
Predictive Value of Blood Pressure,Heart Rate,and Blood Pressure/Heart Rate Ratio in a Chinese Subpopulation with Vasovagal Syncope
2021-03-18 07:41:14ZhuzhiWenJingyingHouZunMiHuifenHungYngxinChenDengfengGengndJingfengWng
Zhuzhi Wen ,,Jingying Hou ,,Zun Mi ,Huifen Hung ,Yngxin Chen ,Dengfeng Geng nd Jingfeng Wng
1 Department of Cardiology,Sun Yat-sen Memorial Hospital of Sun Yat-sen University,Guangzhou,China
2 Guandong Province Key Laboratory of Arrhythmia and Electrophysiology,Guangzhou,China
3 Emergency Medicine,Sun Yat-sen Memorial Hospital,Sun Yat-sen University,Guangzhou,China
4 Breast Tumor Center,Sun Yat-Sen Memorial Hospital,Sun Yat-Sen University,Guangzhou,China
Abstract Objective:The head-up tilt test (HUTT) is widely used but is time-consuming and not cost-effective to evaluate patients with vasovagal syncope (VVS).The present study aims to verify the hypothesis that ambulatory blood pressure(BP) monitoring (ABPM) and the simplistic tilt test may be potential alternatives to the HUTT.Methods:The study consecutively enrolled 360 patients who underwent the HUTT to evaluate VVS.BP),heart rate(HR),and BP/HR ratios derived from ABPM and the simplistic tilt test were evaluated to predict the presence,pattern,and stage of syncope during the HUTT.Results:Mixed response was the commonest pattern,and syncope occurred frequently with infusion of isoproterenol at a rate of 3 μ g/min.During the simplistic tilt test,the cardioinhibitory group had higher tilted BP/HR ratios than the vasodepressor group,while the vasodepressor group had a faster tilted HR and a larger HR difference than the cardioinhibitory group.The higher the BP/HR ratio in the tilted position,the higher the isoproterenol dosage needed to induce a positive response.During ABPM,BP/HR ratios were signif icantly higher in the cardioinhibitory group than in the vasodepressor group.The higher the ABPM-derived BP,the higher the dosage of isoproterenol needed to induce syncope.There were signif icant correlations in BP/HR ratios between ABPM and the supine position in the vasodepressor group,while signif icant correlation was found only for the diastolic BP/HR ratio between ABPM and the tilted position in the cardioinhibitory group.The mixed pattern shared correlative features of the other two patterns.Conclusion:ABPM and the simplistic tilt test might be used as promising alternatives to the HUTT in VVS evaluation in clinical settings.
Keywords:Vasovagal syncope; head-up tilt test; simplistic tilt test; ambulatory blood pressure monitoring; blood pressure/heart rate ratio
Introduction
Vasovagal syncope (VVS) is the commonest cause of syncope,accounting for approximately 68.5%of syncope presentations in specialized clinical settings [1].The head-up tilt test (HUTT) has been established as a useful tool for the evaluation of patients with suspected VVS.However,the HUTT is somewhat time-consuming in busy clinical settings and expensive for diagnosis.Additionally,no conf irmed evidence supports a single measurement or a combination of measurements ableto predict the HUTT result with precision [2].Therefore,novel diagnostic tools rather than the HUTT are being explored to evaluate VVS.
Growing evidence suggests that blood pressure(BP),heart rate (HR),or their ratio may be predictive of HUTT results in advance.To date,few studies have demonstrated the role of BP,HR,BP/HR ratios from ambulatory BP monitoring (ABPM) and the simplistic tilt test (STT) which was def nied as the period from the beginning to positional change during the HUTT at the basic stage,in the appearance of syncope,syncope patterns,and when syncope occurs during the HUTT in VVS patients.In a previous study [3],we observed that many VVS patients had positive responses at the time of a change from supine position to tilted position with or without isoproterenol infusion during the HUTT.Therefore,the present study aims to explore syncopal characteristics in a Chinese subpopulation,clarify predictive roles of BP,HR,and BP/HR ratios derived from ABPM and the STT with regard to the presence,pattern,and stage of syncope during the HUTT.
Methods
Study Population and Data Collection
The study consecutively enrolled 360 patients aged 15- 70 years who were admitted to the Department of Cardiology of Sun Yat-sen Memorial Hospital between January 2007 and December 2017 for unexplained syncope.VVS had been diagnosed in these patients by detailed medical history,physical examination,the HUTT,and other ancillary tests.In the present study,all admitted patients aged from 15 to 70 years,received the HUTT and diagnosed as VVS on discharge for their unexplained syncope within the research period were included.Patients with histories of congestive heart failure,severe coronary heart disease,severe arrhythmia,severe structural heart disease including congenital heart disease,rheumatic heart disease and cardiomyopathy,and pulmonary hypertension that might be related to cardiac syncope were excluded from the study.Patients with clinical manifestations of cerebral infarction,cerebral hemorrhage,and traumatic brain injury that could cause neurological syncope or epilepsy,as well as clinical manifestations of orthostatic hypotension,carotid sinus syndrome,and carotid sinus syndrome were excluded from the study.Patients with signif icant abnormalities in examinations by electrocardiogram,dynamic electrocardiogram,echocardiography,coronary artery angiogram,invasive electrophysiological study,electroencephalogram,and magnetic resonance imaging that indicated that syncope from another cause had not been completely excluded were also excluded from the study.Finally,those with severe diseased states,including severe hepatic dysfunction and renal insuff iciency,and current infectious disease and thus could not complete the HUTT and those with any medical condition that could cause syncope and who had taken any drug that could have inf luenced BP and HR were also excluded from the study.Individuals were assessed,investigated,and treated according to the usual institutional practice.The data collection included demographic data,medical history,body measurements,laboratory tests,electrocardiogram,dynamic electrocardiogram,ABPM,echocardiogram,computed tomography,magnetic resonance imaging,and electroencephalogram.The HUTT,coronary artery angiogram,and an invasive electrophysiological study were performed for patients who provided written informed consent.Investigations were in accordance with the Declaration of Helsinki.The present study was approved by the Ethics Committee of Sun Yat-sen Memorial Hospital of Sun Yat-sen University(SYSEC-KY-KS-2020-175),and all medical records were studied by anonymous means.
