
Risk of Target Organ Damage in Patients with Masked Hypertension versus Sustained Hypertension:A Meta-analysis
2021-03-18 07:41:06YueWuGuoyueZhangRongHuandJianlinDu
Yue Wu ,Guoyue Zhang ,Rong Hu and Jianlin Du
1 Department of Cardiology,The Second Aff iliated Hospital of Chongqing Medical University,Chongqing 400010,China
Abstract Objective:To compare the risk of target organ damage in masked hypertension (MH) and sustained hypertension(SH).Methods:A systematic review and meta-analysis was performed.A search of PubMed,Embase,and the Cochrane Library of relevant case-control studies was performed from inception to December 2019,and articles on MH and SH selected according to the inclusion criteria were analyzed.The primary end point was target organ damage in the heart.The secondary end points were target organ damage in the kidneys and blood vessels.Results: Seventeen studies that met the screening criteria were included in the meta-analysis.Compared with the SH group,in the MH group carotid intima-media thickness (IMT) and E/A ratio were signif icantly greater and the prevalence of left ventricular remodeling and the pulse wave velocity were signif icantly lower.Other indicators in the heart,kidneys,and blood vessels were not statistically different between the two groups.IMT:P = 0.01,E/A ratio:P = 0.01,prevalence of left ventricular remodeling:P = 0.02,pulse wave velocity:P = 0.01.Conclusion: Our study has shown that MH may have almost the same degree of target organ damage as SH,so clinicians may need to consider target organ damage.
Keywords:masked hypertension; sustained hypertension; target organ; meta-analysis
Background
Today,hypertension is still one of the main causes of cardiovascular disease,leading to high mortality and high morbidity [1].The term “ masked hypertension” (MH) was f irst proposed by Pickering in the early years of the f irst decade of this century.He found people in whom hypertension had not been diagnosed by off ice blood pressure measurements[2,3].MH is def ined as normal off ice blood pressure and elevated ambulatory blood pressure (“ controlled blood pressure” if the person is receiving antihypertensive treatment).More and more evidence supports the view that MH is a blood pressure phenotype associated with an increased risk of fatal and nonfatal cardiovascular events compared with normal blood pressure [4 - 6].
Importantly,about one-third of hypertensive patients whose clinical blood pressure measurements show well-controlled blood pressure have higher blood pressure outside the physician’ s off ice [7,8].A high prevalence of up to 30% was described in obstructive sleep apnea [9].Concealed hypertension is often proven to develop into persistent hypertension,including in elderly people [10].It has been shown to have a cardiovascular risk almost similar to that of persistent hypertension in the general population and in patients with diabetes and chronic kidney disease [11].In addition to cardiovascular risk,studies have shown that in patients with MH there is a signif icant association between occult phenomena and target organ damage,such as left ventricular hypertrophy,increased carotid intima-media thickness (IMT),proteinuria,aortic stiffness,high pulse wave velocity (PWV),asymptomatic cerebral infarction,and early hypertensive retinopathy [7,12- 14].
However,the risk of target organ damage in patients with MH and sustained hypertension (SH) was not clear.So we aimed to evaluate the risk of target organ damage in MH compared with that in SH.
Methods
Search Strategy
We methodically searched PubMed,the Cochrane Library,and Embase for the following search keywords:“ masked hypertension,” “ masked hypertensions,” “ hypertensions,masked,” and “ hypertension,masked.” Keyword searches were limited to English only.Data collection was completed by December 2019.References in articles found with the initial search and relevant reviews were further searched to f ind additional eligible studies.
Inclusion Criteria
The inclusion criteria were as follows:(1) the original data are published in the literature; (2) the study participant receives a clinical diagnosis of essential hypertension (the patient’ s age is unlimited); (3) the study is an observational study; (4) the grouping method includes MH and SH; (5) the original literature has clear counting or measurement data on the patient’ s basic characteristics,target organ damage indicators,complications,etc.,and the results summarized in the literature can be expressed with corresponding statistical indicators; (6) for cases where the sample population is the same and the number of documents is more than one,the most recently published document is included.The preliminary screening and full-text evaluation were independently performed by two reviewers.
