
Reduction of muscle contraction and pain in electroporation-based treatments: An overview
2021-08-02 07:47RobertaFuscoElioDiBernardoValeriaAlessioSimonaSalatiMatteoCadossi
Roberta Fusco, Elio Di Bernardo, Valeria D'Alessio, Simona Salati, Matteo Cadossi
Roberta Fusco, Elio Di Bernardo, Valeria D'Alessio, Simona Salati, Matteo Cadossi, Department of Medical Oncology, IGEA SpA, Carpi 41012, Modena, Italy
Abstract BACKGROUND In the first studies of electrochemotherapy (ECT), small cutaneous metastases were treated and only mild or moderate pain was observed; therefore, pain was not considered a significant issue. As the procedure began to be applied to larger cutaneous metastases, pain was reported more frequently. For that reason,reduction of both muscle contractions and pain have been investigated over the years.AIM To present an overview of different protocols described in literature that aim to reduce muscle contractions and pain caused by the electroporation (EP) effect in both ECT and irreversible EP treatments.METHODS Thirty-three studies published between January 1999 and November 2020 were included. Different protocol designs and electrode geometries that reduce patient pain and the number of muscle contractions and their intensity were analysed.RESULTS The analysis showed that both high frequency and bipolar/biphasic pulses can be used to reduce pain and muscle contractions in patients who undergo EP treatments. Moreover, adequate electrode design can decrease EP-related morbidity.Particularly, needle length, diameter and configuration of the distance between the needles can be optimised so that the muscle volume crossed by the current is reduced as much as possible. Bipolar/biphasic pulses with an inadequate pulse length seem to have a less evident effect on the membrane permeability compared with the standard pulse protocol. For that reason, the number of pulses and the voltage amplitude, as well as the pulse duration and frequency, must be chosen so that the dose of delivered energy guarantees EP efficacy.CONCLUSION Pain reduction in EP-based treatments can be achieved by appropriately defining the protocol parameters and electrode design. Most results can be achieved with high frequency and/or bipolar/biphasic pulses. However, the efficacy of these alternative protocols remains a crucial point to be assessed further.
Key Words: Electrochemotherapy; Irreversible electroporation; Pain; Muscle contraction;Monopolar or monophasic pulses; Bipolar or biphasic pulses
INTRODUCTION
Electrochemotherapy (ECT) is a locoregional anti-tumour therapy that combines a low dose of a chemotherapy drug with high-intensity electric pulses to induce cell membrane electroporation (EP). Consequently, the drugs enter the tumour cells and exert their cytotoxicity[1-4]. Unlike other antitumour treatments based on physical phenomena, ECT is able to exert a specific effect at the cellular level, causing the death of the treated tumour cells. Because it is highly effective in treating cutaneous and subcutaneous tumours regardless of histology[5-7], ECT treatment has been extended to more deeply located tumours[8-13].
To increase the efficacy of EP treatment, the voltage amplitude and the duration or the number of electric pulses are often increased, as long as the required current does not exceed the limit set by the pulse generator. The standard operating procedures[6]for ECT define the electric protocol that, combined with intra-tumour or intravenous delivery of bleomycin or cisplatin[14-19], guarantees an adequate efficacy of the therapy: A train of eight high voltage 100 μs monopolar electric pulses with a repetition frequency of either 1 Hz or 5 kHz is often used. However, the application of high voltage monopolar pulses may cause pain and muscle contractions[20]. For that reason, the use of muscle relaxants and general anaesthesia[21-23] are often required.
In the first studies on ECT, small cutaneous metastases were treated with the observation of only mild or moderate pain was[24-26]; therefore, pain was not considered a significant issue[6,7]. Subsequently, as the procedure started to be applied to larger cutaneous metastases, pain was reported more frequently[27,28]. For that reason, reduction of both muscle contractions and pain have been investigated over the years. The main improvements were achieved by applying pulses at a higher frequency[29-34] or by using special electrode designs.
Repetition frequency of electric pulses has a close relationship with muscle contraction, which leads to a painful burning sensation and patient complaints[19,20].An increase in repetition frequency by reducing the pulse-to-pulse pause, seems to reduce unpleasant sensations that occur during ECT[24,35-42]. Moreover, many authors reported that electric pulses lasting microseconds at a high repetition frequency do not decrease ECT antitumour efficacy[35,38]. However, although the pulse frequency is related to muscle contraction, the pain sensation also depends on other pulse characteristics such as voltage amplitude and pulse number, duration and shape[36]. The electrodes used for ECT treatment can also affect the onset of pain.Particularly, needle length, diameter and configuration that changes the distance between needles can be optimised so that the muscle volume crossed by the current is reduced as much as possible. Electrodes with a smaller distance between needles are less painful because they require lower voltages. However, they only treat small portions of tissue, and thus must be applied multiple times to cover the entire lesion.
More recently, it has been demonstrated that the use of high frequency irreversible electroporation (H-FIRE)[28-33], namely bursts of short high frequency bipolar pulses,can further reduce muscle contraction and the subsequent pain caused by the electric pulses. Treatment with H-FIRE pulses, however, may require an electric field intensity higher than the standard electric protocol, both for ECT and for irreversible electroporation (IRE), to reach an equivalent treatment efficacy. An additional disadvantage is delivering pulses at considerably higher voltage amplitudes[34].