Head-Up Tilt Test
The HUTT protocol was performed and syncopal responses,syncope patterns,and syncope stages were def ined as in our previous study [3].In the present study,the HUTT was performed after other causes of syncope had been excluded.Any vasoactive drug inf luencing BP and HR should be withheld for at least f ive half-lives before the HUTT.The modif ied HUTT was performed for all patients in a comforTableand slightly darkened room equipped for cardiopulmonary resuscitation.The test was performed on an electrically adjusTabletilt Table(Siemens HUT-821,Juchi Medical,Beijing).The right antecubital intravenous line was used for isoproterenol infusion.HR was monitored throughout the test and cuff BPs were obtained every 5 min or when symptoms occurred.After the patient had initially rested for 10 min in the supine position,the Tablewas smoothly tilted to 70°,which was def ined as the STT.Subsequently,in the absence of syncope or presyncope,after 10 min in the tilted position,the Tablewas returned to the supine position and increasing dosages of isoproterenol (1,3,and 5 μ g/min) were gradually infused in three successive stages.Each stage consisted of 10 min in the tilted position and 5 min in the supine position between stages.
Positive response was def ined as the development of syncope or presyncope associated with bradycardia (marked bradycardia less than 50 beats per minute or 20% or greater decrease in HR) or hypotension (systolic BP [SBP] of 80 mmHg or less,diastolic BP [DBP] of 50 mmHg less,or 25% or greater decrease in mean arterial pressure),or both.Negative response was def ined as the completion of the protocol without symptoms.Positive response was further classif ied into three syncope patterns:cardioinhibitory when isolated marked bradycardia occurred,vasodepressor when isolated hypotension occurred,and mixed when mild bradycardia accompanied by hypotension was observed at the time of syncope or presyncope.Positive response was further divided into four syncope stages according to the time when syncope occurred during the HUTT:basic stage (without isoproterenol infusion),low-dosage isoproterenol stage (1 μ g/min),mediumdosage isoproterenol stage (3 μ g/min),and highdosage isoproterenol stage (5 μ g/min).HR and BP as well as their differences and ratios in the STT stage were used to predict syncopal response,syncope patterns,and syncope stages.
Twenty-Four-Hour Ambulatory Blood Pressure Monitoring
ABPM was performed with a model 90217 device(Spacelabs Healthcare,USA).Vasoactive drugs that may inf luence BPs and HR were withheld for at least f ive half-lives before ABPM.The reliability of BPs measured with the device was checked against simultaneous measurements with a mercury sphygmomanometer before the monitoring started.Measurements were made every 30 min during daytime (6:00 to 22:00) and every 60 min during nighttime (22:00 to 6:00).BP was measured by the cuff-oscillometric method.Each SBP,DBP,and HR measurement was recorded by the device and evaluated by the software of the same system.The mean SBP,mean DBP,mean HR,and mean BP/HR ratios during a whole day (24 hours),in the daytime,at nighttime,and at each hour were evaluated.
Statistical Analysis
Continuous variables were presented as the mean ±standard deviation and were compared by thettest or one-way ANOVA with the least signif icant difference post hoc test within subgroups.Categorical variables were presented as the number and proportion and tested for statistical signif icance with the χ2test.General line model repeated measures were used to evaluate the distributions of parameters during ABPM.Two-tailed P values less than 0.05 were considered signif icant.All statistical analyses were performed with the software package SPSS for Windows version 16.0.
Results
Demographic and Clinical Characteristics of Participants
There were 360 patients,with a mean age of 42 years,enrolled in the study,including 189 males and 171 females.Because 13 patients did not complete the HUTT,347 patients were included for further evaluation.Although coronary artery angiogram,computed tomography or magnetic resonance imaging was performed,only a few patients were found to have signif icant stenoses in coronary arteries or mild stroke ( Table1).Both coronary artery disease and stroke did not differ signif icantly between positive and negative patients.Positive patients had a higher prevalence of electrocardiogram abnormalities and a signif icantly lower HR at admission when compared with negative patients.
Syncopal Characteristics of the Population
A mixed pattern was the predominant subtype of VVS,which accounted for 52.0% of syncope presentations overall ( Table2).No signif icance was observed in the presence of prodrome,triggers,syncope duration,and syncope episodes between positive and negative groups and among syncope patterns.The cardioinhibitory group had the highest prevalence of sinus arrest when syncope happened,but long R-R intervals were rarely observed,while junctional escape rhythm occurred commonly.Overall,there was a signif icant difference between syncope stages and syncope patterns ( Figure1).A larger number of positive episodes occurred at the medium-dosage stage overall and among different syncope patterns.More vasodepressor patients had a positive response at an earlier stage,especially when compared with cardioinhibitory patients.
Predictive Roles of BP,HR,and BP/HR Ratios Derived from the STT
Positive patients had lower HRs in both the supine position and the tilted position,which were signif icantly lower than in negative patients ( Table3).Signif icantly lower BP/HR ratios in the tilted position but not the supine position were found in positive group when compared with the negative group.Both mixed and cardioinhibitory patients had signif icantly lower HRs than negative patients,while no signif icance of HR was revealed between negat ive patients and vasodepressor patients.Both mixed and cardioinhibitory patients had signif icantly higher BP/HR ratios than negative patients in both the supine position and the tilted position and than vasodepressor patients in the tilted position.However,no signif icance of BP/HR ratios was found between vasodepressor and negative patients.The vasodepressor group had the largest HR difference from the supine position to the tilted position during the STT.The smaller the HR difference,the higher the isoproterenol dosage needed to induced a positive response ( Table4).SBPs in the tilted position and the SBP difference for the STT were signif icantly higher in the medium-dosage and high-dosage stages than in the low-dosage stage.Furthermore,patients with higher BP/HR ratios in the tilted position needed a higher dosage of isoproterenol to induce syncope.
