
Clinical management for malignant afferent loop obstruction
2021-07-19 08:59:26ArataSakaiHideyukiShiomiAtsuhiroMasudaTakashiKobayashiYasutakaYamadaYuzoKodama
Arata Sakai,Hideyuki Shiomi,Atsuhiro Masuda,Takashi Kobayashi,Yasutaka Yamada,Yuzo Kodama
Arata Sakai,Hideyuki Shiomi,Atsuhiro Masuda,Takashi Kobayashi,Yasutaka Yamada,Yuzo Kodama,Division of Gastroenterology,Department of Internal Medicine,Kobe University Graduate School of Medicine,Kobe 650-0017,Hyogo,Japan
Abstract Afferent loop obstruction(ALO)is defined as duodenal or jejunal mechanical obstruction at the proximal anastomosis site of a gastrojejunostomy.With advances in chemotherapy,the incidence of malignant ALO is increasing.Malignant ALO can be complicated by ischemia,gangrenous bowel,pancreatitis,and ascending cholangitis.Moreover,the general condition of patients with recurrent cancer is often poor.Therefore,accurate and rapid diagnosis and minimally invasive treatments are required.However,no review articles on the diagnosis and treatment of malignant ALO have been published.Through literature searching,we reviewed related articles published between 1959 and 2020 in the PubMed database.Herein,we present recent advances in the diagnosis and treatment of malignant ALO and describe future perspectives.Endoscopic transluminal self-expandable metal stent(SEMS)placement is considered the standard treatment for malignant ALO,as this procedure is well established and less invasive.However,with the development of interventional endoscopic ultrasound(EUS)in recent years,the usefulness of EUS-guided gastrojejunostomy has been reported.Moreover,through indirect comparison,this approach has been reported to be superior to transluminal SEMS placement.It is expected that a safer and less invasive treatment method will be established through the continued advancement and innovation of interventional endoscopy techniques.
Key Words:Malignant afferent loop obstruction;Endoscopic self-expandable metal stent placement;Endoscopic ultrasound guided gastrojejunostomy;Lumen-apposing metal stent
INTRODUCTION
Afferent loop obstruction(ALO)is defined as duodenal or jejunal obstruction at the proximal anastomosis site of a gastrojejunostomy.The etiology of ALO can be classified as benign or malignant depending on the cause of the obstruction[1].With advances in surgery,the prevalence of benign ALO seems to be decreasing,whereas with advances in chemotherapy,the prevalence of malignant ALO is increasing[2].The diagnosis of malignant ALO has become easier owing to breakthroughs in crosssectional imaging.In the past,malignant ALO was surgically managed.However,the general condition of patients with recurrent cancer is often not good indicated for surgery.Percutaneous intervention for malignant ALO was reported in the late 1980s,and endoscopic intervention was reported in the 2000s.Endoscopic self-expandable metal stent(SEMS)placement for malignant ALO is considered the current standard.Although most cases of malignant ALO can be successfully treated with SEMS placement,if the stricture is long or an angulated loop,endoscopic SEMS placement across the stricture is challenging.Recently,endoscopic ultrasound(EUS)-guided gastrojejunostomy(EUS-GJ)using a lumen-apposing metal stent(LAMS)has been reported.
The aim of this review is to present the development of diagnosis and treatment for malignant ALO.We identified 104 articles in our search of the PubMed database for English-language literature using Key Words ‘malignant ALO’.After the screening of articles,we reviewed 60 English-language articles on the diagnosis and treatment of malignant ALO published between 1959 and 2020.
PATHOPHYSIOLOGY AND CLINICAL PRESENTATION
The afferent loop is the duodenum and jejunum located proximal to a gastrojejunostomy[3].ALO is duodenal or jejunal mechanical obstruction at the proximal anastomosis site of a gastrojejunostomy[4].It can result in an increased internal pressure caused by the accumulation of bile,pancreatic,and intestinal fluid[5].ALO can be complicated by ischemia,gangrenous bowel,pancreatitis,and ascending cholangitis.Patients with hepaticojejunostomy develop biliary symptoms more frequently than those without,especially those with complete ALO,owing to loss of papillary function[3].