The aim of this review is to present an overview of the different protocols proposed in the literature to reduce muscle contractions and pain caused by the EP effect in both ECT and IRE treatments. The main findings of a number of researchers are reported in the results section. The impact of different electrode designs is also considered, as the reduction of muscle contraction and patient morbidity can also be obtained with an appropriate electrode design.
MATERIALS AND METHODS
This review is the result of a self-study without protocol or a registration number. In order to ensure an adequate variety of the assessed studies, several electronic databases were searched: PubMed (United States National Library of Medicine,http://www.ncbi.nlm.nih.gov/PubMed); Scopus (Elsevier, http://www.scopus.com/); the Web of Science (Thomson Reuters, http://apps.webofknowledge.com/); and Google Scholar (https://scholar.goo-gle.it/). Only studies published between January 1999 and November 2020 were analysed because that time window is consistent with recent developments in the fields of ECT and IRE. Papers not indexed in the electronic databases were evaluated through the references of included studies. The systematic search for papers of interest is shown in the flow chart in Figure 1. The inclusion criteria evaluated the article title, abstract and contents and included pre-clinical and clinical studies that examined pain or muscle contractions caused by reversible or IRE treatments. Only articles written in English were included. Studies with insufficient reported data, case reports, reviews or letters to the editor were excluded Four investigators carried out data extraction from the included papers, focusing on the type of study (i.e.numerical analysis,in vitro,in vivoorex vivo), the type of EP (ECT or IRE),the pulse characteristics and the main results regarding reduction of muscle contraction and pain.
RESULTS
A considerable number of protocols that aim at reducing muscle contractions and pain, caused by the EP effect were found in the literature. The research was conducted with the aim of identifying the parameters that are most responsible for the perception of pain and the stimulation of muscle contraction in patients undergoing EP treatment.Thirty-three studies published between January 1999 and November 2020 were retrieved and papers not indexed in the electronic databases were identified in their reference lists. Asperthe approach described in Figure 1, 15 studies did not meet the abstract inclusion criteria and were therefore rejected. Five papers were found to be case reports, reviews or editorial letters, did not satisfy the inclusion criteria and were not included in the analysis. The remaining thirteen articles[29,30,33,34,37-45] were included in this manuscript, as they met all the required criteria (Figure 2). Four papers described treatment of cutaneous and subcutaneous tumours[37,40,41,44], two papers included sarcomas[38,42] and pancreatic tumours[43,44] and six were conducted in healthy subjects or phantoms[29,30,33,34,39,45].

Figure 1 Systematic search of relevant literature. ECT: Electrochemotherapy; IRE: Irreversible electroporation.
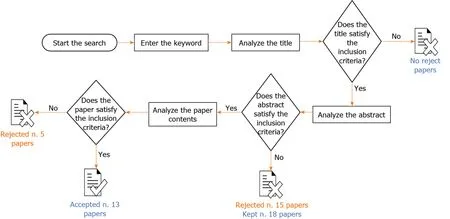
Figure 2 Included and excluded studies in the systematic review.
Reduction of muscle contraction and pain: ECT protocols
In a study published in 1999, Daskalovet al[36] compared monophasic and biphasic pulsesin vivo. The monophasic pulse protocol consisted of eight exponentially or rectangular-shaped pulses of 100 μs with a frequency of 1 Hz. In the biphasic pulse protocol, a rectangular pulse of 50 + 50 μs without intra-pulse delay was used in two different ways: (1) Eight pulses with a 1 s interval; and (2) A single burst of eight pulses spaced at 1 ms, with a total duration of 7.1 ms. In both protocols, the selected pulse amplitude ranged from 750 V to 1250 V, depending on the tumour size, with a resulting electrical field strength varying between 330 V/cm and 1250 V/cm. The study showed that the two pulse protocols (monophasic or biphasic) provided the same effect in terms of treatment result. However, the biphasic pulses were better tolerated by the patients. Particularly, the second biphasic mode, a single burst of eight pulses, was considered more acceptable than the first, which comprised eight separate stimuli. Thus, applying the pulses in a rapid sequence was as effective as the use of a larger inter-pulse interval and was better tolerated by the patients. The results of this study[36] were also confirmed by Melzack[46] who previously noted that increasing the number, (N)of applied pulses led to a better effect compared with increasing the pulse duration (T), provided thatN×Twas constant. In a later study, Miklavcicet al[37] demonstrated that pulse frequencies above the frequency of tetanic contraction(100 Hz) gradually reduced the number of individual muscle contractions. They identified muscle contractions associated with high voltage pulses as the main source of pain for patients undergoing ECT. When the pulse frequency was relatively low, the patient experienced separate muscle contractions associated with each delivered pulse.For that reason, the authors investigated the relationship between muscle contraction and pulse characteristics; particularly, repetition frequency and pulse amplitude. A train of eight 100 μs rectangular pulses at either low or high voltage amplitudes was used. At a low voltage (70 V), the measurements were performed at pulse repetition frequencies of 1, 10, 20, 50, 100, 200, 500, 1000, 2000 and 5000 Hz. At a high voltage (250 V), the measurements were performed at 1, 100, 500, 1000 and 5000 Hz. To investigate the effect of both frequency and amplitude on muscle contraction, they measured the muscle torque in response to electric pulses. They also studied the antitumour efficacy of ECT at different pulse repetition frequencies to be sure that the pain reduction did not lead to a loss of treatment efficacy. Measurements of muscle torque confirmed that high frequency pulses reduced the number of individual contractions to a single muscle contraction. More precisely, with increasing pulse frequency, muscle torque increased up to the frequency of 100 or 200 Hz, reaching a maximum value of 0.16-0.24 nm; however, a further increase of frequency above 200 Hz reduced the muscle torque regardless of the pulse amplitude, with a mean value of about 0.07 nm at 5 kHz, a value similar to that observed during the application of 1 Hz pulse trains. Moreover,by increasing the frequency of electric pulses above the frequency of tetanic contraction (i.e.at pulse frequencies higher than 2000 Hz), the authors reported that, even if the muscle torque was similar to that observed in a typical ECT protocol (1 Hz pulse trains), the patients perceived only one muscle contraction instead of eight. Finally,in vivoexperiments also demonstrated that ECT achieved similar efficacies regardless of the pulse frequency that was used (1 Hz-5 kHz), which suggest that there is a considerable potential for the clinical use of high frequency pulses in ECT.