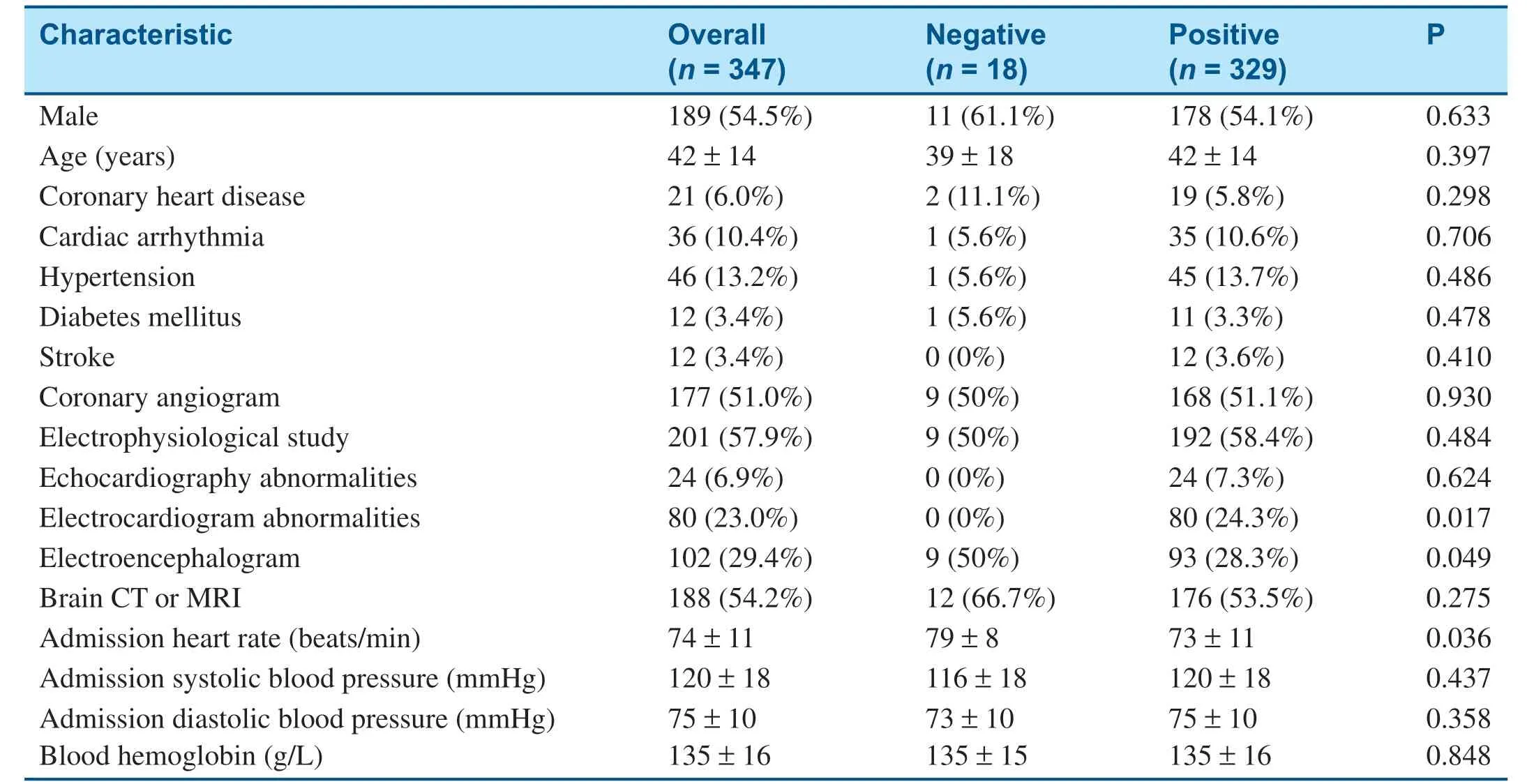
Table1 Baseline Demographics and Clinical Characteristics of the Study Population.
