
Endoscopic retrograde cholangiopancreatography drainage for palliation of malignant hilar biliary obstruction — stent-in-stent or side-by-side? A systematic review and meta-analysis
2021-06-03 05:38GabrielMayoVieiradeSouzaIgorBragaRibeiroMateusPereiraFunariDiogoTurianiHourneauxdeMouraMariaVitriaCuryVieiraScatimburgoJoRemdeFreitasniorSergionchezLunaRenatoBaracatEduardoTurianiHourneauxdeMouraWanderleyMarquesBerna
World Journal of Hepatology 2021年5期
Gabriel Mayo Vieira de Souza, Igor Braga Ribeiro, Mateus Pereira Funari, Diogo Turiani Hourneaux de Moura,Maria Vitória Cury Vieira Scatimburgo, João Remí de Freitas Júnior, Sergio A Sánchez-Luna, Renato Baracat,Eduardo Turiani Hourneaux de Moura, Wanderley Marques Bernardo, Eduardo Guimarães Hourneaux deMoura
Gabriel Mayo Vieira de Souza, Igor Braga Ribeiro, Mateus Pereira Funari, Diogo Turiani Hourneaux de Moura, Maria Vitória Cury Vieira Scatimburgo, João Remí de Freitas Júnior, Renato Baracat, Eduardo Turiani Hourneaux de Moura, Wanderley Marques Bernardo, Eduardo Guimarães Hourneaux de Moura, Gastrointestinal Endoscopy Unit, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo 05403-010, Brazil
Sergio A Sánchez-Luna, Division of Gastroenterology, Hepatology and Nutrition, Center for Advanced Therapeutic Endoscopy, Allegheny Health Network, Pittsburgh, PA 15212, United States
Sergio A Sánchez-Luna, Division of Gastroenterology and Hepatology, Department of Internal Medicine, Basil I.Hirschowitz Endoscopic Center of Excellence, Birmingham, AL 35294, United States
Abstract BACKGROUND Biliary drainage, either by the stent-in-stent (SIS) or side-by-side (SBS) technique, is often required when treating a malignant hilar biliary obstruction (MHBO).Both methods differ from each other and have distinct advantages.AIM To compare both techniques regarding their efficacy and safety in achieving drainage of MHBO.METHODS A comprehensive search of multiple electronic databases (MEDLINE, Embase, LILACS, BIREME, Cochrane) was conducted and grey literature from their inception until December 2020 with no restrictions regarding the year of publication or language, since there was at least an abstract in English.The included studies compared SIS and SBS techniques through endoscopic retrograde cholangiopancreatography.Outcomes analyzed included technical and clinical success, early and late adverse events (AEs), stent patency, reintervention, and procedure-related mortality.RESULTS Four cohort studies and one randomized controlled trial evaluating a total of 250 patients (127 in the SIS group and 123 in the SBS group) were included in this study.There were no statistically significant differences between the two groups concerning the evaluated outcomes, except for stent patency, which was higher in the SIS compared with the SBS technique [mean difference (d) = 33.31; 95% confidence interval: 9.73 to 56.90, I2 = 45%, P = 0.006].CONCLUSION The SIS method showed superior stent patency when compared to SBS for achieving bilateral drainage in MHBO.Both techniques are equivalent in terms of technical success, clinical success, rates of both early and late AEs, reintervention, and procedure-related mortality.
Key Words: Endoscopic retrograde cholangiopancreatography; Biliary tract neoplasms; Biliary; Hilar; Stenting; Drainage
INTRODUCTION
Malignant hilar biliary obstruction (MHBO) is a late manifestation of certain types of cancer.This is diagnosed as unresectable in up to 80% of cases, and capable of causing potentially fatal complications, such as cholangitis and sepsis[1-6].Thus, aimed at improving the quality of life and survival rate of patients, a discussion on the optimal method for palliation of drainage is very valuable[7-10].