ETIOLOGY AND INCIDENCE
The etiology of ALO can be classified as benign or malignant depending on the nature of the obstructive site[1].Malignant ALO is associated with locoregional tumor recurrence,which obstructs the afferent loop at the anastomotic site.Other causes of obstruction include regional lymphadenopathy and peritoneal carcinomatosis[3].There are few reports on the incidence of malignant ALO.Aokiet al[6]reported the incidence of ALO after gastrectomy with Roux-en-Y reconstruction performed using an open approach[6].They reported that of the 1908 patients who underwent distal gastrectomy followed by Ruox-en-Y reconstruction through an open approach(detailed patient background was not shown),4 patients(0.2%)developed ALO,and only 1 patient had malignant ALO.Juanet al[7]reported that of 1100 patients who had undergone gastroenterostomy reconstruction(detailed patient background was not shown),22(2%)patients were diagnosed with ALO after surgery,including Roux-en-Y gastroenterostomy(n= 9),Billroth II gastrojejunostomy(n= 7),and Whipple’s operation(n= 6)[7].In a series of 186 pancreatic cancer patients treated with PD,Pannalaet al[8]reported 24 cases(13%)of ALO,of which 8 were due to cancer recurrence with median follow up duration of 1.2 years[8].
DIAGNOSIS
Malignant ALO was diagnosed by clinical presentation,laboratory data,and computed tomography(CT)findings.Malignant ALO often develops into cholangitis or pancreatitis.When a patient with a history of gastrointestinal(GI)reconstruction for malignant disease develops pancreatitis or cholangitis,malignant ALO should be suspected.
In the late 1970,cases of ALO diagnosed using abdominal CT were reported[9,10].CT has been the mainstay of diagnostic imaging for ALO.CT scans revealed marked dilatation of the afferent loop due to bowel obstruction caused by a recurrent cancer(Figure 1).Juan YH reported the diagnosis of ALO following gastroenterostomy reconstruction using multidetector row CT(MDCT)[7].They reported that a fluidfilled C-shaped afferent loop in combination with valvulae connivences projecting into the lumen was the most common MDCT feature of ALO and that the etiologies of ALO and its associated complications can be predicted to be 100% by MDCT.If malignant ALO can be listed in the differential diagnosis based on patient’s medical history,symptoms,and laboratory data,the diagnosis is not difficult due to advances in CT imaging[7,9-14].

Figure 1 A computed tomography scan.A:Distention of the afferent loop by a recurrent tumor;B:Biliary dilation;C:Coronal section.
THERAPEUTIC APPROACH
Conventionally,malignant ALO is managed surgically[4,15-18].For the management of ALO,surgical revisions,such as jejunojejunostomy or Roux-en-Y conversion,have been established[4].However,the general condition of patients with recurrent cancer is not suitable for surgery.Reoperation is a difficult undertaking,and reoperation itself may cause further morbidity and mortality[1].As nonsurgical treatment is clearly desirable,percutaneous or endoscopic treatment has been reported.
Percutaneous treatment
Regardless of the clinical presentation,dilated afferent loop is the most reasonable therapeutic target for malignant ALO.A majority of the reported cases of malignant ALO developed due to obstructive jaundice.For cases that present with obstructive jaundice,it is possible to approach the dilated bile duct.Malignant ALO with obstructive jaundice has been treated with percutaneous transhepatic biliary drainage[19-23](Figure 2A).However,the procedure is known to cause bacteremia due to severe ascending cholangitis[20,21].Since the development of enteral SEMS,SEMS placementviathe transhepatic route for ALO was reported[24-30].