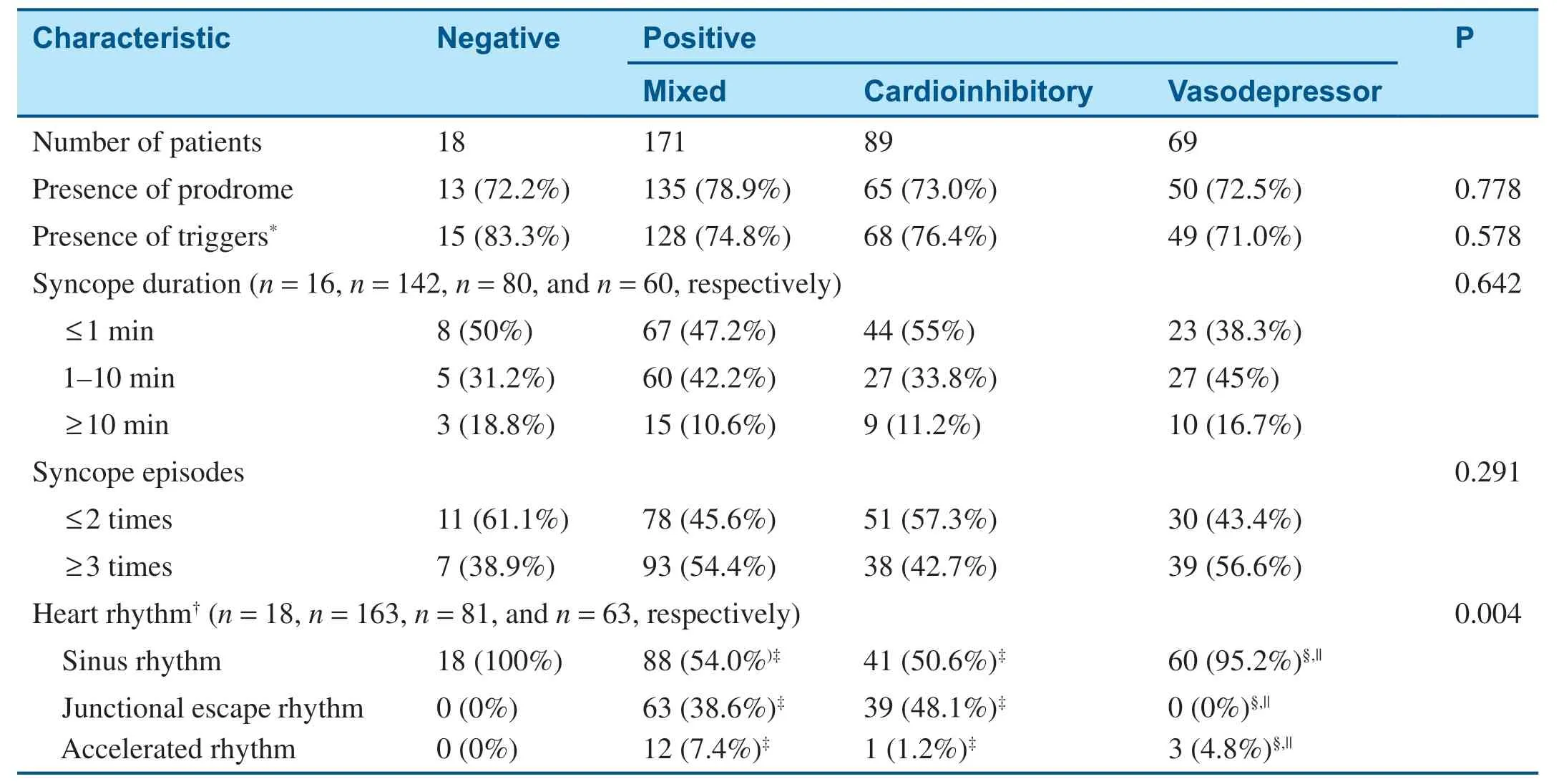
Table2 Syncope Characteristics According to Tilt-Test Results.
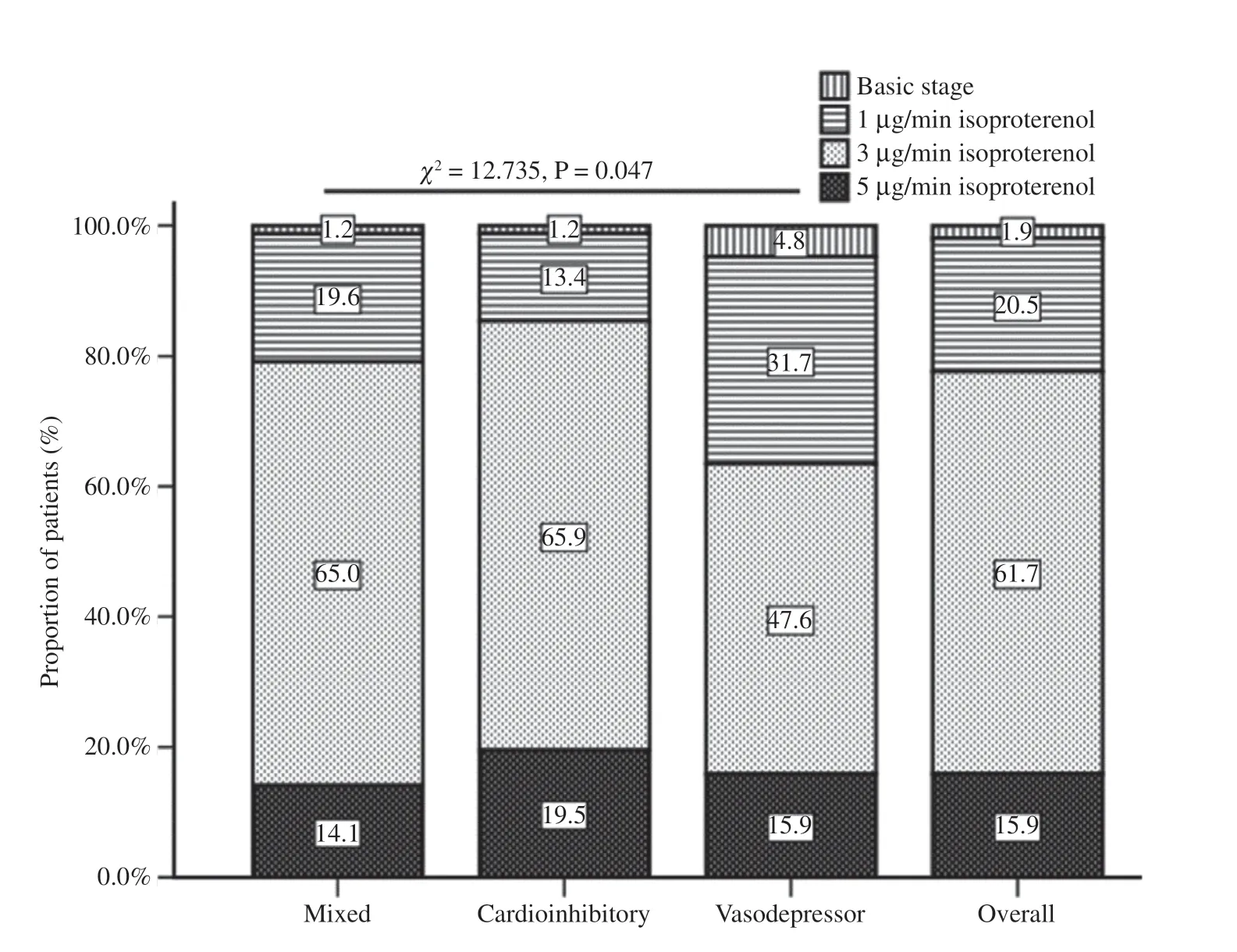
Figure1 Proportion of Patients with Different Syncope Patterns at Different Stages.