The endoscopic biliary stent, introduced at the beginning of the 1980s, was a significant advance in the treatment of extrahepatic obstruction[11-13].In biliary obstruction, self-expandable metal stents (SEMS) seem to provide prolonged patency of drainage when compared to plastic stents[3,4,14-17].The endoscopic approach is preferred for drainage over the percutaneous and surgical approaches due to its more physiological nature, minimal invasiveness[3,4,6,18-20], low rate of adverse events (AEs), and shorter hospital stays[21].One predictor of the effectiveness of biliary drainage is when the drained hepatic volume is above 50%.This often requires a bilateral decompression[15,22], which is associated with a lower chance of reintervention when compared to unilateral drainage in the palliation of drainage of MHBOs[23].
Bilateral drainage of the bile ducts can be performedviatwo methods: Stent-in-stent (SIS) or side-by-side (SBS)[15] placement of metal stents (Figure 1).In the SIS technique, one of the stents is positioned through the wire mesh of the other, configuring into a Y-shaped aspect.On the other hand, in the SBS method, both stents are placed side by side[22].The SIS technique, in contrast to the SBS technique, does not require a dilated common bile duct, and thus allows the placement of higher caliber biliary stents[17], and presents a more physiological nature of drainage[3].The SBS technique provides an easier procedural execution[3,15], and in the case of stent occlusion, reintervention is often more feasible[17].
In theory, there are advantages to both techniques, which casts doubt whether there is enough evidence to favor one method to the detriment of the other.Furthermore, few comparative studies have addressed the subject, making it still unclear which of the two methods is the optimal approach.To gather the best available data in the literature, we have designed this systematic review and meta-analysis on the subject.We aimed to compare the feasibility, safety, and efficacy of both the SIS and SBS techniques for palliative drainage in MHBO.
MATERIALS AND METHODS
Protocol and registration
This study was performed in conformity with the PRISMA[24] and it was registered in the International Prospective Register of Systematic Reviews under the file number CRD42020191262.The study was approved by the Ethics Committee of Hospital das Cl ínicas, Faculty of Medicine at The University of Sao Paulo.
Eligibility criteria
The data search was made without limitations of publication date or language, since there was at least an abstract in English.We considered clinical trials or observational studies published either as full text or as an abstract with the necessary data, comparing SIS and SBS metal stent placement in patients with malignant hilar biliary strictures.The following outcomes were observed: Technical and clinical success, early AEs (occurring within the first month after the procedure), late AEs (occurring after 30 d), stent patency, reintervention, and procedural-related mortality.
The exclusion criteria were studies using non-human subjects and trials that evaluated percutaneous biliary access drainage.
Information sources
We identified the studies by searching electronic databases and scanning reference lists of the selected articles.This search strategy was applied in electronic databases [MEDLINE, Embase, Central Cochrane, LILACS (viaBVS), BIREME, and Google Scholar] and grey literature from their inception until December 2020 (Figure 2).
Search strategy and study selection
The following search strategy was used in all databases: [(Neoplasia OR Neoplasias OR Neoplasm OR Neoplasms OR Tumors OR Tumor OR Cancer OR Cancers OR Malignancy OR Malignancies) AND (Biliary Tract OR Biliary Tree OR Biliary System OR Bile Duct OR Bile Ducts)] OR [(Bile Duct Neoplasms OR Bile Duct Neoplasm OR Bile Duct Cancer OR Bile Duct Cancers OR Biliary Tract Neoplasm OR Biliary Tract Neoplasms OR Biliary Tract Cancer OR Biliary Tract Cancers) AND (Prostheses and Implants)] OR Prosthetic OR Implants OR Implant OR Prostheses OR Prosthesis OR Endoprosthesis OR Endoprostheses OR Stent OR Stents OR Stent-in-stent OR Side-by-Side.
Data collection process and data items
Two researchers reviewed the title and abstract of each article after the removal of duplicated articles.Articles that were found to be relevant were selected for full-text review.The final decision on the selection of the studies was based on predetermined inclusion and exclusion criteria.Any disagreement on the selection of studies was resolved by consensus with a third experienced researcher.The target data of the selected studies were entered and organized in a Microsoft Excel spreadsheet by the same two reviewers who conducted the selection.The reviewers extracted from the articles the outcomes of interest and information concerning the population and study characteristics.When the data of the published articles were insufficient, the corresponding authors were consulted by e-mail for further elucidation.