A direct percutaneous approach to the dilated afferent loop is available if the dilated afferent loop underlies the anterior abdominal wall[31,32](Figure 2B).Satoet al[32]performed percutaneous drainageviathe dilated afferent loop in eight patients.Of these,five patients had malignant ALO,and SEMS placement was subsequently performedviathe afferent loop to address malignant ALO in two patients;however,in the remaining three cases,the external catheter could not be removed.No patients developed specific major complications,such as septic shock,peritonitis,or other procedure-related complications[32].
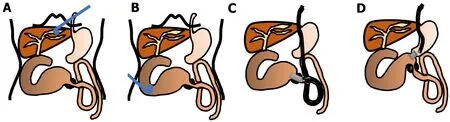
Figure 2 Therapeutic schemas for malignant afferent loop obstruction.A:Treatment of malignant afferent loop obstruction(ALO)with obstructive jaundice by percutaneous transhepatic biliary drainage;B:Treatment of malignant ALO by direct percutaneous afferent loop drainage;C:Treatment of malignant ALO by endoscopic transluminal self-expandable metal stent;D:Treatment of malignant ALO by endoscopic ultrasound-guided gastrojejunostomy.
Endoscopic transluminal SEMS placement
Since the 2000s,endoscopic transluminal SEMS placement for malignant ALO has been reported.An endoscopic treatment would be less invasive and technically easier than a percutaneous treatment[5,33-40](Figures 2C and 3).Kidaet al[41]conducted a retrospective analysis of 11 malignant ALO patients who underwent endoscopic transluminal SEMS placement[41].The procedure was attempted in 13 sessions for 11 patients,and successful in 12 of 13 sessions;there were no adverse events,and the clinical efficacy was high in successful SEMS placement patients.The median survival time after the procedure was 118 d.Ten patients died of primary disease,and one patient died of severe cholangitis after the failure of the procedure.Malignant ALO recurred,and the procedure was repeated for 2 of the 10 patients who ultimately died due to the primary disease.In another study,we reported a detailed method of endoscopic transluminal SEMS placement for malignant ALO.Briefly,an N-tube was inserted into the dilated afferent loop by fluoroscopy guidance,and then SEMS was placed through the stricture after improvement of the physical condition[5].In our case series,we retrospectively examined the records of seven patients who underwent endoscopic SEMS placement for malignant ALO following PD[40].All cases were clinically successful.The median procedure time was 30 min(range,15-50 min).There were no cases of stent dysfunction,and no procedure-related adverse events were observed.All patients died of their primary disease,and the median overall survival period was 155 d(range,96-374 d).We pointed out that our two-step approach would be safe and useful method of endoscopic SEMS placement for malignant ALO.Recently,balloon-assisted endoscopy(BAE)has also been used to place a SEMS in cases where it cannot be reached to the ALO by a standard scope[41-51].The recently designed BAE had a 3.2-mm working channel,enabled through-the-scope SEMS placement,which had been previously challenging because the large diameter of the SEMS delivery system did not allow stent placement by the conventional BAE with the 2.8-mm working channels[48].
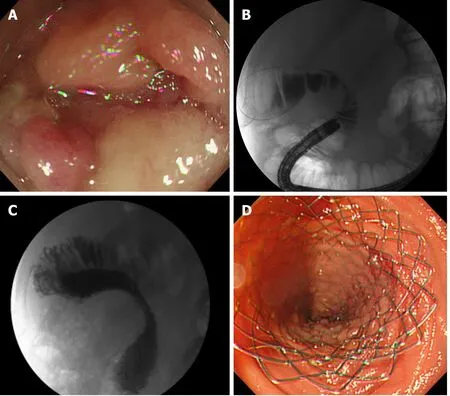
Figure 3 Endoscopic transluminal self-expandable metal stent for malignant afferent loop obstruction.A:Neoplastic stenosis in the afferent loop blocked further passage of the endoscope;B:The stenosis was confirmed with contrast media;C:Self-expandable metal stent was placed by the standard throughthe-scope technique under fluoroscopic view;D:Endoscopic view.