Table3 Heart Rate and Blood Pressure Derived from the Simplistic Tilt Test According to Head-up Tilt Test Results.
Predictive Roles of BP,HR,and BP/HR Ratios Derived from ABPM
With the exception of the mean DBP/HR ratio during the whole day (P = 0.057),the other BP/HR ratios derived from ABPM were signif icantly higher in the positive group than in the negative group ( Table5).Furthermore,BP/HR ratios were signif icantly higher in the cardioinhibitory group than in the negative group in the daytime,at nighttime,and during the whole day,while signif icances were observed only at nighttime between negative and mixed response patients.No signif icance was demonstrated in BP/HR ratios between negative and vasodepressor patients.The higher the mean SBP or DBP,the higher the isoproterenol dosage needed to induce a positive response in the daytime,at nighttime,or during the whole day ( Table6).However,there were no signif icant differences in the mean BP/HR ratios among syncope stages.Similarly,mean BP/HR ratios were higher in the positive group than in the negative group at each time point,although the difference was not signif icant ( Figure2A1- A3).Mean BP/HR ratios to predict syncope patterns were also observed at each hour ( Figure2B1- B3),while signif icant differences in BP were also found at each time point among syncope stages ( Figure2C1- C3).Almost no signif icance of ABPM-derived mean HR was found between positive and negative groups,among syncope subtypes,and among syncope stages.However,the distribution of HR at each time point had a signif icant difference between positive and negative groups,among syncope patterns,and among syncope stages.
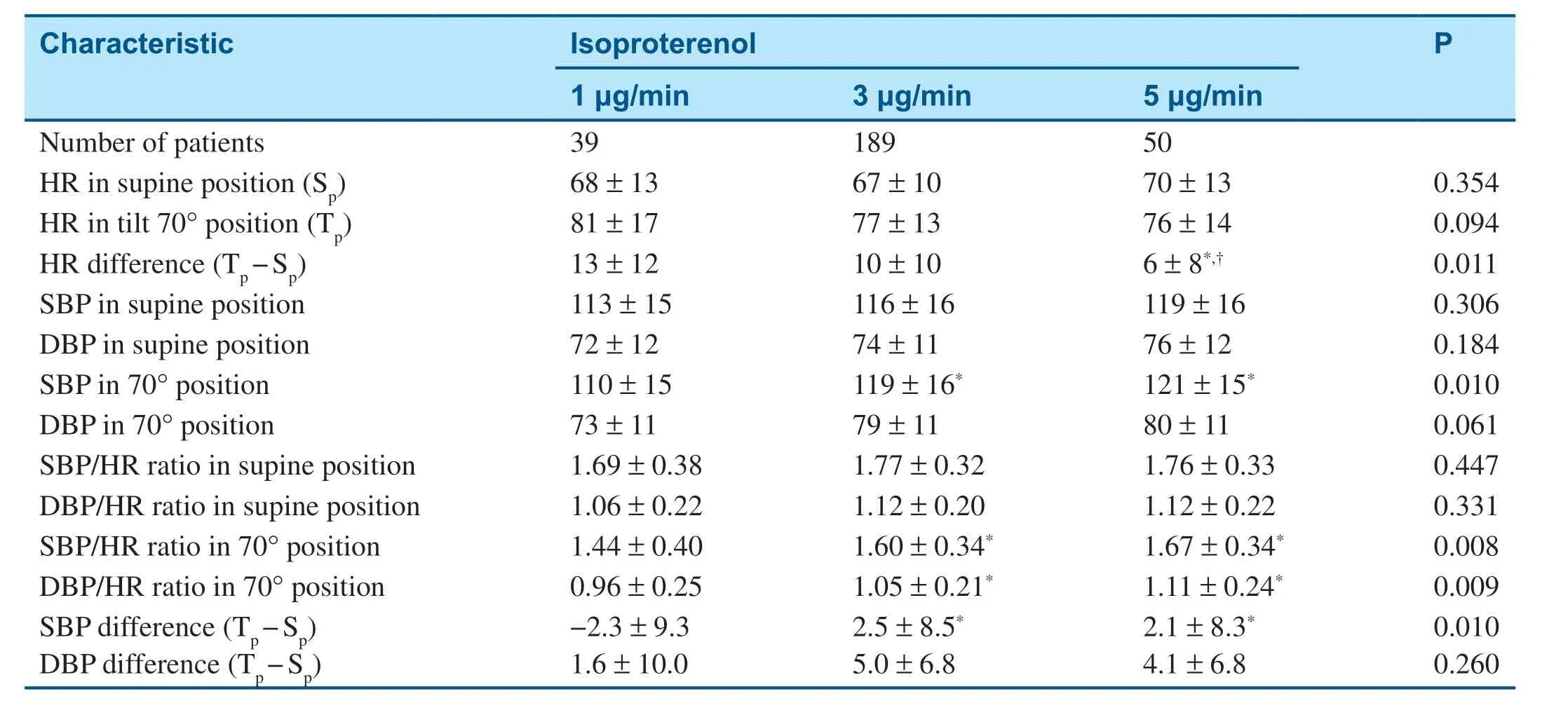
Table4 Heart Rate and Blood Pressure Derived from the Simplistic Tilt Test According to Syncope Stages.