Figure 1 Two methods of bilateral drainage of the bile ducts.

Figure 2 Flow diagram showing the article selection process.
Risk of bias in individual studies and quality of evidence
The risk of bias in the cohort studies was assessed by the Risk of Bias in Nonrandomized Studies-of Interventions (ROBINS I) Cochrane tool[25].For randomized clinical trials, the risk of bias was defined by version 2 of the Cochrane Risk-of-Bias tool for Randomized Trials (RoB2)[26].
The quality of evidence, expressed as high, moderate, low, and very low, was assessed utilizing the objective criteria from GRADE (Grading Recommendations Assessment, Development, and Evaluation) for each of the pre-specified results and outcomes using GRADEpro-Guideline Development Tool software (McMaster University, 2015; Evidence Prime, Inc., Ontario, Canada)[27].
Synthesis of results and data analysis
For continuous variables, we used mean or median values[28] along with the standard deviation and the total number of patients.Regarding the outcomes expressed by categorical variables, the absolute number of events and the total number of patients was employed, with calculation of the regular and absolute risk differences for each group utilizing the Mantel-Haenszel test.The mean values of each continuous outcome were calculated, as well as the 95% confidence interval (CI).Pvalues < 0.05 were considered statistically significant and the results were exposed through forest plots.
Heterogeneity was calculated using the Higgins method (I2).When heterogeneity < 50% was found, the fixed-effect model was used.In outcomes with high heterogeneity among studies (I2> 50%), sensitivity analysis employing funnel plots were conducted to identify publication bias (outliers).If the heterogeneity levels were still high even after outlier exclusion, we maintained the outlier and applied the random-effects model to express the results (true heterogeneity).If the heterogeneity levels were low after outlier exclusion, we applied the fixed-effects model.
The data of interest extracted from the selected studies were meta-analyzed using RevMan software (Review Manager Software version 5.4—Cochrane Collaboration Copyright©2020).
RESULTS
Study selection and study characteristics
A total of 10052 articles were identified through our searches in the MEDLINE, Embase, LILACS, BIREME, and Central Cochrane databases.After the removal of duplicates, evaluation of the titles and abstracts, and text analysis, four retrospective cohort studies[29-32] and one randomized controlled trial (RCT)[33] were included in the meta-analysis (Figure 2).The characteristics of the included studies are summarized in Table 1.
Three[29,30,32] of the four retrospective studies presented a moderate overall risk of bias, assessed by the ROBINS-I tool, mainly due to confounding, the bias in the selection of participants, and bias in the selection of the reported results.The other included study[31] presented a serious risk of bias.The RCT study[33] presented a low risk of bias in our analysis (RoB2) (Tables 2 and 3).Detailed information concerning the risk of bias for each outcome is described in Table 4.
Technical success
All four cohorts[29-32] (181 patients) and the RCT study[33] (69 patients) assessed technical success.The overall analysis showed no difference between both SIS and SBS [risk difference (RD) = 0.06; 95%CI: -0.00 to 0.13,I2= 0%,P= 0.06] (Figure 3).
The overall certainty of the evidence was moderate for the cohorts and high for the RCT study, according to GRADE.
Clinical success
Three studies evaluated clinical success, namely two cohorts[30,32] (116 patients) and the RCT study[33] (69 patients).This outcome was similar for both SIS and SBS techniques in the overall analysis (RD = 0.07; 95%CI: -0.05 to 0.18,I2= 56%,P=0.26) (Figure 4).
The overall certainty of the evidence was low for the cohort and high for the RCT study, according to GRADE.
Early AEs
Three cohorts[30-32] (157 patients) and the RCT study[33] (69 patients) evaluated early complications.In the overall analysis, both SIS and SBS techniques performed similarly regarding this outcome (RD = -0.09; 95%CI: -0.19 to 0.01,I2= 2%,P=0.07) (Figure 5).

Table 1 Type of intervention and outcome of study
The overall certainty of the evidence was moderate for both cohorts and the RCT study, according to GRADE.
Late AEs
Five studies[29-33] compared late complication rates, evaluating a total of 181 patients in the cohorts and 69 patients in the RCT.In the overall analysis, there was no significant difference between the two groups (RD = -0.04; 95%CI: -0.14 to 0.05,I2= 0%,P= 0.39) (Figure 6).
