
ECMO/CRRT Combined Support in the Treatment of Critically Ill SARS-CoV-2 Pneumonia Patients
2021-03-18 07:41:10HaiZouandShengqingLi
Hai Zou and Shengqing Li
1 Institute of Pulmonary and Critical Care Medicine,Huashan Hospital,Fudan University,200040 Shanghai,China
Abstract Objective:To explore the experience with and complications of extracorporeal membrane oxygenation (ECMO)combined with continuous renal replacement therapy (CRRT) for treatment of critically ill patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia.Methods:The data on critically ill COVID-19 patients who received ECMO/CRRT at Tongji Hospital,which is aff iliated with Huazhong University of Science and Technology,in February and March 2020 were collected and analyzed.All three patients were male,and the mean age was 50.6 years (range 44- 58 years).The indications for ECMO in critically ill SARS-CoV-2 pneumonia patients at our center were severe acute respiratory distress syndrome with Pa o 2/F i o 2below100mmHgunderan effectiveprotectivepulmonary ventilationstrategyand infalmmatorystorm accompanied byacute kidney injury.One patient,with severeheart failure,wasselected forvenoarterial ECMO,and the other two patients were selected for venovenous ECMO.Results:In the three patients who received ECMO combined with bedside CRRT,the mean duration was 9.7 days(range 7- 13 days).Four complications occurred during ECMO/CRRT,especially thrombocytopenia.Laboratory testing showed increased counts of leukocytes and lymphocytes and decreased levels of inf lammatory factors.Lung CT was suggestive of signif icantly absorbed and reduced lesions and interstitial f ibrosis.Conclusions:The survival rate of patients with cardiopulmonary failure treated with ECMO/CRRT in whom conventional treatment failed in this group was 100%,which indicates that combined treatment with ECMO and CRRT is an important treatment technique.
Keywords:Extracorporeal membrane oxygenation; continuous renal replacement therapy; critically ill SARS-CoV-2 pneumonia patients
Introduction
Critical cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia account for approximately 15% of all patients with diagnosed COVID-19,and most of them experience multiple organ damage.Timely and effective treatment is the key to reducing the mortality rate in this epidemic.Among various treatment techniques,multiple organ support therapy with extracorporeal membrane oxygenation (ECMO)/continuous renal replacement therapy (CRRT) as the core is being considered.ECMO,an effective cardiopulmonary support therapy,plays an important role in the treatment of patients with severe heart and respiratory failure,and protective ventilation via a ventilator is an important means of respiratory support.CRRT is a relatively simple and effective method for kidney replacement,f luid management,and the clearance of cytokine storms.In this study,the data on three critically ill SARS-CoV-2 pneumonia patients who received combined ECMO/CRRT in the ICU of Optical Valley Branch,Tongji Hospital,which is aff iliated with Huazhong University of Science and Technology,are summarized and analyzed,with a focus on their medical conditions and complications,to further increase the cure rate of critically ill COVID-19 patients.
Materials and Methods
The data on patients who received combined ECMO and CRRT at Optical Valley Branch,Tongji Hospital,in February and March 2020 were analyzed retrospectively.The data included sex,age,initial symptoms,clinical symptoms,medical history,and complications.In addition,changes in inf lammatory indicators,including white blood cell count,lymphocyte count,and inf lammatory factors,at admission and during ECMO/CRRT combined treatment were monitored.All adult patients (18 years or older) were eligible for inclusion.This research,based on the revised Declaration of Helsinki,was approved by the ethics committee of Optical Valley Branch,Tongji Hospital.Informed consent was waived because of the unobtrusive retrospective design of the survey.
Diagnostic and Classif ication Criteria
All patients met the COVID-19 diagnostic criteria in“Guidelines for the Diagnosis and Treatment of COVID-19” (trial version 6) [1] issued by China’ s National Health Commission.The diagnosis of COVID-19 was conf irmed by a positive real-time f luorescent reverse transcription PCR test for SARS-CoV-2 nucleic acid.Patients were enrolled in the study if they were in a clinically critical condition on admission and had any of the following conditions:respiratory failure requiring mechanical ventilation,shock,or failure of other organs requiring ICU care and treatment.All three patients received tracheal intubation and ventilation.According to the patient’ s ideal body weight,a protective lung ventilation strategy was adopted,with a tidal volume of 4- 6 mL/kg,a plateau pressure no greater than 30 cm H2O,driving pressure less than 15 cm H2O,and positive end-expiratory pressure adjusted according to the optimal oxygenation.