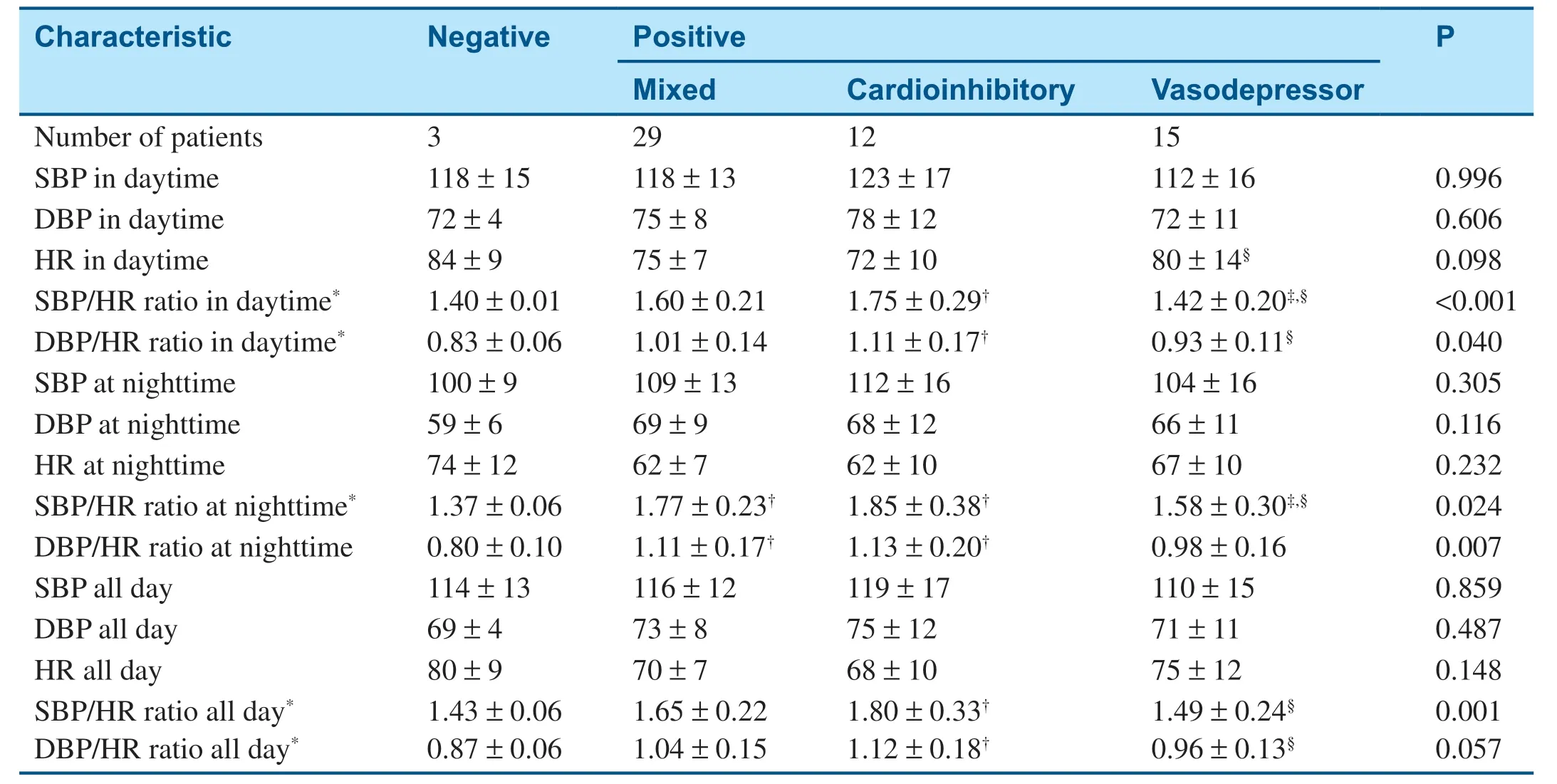
Table5 Mean Blood Pressure,Mean Heart Rate,and their Ratios Derived from Ambulatory Blood Pressure Monitoring According to Tilt-Test Results.

Table6 Mean Blood Pressure,Mean Heart Rate and their Ratios Derived from Ambulatory Blood Pressure Monitoring According to Syncope Stages.
Correlation of BP/HR Ratios between ABPM and the STT
Overall,there were signif icant differences in SBP/HR ratios between the STT in the supine position and ABPM in the daytime,at nighttime,and during the whole day,while for syncope subtypes,signif icant differences were found between the STT in the supine position and ABPM in the daytime,at nighttime,and during the whole day in mixed and vasodepressor patients but not cardioinhibitory patients ( Table7).There were signif icant differences in SBP/HR ratios between the STT in the tilted position and ABPM in the daytime,at nighttime,and during the whole day but not in any syncope pattern.For DBP/HR ratios,signif icant differences were also demonstrated overall and in mixed and vasodepressor groups but not in the cardioinhibitory group between the STT in the supine position and ABPM in the daytime,at nighttime,and during the whole day( Table8).Furthermore,signif icant correlations of the DBP/HR ratio were found overall and in the cardioinhibitory group between the STT in the tilted position and ABPM in the daytime,at nighttime,and during the whole day.
Discussion
The detailed medical history,physical examination,including supine and standing BP measurements,and electrocardiogram are usually used for diagnosis of VVS.However,additional tests may be performed for specif ic features that need further evaluation.Echocardiogram,angiogram,electrophysiological study as well as electroencephalogram,computed tomography and magnetic resonance imaging of the brain are not recommended for causal diagnosis of syncope,unless patients have specif ic features that need further evaluation [4,5].Our f indings further demonstrated that the aforementioned tests have low diagnostic yield and very high cost for diagnosis.Therefore,it is meaningful to avoid costly or invasive tests in patients without a complete evaluation with simple methods.