Appraisal of the Quality of the Studies
The quality of the studies was evaluated independently by the two assessors with use of the Newcastle-Ottawa Scale for qualitative evaluation of observational studies.Any disagreement in quality assessment was resolved through consensus.Studies scoring more than 7 were considered to have low risk of bias,scores of 5- 7 indicated moderate risk of bias,and a score of less than 5 indicated high risk of bias [15].
Data Extraction
Data extraction included the following:
1.Basic research information:publication journal,year of publication,whether blood pressure treatment was received,study population,sample source,etc.
2.Basic patient data,including age,number of males,number of current smokers,and body mass index.
3.Target organ damage- related indicators:creatinine level,estimated glomerular f iltration rate(eGFR),heart rate (HR),left ventricular mass index (LVMI),left ventricular ejection fraction(LVEF),left atrial diameter (LAD),left ventricular diastolic diameter (LVDD),interventricular septal thickness (IVST),relative wall thickness(RWT),E/A ratio,prevalence of left ventricular remodeling (LVR),PWV,and carotid IMT.
The full text of the articles selected by one or both of the assessors was retrieved for full evaluation.Two assessors read the full texts and independently extracted the information from the selected studies.A third assessor reviewed the data extraction,and any disagreement was resolved through consensus.
Data Synthesis and Analysis
Meta-analysis was performed with Stata 16.0.Before the effect amounts were merged,the included trialsweretestedforheterogeneity.Heterogeneity wasassessed withtheI2statistic.The chi-square test statistic was used to assess homogeneity between studies.I2is the proportion of total variation observed between the trials attribuTableto differences between the trials rather than sampling error (chance).The combined log odds ratio of counting data and the standardized mean difference of the measurement were both expressed by point estimates and the 95% conf idence interval.Publication bias was estimated visually by funnel plots and quantitatively by Egger’ s test.
Results
Literature Retrieval
Through the literature search,we retrieved 3729 articles.In total,2455 publications from the literature were found after removal of duplicates and reviews.After reading of the titles and abstracts,2360 articles were excluded.From the remaining 95 articles,17 were considered for inclusion in the study after review of the full text ( Figure1 ).
Study Characteristics
A total of 3756 participants with a mean age ranging from 41 to 69 years were recruited in the 17 eligible studies.Most studies include outpatients and inpatients as participants,and only four studies included community-dwelling participants.Most studies included participants who did notreceive antihypertensive treatment [7,16- 31]( Table1).
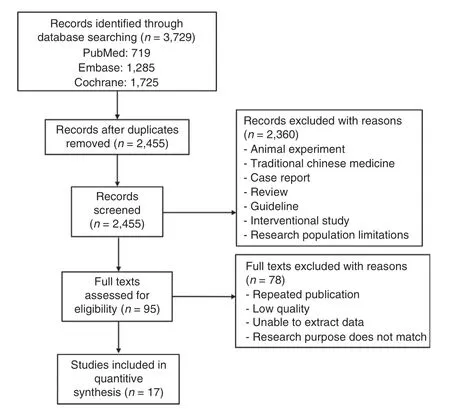
Figure 1:Flowchart of Literature Screening.
Analysis of Cardiovascular-Related Indicators
The cardiovascular-related indicators analyzed included HR,LVEF,LVMI,LAD,LVDD,IVST,RWT,E/A ratio,prevalence of LVR,IMT,and PWV.Among them,the prevalence of LVR and PWV in the MH group were signif icantly lower than in the SH group,which was statistically signif icant(P < 0.05),but PWV showed large heterogeneity(I2> 50%,P < 0.05) ( Figure2).Compared with the SH group,in the MH group IMT and E/A ratio were signif icantly greater (P < 0.05),without heterogeneity (I2< 50%,P > 0.05).HR,LVEF,LVMI,LAD,LVDD,IVST,and RWT were not signif icantly different between the two groups (P > 0.05).Except for LVMI and RWT,heterogeneity tests showed good homogeneity across the studies (I2< 50%,P > 0.05).According to Egger’ s test and the funnel plot of PWV(P < 0.05) ( Figure3),publication bias was likely to exist in the analysis.No signif icant publication bias with regard to HR,LVEF,LVMI,LAD,LVDD,IVST,RWT,and E/A ratio was observed ( Table2,Online Appendix Figures 1- 8).Prevalence of LVR:P = 0.02,LVEF:0.17,LVMI:P = 0.18,LAD:P = 0.11,LVDD:P = 0.85,IVST:P = 0.10,RWT:P = 0.34,E/A ratio:P = 0.01,Carotid IMT:P = 0.01,PWV (SMD):P = 0.01,Creatinine level:P = 0.03,eGFR:P = 0.30.