The overall certainty of the evidence was moderate for both cohorts and the RCT study, according to GRADE.
Stent patency
Three studies assessed stent patency: two cohorts[30,32] (116 patients) and the RCT[33] (69 patients).The overall analysis revealed increased stent patency when SIS was performed [mean deviation (MD) = 33.31; 95%CI: 9.73 to 56.90,I2= 45%,P= 0.006] (Figure 7).
The overall certainty of the evidence was moderate for the cohort and high for the RCT study, according to GRADE.
Reintervention
One cohort[29] compared reintervention rates, evaluating a total of 24 procedures—7 in the SIS group and 17 in the SBS group.We found no difference between the two groups in the overall analysis (RD = 0.05; 95%CI: -0.15 to 0.26,I2= 0%,P= 0.60) (Figure 8).
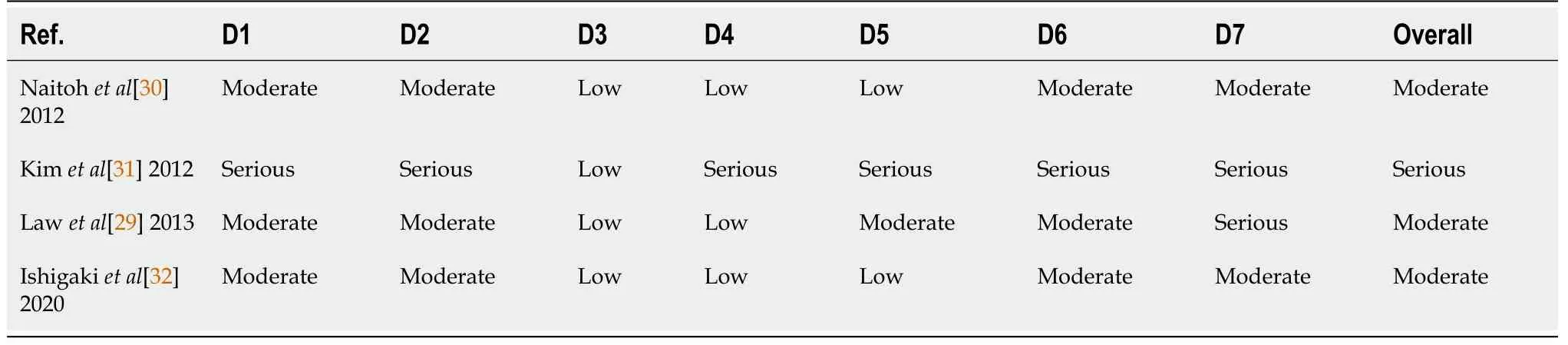
Table 2 Risk of bias for ROBINS-I

Table 3 Risk of bias for RoB2
The overall certainty of the evidence was low for the cohort and high for the RCT study, according to GRADE.
Procedure-related mortality
Two cohorts[29,30] compared procedure-related mortality, evaluating a total of 76 procedures—31 in the SIS group and 45 in the SBS group.We found no difference between the two groups (RD = 0.00; 95%CI: -0.05 to 0.05,I2= 0%,P= 1.00) (Figure 9).The overall certainty of the evidence was moderate for the cohorts and high for the RCT study, according to GRADE.
DISCUSSION
Despite being targeted by promising therapies in several clinical trials[34,35], bile duct tumors are often diagnosed as unresectable when they present with biliary obstruction.Therefore, internal drainageviathe endoscopic deployment of stents has a pivotal role in this condition.
To the best of our knowledge, this is the first systematic review and meta-analysis comparing both the SIS and SBS techniques for the palliation of biliary drainage in MHBOs.This is a relevant topic for clinical practice, and many studies have noncomparatively evaluated these biliary drainage methods in the past.Despite presenting higher stent patency with the SIS method, we have found through our meta-analysis that there were no statistically significant differences concerning technical success, clinical success, early AEs, late AEs, reintervention, and procedurerelated mortality.