The relationship of pulse frequency and muscle contraction and subsequent patient pain, was successively studied by Zupanicet al[38]. A train of eight electric pulses, of 1 Hz and 5 kHz repetition frequencies, was delivered to 40 healthy patients. After the conclusion of each protocol, the subjects completed the short-form McGill Pain Questionnaire[47] with separate visual analogue scales for pain intensity and unpleasantness. Their results confirmed what Miklavcicet al[37] had previously demonstrated,by finding that muscle contractions, which contribute to the discomfort felt by the subjects during the delivery of electric pulses, are strictly related to pulse frequency.When evaluating the sensorial and affective quality of pain (in the short-form McGill Pain Questionnaire, the most frequently selected pain descriptors were stabbing (80%),cramping (57.5%), throbbing (60%), shooting (60%) and hot-burning (53.8%). However,while both protocols of EP received similar average intensity scores for most descriptors (1.4 for stabbing, 1.0 for cramping, 1.1 for throbbing, 1.1-0.9 for shooting and 1.0-0.7 for hot-burning), treatment with 5 kHz electric pulses was less unpleasant.Therefore, the latter (P= 0.017) was preferred over the standard 1 Hz pulses, even though the perceived pain intensity, ranging from 6 mm to 94 mm, with similar visual analogic scores, was almost the same regardless of the frequency.
In a 2014 study, Spugniniet al[39] analysed the effects of biphasic pulse length on both treatment efficacy and morbidity. The authors investigated two different protocols of trains of eight biphasic pulses, at a voltage of 1300 V/cm. The standard protocol consisted of pulses lasting 50 + 50 ms each, with a frequency of 1 Hz and with 1 ms intra- and inter-pulse intervals. The investigational protocol consisted of pulses lasting 50 + 50 μs each, with a frequency of 1 Hz and with 10 μs intra- and inter-pulse intervals. The protocols were tested bothin vitro(human lung cancer cell line A549)andin vivo(mice xenografts; privately owned rabbits with spontaneous tumours).Three of the mice treated with the standard protocol had a strong (grade 4) muscular contraction and the other four had a moderate (grade 3) muscular contraction. Mice treated with the investigational protocol had muscular contractions reported as flicker(grade 1, two mice), weak (grade 2, four mice) and moderate (one mouse). The rabbits treated with the investigational protocol had muscular contractions graded as flicker(two rabbits), weak (three rabbits) and moderate (one rabbit). Given the results obtained from the study, it was concluded that the investigational protocol substantially reduced the morbidity associated with the delivery of electric pulses and achieved a significantly higher efficacy compared with the standard protocol.
In a more recentin vitrostudy in mouse skin melanoma (B16-F1) cells, Scuderiet al[40] delivered the electric pulses after adding 1–330 μM cisplatin. Two pulse protocols were evaluated: (1) Eight 100 μs monopolar pulses, 0.4–1.2 kV/cm, 1 Hz (standard ECT protocol); and (2) Eight bursts at 1 Hz, consisting of 50 bipolar pulses with 1 + 1 μs width, 0.5–5 kV/cm, 1 μs intra-pulse delay [high frequency EP (HF-EP)]. The analysis of the results was conducted by evaluating the difference between the two protocols (monopolar or bipolar pulses), focusing on their effect on both the efficacy of the treatment and the associated cytotoxicity. First, the results showed that both monopolar and bipolar pulse protocols, in combination with cisplatin, achieved the desired efficacy in killing cells. However, as the onset of membrane permeabilisation was higher in the HF-EP (2 kV/cm) protocol than in the ECT (0.8 kV/cm,P= 0.036)protocol, the bipolar pulse protocol needed a higher electric field (2 kV/cm,P< 0.001vs1.2 kV/cm,P< 0.001). Second, the results obtained suggest that HF-EP could be used in ECT with potential alleviation of muscle contractions and pain. In fact, even if the pain was not evaluated, it has been previously demonstrated that a short negative pulse delivered after a positive pulse accelerates passive repolarisation that abolishes the action potential. That means that fewer muscle contractions, and thus less pain, can be expected with HF-EP than with the classic 100 μs pulses. As the authors themselves concluded, although it is still at thein vitrotesting stage, the clinical use of HF-EP pulses for ECT could potentially decrease the discomfort associated with muscle contractions and pain, and simplify the treatment procedure by lowering the dose of muscle relaxants and anaesthesia and avoiding synchronisation with the electrocardiogram.