Analysis of Kidney-Related Indicators
The kidney-related indicators analyzed included creatinine level and eGFR.Compared with the SH group,in the MH group the creatinine levels were signif icantly lower (P < 0.05),without heterogeneity(I2< 50%,P > 0.05) ( Figure4).There was no signif icant difference in the eGFR between the two groups(P > 0.05),without heterogeneity (I2< 50%,P > 0.05)( Table2).
Discussion
The latest data show that the treatment and control of hypertension have improved.However,48% of the patients in the United States did not meet the blood pressure target of 140/90 mmHg [32].InEuropean hypertensive patients,the proportion is even higher at ≥ 90% [33].Importantly,about onethird of hypertensive patients have normal blood pressure in the clinic but higher blood pressure outside the clinic [7,8].Different hypertension phenotypes seem to have different types of organ damage mediated by hypertension.In addition to the obvious relationship between normal blood pressure and hypertension and organ damage,there are two other hypertension phenotypes.The white coat hypertension and MH phenotypes may also be associated with a higher risk of hypertension-mediated organ damage [11,34].

Table1 Characteristics of the Included Studies.
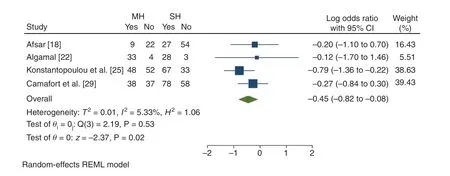
Figure2:Forest Map of the Prevalence of Left Ventricular Remodeling.

Figure3:Funnel Plot of Pulse Wave Velocity (PWV).
Since 1999,many lateral studies have evaluated left ventricular mass [35 - 39],RWT [40],andposterior wall thickness [41],and patients with MH are more likely to have left ventricular hypertrophy [38,42].Similarly,patients with MH are more likely to exhibit carotid artery wall thickening [39] or intima-media thickening [41].Our research showed that HR,LVEF,LVMI,LAD,LVDD,IVST,RWT,and eGFR were not statistically different between the MH group and the SH group.In addition to organ damage mediated by hypertension,an analysis of the Dallas Heart Study showed that MH is independently associated with vascular injury,renal injury,and cardiovascular events in the multiethnic population in the United States [12].Studies have shown that compared with patients with persistent hypertension,MH patients have similar incidences of fatal and nonfatal coronary events,stroke,and peripheral vascular death.The relative risks are 2.8 and 2.9,respectively,compared with those with true normal blood pressure [40].Therefore,consistent with previous studies,our research also proves that MH may not be innocent in clinical practice.