For both groups, technical success was achieved in most cases, and we consider that the included studies were conducted at high-volume centers.The main challenge in the SBS method consists of the deployment of the second stent along with the first one.This is especially important since the distal end of both stents should ideally remain at the same level to facilitate an eventual reintervention.New devices have been developed, including systems with a thinner delivery system, which allows the simultaneous deployment of both prostheses.This system prevents the risk of a failed second placement and is associated with a shorter procedural time, as reported by Inoueet al[36].Traditionally, the dilation on the wire mesh of the first stent before inserting the second one is necessary for the SIS technique.This prerequisite increases the difficulty and cost of the procedure.However, stents with larger cells have been developed, specifically for this usage, with high rates of technical success for the SIS method[37].We consider that despite the fact that achieving bilateral biliary drainage in the MHBOs is technically challenging, technical success rates were increased and equivalent between both SIS and SBS, probably due to the endoscopist’s vast expertise and the availability of suitable material.

Table 4 Description of bias for each outcome (GRADE)

1There are risk of bias in selection of the reported result, according to ROBINS-I tool.2Wide confidence interval range.3High heterogeneity, calculated using the Higgins method (I2).CI: Confidence interval; RR: Risk ratio; MD: Mean difference; RCT: Randomized controlled trial.
Clinical success was defined in the studies as a total bilirubin decrease in the first month to at least 50% or 75% of the pre-treatment value.Although there was no statistical difference between the groups, we have reservations regarding this outcome definition and we think this outcome should be evaluated very carefully.One reason for this could be that the studies that evaluated this outcome opted for a conservative definition, based on a little significant drop in bilirubin levels, and not on laboratory level standards.Also, they failed to assess other laboratory or clinical parameters.
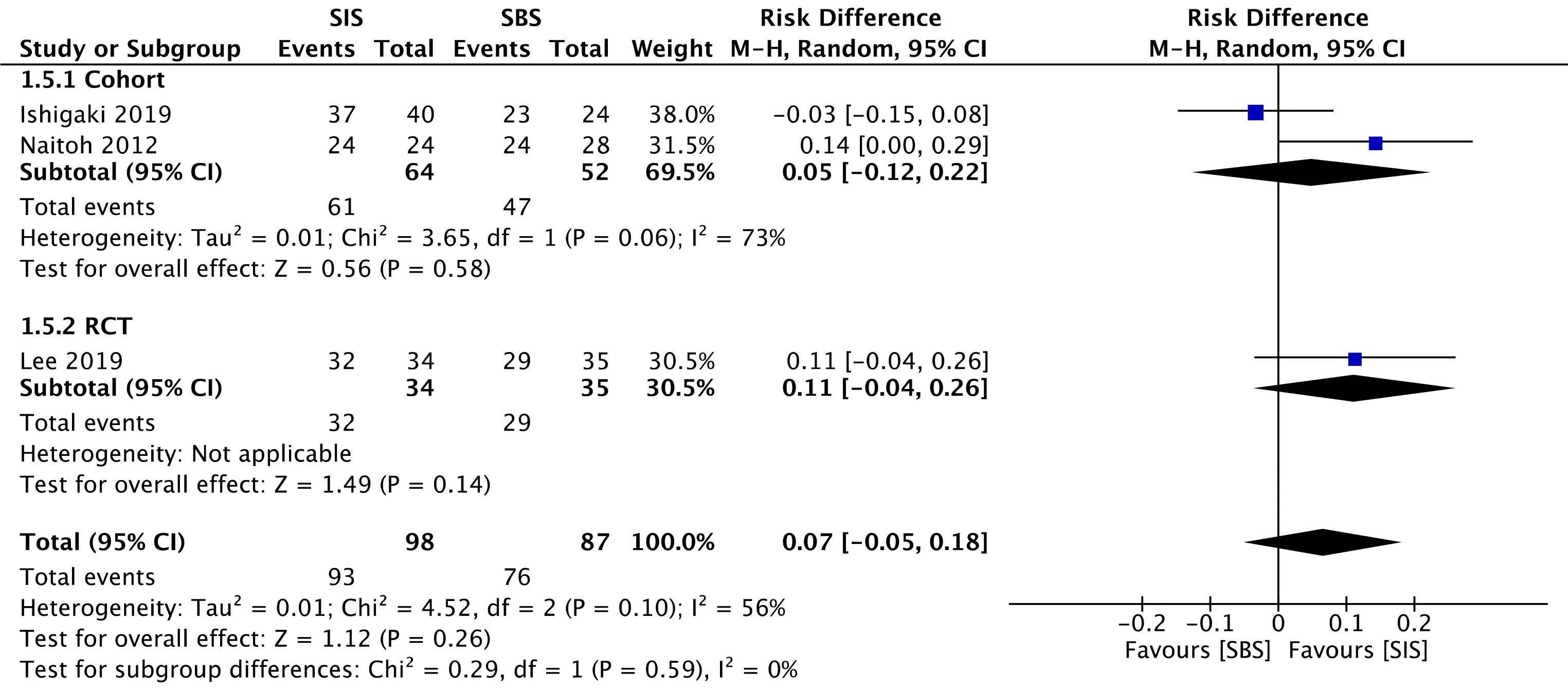
Figure 4 Forest plot — studies reporting rate of clinical success using a random-effects model.