ECMO Application Criteria
A MAQUET extracorporeal heart-lung machine and a heparin-coated ECMO circuit were used for all patients with Pa o2/F io2below 100 mmHg under an effective protective pulmonary ventilation strategy.The cannula was placed in the femoral vein and artery,and the selection of the right versus the left femoral vein and artery was based on the patient’ s individual conditions.The cannula was placed in the femoral vein and artery under direct vision.Sheaths of appropriate specif ications (14 F to 24 F for the artery and 16 F to 26 F for the vein) were selected according to intraoperative investigation.In our treatment protocol,ECMO was in venovenous mode or venoatrial mode.During ECMO assistance,the patient’ s oxygenation index,cardiac function,and hemodynamic parameters were monitored to adjust the ECMO f low and the dosage of positive inotropic drugs.Heparin was used to maintain an activated coagulation time of between 180 s and 220 s,and ventilator parameters and oxygen concentrations were appropriately adjusted according to the results of artery and vein blood gas analysis.None of the three patients experienced venous thromboembolism.Appropriate amounts of sedative and analgesic drugs were used during ECMO support.
ECMO Withdrawal Criteria
When a patient’ s condition was stable,the ECMO f low was gradually reduced to 10 mL/kg,and ECMO was withdrawn if the following conditions were maintained for 3- 4 h:average blood pressure greater than 60 mmHg with no or a small dosage of positive inotropic drugs; oxygenation index greater than 200 mmHg (the oxygen concentration delivered by the extracorporeal circuit is 21%,and the oxygen concentration delivered by the ventilator circuit is less than 40%).
CRRT Application Criteria
CRRT was indicated when acute kidney injury,cytokine storms,and f luid overload ( > 10%)occurred and were not relieved by diuretics.The Prismaf lex blood purif ication system was used.
Intubation,operation,daily management,and withdrawal of ECMO/CRRT were performed by the ECMO/CRRT multidisciplinary therapy (MDT)team.During ECMO/CRRT administration,attending physicians from the ECMO/CRRT MDT team and nurses specializing in ECMO/CRRT were on 24-h duty.Vital signs (mean arterial pressure,urine volume,infusion volume),analgesia and sedation management,nutrition management,and ECMO/CRRT function (considering possible thrombus and cannula damage) were recorded.The patient’ s mixed central venous blood oxygen saturation was maintained at 0.65- 0.75,hemoglobin level was maintained at more than 110 g/L,and hematocrit was maintained at more than 0.30.
Blood gas analysis (from before the membrane,after the membrane,and the patient),routine blood tests,blood biochemistry tests,blood lactic acid tests,bedside chest X-ray,and bedside cardiac ultrasonography were performed daily.
Routine blood,inf lammatory factor,liver and kidney function,and coagulation function tests were performed daily.Arterial and venous blood gas analysis,bedside cardiac ultrasonography,and chest radiography were performed every 2- 6 h.All of these data were required as indicators of patients’function during ECMO/CRRT therapy.
Statistical Methods
PASW Statistics was used.The associated data were presented.
Results
Three critically ill SARS-CoV-2 pneumonia patients received ECMO/CRRT in our study.The characteristics of the patients before ECMO are shown in Table1.The average age of the three patients was 50.6 years.They were all male.Patient 3 had a history of hypertension and diabetes.The other two patients had no signif icant comorbidity.All patients received protective mechanical ventilation,expectoration,and symptomatic support therapy,and there was no signif icant difference in treatment.
The ECMO and CRRT parameters are shown in Table2.Venovenous ECMO combined with CRRT was used in two patients with respiratory failure,and venoarterial ECMO combined with CRRT was used in one patient with both respiratory failure and heart failure.One patient underwent ECMO within 2 days after ICU admission,and two patients underwent ECMO 2 days later.One patient began CRRT before ECMO,and two patients began CRRT after ECMO.ECMO lasted 7- 13 days,and CRRT lasted 2- 9 days.All patients received unfractionated heparin sodium for anticoagulation.We used two methods of combining ECMO and CRRT.In the f irst method,the CRRTcircuit drew blood after the ECMO oxygenator and sent it back before the oxygenator but just after the ECMO pump ( Figure1A).In the second one,the CRRT circuit drew blood before the ECMO pump and sent it back after the pump but just before the ECMO oxygenator ( Figure1B).

Table1 Clinical Features of the Patients at the Time of Admission.