Finally, in 2020, García-Sánchezet al[41] assessed the ability of sine waves to perform ECT. They compared the classic ECT protocol (eight squared unipolar pulses of 100 μs and 1 Hz repetition frequency, electric field of 1300 V/cm) with both bipolar square pulses and sinusoidal bursts. The analysed protocols (bipolar and sinusoidal)were made for pulses with no intra- nor inter-pulse pauses. The bursts were delivered at various frequencies between 10 and 100 kHz and with electric fields of at least 1300 V/cm, and the duration and number of pulses varied depending on the experiment.The authors also carried out a computer simulation to calculate the electric field distribution and the temperature increase during the delivery of the treatment.Furthermore, verification of the effectiveness of the treatment was essential in the comparison between the different protocols, which was taken into account by considering the tumour response. Specifically, the efficacy of the treatment was assessed by comparing sinusoidal bursts at three frequencies (10, 50 and 100 kHz) and two electric field intensities (1300 and 1600 V/cm). Their results showed that sinusoidal pulses reduced both the extent of muscle contractions and skin damage.The effects were significantly lower when a high frequency wave was applied and when the square bipolar pulse was used. However, there was a clear loss of efficacy with the increase in frequency, confirming that the external electric field should be increased to 1600 V/cm in to achieve an equivalent EP effect, thus allowing for a tumour volume growth of less than 200 mm2within a 25 d follow-up period.
Reduction of muscle contraction and pain: Numerical analysis
Golberg and Rubinsky[28] performed a numerical analysis to evaluate the influence of the electrode geometry in the reduction of pain and muscle contractions. The numerical analysis considered various electrode configurations. For each experimental setup, a single pulse of 400 V and 100 μs was delivered. The results showed that conventional EP protocols and electrode design could generate muscle contraction,inducing electric fields in surprisingly large volumes of non-target tissue surrounding the EP-treated tissue. They also found that electrode placement in a structure referred to as a “current cage” substantially reduced the volume of non-target tissue exposed to electric fields above the threshold of muscle contraction. Furthermore, in an experimental study using a tissue phantom, they compared a commercial two parallel needle EP system with the current cage design. They found that a certain arrangement of needle electrodes limited the amount of tissue exposed to electric fields that above the muscle contraction threshold, while having a minimal impact on the extent of EP. The design consisted of a central, energised electrode surrounded by an array of grounded electrodes. Similar geometries have been used successfully for cardiac defibrillation and ECT. Interestingly, by having 16 or more grounded electrodes and by reducing the insertion depth of the central energised electrode relative to the grounded electrodes,the predicted amount of tissue experiencing muscle contractions fell dramatically. In fact, the analysis revealed that the ratio of the volume affected by the muscle contraction (Vmc) and that affected by the EP phenomenon (Vep) using a commercial parallel eight-electrode array, was 135 and was 410, with an electric field of than 600 V/cm and 1120 V/cm. The corresponding ratios were 73 and 26 when the 26-electrode current cage was used. Moreover, the total Vmcwas 15.09 mm2when the commercial parallel eight-electrode array was used, compared with 2.90 mm2when using the 26-electrode current cage.
Reduction of muscle contraction and pain: IRE protocols
In 2011, Arenaet al[32] used a combination of analytical, numerical and experimental techniques to investigate H-FIRE. In theirin vivoprotocols, they compared a standard IRE pulse protocol to H-FIRE. In both protocols, 180 bursts were delivered, with each burst lasting 200 μs and being delivered at a frequency of 1 Hz. In the IRE protocol,each burst consisted of a single pulse of 200 μs width. In the H-FIRE protocol, each burst consisted of (1) 50 bipolar pulses at 250 kHz and a single polarity duration of 2 μs; and (2) 100 bipolar pulses at 500 kHz with single polarity duration of 1 μs. No visual or tactile evidence of muscle contraction was seen during H-FIRE, but all IRE protocols resulted in detectable muscle contractions. The mean peak accelerations (0.8g, 0.4gand 0.1g) during IRE treatments at the cervicothoracic junction for each applied voltage (200 V, 100 V and 50 V) were significantly different from each other.On the other hand, H-FIRE resulted in no detectable acceleration at the cervicothoracic junction. Thein vivoexperiments also showed that H-FIRE produced an ablative effect on brain tissue comparable to that obtained in non-thermal IRE treatments.Specifically, there was complete uniformity of tissue death within the targeted areas. A sharp transition zone was present between lesions and normal brain tissue.