EUS-guided gastrojejunostomy
The creation of a GI anastomosis has been useful for relieving pancreatobiliary symptoms in patients with malignant ALO.However,surgical techniques are costly and time-consuming,and can be associated with high mortality and morbidity.Technological and clinical innovations in interventional endoscopy have allowed endoscopists to create a GI anastomosis with minimally invasive manner[52].EUS-GJ has been shown to be a safe and effective method to bypass portions of bowel.Since it was first reported by Fritscher-Ravenset al[53]in 2003,technological advancements and technique alterations have made EUS-GJ a safe approach.The case of malignant ALO that was treated with EUS-GJ using a LAMS was first reported in 2015[54,55](Figure 2D).EUS-GJ with LAMS has been reported to be useful for malignant ALO[56-58].A multicenter retrospective study showed that complete resolution of symptoms was higher in patients treated with EUS-guided entero-enterostomy(EUS-EE),with less need for re-interventions,than in those undergoing enteroscopy-assisted luminal stent placement[59].In this study,18 patients underwent EUS-EE.Clinical success included resolution of symptoms(88.9 %)and improvement in hospital discharge(11.1%).Technical success was achieved in 100% of the cases,with a mean procedure time of 29.7 min.The most common procedure was gastrojejunostomy(72.2%).Three adverse events(16.7 %)occurred(two mild,one moderate).When compared with data on endoscopic transluminal SEMS placement,patients treated with EUS-EE required fewer re-interventions(16.6 %vs76.5 %;P< 0.001).However,although LAMS has the advantages of preventing both stent migration and fluid leakage,it is not available in many countries and is more expensive than that is conventional SEMS.We reported a method involving a conventional biliary SEMS with antimigration properties,comprising a large loop double-pigtail plastic stent within a fully covered biliary SEMS(Figure 4)[60].
