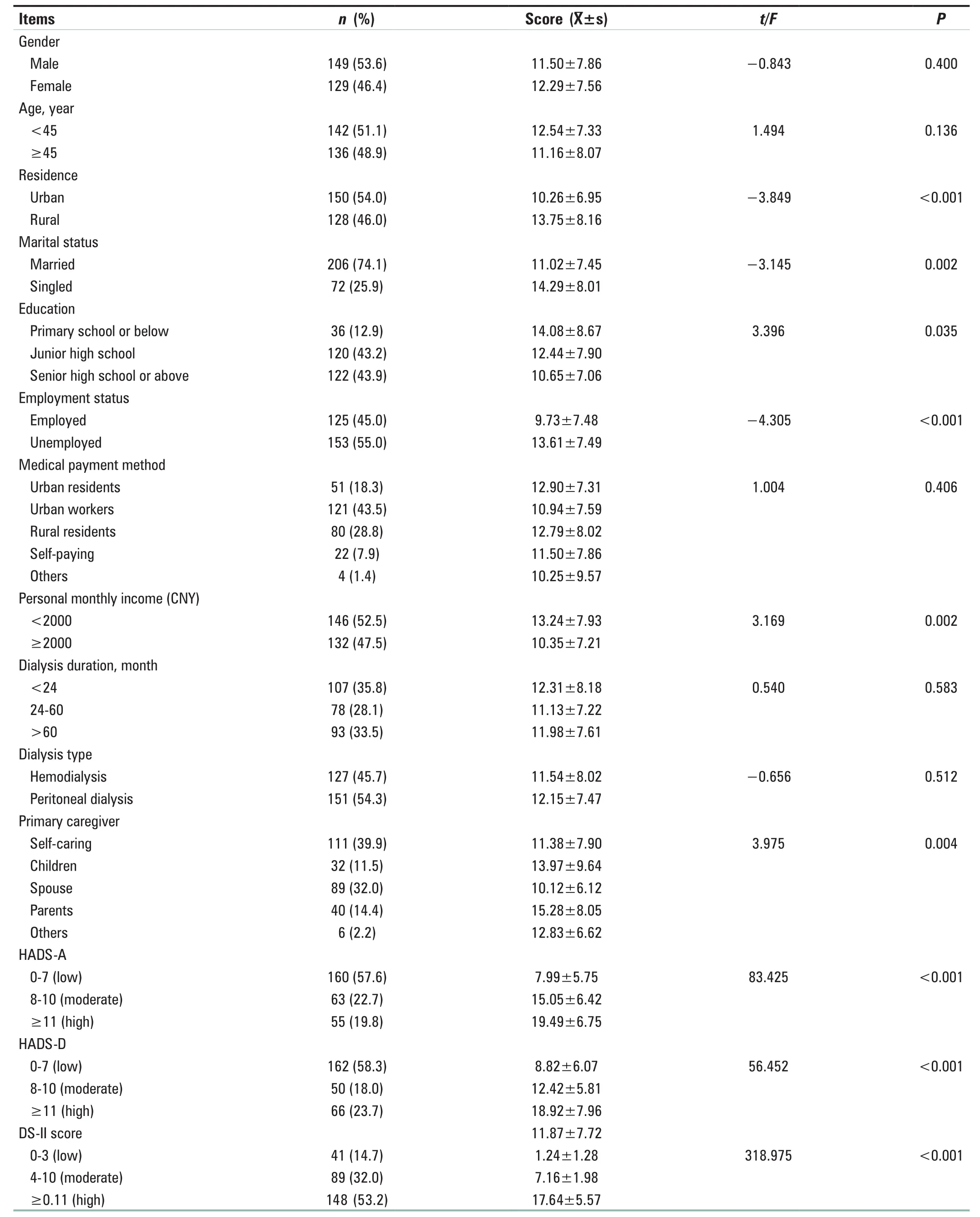
Table 1: Participants’ characteristics and their correlations with demoralization (n=278)
The mean (SD) DS-II total score was 11.87 (7.72) (range, 0-32),and the scores for each dimension were as follows: meaning and purpose 5.14 (4.10) and distress and coping ability 6.73 (3.95).Specifically, there were 53.2% of dialysis patientsgetting a high score of demoralization.Table 2 reported the means and SD of the HADS score; Pearson’s correlation analysis revealed that HADS-A and HADS-D were correlated with demoralization scores.