In 2014, Sanoet al[42] studied the effects of bipolar pulses on both muscle contractions and cell viability using an IRE protocol. Each monopolar waveform typical of the standard protocol was replaced with a burst of alternating polarity pulses; the total energised burst time was the same as that used in the standard protocol (100 μs). The bipolar protocol consisted of 80 bursts at a frequency of 1 Hz; in each burst, the positive/negative wavelength varied from 250 ns to 50 μs, with an intra-pulse delay fixed at 2 μs. The authors showed that, at 1500 V/cm, only treatments with bursts containing 50 + 50 μs pulses (Table 1) resulted in an interesting compromise between low viability (below 10%) and muscle contraction reduction that less undesirable than those associated with longer monopolar pulses. Sanoet al[43].analysed muscle contraction in a murine model when using different pulse protocols[43]. Treatment efficacy was also tested in anin vitrotumour model using PPT8182 murine primary pancreatic tumour cells. To facilitate comparison between groups, the authors applied the following simplified electrical dose formula:
Dose = V2 × Tp × n × N
WhereVis the applied voltage,Tpis the pulse width,nis the number of pulsesperburst, andNis the number of burstspertreatment, which was typically 80. Thanks to the use of a custom pulse generation system, bursts of bipolar pulses with constitutive pulse widths of 250 ns, 500 ns, 1 μs, 2 μs, 5 μs, 10 μs and 50 μs were delivered. They also used custom-made electrodes with 1.27 mm diameter dispensing needles and a 2.0 mm edge-to-edge separation distance. Given the formula above, the lethal electric field thresholds were found to be 2022, 1687, 1070, 755, 640, 629 and 531 V/cm for bursts containing 0.25, 0.5, 1, 2, 5, 10 and 50 μs pulses, respectively. Qualitatively, the results showed that muscle contractions occurred to a lesser extent in treatments with bipolar bursts of pulses between 1µs and 5 μs, compared with those in treatments with standard IRE protocol (100 μs monopolar pulses at 200 V). At 400 V, the 100-μs pulses induced such strong muscle contractions that complete anaesthesia was necessary to carry out the procedure. In contrast, 1000 V treatments with bursts of 5 μs pulses were well tolerated with light sedation and local anaesthesia.
Similarly, in 2016, Sweeneyet al[33] carried out a quantitative comparison between different pulsing schemes. They compared trains of 100 μs monopolar pulses conventionally used in IRE and ECT, with pulse trains containing bursts or evenly spaced 1 μs bipolar pulses. They assessed both the reduction of muscle contractions and the cell permeability obtained with the different pulsed electric field protocols. Cell permeability was evaluated by real-time microscopic imaging of propidium iodide transport at the single cell level during and after each treatment. The protocols under investigation were: (1) A train of 200 monopolar pulses of 300 V amplitude, each
lasting 100 μs and repeated at a rate of 2 kHz for 500 μs; (2) A train with the same characteristics but with a pulse amplitude of 500 V; and (3) 200 bursts of 25 bipolar pulses with a 1 + 1 μs duration and 500 V, separated by a 4 μs intra- and inter-pulse delay. Each treatment consisted of 200 periods (bursts) lasting 500 μs each, for a total treatment time of exactly 100 ms for each pulsing scheme. Even though bipolar pulses at a high frequency were able to mitigate undesirable muscle contraction during IRE,the bipolar pulses induced less evident membrane permeabilisation than equivalent monopolar pulses. In fact, intracellular detection of propidium iodide was observed at electric field intensities of approximately 500 V/cm, which was lower than that observed in bipolar pulse treatments (900-1250 V/cm). That was attributed to the inability of the short-duration bipolar pulses to complete the membrane charging despite the higher applied voltages. However, bipolar pulse protocols can be designed to obtain more efficient, symmetric and homogeneous uptake of small molecules into cells than conventional monopolar pulses.
In 2017, Yaoet al[44] explored the effect of IRE ablation on muscle contractions. The authors studied how to reduce muscle contractions by acting both on the frequency of monopolar pulses and on the nature of the electrodes used. The study was conducted with rabbit liver tissue. The H-FIRE protocol consisted of a series of 90 bursts. Each burst had a repetition frequency of 1 Hz and comprised 50, 20, 10, 4 or 2 monopolar pulses with individual pulse widths of 2, 5, 10, 20 or 50 μs. The total energised time was 100 μs. The experiments were conducted with both traditional and insulated needle electrodes with the aim of investigating how the electrode design influenced the muscle contractions. Each pair of electrodes were separated by a fixed distance of 10 mm. A finite element model was also used to establish the lethal thresholds of HFIRE protocols; consequently, the pulse voltage amplitude range was set from 800 V to 2000 V. An accelerometer was used to measure muscle contractions. The authors observed that the H-FIRE protocol reduced muscle contractions. The muscle contraction strength increased with the increase in voltage amplitude and pulse width.A quite linear increase in acceleration occurred when the voltage was increased,regardless of the pulse duration. For example, a 10 μs pulse produced an acceleration of about 1.5gat 1000 V, and about 4gat 2000 V Conversely, at a fixed voltage, a consistent increase in the acceleration value was observed when the pulse length was also increased (e.g., less than 1 g of acceleration for 2 μs pulses at 1500 Vvsmore than 7gof acceleration for 100 μs pulses at 1500 V). Moreover, fewer muscle contractions were detected when using insulated needle electrodes and the ablation area was smaller than that obtained with traditional needle electrodes (e.g., about 5gof acceleration with 50 μs pulses at 1500 V using insulated needlesvsabout 6.5gof acceleration with 50 μs pulses at 1500 V using non-insulated needles).