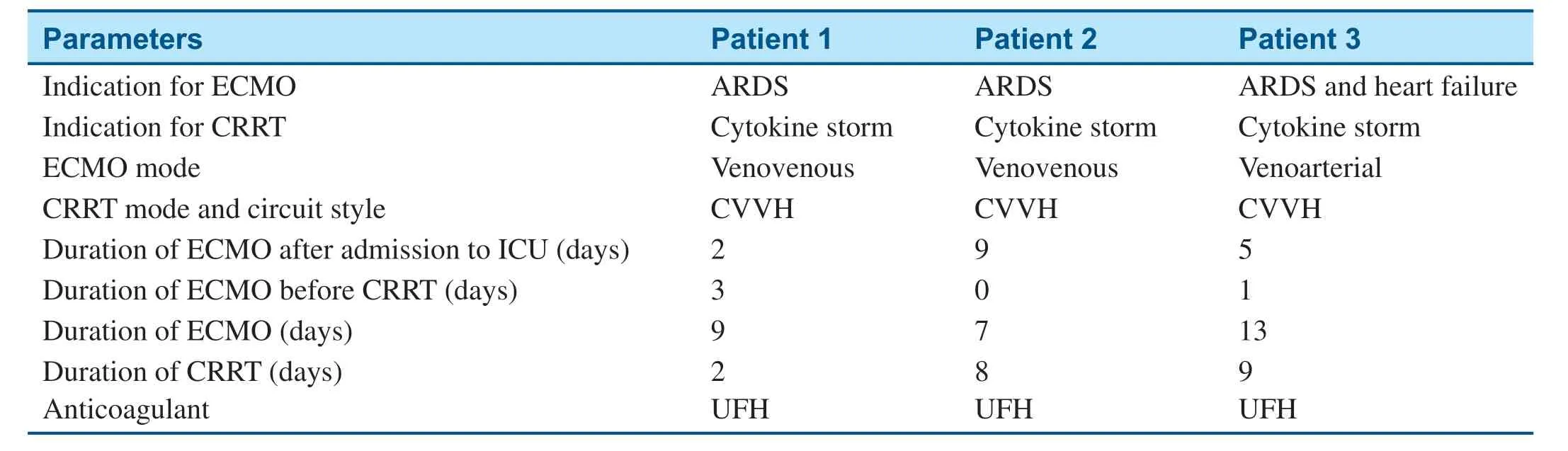
Table2 Extracorporeal Membrane Oxygenation (ECMO) and Continuous Renal Replacement Therapy (CRRT) Parameters for the Patients.
All three patients received serial blood purif ciation after ECMO,and the red indicate that they received blood purif ication treatment on the same day( Figure2,the CRRT time is marked on the f giure).All patients received continuous venovenous hemof iltration.The treatment time for blood purif ication ranged from 2 to 9 days.All patients were removed from the breathing machine and ECMO.CT scans of two patients showed a signif ciant decrease in groundglass opacity,and CT scan of one patient showed a continuous decrease in plaque opacity ( Figure3).One more CT scan was performed in each patient to view the reduce of residual f ibrosis.The changes in the levels of inf lammatory factors in the three patients are demonstrated individually in