Table 2: Correlation analysis of demoralization and Hospital Anxiety and Depression Scale in dialysis patients (n=278)
The multicategory discontinuous variables and the assignment of independent variables were shown in Table 3.Multivariate linear regression analysis was used to identify factors related to demoralization [Table 4].The resulting model had an R2of 0.571.In this model, demoralization was positively correlated with marital status (β = 0.141;P = 0.001), employment status (β = 0.113; P = 0.006),anxiety (β = 0.393; P < 0.001), and depression (β = 0.224;P < 0.001).
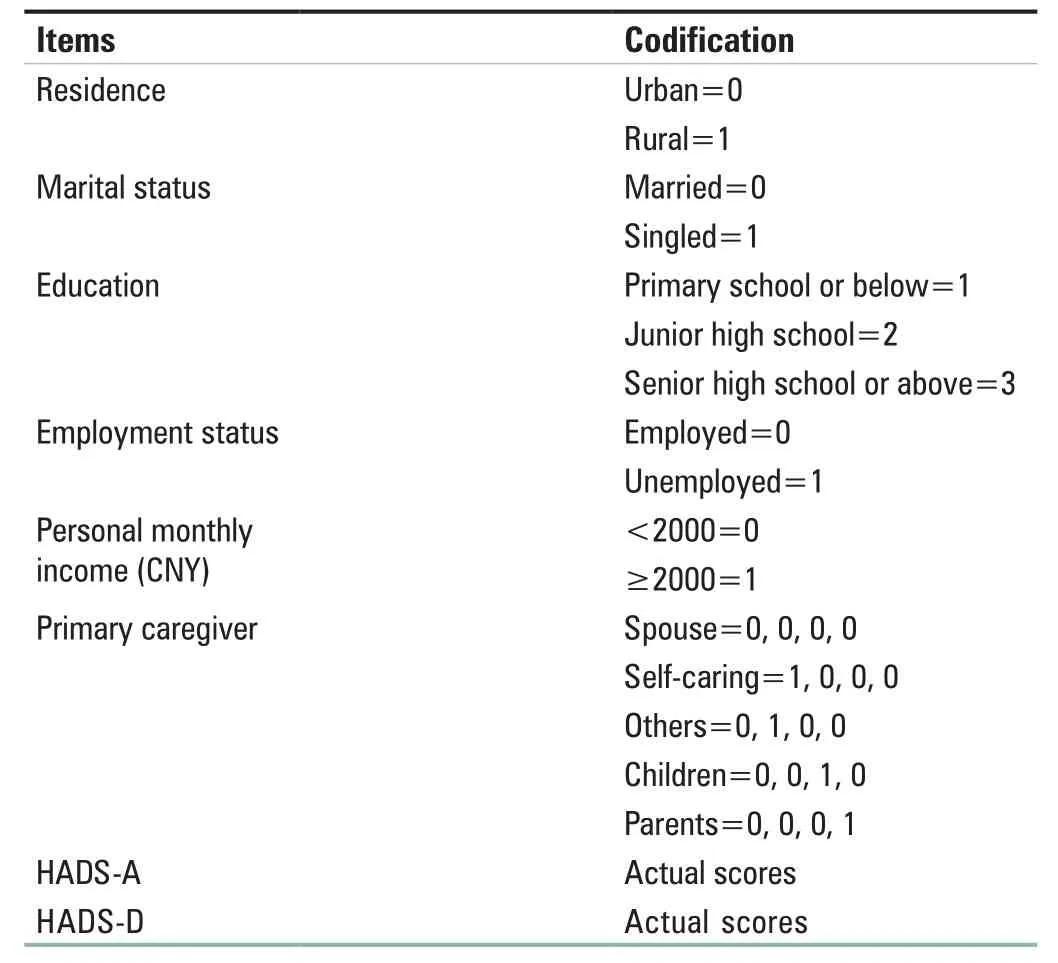
Table 3: Codification of variables included in linear regression models
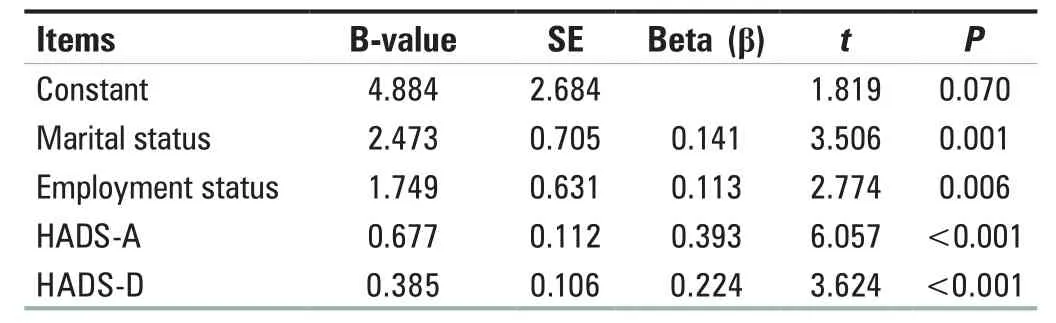
Table 4: Multiple linear regression analysis of demoralization of dialysis patients (n=278)
DISCUSSION
The main finding of this study is that demoralization is common among dialysis patients, approaching 53.2% of patients who got a DS-II score of >11.The total mean DS-II score in the present sample (11.87) was found higher than a study of 211 patients with cancer or other progressive diseases who were receiving palliative care (mean [SD],7.64 [6.43]).[14]The dimension with the highest score was distress and coping ability, indicating that the dialysis patients in this study were relatively dysphoria, disheartenment,and had a sense of incompetence.A previous study showed that demoralization is associated with stress and adverse health outcomes.[6]Although dialysis is an acceptable mode of renal replacement therapy, it does have its limitations,which include lower life expectancy, risk of infections, and metabolic disorders.[18]Long-term regular dialysis therapy can negatively affect their social, financial, and psychological well-being.Therefore, clinical health-care providers might regularly monitor demoralization among dialysis patients,as this would help in understanding how demoralization changes throughout the disease process.Furthermore,cognitive and supportive therapies may change patients’negative disease cognition and understand their beliefs about the meaning of life.