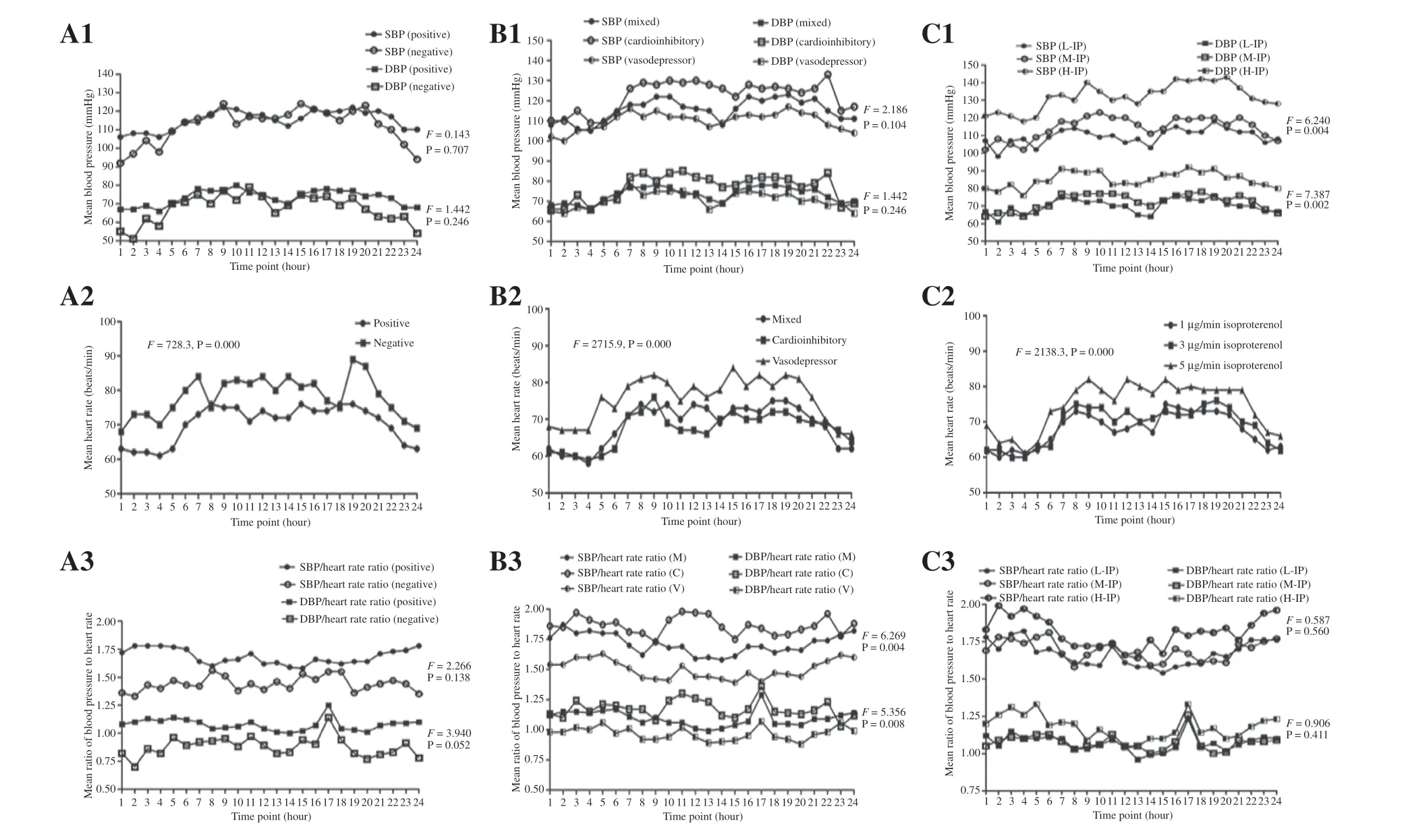
Figure2 The Trend of Parameters from Ambulatory Blood Pressure (BP) Monitoring According to Head-up Tilt Test Results at Each Hour.
The HUTT is widely accepted as a useful tool to demonstrate the susceptibility of a vasovagal response to a change from the supine position to the tilted position.If the diagnosis is unclear after initial evaluation,the HUTT can be useful for patients with suspected VVS [5].The HUTT for the diagnosis of VVS is useful and should not be abolished[6].There was a positive response in 94.8% of our selected patients,and more than half of positive reactions occurred with a isoproterenol infusion dosage of 3 μ g/min.Overall,mixed vasovagal response is the commonest syncope pattern.The prevalence of syncope pattern is inconsistent with another study[7],and difference in age and population selection might partly account for the phenomenon.However,the HUTT is somewhat time-consuming and expensive for diagnosis in busy clinical settings,and thus the STT and ABPM explored in the present study may be used as alternative tools in the clinical diagnosis of VVS.
Syncope during the HUTT seemed to be preceded by increased sympathetic activity manifested by an increase in HR as well as by a decreased parasympathetic tone before the episode [8].A prediction algorithm using simultaneous analysis of HR and SBP during the HUTT has been found to be a clinically relevant tool and could have applications,including providing a patient alarm,
shortening the tilt-test time,and triggering pacing intervention in implanTabledevices [9,10].Other studies also demonstrated that HR and BP are useful parameters for the prediction of VVS subtypes during the HUTT [9,11].As for other f indings[2],the present study revealed that patients with a positive test result had signif icantly lower HR during the STT.Signif icantly lower HRs mainly account for mixed and cardioinhibitory patterns rather than negative and vasodepressor patients.The changes in BP from the STT are different from those in pediatric VVS patients [12],suggesting different mechanisms account for different age groups.Consistent with other f indings [13],changes in HR during the STT tended to be larger in vasodepressor patients than in mixed and cardioinhibitory patients,with the largest HR difference occurring in vasodepressor patients.Resting SBP was higher in cardioinhibitory patients than in vasodepressor patients during the STT,which is consistent with other f indings [13].Our f indings demonstrated that BP/HR ratios in the tilted position could predict a positive response and when syncope would happen.The higher the BP/HR ratio in the tilted position,the greater possibility of a cardioinhibitory pattern and the higher the isoproterenol dosage needed to induce an episode.The larger the HR difference during the STT,the shorter the time to the occurrence of syncope.BP/HR ratios in the 70° position during the STT may be used as good predictors of a positive response,especially to indicate the cardioinhibitory pattern,as well as to predict the time when syncope will occur.In contrast,HR difference and SBP difference during the STT may predict syncope stages but not syncope patterns.These f indings suggest that a prediction algorithm using simultaneous analysis of HR and BP from the STT may be favored for use in a busy clinical practice and free patients from experiencing syncope during the HUTT,even as an alternative to the expensive and time-consuming HUTT.