Figure2.After ECMO/CRRT,the lymphocyte counts of all three patients increased,and the levels of IL-2 and IL-6 decreased.Cardiac structure and valvular dysfunction were not found in all three patients during follow-up echocardio graphy.The left and right ventricles were normal in size and function.Two patients developed thrombocytopenia and aggravated active bleeding.All three patients survived.
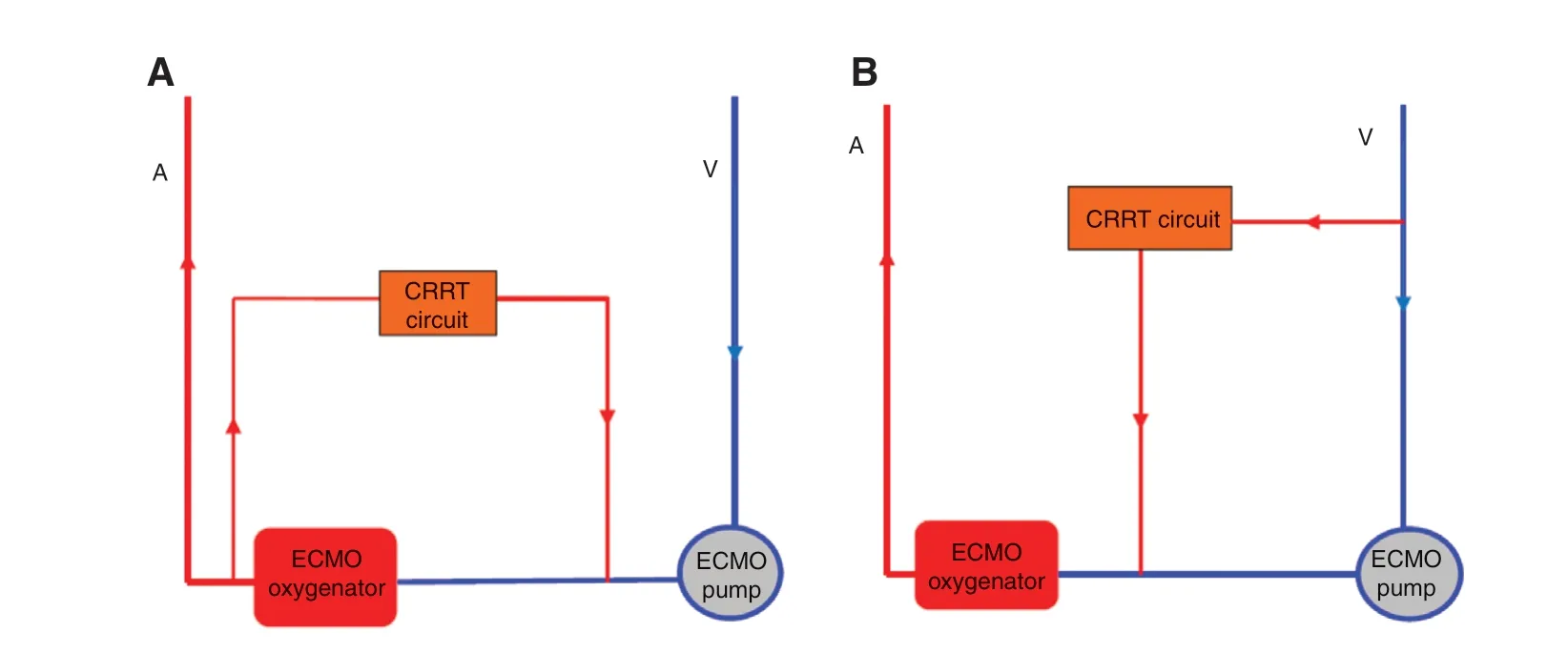
Figure1 Two Methods of Combining Extracorporeal Membrane Oxygenation (ECMO) and the Continuous Renal Replacement Therapy (CRRT) Circuit.A.The blood is drawn after oxygenation by ECMO,and returns to the end of the ECMO vein after f iltration.B.The blood goes through the f iltration,and returns to the end of the ECMO vein before oxygenation by ECMO.
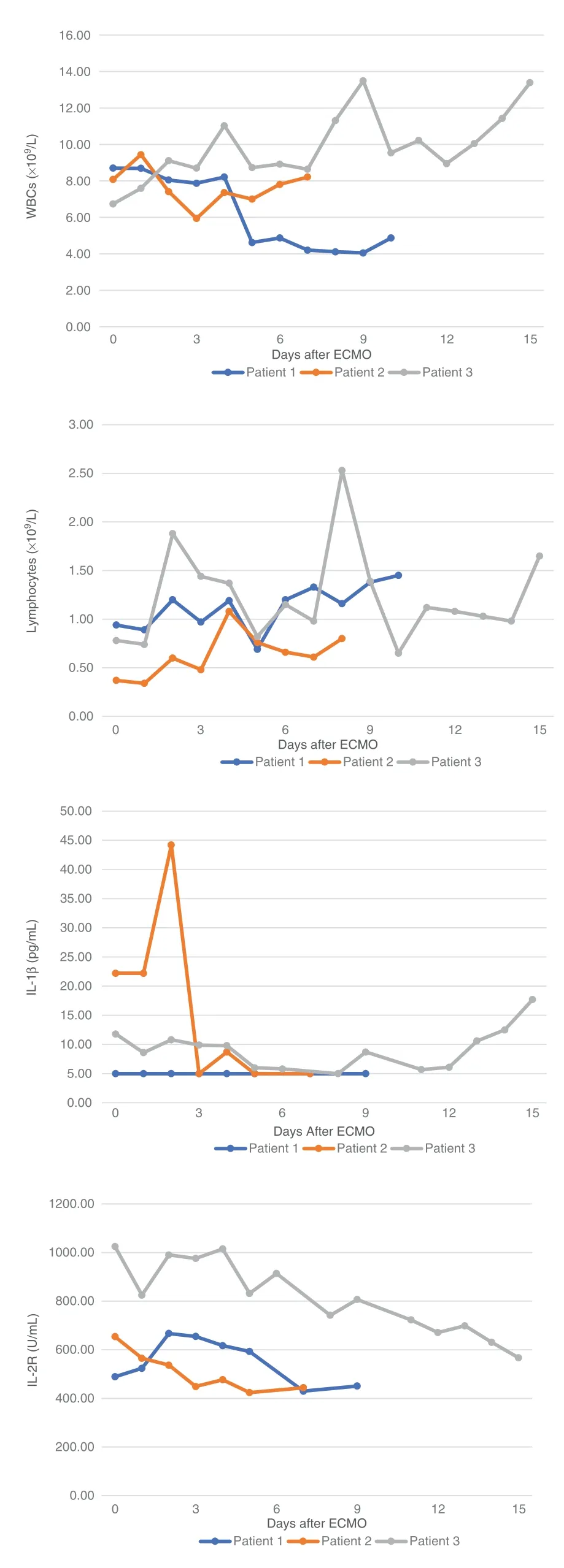
Figure2 (Continued)
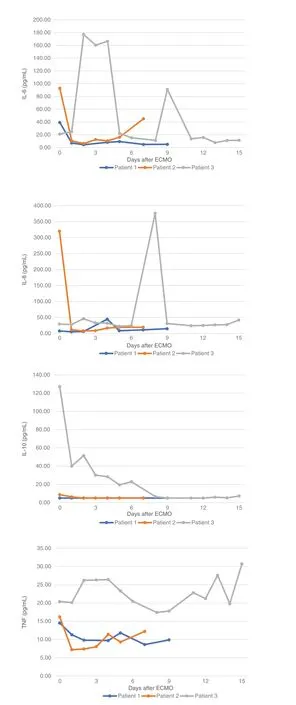
Figure2 Results of Laboratory Tests.