Sanoet al[29] compared the effect on muscle contraction associated with IRE to those associated with different H-FIRE protocols. The experiments were conductedex vivoand muscle contractions were measured with an accelerometer. In order to make the comparison consistent, the total energised time in H-FIRE protocols was ensured to be equal to one of the standard IRE protocols. The traditional IRE protocols consisted of five monopolar pulses lasting 25, 50, 75 and 100 μs, with a repetition frequency of 0.5 or 1 Hz and with an amplitude of 3000 V. To examine alternative strategies, highenergy bipolar bursts with energised times between 100 μs and 200 μs and voltages between 3000 V and 4500 V were delivered. The investigated H-FIRE protocols were split into three subgroups: (1) Symmetric 2 + 2 μs high frequency pulses with an intrapulse delay of 2 μs, voltages of from 500 to 5000 V and total energised times of 100 or 200 μs; (2) Symmetric 2 + 2 μs high frequency pulses with an intra-pulse delay of 5 μs or 10 μs, a voltage of 5000 V and a total energised time of 100 μs; and (3) Asymmetric high frequency pulses with a 2 μs positive wave, an intra-pulse of 2 μs and negative waves of 0.25, 0.5 or 1 μs (voltage of 3000 V). An energised time of 100 μs with 2–2–2 H-FIRE pulses produced muscle contractions that increased with the voltage (accelerations of 0.005gand 0.210gfor voltages of 500 and 5000 V, respectively). When the voltage was set at 3000 V, the acceleration peak obtained in the symmetrical H-FIRE protocol was 9-12 times smaller than that seen with traditional IRE pulses (0.72gwith a 75 μs pulse length). Moreover, symmetrical high frequency pulses enabled the delivery of substantially higher voltages and energised times while producing smaller accelerations than traditional IRE pulses. In fact, the acceleration values remained relatively constant when the total energised time was increased from 100 μs to 200 μs,and even when the applied voltage was increased to 4500 V. Conversely, both symmetric pulses with a variable intra-pulse delay and asymmetric pulses produced significantly greater muscle contractions. However, asymmetrical H-FIRE produced significantly greater (α < 0.001) muscle contractions at 3000 V compared with the symmetrical waveforms. The maximum peak acceleration (0.80g) comparable to that achieved with the traditional IRE pulses, was achieved with the 2–2–0.25 waveform.The authors concluded that muscle contractions can be reduced with H-FIRE pulses when the voltage and energised time are held constant (3000 V, 100 μs). Additionally,high voltage and high-energy H-FIRE treatments produced less intense muscle contractions. However, since the experiments were conductedex vivo, it is reasonable to consider that muscle contractionsin vivomay be greater than those observed in this study. Ablation efficacy should also be assessed.
Summary table
Table 1 summarises the outcomes of the literature analysis. The type of study(numerical analysis,in vitro,in vivoorex vivo), the type of electroporation protocol(ECT or IRE), the pulse characteristics and the main results are reported. With reference to the pulse characteristics, it was considered of particular interest to report:(1) The type of pulse; (2) The number of pulses (i.e.the number of bursts and the number of pulsesperburst); (3) The pulse duration (when bipolar/biphasic, as positive pulse width–intra-pulse delay–negative pulse width); (4) The pulse frequency (i.e.the inverse of a single monopolar/monophasic or bipolar/biphasic pulse period); and (5)The electric field applied (Figure 3).