The use of uncovered SEMS is preferred over fully covered SEMS (FCSEMS) for palliative drainage of malignant biliary obstructions[21], just as it was done in the assessed studies.This is due to the risk of obstruction in intrahepatic lateral branches and cystic and pancreatic ducts, abscess-related factors, cholecystitis, and acute pancreatitis (AP).Inoueet al[38] and Yoshidaet al[39] reported the occurrence of hepatic abscesses (11.8% and 6.3% of cases, respectively) when using 6 mm FCSEMS.Although these results cannot be attributed to the stents, they allow us to consider such a hypothesis.In our study, the SIS and SBS techniques presented similar results regarding late complications, such as cholangitis, cholecystitis, and biloma formation.In the cohort meta-analysis, SBS resulted in higher early complication rates (RD = -0.14; 95%CI: -0.27 to -0.01,I2= 0%,P= 0.03), such as AP.Tarnaskyet al[40] had already reported a higher risk of AP in patients referred to biliary stenting for hilar biliary stricture.Furthermore, stent deployment in SBS with the distal end of the stent across the papilla, instead of above the papilla, seems to raise the risk of AP[41].Nevertheless, in the cohorts meta-analyzed in the present study both techniques were utilized, thus impeding the attribution of the aforementioned complication exclusively to that reason.However, a RCT and general analysis showed no statistically significant differences.These data suggest that both techniques are safe as part of a minimally invasive treatment, with no differences regarding the occlusion of intrahepatic, cystic, or pancreatic ducts.Even if it is not possible to arrive at this conclusion from only this meta-analysis, it seems to us that the stent type has more influence on the complication rates than the drainage technique itself.The safety of endoscopic treatment and each specific technique, is reinforced by the absence of procedural-related deaths in all the casuistry of this study.
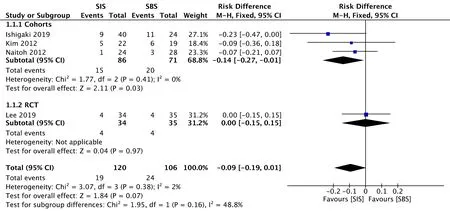
Figure 5 Forest plot — studies reporting rate of early adverse events using a fixed-effects model.