Discussion
In December 2019,a large number of SARS-CoV-2 infection cases emerged in Wuhan,Hubei province,China.Through sequencing analysis of respiratory or blood samples,a novel betacoronavirus was found; the World Health Organization named the disease caused by this virus “ COVID-19.” COVID-19 is caused by the seventh known coronavirus that can infect humans.Its transmission method and virus homology have many similarities with severe acute respiratory syndrome coronavirus (SARSCoV),so this virus was named “ severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2).In relation to the pathogenicity rates of SARS-CoV and Middle East respiratory syndrome coronavirus,SARS-CoV-2 is the third most deadly virus in the coronavirus family [2].As of March 11,2020,there were more than 80,000 conf irmed cases of SARSCoV-2 infection in 117 cities in China.All patients infected with SARS-CoV-2 developed pneumonia,and their clinical signs were suggestive of viral pneumonia; hence,this disease was f irst called“ novel coronavirus pneumonia.” Patients with mild SARS-CoV-2 pneumonia develop symptoms such as fever,cough,and fatigue,while patients with severe cases may have dyspnea,acute respiratory distress syndrome (ARDS),septic shock,incorrigible metabolic acidosis,and coagulation disorders [3- 5].Therefore,in-depth research on the treatment of critically ill SARS-CoV-2 pneumonia patients is of great importance.
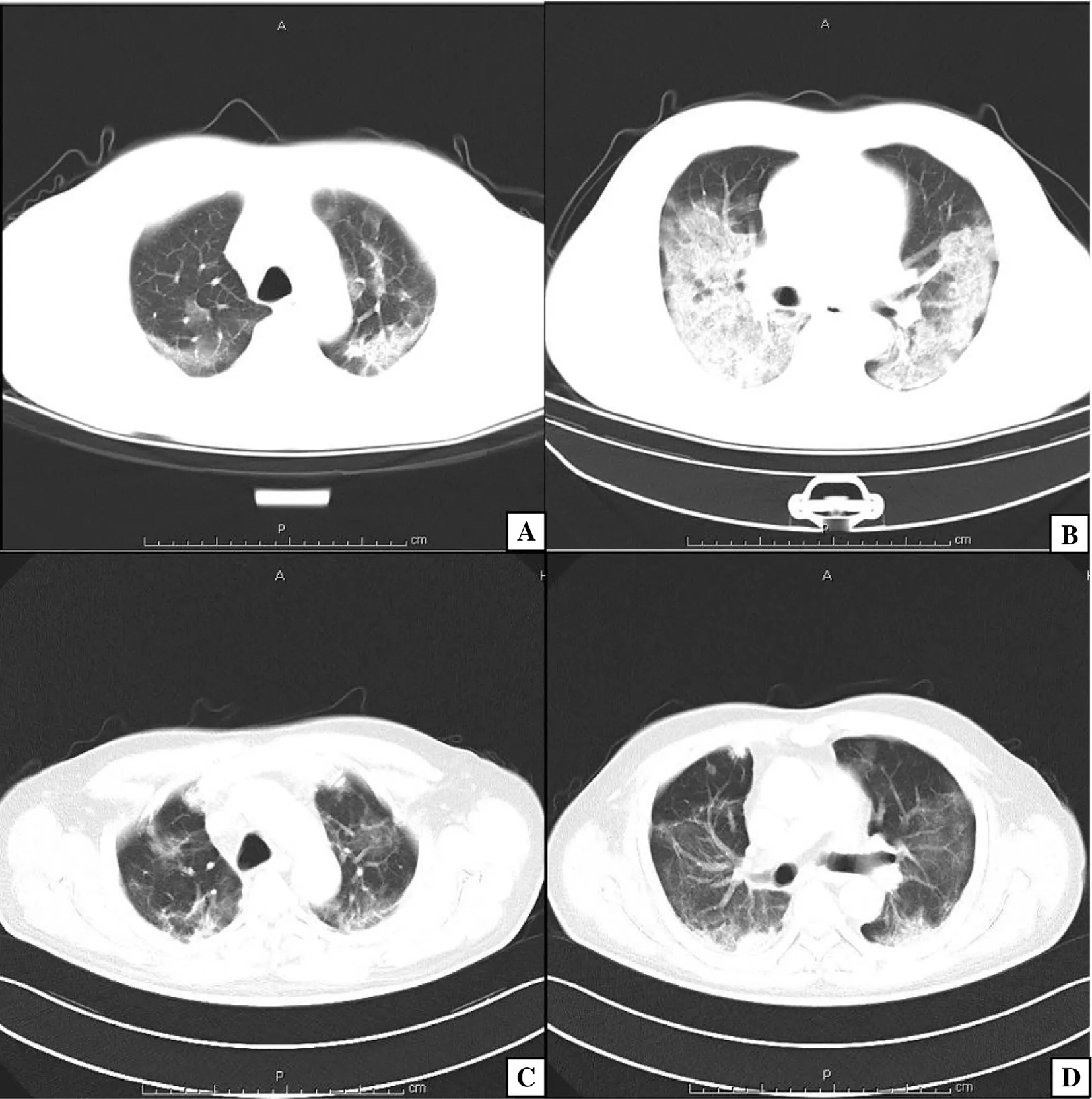
Figure3 (Continued)
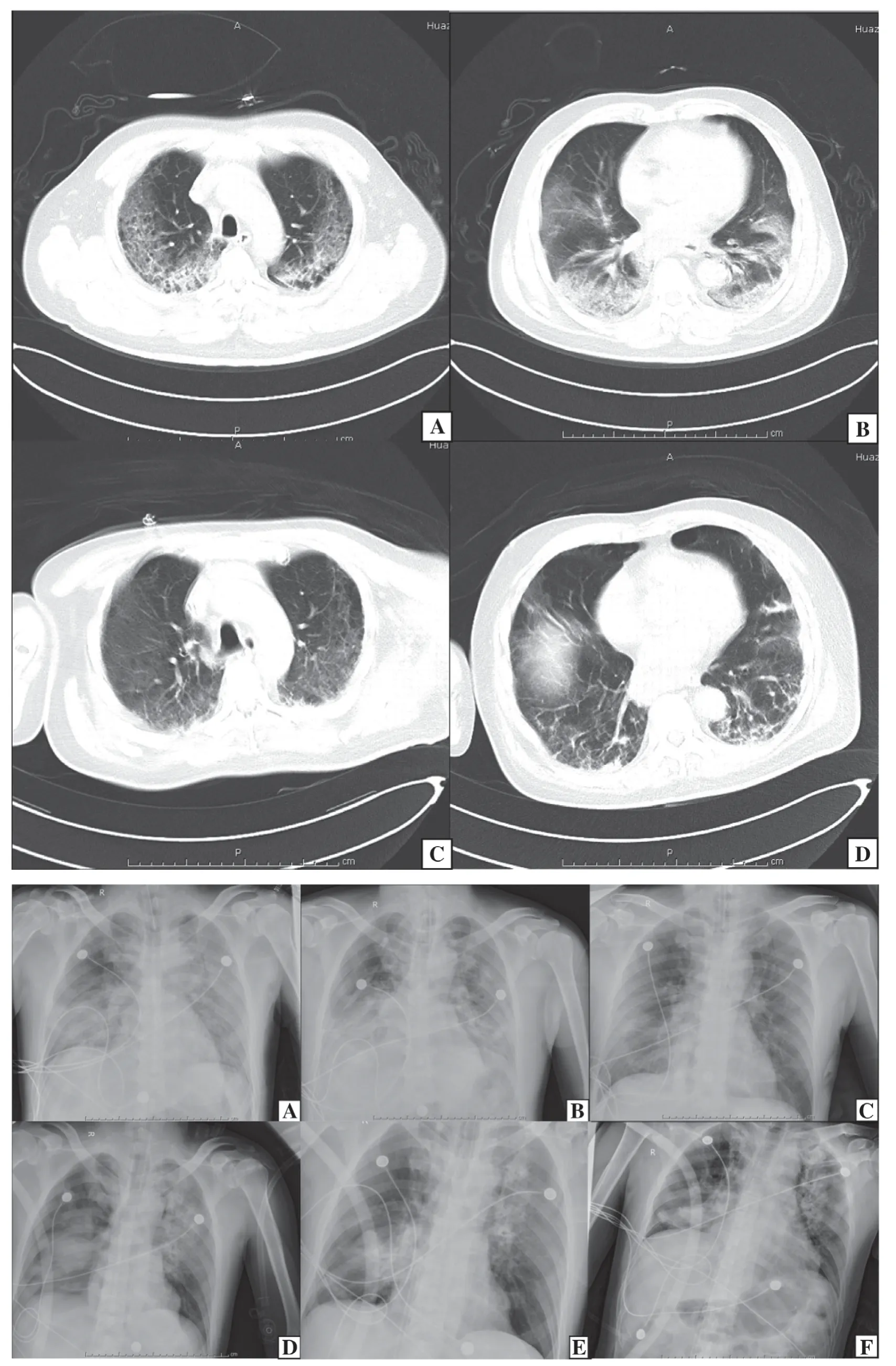
Figure3 (A) CT of Patient 1 Before (Panels A and B) and After (Panels C and D) Extracorporeal Membrane Oxygenation (ECMO) and Continuous Venovenous Hemof iltration (CVVH).(B) CT of Patient 3 Before (Panels A and B)and After (Panels C and D) ECMO and CVVH.(C) Chest Radiography of Patient 2 Before (Panels A- C) and After (Panels D- F) ECMO and CVVH.