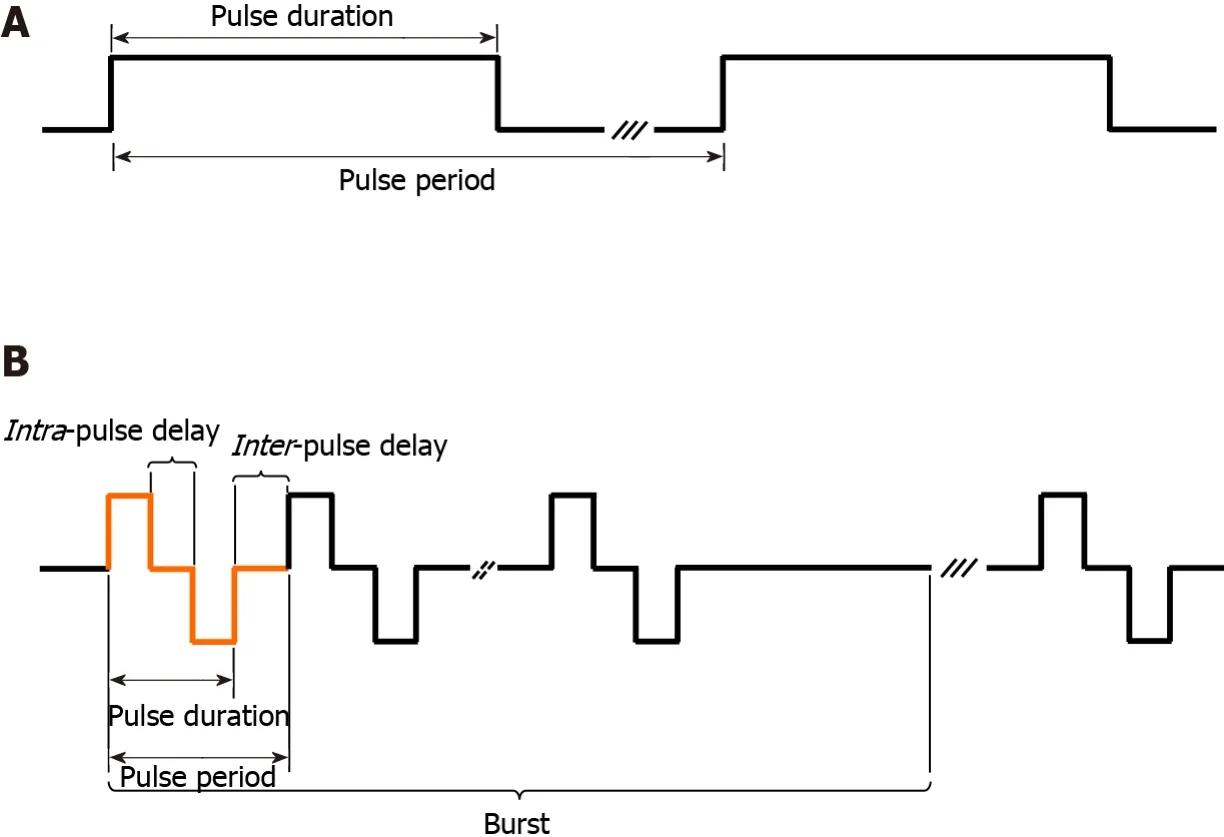
Figure 3 Pulse structure. A: Monopolar/monophasic pulse; B: Bipolar/biphasic pulse.
DISCUSSION
Muscle contractions and pain are the main undesirable effects associated with EP treatments, both ECT and IRE. Many authors have investigated different protocol designs and electrode geometries in order to reduce patient pain, the number of muscle contractions and their intensity. As this review shows, particular importance was given to the length, frequency and type of the delivered pulses. Less attention was paid to the influence of the electrode design even though it does affect the portion of the muscle through which the current flows. As reported by Miklavcicet al[37] the reduction of voltage amplitude, does not result in an appreciable reduction of patient discomfort. Moreover, even if it is widely accepted that a decrease in the pulse amplitude can be balanced by an increase in the pulse duration, there is still disagreement as to how to determine the correct increase in the number of pulses to be applied in order not to alter treatment efficacy.
Pain reduction and pulse frequency
The reduction of pain due to muscle contractions can be obtained by increasing the pulse repetition frequency above that of tetanic contraction (100 Hz)[38]. When the frequency was higher than 2 kHz, patients experienced a single muscle contraction rather than multiple muscle contractions after every single pulse[38,39]. Moreover,treatment efficacy was not altered by an increase in frequency of up to 5 kHz[38,39].That was confirmed by Yanget al[47], who observed that steep pulsed electric fields with a given frequency and appropriate electric field intensity achieved a cytotoxicity of close to 100%. However, even though the total number of muscle contractionspertreatment was reduced, the intensity of the contractions remained similar to that observed in standard protocols.
When altering the pulse repetition frequency, attention should be paid to the choice of pulse numbers and amplitude[48,49]. In fact, the relationship between the pulse parameters for ECT and treatment efficacy, assessed by the cell cytotoxicity rate, can display a highly linear behaviour up to a certain number of pulses and/or field intensity. Thereafter, an exponential model is more appropriate. That is consistent with a recent study by García-Sánchezet al[41], which found that convenient,reversible EP and efficient ECT of subcutaneous tumours and a remarkable reduction of muscle contraction could be achieved by applying sinusoidal fields. However, the frequency of sine waves has been shown to significantly affect ECT effectiveness. At 100 kHz, a clear loss of efficacy was observed[41]. In order to achieve a tumour regression similar to that obtained at 10 kHz, the electric field intensity should be theoretically increased 1.56 times. Those results highlight the charge-dependent nature of the EP phenomenon, where the cell membrane must be charged at the minimum induced transmembrane voltage in order to achieve effective electro-permeabilisa-tion[49,50].
Pain reduction and bipolar/biphasic pulses
Several authors have investigated reduction in morbidity achieved with bipolar/biphasic pulses. They all reported that altering the pulse polarity not only reduced the occurrence but also the intensity of muscle contractions. In fact, when a μs-pulse was applied, there was a latency period between the end of the pulse and the rising phase of the action potential. A rapid reversal of polarity within this latency period can accelerate passive repolarisation and inhibit the action potential generation. Therefore,with proper tuning of the bipolar/biphasic pulse parameters, it is possible to achieve a drop in muscle force that can be attributed to the termination of action potentials in part of the motor unit population[33,34,40,43,44,48,51], without losing in EP efficacy.With that in mind, interesting results were reported by Spugniniet al[39]. They reported that trains of eight biphasic electric pulses lasting 50 + 50 μs each, at a frequency of 1 Hz, and 10 μs interpulse intervals at 1300 V/cm, achieved a significantly higher response in mice (70%-90% tumour necrosis) compared with that achieved with trains of eight biphasic electric pulses lasting 50 + 50 ms each, at a frequency of 1 Hz and 1-ms interpulse intervals (40%-55% tumour necrosis)[40].