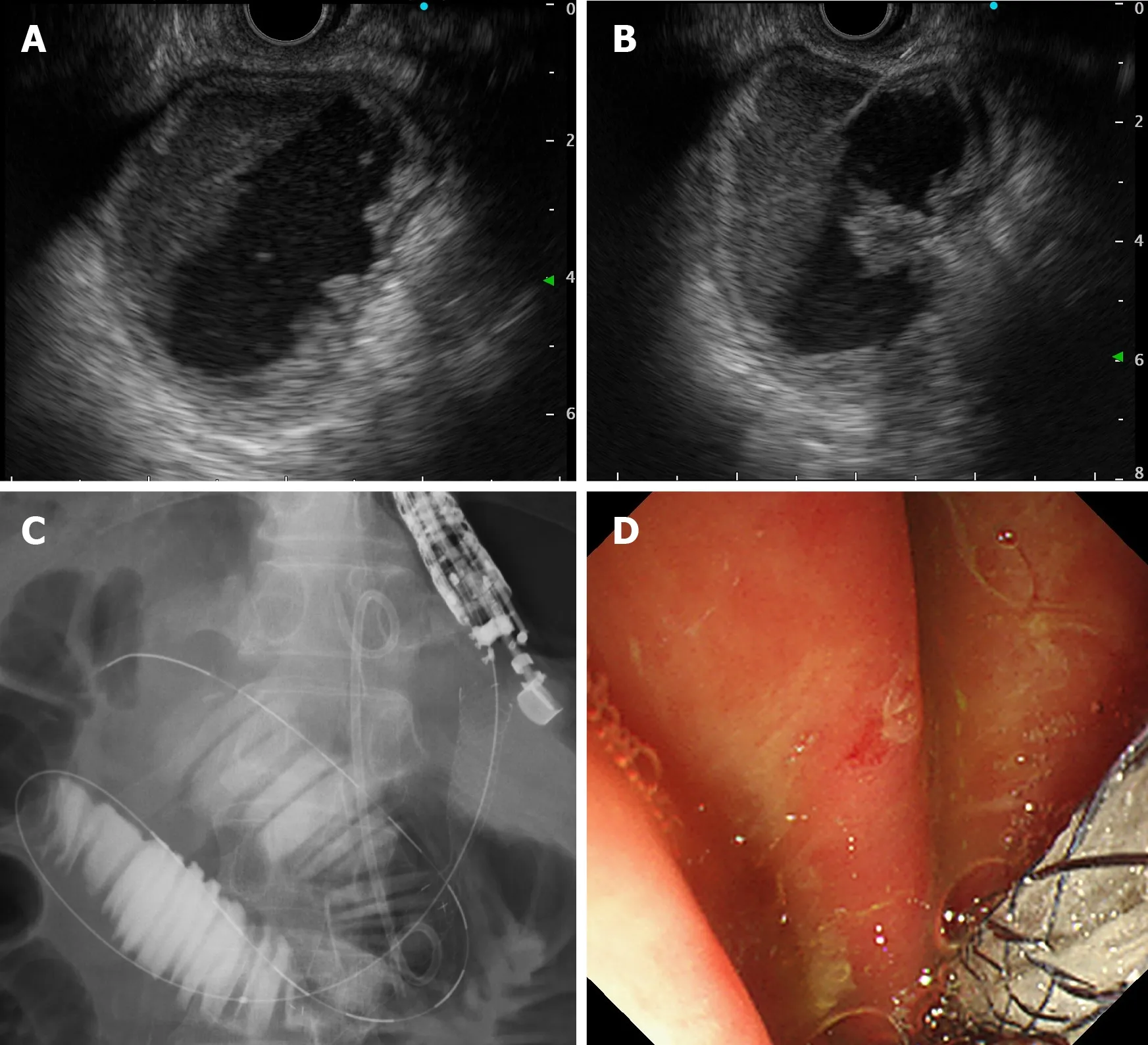
Figure 4 Endoscopic ultrasound-guided gastrojejunostomy for malignant afferent loop obstruction.A:Endoscopic ultrasound(EUS)shows the dilated afferent loop;B:Dilated afferent loop was punctured using a 19G FNA needle with an EUS guide;C:Self-expandable metal stent was placed using the standard through-the-scope technique under fluoroscopic view;D:Endoscopic view.
CONCLUSION
This review outlines the clinical management of malignant ALO.The prevalence of malignant ALO is increasing because of advances in chemotherapy for advanced cancers.As the diagnosis of malignant ALO has become easier with the development of cross-sectional imaging,it is possible to diagnose it earlier.At this point,endoscopic transluminal SEMS placement is considered the standard treatment for malignant ALO because the procedure is well established and less invasive.However,with the development of interventional EUS,the usefulness of EUS-GJ has been reported in recent years.It is expected that a safer and less invasive treatment method will be established through the continued advancement and innovation of interventional endoscopy techniques.
 World Journal of Gastrointestinal Oncology2021年7期
World Journal of Gastrointestinal Oncology2021年7期
- World Journal of Gastrointestinal Oncology的其它文章
- Laparoscopic liver resection for colorectal liver metastases — shortand long-term outcomes:A systematic review
- High expression of protein phosphatase 2 regulatory subunit B''alpha predicts poor outcome in hepatocellular carcinoma patients after liver transplantation
- Robotic resection of duodenal gastrointestinal stromal tumour:Preliminary experience from a single centre
- Cryptotanshinone inhibits cytotoxin-associated gene A-associated development of gastric cancer and mucosal erosions
- Neoantigen vaccine:An emerging immunotherapy for hepatocellular carcinoma
- Sporadic fundic gland polyps with dysplasia or carcinoma:Clinical and endoscopic characteristics