In 1970,ECMO was f irst used in clinical practice to treat respiratory failure.ECMO can be an alternative for full lung function and partial heart function,providing effective circulatory and/or oxygenation support.Therefore,it is one of the most effective support techniques for patients with ARDS [6,7].What is more,ECMO is an effective technique for patients with acute severe cardiovascular disease,particularly acute fulminant myocarditis,providing heart and lung support and particularly adequate gas exchange or perfusion to sustain life.As Lin et al.[8] reported,ECMO can reduce the time to recapture sinus rhythm in acute fulminant myocarditis patients with hemodynamic compromise arrhythmia.Moreover,early ECMO use before cardiac arrest may be correlated with better outcomes [9].Additionally,ECMO is impacted by conditions of cardiac injury.Matsumoto et al.[10] reported that weaning fulminant myocarditis patients from ECMO also depends on cardiac rhythm disturbances and myocardial injury.Because traditional treatment methods such as protective lung ventilation,recruitment maneuvers,and prone ventilation failed to relieve hypoxemia in critically ill SARS-CoV-2 pneumonia patients,ECMO was considered as an alternative treatment.Because of the rapid progression of critically ill SARS-CoV-2 pneumonia patients and their gradual improvement with ECMO treatment methods,the indications for ECMO were expanded.Therefore,our team proposed that ECMO intervention treatment be applied at an earlier stage of SARS-CoV-2 pneumonia progression.As a result,the number of critically patients who were eligible to receive ECMO treatment increased signif icantly,and early treatment was conducive to relieving tissue hypoxia and protecting the airway mucosal barrier in critically ill SARS-CoV-2 pneumonia patients.According to clinical survey statistics,among severe ARDS patients with inf luenza A virus subtype H1N1 infection who received ECMO treatment,71% were cured and discharged [11].In this research,the survival rate of the three critically ill SARS-CoV-2 pneumonia patients treated with ECMO/CRRT was 100%.We analyzed and compared arterial blood gas indicators,hemodynamic indicators,and mechanical ventilation parameter settings before and after the treatment.The results showed that after ECMO/CRRT,the patients’ vital signs gradually recovered,and ventilation and oxygenation conditions improved signif icantly,which allowed the lungs to rest and allowed time for the primary lung disease to be treated fully.However,many studies show that as an invasive supportive treatment involving nonbiological materials,the ECMO technique may lead to a series of complications,such as systemic or local inf lammatory response and heart,lung,and kidney function damage.Therefore,during ECMO,most patients need CRRT to reduce the systemic inf lammatory response and the damage to lung,heart,and kidney function caused by ECMO [12].