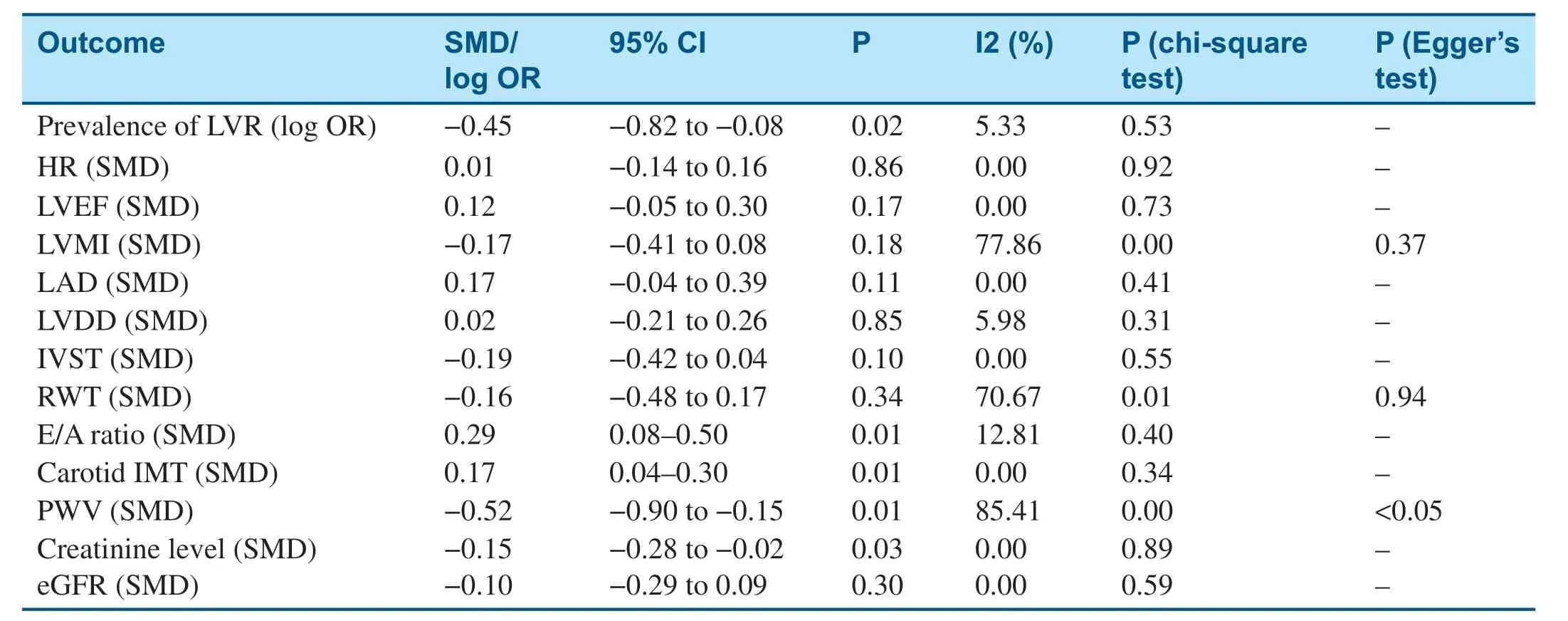
Table2 Meta-Analysis for Studies Included in the Analysis.
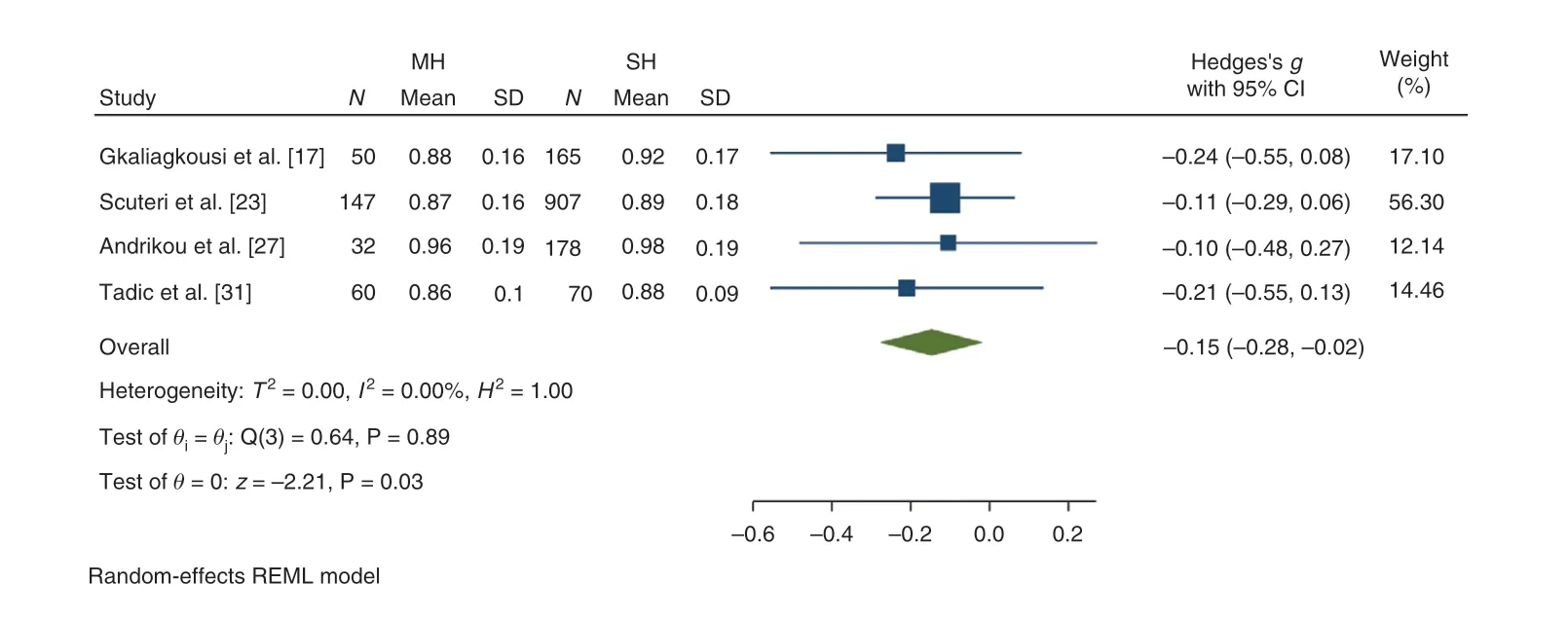
Figure4:Forest Map of Creatinine Level.
The factors that cause recessive hypertension are far from being understood.According to reports,when factors predicting latent hypertension in multivariate analysis are evaluated,male sex,smoking,and high body mass index are often identif ied as risk factors,but these predictors are still unclear [43- 46].This suggests that more clinical studies are needed to explore this issue in the future.
In clinical practice,MH is considered to have normal blood pressure in the normal population,and hypertensive patients in whom hypertension is treated seem to be under clinical control [47,48].Although most authorities generally recommend ambulatory blood pressure measurement [49,50],perhaps because of its higher sensitivity,its superiority over home blood pressure measurement is not supported by evidence on the basis of clinical results [6,51,52].In addition,from a practical point of view,home blood pressure measurement may be less troublesome for patients [53],and the ability to track off ice blood pressure within days,weeks,and months may not be logically feasible for ambulatory blood pressure.Given that ambulatory blood pressure and home blood pressure have diagnostic differences in the diagnosis of MH,and there is limited evidence