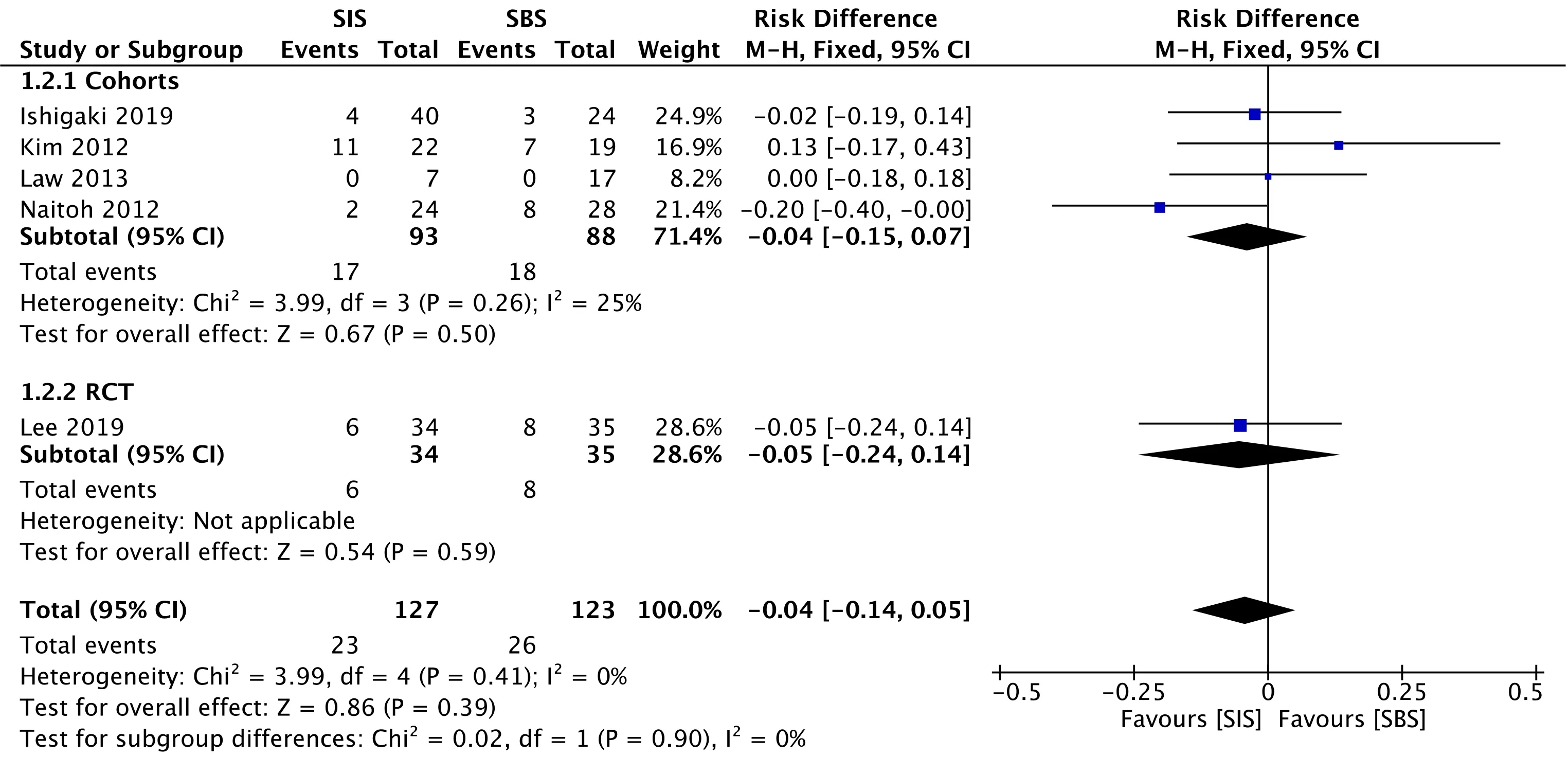
Figure 6 Forest plot — studies reporting rate of late adverse events using a fixed-effects model.
The outcome of stent patency, evaluated as moderate and high levels of evidence for the cohort and the RCT, respectively, showed a MD = 33.31, favoring SIS, with a 95%CI: 9.73 to 56.90.Although the reason behind such a difference is unclear, we believe that the SIS technique may allow greater stent expandability, and consequently larger internal caliber, in comparison with the SBS technique.Nevertheless, this result should be analyzed very carefully since some studies do not specify the exact caliber of the employed stent, and one of them disclosed the use of calibers slightly larger in the SIS technique.The use of SEMS in the studies is a positive factor regarding stent patency, corroborating the findings of the specific study that showed higher patency with these types of stents when compared with the plastic stents (131 dvs47 d)[42].Our study found no difference regarding the reintervention rate.The main cause of post-procedural obstruction was tumor progression (ingrowth or overgrowth) provoking cholestasis and cholangitis, and thus requiring reintervention.The reintervention approach usually adopted in these cases is the placement of an inner metallic stent, after the cleansing of ductal debris with a balloon extraction and/or cholangioscopy.Radiofrequency ablation can also be considered, but related studies are still scarce[21].