According to the results of multiple linear regression analysis,marital status, employment status, anxiety, and depression had significant correlations with demoralization.Around 57.1% of the variance of demoralization could be explained by these four variables.Moreover, these variables have shown a significant correlation with demoralization in previous studies.[19,20]The patients who were single, such as unmarried,divorced, and widowed, had a higher level of demoralization,which indicated that family support is a protective factor against high demoralization.Furthermore, family support is directly affected the mental health of dialysis patients,reduced the level of negative emotion, and improved the patients’ adherence to medical care as well as quality of life.[21,22]It is suggested that health-care providers should pay more attention to single patients in the future, determine the demoralization level of patients, and meet their spiritual health-related needs.
As in our study, a significantly lower level of demoralization was found in patients who worked full-time or part-time,which may be because staying on a job can benefit the patients in many ways, such as a source of social support, managed depressive symptoms, increased activity level, and reduced financial burden.[23,24]This suggests that dialysis facilities could set a convenient dialysis schedule for promoting gainful employment among dialysis patients.What’s more, social support programs such as spiritual care and employment counseling may lower some of the barriers to employment.
Anxiety and depression are the most common psychiatric disorders among patients undergoing dialysis.[25]Regarding anxiety, depression, and demoralization, it was found that patients with low levels of anxiety or depression had low levels of demoralization, which is consistent with a previous research.[26]In our study, we found a stronger correlation between anxiety and demoralization, while depression seems more closely to demoralization in previous studies.This could be explained by the use of different measurement tools, and the difference in patient characteristics.Moreover, depression and anxiety often coexist and share symptoms.This suggests that health-care providers should take more insight into the causes of anxiety symptoms, such as frequent alarms from the dialysis machines and decreased social support.[27]Encouraging patients to express their feelings and addressing their psychological needs may be an essential measure to confront psychiatric disorders.
Although we had a sizeable sample, the study was not representative of dialysis patients in China.The relevant sampling method limits the generalizability of results.Besides, qualitative research can be carried out to further understand the factors affecting patients’ demoralization to provide a reliable reference for demoralization intervention.
CONCLUSIONS
Dialysis patients exhibited a high level of demoralization.Multiple linear regression analysis suggested that marital status, employment status, anxiety, and depression were significant predictors of demoralization.The results provided implications for clinical health-care providers that early and appropriate assessment of dialysis patients’demographic characteristics and mental health is important for demoralization.Moreover, government authorities and medical institutions should improve related support systems and resources to benefit dialysis patients.Psychosocial intervention should be considered to investigate the effect on demoralization in dialysis patients in future studies.
Financial support and sponsorship
Nil.
Conflicts of interest
There were no conflicts of interest.
 Journal of Integrative Nursing2021年4期
Journal of Integrative Nursing2021年4期
- Journal of Integrative Nursing的其它文章
- Knowledge on malaria among caregivers with children aged under 5 years at Kenyasi Health Center
- Self-management of cataract extraction among diabetes patients
- A study on the correlation between function motivation and professional identity among nursing volunteers
- Application of five-element music therapy in pain coping skills training in patients with knee osteoarthritis
- Moxibustion plus acupuncture improves the efficacy and quality of life of patients with polycystic ovary syndrome:A randomized controlled trial
- lnsigni ficant small can still be mighty: Trend of chronic kidney disease in Nigeria