that patients in whom diagnosis is made by these two methods may have a higher cardiovascular risk than patients in whom diagnosis is made by any of the other methods described above [6].Therefore,we recommend evaluation and followup by two methods in clinical work,which may increase the overall diagnosis rate and may translate into improved patient prognosis.It is very important to detect MH as early as possible and give reasonableand standard antihypertensive treatment.
In conclusion,our study has shown that MH may have almost the same degree of target organ damage as SH,so clinicians may need to consider target organ damage.
 Cardiovascular Innovations and Applications2021年1期
Cardiovascular Innovations and Applications2021年1期
- Cardiovascular Innovations and Applications的其它文章
- Coronavirus 19 (some thoughts about the Disease)
- Relation between Cardiac Injury and Elevated Levels of Inf lammatory Biomarkers in Patients with Severe COVID-19
- The Challenges of Treating Acute Myocardial Infarction due to Variant Angina:Lesson from an Interesting Case
- Implantation of an S-ICD in a Patient with a DDD Pacemaker and Congenitally Corrected Transposition of the Great Arteries
- Predictive Value of Blood Pressure,Heart Rate,and Blood Pressure/Heart Rate Ratio in a Chinese Subpopulation with Vasovagal Syncope
- ECMO/CRRT Combined Support in the Treatment of Critically Ill SARS-CoV-2 Pneumonia Patients