Figure 7 Forest plot — studies reporting the number of days of stent patency using a fixed-effects model

Figure 8 Forest plot — studies reporting the rates of reintervention using a fixed-effects model.
Our study has some limitations.There is only one RCT in the literature comparing both analyzed techniques.Besides the RCT, only 4 comparative retrospective observational studies are available in the literature.Furthermore, the number of patients in the included studies is small, perhaps because this disease does not have a high prevalence.Although the study by Kimet al[31] is available only as an abstract, it possessed all the necessary data for this analysis.Moreover, the prostheses used in different studies were from different manufacturers, with no information on diameter measurements for comparison.Given such limitations, new RCTs may have a valuable role in new systematic reviews, thus improving the quality of evidence.
Despite the aforementioned limitations and to the best of our knowledge, our study is the first systematic review with a meta-analysis on this topic.We firmly believe this has significant clinical applicability given the increasing demand for bile duct drainage in the palliation of malignant hilar tumors.
CONCLUSION
There is no significant difference between the SIS or SBS techniques in terms of early and late complication rates, technical success, clinical success, reintervention, and procedural-related mortality.The SIS technique was superior in terms of stent patency when compared to the SBS technique, which may guide decision-making regarding the best therapeutic modality for each patient.

Figure 9 Forest plot — studies reporting the rates of procedural-related mortality using a fixed-effects model.
ARTICLE HIGHLIGHTS
Research background
Patients with malignant hilar biliary obstruction (MHBO) benefit from bilateral palliative endoscopic drainage.However, there is no consensus on which is the optimal technique for placing a metal stent: Stent-in-stent (SIS) or side-by-side (SBS).
Research motivation
Many patients undergo palliative endoscopic retrograde cholangiopancreatography(ERCP) drainage, due to the advanced stage of the disease at the time of diagnosis,unresectable in most cases.However, choosing the best management for drainage can be a real technical challenge.Therefore, we aimed to compare both drainage techniques in an attempt to identify the optimal approach.
Research objectives
To perform a systematic review and meta-analysis of available studies that compare SIS and SBS deployment in patients with MHBO undergoing ERCP drainage.
Research methods
The systematic review and meta-analysis followed the PRISMA Guidelines.Electronic searches were performed in MEDLINE, Embase, Cochrane, LILACS, and BIREME databases, and the grey literature.Comparative cohorts and randomized controlled trials (RCTs) were included.Studied outcomes were technical and clinical success,early and late adverse events (AEs), stent patency, reintervention, and procedurerelated mortality.
Research results
Four comparative cohorts and one RCT were included in the final analysis with a total of 250 patients, of whom 127 belonged to the SIS group and 123 to the SBS group.Stent patency was significantly higher in the SIS group.Procedure-related mortality was similar in both groups, and no significant differences were found in the rates of technical success, clinical success, early AEs, late AEs, and reintervention.
Research conclusions
There was no difference be tween the groups concerning technical and clinical success,early and late AEs, reintervention, and procedure-related mortality.However, there was longer stent patency in patients undergoing the SIS technique.This result suggests that SIS may be the preferred technique for bilateral palliative metal stent deployment in patients with inoperable MHBO.
Research perspectives
Palliative biliary drainage is an increasingly performed procedure, but without consensus on the optimal technique, SIS or SBS.There is a small number of comparative studies in the literature.Future RCTs will have an important role in elucidating the most optimal drainage technique.
 World Journal of Hepatology2021年5期
World Journal of Hepatology2021年5期
- World Journal of Hepatology的其它文章
- COVID-19 and the liver: What do we know so far?
- Direct, remote and combined ischemic conditioning in liver surgery
- Bile acid indices as biomarkers for liver diseases II: The bile acid score survival prognostic model
- Gut dysbiosis is associated with poorer long-term prognosis in cirrhosis
- Combination of type IV collagen 7S, albumin concentrations, and platelet count predicts prognosis of non-alcoholic fatty liver disease
- Surgical treatment outcomes of primary hepatic sarcomas: A singlecenter experience