Sanoet al[43] reported that bursts of bipolar pulses resulted in both instantaneous and delayed cell death and that an inverse relationship existed between pulse width and toxicity, despite the delivery of equal quantities of energy. However, 1500 V/cm bursts containing 50 + 50 μs pulses resulted in a viability below 10% and low muscle contractions, which was less undesirable than those induced by longer monopolar/monophasic pulses. This result is comparable with the standard IRE protocol, as reported by Arenaet al[51], who showed that after eighty 100 μs monopolar pulses at 1500 V/cm, cell viability was approximately 8%. Bipolar/biphasic pulses in the same electric field seem to have appreciable efficacy when biphasic pulses of 50 + 50 μs are used; however, in order to obtain a comparable cytotoxicity rate with bipolar/biphasic and monopolar/monophasic protocols, the bipolar/biphasic pulses generally need a stronger electric field[41].
Finally, the protocols described by Scuderiet al[40] and Sweeneyet al[33] achieved the results obtained with high frequency pulses together with those achieved with bipolar pulses in ECT and IRE. They found that bipolar pulses at a high frequency were able to mitigate both undesirable muscle contraction and patient pain in EP therapies. Additional reduction was achieved when the bipolar pulse had a symmetrical structure[30]. However, short bipolar pulses may result in less pronounced membrane permeabilisation, suggesting that pulse duration is a critical parameter that must be carefully chosen[34,50].
Pain reduction and electrode design
Reductions of muscle contraction and morbidity can be achieved with an appropriate electrode design. Fewer and less intense muscle contractions were reported by Yaoet al[44] when using insulated needle electrodes. A more sophisticated electrode design was proposed by Golberg and Rubinsky[28] where a central energised electrode was surrounded by at least 16 grounded electrodes, obtaining significant pain reduction.However, the impact of the new electrode designs on treatment efficacy remains to be more deeply evaluated.
CONCLUSION
This review found that both pulse frequency and shape can be modified to reduce pain and muscle contractions in patients who undergo EP treatments. Furthermore, a combination of high frequency pulses with bipolar/biphasic ones were shown to enhance this capability. However, simply ensuring that equivalent energy is administered by standard and new protocols (high frequency, bipolar/biphasic) is not sufficient to guarantee clinical efficacy. Preclinicalin vitroandin vivostudies together with clinical data are necessary to evaluate the clinical relevance of alternative pulse protocols. In addition, sinusoidal pulses with the appropriate frequency, as well as electrode design (e.g., insulated needles), may successfully mitigate these drawbacks.Further study is required to evaluate how these aspects influence the efficacy of the therapy. A main limitation of this systematic review is the absence of a risk of bias analysis both in individual studies and across studies. Moreover, the authors did not investigate principal summary measures (e.g., risk ratio, difference in means, and others), as most studies did not report numerical results. Those deficiencies should be addressed in subsequent investigations. To summarise, pain reduction in EP-based treatments can be achieved by appropriately defining the protocol parameters and the electrode design. The desired results can be achieved with high frequency and/or bipolar/biphasic pulses. However, the efficacy of these alternative protocols remains a crucial point to be assessed further.
ARTICLE HIGHLIGHTS
Research background
In electrochemotherapy (ECT), pain and muscular contractions were reported as the most frequent drawbacks.
Research motivation
To review aimed to assess the literature describing technical advances intended to reduce muscle contraction and pain associated with electroporation (EP) effects.
Research objectives
The objective was to present an overview of different protocols proposed in the literature that aim to reduce muscle contraction in both ECT and irreversible EP treatments.
Research methods
Thirty-three published studies reporting different protocol designs and electrode geometries were selected for analysis.
Research results
Both high frequency and bipolar/biphasic pulses can be used to reduce pain and muscle contractions in patients who undergo EP treatments. Moreover, adequate electrode design can lower EP-related morbidity.
Research conclusions
Pain reduction in EP-based treatments can be achieved by appropriately defining the protocol parameters and the electrode design.
Research perspectives
The desired results can be achieved with high frequency and/or bipolar/biphasic pulses.
 World Journal of Clinical Oncology2021年5期
World Journal of Clinical Oncology2021年5期
- World Journal of Clinical Oncology的其它文章
- Cellular based treatment modalities for unresectable hepatocellular carcinoma
- COVID-19: Where is the treatment?
- Immune response evaluation criteria in solid tumors for assessment of atypical responses after immunotherapy
- Hepatic Langerhans cell histiocytosis: A review
- Thymoquinone anticancer activity is enhanced when combined with royal jelly in human breast cancer
- Prognostic role of sarcopenia in metastatic colorectal cancer patients during first-line chemotherapy: A retrospective study