On the basis of current clinical studies,the severe condition of SARS-CoV-2 pneumonia patients is related to the intensity of the body’ s inf lammatory response to virus particles.If there is an excessive inf lammatory response in the body,namely,a cytokine storm,this can lead to serious consequences and even death [13].The cytokine storm is an important factor leading to a poor prognosis,such as lung and other organ failure,in SARSCoV-2 pneumonia patients.According to Wu et al.[14] and Russell et al.[15] there is currently no specif ic treatment for large increases in the levels of cytokines such as IL-6,TNF,and interferon- γ.Glucocorticoids are mainly administered to nonspecif ically inhibit inf lammatory responses;thus,their long-term use has signif icant side effects and is likely to cause reinfection.Recent clinical analyses of early clinical data on the treatment of SARS and other infections have clearly indicated that nonspecif ic treatment with glucocorticoids is not supported for the treatment of lung injury [16].Therefore,clearing the cytokine storm is the key to increasing the survival rate of SARS-CoV-2 pneumonia patients.CRRT is considered a promising therapeutic strategy [17].Compared with conventional hemodialysis,CRRT shows better cardiovascular tolerance and metabolic regulation and relatively constant changes in plasma osmotic pressure,and it helps to correct acid-base and electrolyte disorders,thereby promoting the elimination of inf lammatory mediators.The convective transport of CRRT depends mainly on water permeability and transmembrane water f low and has nothing to do with particle size [18].Studies show that CRRT can adjust the body’ s immune response,eliminate interstitial edema,improve microcirculation,and increase cellular oxygen uptake capacity.It can also regulate electrolyte disorders and signif icantly clear inf lammatory mediators related to severe sepsis,such as TNF,IL-6,and IL-8,and increase the patient survival rate [19,20].Therefore,in terms of the cytokine storm that occurs in SARS-CoV-2 pneumonia patients,the immunoregulatory effect of CRRT has signif icant clinical therapeutic advantages.ECMO/CRRT,together with immunotherapy,can effectively reduce the mortality and organ failure rates.In the three patients in this study,CRRT was applied in parallel with the ECMO circuits,which was a simple operation.No serious adverse reactions occurred during the treatment; however,two patients developed thrombocytopenia and aggravated active bleeding,suggesting that CRRT combined with ECMO may increase the risk of coagulation disorders,a possibility that should be given further attention.
During the ECMO operation,the monitoring and treatment of complications is the key to increasing the success rate and should always be given top priority.Venovenous ECMO complications account for approximately 6.9% of deaths in adults with severe or refractory ARDS (95% conf idence interval 4.1- 11.2%) [21].The complications of ECMO are divided mainly into two categories:technologyrelated and body-related complications.Common technology-related complications include oxygenator dysfunction,intubation-related complications,hemolysis and thrombosis wherever during ECMO support,followed by power pump failure,cannula break,and air embolism.Observation and management by the ECMO/CRRT MDT team during the ECMO and CRRT monitoring process achieved good results.Generally,when this technique is used,there are numerous complicated monitoring indicators,and nurses may overlook some of them.In contrast,the medical team model helps nurses continuously observe and record patients’medical conditions,and mutual feedback between physicians and nurses also contributes to addressing problems in a timely manner.Body-related complications include mainly hemorrhage and embolism,infection,renal dysfunction,and nervous system injury.Among these,hemorrhage is the most common clinical complication.Mortality and prognosis of hemorrhage,infection,and nervous system injury are highly correlated.In the three patients treated with ECMO support in this study,four complications occurred; these comprised two mechanical complications and two physical complications,which occurred an average of once each.The incidence of complications was lower than that indicated in previous reports [22],which may be due to the small number of cases and the timely provision of treatment by the MDT team.
The wound is exposed for a long time during ECMO support,and wound infections and delayed healing are likely to occur after withdrawal.In the three patients included in this study,conventional wound drainage and incision debridement were not performed at the venous puncture site during ECMO withdrawal.Nevertheless,local debridement of the incision was performed at the arterial puncture site,and drainage tubes were placed when necessary.The wound was then closed in layers,and adipose tissue was ligated carefully to avoid the formation of a lymphatic f istula.With this method,none of the three patients experienced slow wound healing or infection.
In summary,ECMO/CRRT may be an effective treatment for critically ill SARS-CoV-2 pneumonia patients that has a good effect on recovery and prognosis.However,this study has limitations:f irst,it was a retrospective single-center study using observation analysis; second,the sample size of this study was small,and the sample size needs to be increased in the future; third,this study lacks follow-up of the patients outside the hospital.
Conf ilcts of Interest
The authors conf irm that there is no conf lict of interest.
 Cardiovascular Innovations and Applications2021年1期
Cardiovascular Innovations and Applications2021年1期
- Cardiovascular Innovations and Applications的其它文章
- Coronavirus 19 (some thoughts about the Disease)
- Relation between Cardiac Injury and Elevated Levels of Inf lammatory Biomarkers in Patients with Severe COVID-19
- The Challenges of Treating Acute Myocardial Infarction due to Variant Angina:Lesson from an Interesting Case
- Implantation of an S-ICD in a Patient with a DDD Pacemaker and Congenitally Corrected Transposition of the Great Arteries
- Predictive Value of Blood Pressure,Heart Rate,and Blood Pressure/Heart Rate Ratio in a Chinese Subpopulation with Vasovagal Syncope
- Risk of Target Organ Damage in Patients with Masked Hypertension versus Sustained Hypertension:A Meta-analysis