Table7 Correlation of Ratios of Systolic Blood Pressure to Heart Rate Between the Simplistic Tilt Test and Ambulatory Blood Pressure Monitoring.

Table8 Correlation of Ratios of Diastolic Blood Pressure to Heart Rate Ratios Between the Simplistic Tilt Test and Ambulatory Blood Pressure Monitoring.
Although ABPM is generally not diagnostically helpful in patients who experience syncope,it does play a role in the monitoring of hypotension as well as therapeutic interventions [4,14].ABPM may help identify larger patients at high risk of syncope episodes and whether BP is low during syncope episodes [4,15],and be used as a noninvasive tool for exclusion of postural hypotension that is more sensitive than the HUTT [16].However,little is known about ABPM-derived BP,HR,and BP/HR ratios for predicting HUTT results in VVS patients.Our present study demonstrates that mean BP/HR ratios differed between positive and negative groups in the daytime,at nighttime,during the whole day,and at each time point.Furthermore,our study also demonstrates that BP/HR ratios were signif icantly higher in cardioinhibitory patients but not vasodepressor patients in comparison with the negative group in the daytime,at nighttime,and during the whole day.The mean SBP in the daytime was indistinguishablebetween the positive and negative groups,but was signif icantly lower than in the control group in another study [17].The derivative of the ratio between R-R interval and SBP was also demonstrated to be ableto predict the occurrence of syncope in all three patterns of VVS in advance during the HUTT [18].Predicting the occurrence of syncope in advance during the HUTT could be useful to prevent complications associated with the procedure,particularly in patients without any prodrome.Our f indings demonstrate that the lower the ABPM-derived BP,the earlier the time of occurrence of syncope.Additionally,patients with higher BPs at each time point usually have a positive response with the need for high-dosage isoproterenol.It is anticipated that BP/HR ratios may be better predictors of the presence and pattern of VVS,while BP should be used to predict the time when syncope will happen during the HUTT.
Our f indings further demonstrate that there are signif icant correlations of BP/HR ratios between ABPM and the STT.For syncope patterns,our f indings f irstly demonstrated that the correlation of SBP/HR and DBP/HR ratios in the supine position and ABPM may indicate a vasodepressor pattern,while the correlation of DBP/HR ratio in the tilted position and ABPM may suggest a cardioinhibitory subtype.Furthermore,the mixed pattern shares features of correlations of both vasodepressor and cardioinhibitory patterns between ABPM and the STT.It is obvious that different syncope patterns share different BP/HR ratios and different correlative patterns between ABPM and the STT.These f indings suggest that BP/HR ratios derived from ABPM may be used in combination with the STT to provide valuableinformation in the diagnosis of VVS,especially in the discrimination of cardioinhibitory patients from vasodepressor patients.However,a larger population with control groups is needed to explore diagnostic cut-points of these parameters from ABPM and the STT for management of VVS.
For extra information,please see the supplementary Figures S1- S3 online and also the supplementary information for Tables 3- 6.
Limitations
The cross-sectional and single-center nature is an important limitation of the present study.Additionally,that fewer patients in the negative group and not all patients had ABPM are other limitations of the present study.Attention should also be paid to the gap between the minimum and the maximum ages in the present study because age can sometimes affect the mechanisms and patterns of syncope.Finally,the cut-points for the diagnosis of VVS from both ABPM and the STT could not be provided because of the small population.
Conclusion
In summary,the STT providing diagnostic parameters,such as BP,HR,and BP/HR ratios,should be used as an alternative to the HUTT in busy clinical settings.BP/HR ratios derived from ABPM may be better predictors of the presence and pattern of VVS,while ABPM-derived BP should be used to predict the time when syncope will happen.It is believed that ABPM should be a cost-effective and noninvasive diagnostic method in combination with the STT for VVS evaluation and management,especially in patients refusing to have the HUTT and in busy clinical settings.
Acknowledgments
This work was supported by the Guangdong Natural Science Foundation Project (2018A030313531)and the Yat-Sen Scholarship for Young Scientists.
Conf ilcts of interest
The authors declare that they have no conf licts of interest.
 Cardiovascular Innovations and Applications2021年1期
Cardiovascular Innovations and Applications2021年1期
- Cardiovascular Innovations and Applications的其它文章
- Coronavirus 19 (some thoughts about the Disease)
- Relation between Cardiac Injury and Elevated Levels of Inf lammatory Biomarkers in Patients with Severe COVID-19
- The Challenges of Treating Acute Myocardial Infarction due to Variant Angina:Lesson from an Interesting Case
- Implantation of an S-ICD in a Patient with a DDD Pacemaker and Congenitally Corrected Transposition of the Great Arteries
- ECMO/CRRT Combined Support in the Treatment of Critically Ill SARS-CoV-2 Pneumonia Patients
- Risk of Target Organ Damage in Patients with Masked Hypertension versus Sustained Hypertension:A Meta-analysis